Embed Size (px)
Citation preview

University of Groningen
Buruli ulcer in West Africade Zeeuw, Janine
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2016
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):de Zeeuw, J. (2016). Buruli ulcer in West Africa: suffering beyond the wound. [Groningen]: University ofGroningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 19-10-2020

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
7
Introduction on Buruli ulcer - a neglected tropical disease
1
501598-bw-deZeeuw.indd 7 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
8
501598-bw-deZeeuw.indd 8 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
9
Introduction on Buruli ulcer - a neglected tropical disease Codjo, 10 years of age, lives in a remote area in Benin. In this district, Buruli ulcer is highly endemic. Some months ago Codjo fell ill with Buruli ulcer and visited a traditional healer without sufficient result. Some weeks ago he went to a specialized Buruli ulcer treatment center and currently he is treated with antimicrobial therapy. He suffers from painful wound dressing changes and wonders if pain medication can relieve his pain. At this point in time, his physician doubts the effect of the antimicrobial therapy as his lesion has become larger. Codjo his sister suffered from Buruli ulcer last year and struggles with limitations in daily activities such as fetching water from the pump. Moreover she sometimes feels people avoid her, and discourage her from visiting traditional festivals in the village. They both acknowledge that they should have gone to the hospital earlier for medical treatment.
The story of Codjo and his sister touch upon the main themes addressed in this thesis. In this thesis pain related to Buruli ulcer (BU) and practices to identify and relieve pain are addressed, as well as the potential value of neopterin in detecting paradoxical reactions, social disabilities former patients experience and the referral system of BU patients to specialized BU treatment centers. Management of BU patients should include an array of interventions and to address patients’ needs, a perspective in which medical, psychological and social aspects, should be taken into account.
The history of Buruli ulcer BU is categorized by the World Health Organization (WHO) as one of the neglected tropical diseases [1]. It is the third most common mycobacterial infection in immuno-competent humans globally, after tuberculosis and leprosy [2]. At the end of the nineteenth century, BU was first described by Albert Cook, describing skin ulcers consistent with BU. In 1948, BU was related to its causative agent, Mycobacterium ulcerans, by Peter MacCallum and his colleagues in Australia [3, 4]. In the 1960s, large numbers of cases were described in the Buruli County, near the Nile River in Uganda, giving rise to the name BU [5]. Over the past decade, a growing number of cases have emerged [6]. To stress the importance of BU control and to understand this ‘mysterious’ condition, the WHO organized the first international meeting on BU in Côte d’Ivoire in July 1998. This resulted in the Yamoussoukro Declaration on BU [7]. In May 2004, a resolution was adopted on increasing surveillance and control of BU and member states were encouraged to develop tools to diagnose, treat and prevent BU [8]. Buruli ulcer prevalence Today, BU has been reported in over 30 countries worldwide, mainly with humid tropical and subtropical climates. Although the number of cases has dropped [6], in West Africa still high number of cases are reported, especially in Côte d’Ivoire, Benin and Ghana [9]. In Benin, prevalence rates between 5.4 and 60.7 per 10.000 inhabitants have been reported [10], and in Ghana, prevalence rates have fluctuated between 2.0 and 15.0 per 10.000 inhabitants [11]. BU affects all ages, but especially children are likely to become infected [12].
Introduction on Buruli ulcer - a neglected tropical disease
501598-bw-deZeeuw.indd 9 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
10
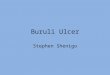
Causative agent, clinical manifestation and treatment BU is caused by infection with Mycobacterium ulcerans, an environmental bacterium, producing mycolactone, a toxin responsible for the extensive tissue necrosis and immunosuppression [13]. The cytotoxicity of mycolactone towards the immune cells causes immunosuppression, and eventually the pathogenicity [13]. Mycolactone molecules interfere with the cytoskeleton of immune competent and other cells by attacking the Wiskott-Aldrich proteins [14-16]. Infection usually starts as a nodule (Figure 1), or a plaque (Figure 2), sometimes accompanied with edema, developing into deep ulcers (Figure 3) with typical undermined edges surrounding the ulcer in later stages [17]. The treatment of BU entails antimicrobial treatment (8 weeks of oral rifampicin and intramuscular streptomycin), supplemented with surgical intervention if required, wound care, and Prevention of Disability [18, 19]. Effective antimicrobial therapy became available in 2005, and has shown being safe and effective to manage small lesions (< 10 cm, cross-sectional diameter) [20].
