Embed Size (px)
Citation preview

135
□ CASE REPORT □
Tuberculous Osteomyelitis in the Ulna of a PatientUndergoing Hemodialysis
Yuka Nakazawa 1, Tomoya Nishino 1, Atsushi Mori 1, Tadashi Uramatsu 1,2, Yoko Obata 1,3,
Hideyuki Arai 1, Hideyuki Hayashi 4, Shoko Tsukasaki 5, Yoshiaki Muraya 6, Yuichi Inoue 6,
Yoshihiro Yamamoto 1 and Shigeru Kohno 1
Abstract
A 76-year-old woman on hemodialysis (HD) presented with pain and swelling in the left wrist and fore-
arm. The osteomyelitis occurred in the part of the ulna adjacent to the arteriovenous fistula. Mycobacteriumtuberculosis was identified in pus obtained from the left forearm, leading to a diagnosis of tuberculous osteo-
myelitis. The patient was treated with anti-tuberculous drugs and her symptoms improved. In this study, we
report a case of tuberculous osteomyelitis occurring in the ulna, which is not the usual site of predilection for
tuberculosis infection. As HD patients exhibit a high frequency of extrapulmonary tuberculosis, tuberculous
osteomyelitis should be considered in the differential diagnosis of infectious osteomyelitis. In addition, it may
be useful to perform stab cultures at an early stage in order to diagnose tuberculous osteomyelitis.
Key words: tuberculous osteomyelitis, ulna, hemodialysis, arteriovenous fistula, Mycobacterium tuberculosis
(Intern Med 52: 135-139, 2013)(DOI: 10.2169/internalmedicine.52.8437)
Introduction
Tuberculosis (TB) is the leading cause of illness and
death in many countries and has become a global public
health problem. Moreover, decreased immunity in end-stage
renal disease (ESRD) patients results in a high prevalence
and mortality rate of TB in this population compared to that
observed in the general population (1, 2).
Extrapulmonary TB, either isolated or associated with
pulmonary TB, has been reported to occur in approximately
60-80% of patients undergoing hemodialysis (HD) (3-6). Pa-
tients with extrapulmonary TB often present with many non-
specific symptoms such as general malaise, poor appetite,
low-grade fever, weight loss, night sweats and lymphadeno-
pathy (2, 7). It is particularly difficult to differentiate tuber-
culous osteomyelitis from bacterial osteomyelitis or bone tu-
mors. Therefore, there is an average time gap of 3-6 months
between the first appearance of symptoms and diagno-
sis (8-11). This held true in the present case, as six months
were required to reach a diagnosis of tuberculous osteomye-
litis. At the onset of symptoms, the patient experienced pain
and swelling of the left wrist and forearm. Magnetic reso-
nance imaging (MRI) showed osteolytic changes and ab-
scess formation in the left ulna. Based on these findings, we
first suspected a diagnosis of pyogenic osteomyelitis caused
by bacteria. The results of a culture test of the pus dis-
charged from the disintegrated skin of the left forearm were
positive for M. tuberculosis, and the patient was definitively
diagnosed with tuberculous osteomyelitis. To the best of our
knowledge, there have been no previous reports of tubercu-
lous osteomyelitis occurring in the ulna of an HD patient.
Even though the ulna is not a site of predilection for TB in-
fection, tuberculous osteomyelitis should be considered in
the differential diagnosis of infectious osteomyelitis in
ESRD patients.