Figure 1, a nodule
Figure 2, plaque
Figure 3, an ulcer
1
501598-bw-deZeeuw.indd 10 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
11
Pain associated with wound care treatmentIn literature BU is described as a painless condition, despite the large ulcers [21-23]. Previous studies suggested analgesia is caused by mycolactone either damaging nerves or causing hyperpolarisation of neurons [21, 23]. In contrast studies described patients reporting painful ulcers [24-26], and clinical observations indicated painful wound dressings for at least some of the patients affected by BU. Especially the removal of the soiled dressing and cleaning of the wound seemed to be painful. Pain during wound care dressings negatively influences the healing process [27] and might negatively shape people’s ideas regarding treatment, possibly impacting health care seeking behaviour. Wound care is a major aspect of BU treatment and is performed varying from daily to thrice a week by a trained nurse, either in a hospital or in a health care center [28]. The wound dressing procedure consists of three stages, firstly, removal of the soiled dressing, secondly, cleaning of the wound with normal saline and if required debridement, and lastly, redressing of the wound. Wound care is essential for protection to enable healing of the wound; and it potentially reduces environmental infections of the wound and hospitalization duration [29]. Pain can be distinguished in background pain, breakthrough pain or procedural pain. The latter is pain associated with invasive procedures, wound cleansings and dressings, and physiotherapy [30]. Clinical features of pain involve: location, intensity, duration and quality [31]. The International Association for the Study of Pain defines pain as: ‘An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.’
The function of pain is to protect the body against tissue damage. Nociceptive stimulation activates free nerve endings initiating a cascade of events such as the release of various substances inducing an immune response [32]. The afferent A-δ and C-fibers transmit nociceptive signals to the secondary neurons, located in zones of the dorsal horn, the lamina of the spinal cord. These secondary neurons further transmit signals to thalamic nociceptive neurons and specific nuclei of the brainstem using different pathways. In the cortex the nociceptive stimulus is perceived [32]. Pain is a personal experience covering the sensation of pain along with an automatic reactive response and the association with cognitive and psychological processes. The interpretation of pain is influenced by former experiences, emotional, somatic, and cognitive factors. For example, it has been discribed that anticipatory fear and anxiety increases pain experiences [33], and cultural beliefs might shape response behaviours and attitudes on pain [34], and might affect pain perception determining interpretation of pain and the reaction towards it [35]. A common reaction found in various cultures is the denial of physical pain and the stoic reaction towards pain [36-39]. Most commonly used approaches to measure pain are self report; observational or behavioral; and psychological [40]. Ideally, self-report measures are used to obtain pain measures to capture the subjectivity of the pain experience not directly observable to others [40]. Among children, faces scales are generally preferred, of which the Faces Pain Scale-Revised, the Oucher pain scale, and Wong-Baker Faces Pain Rating Scale (WBS) have been most widely used and extensively validated [41]. in this thesis the WBS was selected, as health care professionals involved in BU treatment centers in Ghana favoured this instrument. The WBS has undergone extensive psychometric testing of the validity and reliability, and children reported no difficulties with rating their pain using this instrument [41].
Introduction on Buruli ulcer - a neglected tropical disease
501598-bw-deZeeuw.indd 11 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
12
Current pain practices in Buruli ulcer treatmentGiven the fact that BU has always been described as a painless condition, little is known on the practices regarding pain in specialized treatment centers. In general, pain is undertreated in poor-resource countries [42] and the WHO has stressed the need to integrate pain treatment in daily practice using guidelines for pain management [43]. In this thesis, pain management and pain practices are used synonymously and refer to the assessment and treatment of pain, including pharmaceutical and non- pharmaceutical aspects. One of the most adhered guideline in prescribing pain medication is the WHO pain ladder consisting of three steps of drugs with increasing analgesic effects [44] recommended for pain relief in wound pain [45]. Previous studies show that perceptions, attitudes and beliefs of health professionals are important in pain practices. A review on challenges in effective pediatric pain management in sub-Saharan Africa showed barriers related to the availability of- and access to analgesics, a lack of education and information among various health workers, and legal barriers such as regulatory restrictions on opiates [46]. Furthermore, attitudinal barriers and cultural differences between patients and health professionals play a role, as was illustrated in a study among 28 emergency department nurses from Central Africa. The study showed that a fear of addiction to opioids, the view that taking medication for pain is a sign of weakness, and the belief that pain relief could interfere with healing, influenced pain management [47]. Paradoxical reactionsPatients indicated to experience pain on the lesion site just before and after ulceration [26]. Concurrent a paradoxical reaction, which is a sudden deterioration after initial improvement in response to antimicrobial treatment might have occurred [26, 48, 49]. Paradoxical reactions have been associated with tuberculosis [50-52], and reversal reactions with leprosy [53]. Paradoxical reactions are proposed to occur due to killing of the organism along with a reduction in mycolactone which allows an intense immunological response [49]. Such a reaction can easily be mistaken for treatment failure unnecessarily leaving medical doctors with the decision to perform surgical intervention to remove necrotic tissue and the bacilli. Neopterin is an indicator of activated cellular immunity [54] and appeared to have promising value to function as a biomarker to monitor leprosy patients during treatment, along with the occurrence of paradoxical reactions [55, 56]. Neopterin is one of the cytokines secreted by monocytes, macrophages, dendritic cells, under the control of T-lymphocytes and Natural killer cells releasing interferon-γ and tumor necrosis factor [54]. International Classification of Functioning and HealthThe majority of BU patients still report with advanced disease stages to the specialised treatment centers [57] and are more likely to develop disabilities [58] (Figure 4). Historically, disabilities were expressed in terms of problems at body levels using a ‘medical lense’. Over the past years the emphasis has shifted from medical aspects to more complex forms of disabilities using a ‘social lens’, acknowledging the crucial role of society.
1
501598-bw-deZeeuw.indd 12 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
13
Impairment
Contextual factors
Functioning
RestrictionsLimitations
Health Condition
Body functions & Structures
Activity Participation
Environmental factors Personal factors
Figure 4, a disability
Disabilities might be envisioned using the International Classification of Function, Disability and Health (ICF) launched in 2001 by the WHO building on an existing framework. Worldwide, the model serves to ‘provide a scientific basis for understanding and studying health and health-related states, outcomes and determinants [59]. This model is widely applied and uses a biopsychosocial approach, meaning that it integrates a medical and social model. The ICF consists of three main components which are a health condition, functioning and contextual factors, graphically represented in Figure 5. In this model functioning in society is an interaction between a health condition and contextual factors. Functioning consists of three different interrelated components, namely body functions & structures, activity, and participation [59, 60]. Body functions and structures imply the physiological functions and anatomical parts of the body. Activity refers to the tasks or actions performed by an individual while participation means to what extent an individual is involved in certain life situations. The contextual factors include environmental and personal factors. Environmental factors refer to the environment an individual lives in such as the physical and social environment whereas, personal factors entail individual characteristics such as sex, age, profession, social status, and education [59, 60].
Figure 5, International Classification of Functioning, Disability and Health
Introduction on Buruli ulcer - a neglected tropical disease
501598-bw-deZeeuw.indd 13 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
14
A health condition relates to the presence of a disease, disorder or injury which might negatively impact functioning and causes disabilities. The definition of disabilities as used in the ICF adhered to in this thesis is: ‘a difficulty in functioning at the body, person or societal level in one or more life domains, as experience by an individual with a health condition in interaction with contextual factors’[61]. A disability might occur at body level (impairments), personal level (activity limitations), and at social level (participation restrictions). Impairments are defined as ‘problems in body function or structure such as significant deviation or loss’, activity limitations are defined as ‘difficulties an individual may have in executing activities’, and participation restrictions are defined as ‘problems an individual may experience in involvement in life situations’ [59]. In other words, a person facing a health condition is facing a reduced range of motion or sensory loss, and otherwise can experience difficulties in walking, or is affected in attending social gatherings in the community.