1The Second Department of Internal Medicine, Nagasaki University School of Medicine, Japan, 2Division of Blood Purification, Nagasaki Uni-
versity Hospital, Japan, 3Medical Education Development Center, Nagasaki University Hospital, Japan, 4Department of Radiology and Radiation
Biology, Nagasaki University Graduate School of Biomedical Sciences, Japan, 5Tanaka Clinic, Japan and 6Isahaya Health Insurance General
Hospital, Japan
Received for publication June 21, 2012; Accepted for publication September 23, 2012
Correspondence to Dr. Tomoya Nishino, [email protected]

Intern Med 52: 135-139, 2013 DOI: 10.2169/internalmedicine.52.8437
136
Table. Laboratory Data on Admission
RBC 362×104 Na 142 mEHb 10.5 K 4.4 mEPlt 33.1×104 Cl 104 mEWBC 6,600 Ca 10.6
Neut 67.4 % BUN 44ym 18.8 % Creatinine 8.6
Mon 9.0 % TP 6.8Eosi 3.9 % 2.8Baso 0.9 % T-Cho 182
T-Bil 0.3PT 86.9 % AST 13PT(INR) 1.10 5APTT 28.3 sec 157Fibrinogen 491 -GTP 18
163ESR 1hr 48 mm Glucose 126
2hr 60 mm CRP 1.74RBC: red blood cells, Hb: hemoglobin, Plt: platelets, WBC: whiteblood cells, Neut: neutrocytes, ym: lymphocytes, Mon: monocytes, Eosi: eosinophils, Baso: basophils, PT: prothrombin time, INR: international normalized ratio, APTT: activated partial thromboplastin time, ESR: erythrocyte sedimentation rate, Na: sodium, K: potassium, Cl: chrolide, Ca: calcium, BUN: blood urea nitrogen, TP: total protein,
B: albumin, T-Cho: total cholesterol, T-Bil: total bilirubin, AST: aspartate aminotransferase, A T: alanine aminotransferase, P: alkaline phosphatase, -GTP: -glutamyltransferase, H: lactate dehydrogenase, CRP: C-reactive protein
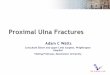
Figure 1. Radiographs of the left forearm region on ob-tained admission and 18 months after the initiation of treat-ment. A. A radiograph of the left forearm region obtained on admission showing fractures in the distal end of the left ulna with osteolytic changes. B. A radiograph of the left forearm region obtained 18 months after the initiation of treatment showing bone reconstruction and formation of the ulna.
Case Report
The patient was a 76-year-old woman without a history of
TB. She began to undergo HD in January 2005 due to
ESRD caused by benign glomerulosclerosis. Since then, she
had undergone HD three times a week at a nearby hospital.
Since December 2006, she had experienced pain in her left
wrist and forearm. In March 2007, she developed worsening
pain and swelling in the left wrist and forearm and pre-
sented with a low-grade fever and elevated levels of white
blood cells (WBCs) and C-reactive protein (CRP). A diag-
nosis of bacterial cellulitis was suspected, and antibiotics
(amoxicillin, levofloxacin and minocycline hydrochloride)
were administered. After receiving antibiotic treatment, the
patient showed a slight improvement in her symptoms; how-
ever, the elevated levels of WBCs and CRP did not return to
normal. She was admitted to our hospital in April 2007 for
further examination and treatment.
On admission, the patient’s height was 153 cm, her dry
weight was 59.8 kg, her body temperature was 36.2℃ and
her blood pressure was 191/83 mmHg. Upon physical ex-
amination, she showed redness and swelling on the distal
side of the left forearm. The laboratory data were as fol-
lows: WBCs, 6,600/μL; neutrophils, 67.4%; lymphocytes,
18.8%; monocytes, 9.0%; CRP level, 1.74 mg/dL; erythro-
cyte sedimentation rate (ESR) 1 h/2 h, 48/60 mm; total pro-
tein (TP) level, 6.8 g/dL; albumin level, 2.8 g/dL; and Ca
level, 10.6 mg/dL. These data indicated the presence of a
mild inflammatory reaction, hypoalbuminemia and hypercal-
cemia (Table). Radiographs of the left forearm revealed a
fracture with osteolytic changes at the distal end of the ulna
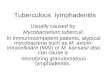
(Fig. 1A). MRI revealed bone destruction in the left ulna
(Fig. 2A, B), and the bone marrow showed low signal inten-
sity on T1-weighted images with fluid accumulation in the
surrounding soft tissue (Fig. 2A). On the basis of these re-
sults, we suspected the presence of bacterial osteomyelitis
and abscess formation.