Buruli ulcer related disabilitiesWhen looking at BU related disabilities, studies have described contractures, deformities, and limited movements of joints as a consequence of soft tissue destruction, including tendons, and joints. In Ghana, 27% of the former patients, experienced a reduced range of motion and 22% encountered a BU related functional limitation in daily life [62]. Disabilities at the personal level have also been described in Benin as functional limitations which remained a major problem for almost half of the treated patients irrespective of treatment [58]. More recently, a large cohort study showed that in former afflicted patients, 22% had permanent functional problems [63]. When looking at the stigma attached to BU, it has been described that cultural beliefs on the mode of transmission and not having proper treatment are the most important elements of stigma related to BU [64, 65]. Stigma attached to a health condition is considered to be as devastating as the disease per see [66] and has major implications on psychosocial aspects of life [67] including on participation in society [68].
Participation restrictionsParticipation restrictions occur in nine life domains, namely learning and applying knowledge, general tasks and demands, communication, mobility, self-care, domestic life, interpersonal interactions and relationships, major life areas, and community, social and civic life [60]. In Ghana, people felt restricted in employment, education and training, mobility, and helping and supporting other people [69]. Furthermore, in India, restrictions were predominantly encountered restrictions related to employment [70]. In Nigeria, most reported restrictions were related to employment, domestic life and interpersonal relations [71]. Visible signs of a health condition, severity of impairments, but also severity of activity limitations might aggravate the severity of participation restrictions [72, 73]. The confusion on conceptualisation of participation restrictions remains an obstacle [74, 75] resulting in numerous instruments that have been developed [76-79]. When searching for an instrument to assess participation restrictions suitable for the West African context, the Participation Scale (P-scale) (appendix 1) showed most promising value [80]. The P-scale was developed and validated among people with disability related conditions or other stigmatising conditions aged 15 years or older in Brazil, Nepal and India [80]. To date, the P-scale has been predominantly used in low-and middle income countries [70-73, 81-89], shows acceptable
Introduction on Buruli ulcer - a neglected tropical disease1

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
15
psychometric properties [70, 72, 80, 88], is generic, and is relatively easy to administrate by local health care personnel [80]. It is recommended to explore the quality of P-scale in a new cultural context. In literature, several definitions are given for various concepts in psychometric properties; in this thesis the definitions as proposed in de Vet et al. (2011) are used [90].
Buruli ulcer controlIn order to reduce disabilities, the mainstay of BU control entails early case detection by active case finding and health education, and early medical treatment. The WHO has developed a system to classify lesion sizes which is commonly used to measure early disease presentation. This system classifies lesions as category I: lesions cross-sectional diameter of less than 5 cm; as category II: lesions of 5-15 cm and category III: lesions of >15 cm; category III also includes lesions on important sites (for example eyes) and multiple lesions. Despite extensive efforts, only 32 % of the patients report to the hospital with Cat I lesions. There are suggestions that community health volunteers can play a vital role in early case detection [91, 92] but further exploration is required [93]. Currently, key activities of community health workers are to actively screen community members in households, schools, and churches and to refer suspected cases.