After performing curettage of the left ulnar lesion, we
scheduled placement of a continuous perfusion drain. How-
ever, since the arteriovenous fistula used for vascular access
was located ipsilateral to the lesion, there were risks for
massive bleeding during the procedure and for infection
spreading to the arteriovenous fistula and subsequently to
the patient’s entire body. Therefore, we performed surgery
to close the arteriovenous fistula. After surgery, pus dis-
charge was observed from the disintegrated skin surrounding
the swollen region of the left forearm. To identify the spe-
cific pathogen causing the osteomyelitis, we performed a
culture test and a polymerase chain reaction (PCR) test on
the pus. The results of Gram and Ziehl-Neelsen staining
were negative; however, the culture and PCR test results
were positive for M. tuberculosis. Based on these findings,
the patient was diagnosed with tuberculous osteomyelitis of
the left ulna. Therefore, we cancelled the planned drainage
and initiated treatment with anti-tuberculous drugs (rifam-
picin, 450 mg/day; isoniazid, 300 mg/HD day; and strepto-
mycin, 0.5 g/twice a week; via intramuscular injection). We
also assessed the patient for pulmonary TB using chest radi-
ography and computed tomography; however no pulmonary
lesions were found. Four weeks after the initiation of anti-
mycobacterial treatment, the patient began to show de-
creased inflammation and improved imaging findings on
both radiography and MRI (Figs. 1B, 2C, D). The patient
received 15 months of anti-mycobacterial treatment (rifam-
picin, 450 mg/day; isoniazid, 300 mg/HD day; streptomycin,
0.5 g/twice a week; via intramuscular injection) and thus far

Intern Med 52: 135-139, 2013 DOI: 10.2169/internalmedicine.52.8437
137
Figure 2. MRI images of the left forearm obtained on admission and eight weeks after the initia-tion of treatment. On admission, bone destruction was observed in the metaphysis of the left ulna. The surrounding marrow presented a low signal on a T1-weighted image. Fluid accumulation was also observed in the surrounding soft tissue. New bone formation was observed and fluid accumula-tion was decreased in the soft tissue eight weeks after the initiation of treatment. A. A T1-weighted image (T1WI) obtained on admission; B. A T2-weighted image (T2WI) obtained on admission; C. A T1WI obtained eight weeks after the initiation of treatment; and D. A T2WI obtained eight weeks after the initiation of treatment.
has shown no evidence of relapse.
Discussion
The incidence of TB among HD patients is reported to be
6-25 times higher than that observed in the general popula-
tion (2). Moreover, the mortality rate of HD patients with
TB is 17-75% (1). A common finding associated with ure-
mia is impaired immunity, including disorders of T-
lymphocyte growth and activation, lymphopenia and de-
creased antigen-specific humoral immunity mediated by T-
lymphocytes (12). In addition, several factors specific for
HD patients, such as malnutrition, anemia, vitamin D defi-
ciency and hyperparathyroidism, may further contribute to
impaired immunity (13-16). Therefore, HD patients are con-
sidered to have high susceptibility to TB, and latent TB is
52.5 times more likely to be reactivated in patients with re-
nal failure than in the general population (1, 17).
Extrapulmonary TB, either isolated or associated with
pulmonary TB, has been reported to occur in approximately
60-80% of HD patients. The most common forms of ex-
trapulmonary TB are lymphadenitis, gastrointestinal, bone,
genitourinary, peritoneal, pleural, pericardial and miliary
TB (3-6). Osteoarticular TB has been reported to account
for 12.5% of extrapulmonary TB cases in HD patients. The
most common site of osteoarticular TB is the spine, ac-
counting for 56% of all cases, followed by joints. Tubercu-
lous osteomyelitis occurring in the long bones, as was ob-
served in our patient, is uncommon (18). Although the
mechanisms by which M. tuberculosis reaches bone are un-
known, the pathogen is thought to do so hematogenously, as
it commonly grows within the marrow cavity. In most cases,
osteoarticular TB is caused by an endogenous reactivation of
M. tuberculosis from a latent lesion. Usually, these lesions
remain inactive; however, they can reactivate when cellular
immunity is decreased (19, 20). In the present case, no pul-
monary lesions were found. Therefore, in the present case,
tuberculous osteomyelitis likely developed from an already
infected focus of the previously disseminated ulnar region.
However, another possible pathogenesis in this case is that

Intern Med 52: 135-139, 2013 DOI: 10.2169/internalmedicine.52.8437
138
reactivated M. tuberculosis, as a result of decreased immu-
nity due to advanced age and ESRD, moved to the left ulna
via the blood stream and became associated with the arte-
riovenous fistula.
Since tuberculous osteomyelitis does not generally present
with any characteristic imaging findings or clinical manifes-
tations, it is difficult to differentiate between bacterial osteo-
myelitis and bone tumors. Therefore, an average time of 3-6
months passes from the first appearance of symptoms to di-
agnosis. As possible points of differentiation between bacte-
rial osteomyelitis and tuberculous osteomyelitis, Monach et
al. reported that patients with tuberculous osteomyelitis pre-
sent with a low-grade fever and exhibit so-called “cold ab-
scesses” that are without local redness or warmth (21).
However, in the present case, redness and swelling were ob-
served on the distal side of the left forearm, which is an un-
common site of tuberculous osteomyelitis. Another differen-
tial point is that hypercalcemia is observed in 2.3-51% of
TB patients, although the prevalence of hypercalcemia in pa-
tients with TB varies widely (13). Hypercalcemia in TB pa-
tients is considered to be caused by an increased production
of 1,25(OH)2D3, which enhances calcium absorption in
granulomatous lesions (22). It is important to note that our
patient was not administered drugs, such as calcium carbon-
ate or active vitamin D, that can elevate the serum Ca lev-
els. In addition, the patient did not have secondary hyper-
parathyroidism, malignant tumors or any granulomatous dis-
eases other than TB. After the administration of anti-
tuberculous treatment, the patient’s levels of serum Ca de-
creased and became normal (Ca; 9.0 mg/dL). Therefore, the
hypercalcemia observed in the present case may have been
caused by the tuberculous osteomyelitis.
Regarding the early diagnosis of extrapulmonary tubercu-
losis in HD patients, there are some points that should be
considered. First, as extrapulmonary TB is common in HD
patients, the possibility for tuberculosis should be always
considered. Second, because appropriate specimens may be
difficult to obtain from some sites, acquiring bacteriological
confirmation is often more difficult for extrapulmonary TB
than for pulmonary TB. Moreover, relatively few M. tuber-culosis organisms are present in extrapulmonary sites, and
identification of acid-fast bacilli in specimens obtained from
these sites using microscopy is infrequent. Therefore, per-
forming PCR tests for TB in addition to cultures and histo-
pathological examinations of tissue specimens, such as those
that may be obtained with needle aspiration or biopsies, as
diagnostic tests for extrapulmonary TB is recom-
mended (23). Third, the tuberculin skin test exhibits poor
sensitivity in HD patients. Recently, many reports have in-
vestigated the usefulness of the QuantiFERON-TB test
(QFT) as a tool for diagnosing TB (2). Although we did not
perform a QFT in our patient because the practice had not
been widely adopted at the time of treatment, QFTs might
be useful for making future diagnoses. Therefore, enhanced
awareness of TB in HD patients along with providing earlier
diagnosis and treatment may improve the outcomes of infec-
tion in these patients.
Regarding the treatment of tuberculous osteomyelitis,
multidrug therapy using three to four drugs for six to 12
months or more is recommended, while surgical drainage is
not usually recommended as an initial therapy (24). In the
present case, 15-month treatment with rifampicin, isoniazid
and streptomycin resulted in improvements in the patient’s
inflammatory reaction and imaging findings, and no recur-
rence has since been reported. We selected this treatment
regimen for the patient, although it was not the standard
protocol, because the patient was elderly and had defective
cellular and humoral immunity caused by ESRD and HD.
Additionally, she showed gradual improvements on imaging
tests.
In this case, the osteomyelitis occurred in the part of the
ulna adjacent to the arteriovenous anastomotic region. Gen-
erally, patients on HD are at an increased risk of developing
infections and bacteremia. The incidence rate of bacteremia
ranges from 0.04 to 0.55/1,000 patient-days for arte-
riovenous grafts or arteriovenous fistulae (25). Most cases of
infectious arthritis and osteomyelitis in HD patients are most
likely caused by bacteremia (26). Al-Nammari et al. re-
ported that the incidence of microbiologically proven infec-
tious arthritis in HD patients is under 0.5% per year (27).
The majority of bacteremia and infectious osteomyelitis
cases are caused by Gram-positive organisms; Staphylococ-cus aureus and S. epidermidis are the responsible organisms
in approximately 70% of cases (28, 29). Therefore, at first,
we suspected a diagnosis of osteomyelitis caused by bacte-
ria, and the patient was treated with antibiotics. In addition,
considering the location of the lesion, the risk that the infec-
tion might spread throughout the patient’s entire body or
that the arteriovenous fistula might rupture was high. There-
fore, we also performed closure surgery on the arteriovenous
fistula in order to prevent dissemination of the infection.
When an arteriovenous fistula is located adjacent to a lesion
of infectious osteomyelitis, closure of the fistula and recon-
struction of the arteriovenous fistula in the contralateral limb
should be considered.
The number of HD patients is increasing worldwide, in-
cluding in Japan; therefore, we speculate that the incidence
of TB among HD patients will also increase in the future.
Therefore, when HD patients develop infectious osteomyeli-
tis, it is important to determine if the infection is caused by
M. tuberculosis. Furthermore, it is also necessary to perform
a stab culture or a PCR test for M. tuberculosis at an early
stage in patients with infectious osteomyelitis who show a
poor response to antibiotic therapy.
The authors state that they have no Conflict of Interest (COI).
References
1. Hussein MM, Mooij JM, Roujouleh H. Tuberculosis and chronic
renal disease. Semin Dial 16: 38-44, 2003.
2. Segall L, Covic A. Diagnosis of tuberculosis in dialysis patients:

Intern Med 52: 135-139, 2013 DOI: 10.2169/internalmedicine.52.8437
139
current strategy. Clin J Am Soc Nephrol 5: 1114-1122, 2010.
3. Abdelrahman M, Sinha AK, Karkar A. Tuberculosis in end-stage
renal disease patients on hemodialysis. Hemodial Int 10: 360-364,
2006.
4. Dervisoglu E, Yilmaz A, Sengul E. The spectrum of tuberculosis
in dialysis patients. Scand J Infect Dis 38: 1040-1044, 2006.
5. Kayabasi H, Sit D, Kadiroglu AK, Kara IH, Yilmaz ME. The
prevalence and the characteristics of tuberculosis patients undergo-
ing chronic dialysis treatment: experience of a dialysis center in
southeast Turkey. Ren Fail 30: 513-519, 2008.
6. Sen N, Turunc T, Karatasli M, Sezer S, Demiroglu YZ, Oner
Eyuboglu F. Tuberculosis in patients with end-stage renal disease
undergoing dialysis in an endemic region of Turkey. Transplant
Proc 40: 81-84, 2008.
7. Milburn HJ. How should we treat tuberculosis in adult patients
with chronic kidney disease? Key messages from the British Tho-
racic Society Guidelines. Pol Arch Med Wewn 120: 417-422,
2010.
8. Abdelwahab IF, Bianchi S, Martinoli C, Klein M, Hermann G.
Atypical extraspinal musculoskeletal tuberculosis in immunocom-
petent patients, a review. Part I: atypical osteoarticular tuberculosis
and tuberculous osteomyelitis. Can Assoc Radiol J 57: 86-94,
2006.
9. Lazzarini L, Mader JT, Calhoun JH. Osteomyelitis in long bones.
J Bone Joint Surg Am 86-A: 2305-2318, 2004.
10. Salliot C, Allanore Y, Lebrun A, et al. Disseminated extrapulmo-
nary tuberculosis revealed by humeral osteomyelitis with chronic
unremarkable pain. Joint Bone Spine 72: 263-266, 2005.
11. Vallejo JG, Ong LT, Starke JR. Tuberculous osteomyelitis of the
long bones in children. Pediatr Infect Dis J 14: 542-546, 1995.
12. Descamps-Latscha B, Chatenoud L. T cells and B cells in chronic
renal failure. Semin Nephrol 16: 183-191, 1996.
13. Chan TY. Vitamin D deficiency and susceptibility to tuberculosis.
Calcif Tissue Int 66: 476-478, 2000.
14. Christopoulos AI, Diamantopoulos AA, Dimopoulos PA, Gumenos
DS, Barbalias GA. Risk of tuberculosis in dialysis patients: asso-
ciation of tuberculin and 2,4-dinitrochlorobenzene reactivity with
risk of tuberculosis. Int Urol Nephrol 38: 745-751, 2006.
15. Girndt M, Sester U, Sester M, Kaul H, Kohler H. Impaired cellu-
lar immune function in patients with end-stage renal failure.
Nephrol Dial Transplant 14: 2807-2810, 1999.
16. Tzanno-Martins C, Futata E, Jorgetti V, Duarte AJ. Restoration of
impaired T-cell proliferation after parathyroidectomy in hemo-
dialysis patients. Nephron 84: 224-227, 2000.
17. Passalent L, Khan K, Richardson R, Wang J, Dedier H, Gardam
M. Detecting latent tuberculosis infection in hemodialysis patients:
a head-to-head comparison of the T-SPOT.TB test, tuberculin skin
test, and an expert physician panel. Clin J Am Soc Nephrol 2: 68-
73, 2007.
18. Chou KJ, Fang HC, Bai KJ, Hwang SJ, Yang WC, Chung HM.
Tuberculosis in maintenance dialysis patients. Nephron 88: 138-
143, 2001.
19. Burke HE. The pathogenesis of certain forms of extrapulmonary
tuberculosis; spontaneous cold abscesses of the chest wall and
Pott’s disease. Am Rev Tuberc 62: 48-67, 1950.
20. Davidson PT, Horowitz I. Skeletal tuberculosis. A review with pa-
tient presentations and discussion. Am J Med 48: 77-84, 1970.
21. Monach PA, Daily JP, Rodriguez-Herrera G, Solomon DH. Tuber-
culous osteomyelitis presenting as shoulder pain. J Rheumatol 30:
851-856, 2003.
22. Sharma OP. Hypercalcemia in granulomatous disorders: a clinical
review. Curr Opin Pulm Med 6: 442-447, 2000.
23. Versfeld GA, Solomon A. A diagnostic approach to tuberculosis
of bones and joints. J Bone Joint Surg Br 64: 446-449, 1982.
24. Taylor Z, Nolan CM, Blumberg HM. Controlling tuberculosis in
the United States. Recommendations from the American Thoracic
Society, CDC, and the Infectious Diseases Society of America.
MMWR Recomm Rep 54: 1-81, 2005.
25. Lafrance JP, Rahme E, Lelorier J, Iqbal S. Vascular access-related
infections: definitions, incidence rates, and risk factors. Am J Kid-
ney Dis 52: 982-993, 2008.
26. Nicholls A, Edward N, Catto GR. Staphylococcal septicaemia, en-
docarditis, and osteomyelitis in dialysis and renal transplant pa-
tients. Postgrad Med J 56: 642-648, 1980.
27. Al-Nammari SS, Gulati V, Patel R, Bejjanki N, Wright M. Septic
arthritis in haemodialysis patients: a seven-year multi-centre re-
view. J Orthop Surg (Hong Kong) 16: 54-57, 2008.
28. Butterly DW, Schwab SJ. Dialysis access infections. Curr Opin
Nephrol Hypertens 9: 631-635, 2000.
29. Nassar GM, Ayus JC. Infectious complications of the hemodialysis
access. Kidney Int 60: 1-13, 2001.
Ⓒ 2013 The Japanese Society of Internal Medicine
http://www.naika.or.jp/imonline/index.html