Introduction on Buruli ulcer - a neglected tropical disease
501598-bw-deZeeuw.indd 15 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
16
Thesis outline The aim of the thesis is to explore pain related to BU and current pain practices, social disabiity the psychosocial impact of BU, the value of neopterin to detect paradoxical reactions and the role of various actors in BU control. In the patient history, the story of Codjo reflects the problem that patients might experience pain during wound dressing changes and chapter 2 describes pain experiences during wound care treatment. Furthermore it is unclear how current pain management is organised in specialized treatment centers as indicated by the story of Codjo; Codjo suffers from painful wound dressing changes and wonders if pain medication can relieve his pain. Chapter 3 provides insights in current pain management in BU treatment and chapter 4 addresses the topics discussed during a multidisciplinary workshop on pain management and proposes a guide to identify and treat pain. Another topic addressed in this thesis is the detection of paradoxical reactions as physicians might perform surgery while a patient shows a paradoxical reaction, requiring a biomarker that could aid in decision making regarding surgery. Unnecessary surgery might put people at risk for other infections and development of disabilities. As described in the story of Codjo, Codjo his physician doubts the effect of the antimicrobial therapy as his lesion has become larger. Chapter 5 provides insight in the potential value of neopterin to detect paradoxical reactions. Furthermore this thesis addresses social participation restrictions among former BU patients after medical treatment. When looking at the story of Codjo his sister as described in the casus it is possible that patients might experience participation restrictions in social life. Codjo his sister suffered from BU last year and struggles with limitations in daily activities such as fetching water from the pump. Moreover she sometimes feels people avoid her, and discourage her from visiting traditional festivals in the village. Chapter 6 explores the proportion of former BU patients experiencing participation restrictions and provides insights in predictors of these restrictions. Chapter 7 explores the quality of the P-scale in a new cultural context describing the analysis regarding psychometric properties. Finally, detecting patients with early lesions, and treatment is the mainstay of BU control with the aim to reduce morbidities. This is also described in the story of Codjo and his sister; they both acknowledge that they should have gone to the hospital earlier for medical treatment. Chapter 8 explores the role of various actors in referral of patients to BU treatment centers in Benin.
1
501598-bw-deZeeuw.indd 16 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
17
Appendix 1: The Participation Scale (v.6.0) (van Brakel et al. 2006)
No
NO
Participation Scale
Not
spec
ified
Yes
Som
etim
es
No
Don
’t w
ant t
o
No
prob
lem
Smal
l
Med
ium
Larg
e
SCO
RE
1 Do you have equal opportunity as your peers to find work?
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
2 Do you work as hard as your peers do? (same hours, type of work etc)
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
3 Do you contribute to the household economically in a similar way to your peers?
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
4 Do you make visits outside your village / neighbourhood as much as your peers do? (except for treatment) e.g. bazaars*, markets
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
5 Do you take part in major festivals and rituals as your peers do? (e.g. weddings, funerals, religious festivals)
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
6 Do you take as much part in casual recreational / social activities as do your peers? (e.g. sports, chat, meetings)
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
Appendix 1: The Participation Scale (v.6.0) (van Brakel et al. 2006)
Introduction on Buruli ulcer - a neglected tropical disease
501598-bw-deZeeuw.indd 17 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
18
1
No
NO
Participation Scale
Not
spec
ified
Yes
Som
etim
es
No
Don
’t w
ant t
o
No
prob
lem
Smal
l
Med
ium
Larg
e
SCO
RE
7 Are you as socially active as your peers are? (e.g. in religious / community affairs)
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
8 Do you have the same respect in the community as your peers?
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
9 Do you have opportunity to take care of yourself (appearance, nutrition, health, etc) as well as your peers?
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
10 Do you have the same opportunities as your peers to start or maintain a long-term relationship with a life partner?
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
11 Do you visit other people in the community as often as other people do?
0 0
[if sometimes or no] How big a problem is it for you?
1 2 3 5
12 Do you move around inside and outside the house and around the village / neighbourhood just as other people do?
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
13 In your village / neighbourhood, do you visit public places as often as other people do? (e.g. schools, shops, offices, market and tea/coffee shops*)
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
501598-bw-deZeeuw.indd 18 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
19
Introduction on Buruli ulcer - a neglected tropical diseaseN
o
NO
Participation Scale
Not
spec
ified
Yes
Som
etim
es
No
Don
’t w
ant t
o
No
prob
lem
Smal
l
Med
ium
Larg
e
SCO
RE
14 In your home, do you do household work? 0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
15 In family discussions, does your opinion count? 0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
16 Do you help other people? (e.g. neighbours, friends or relatives)
0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
17 Are you comfortable meeting new people? 0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
18 Do you feel confident to try to learn new things? 0 0
[if sometimes or no] How big a problem is it to you?
1 2 3 5
* deleted
Comment: TOTAL:
Name:________________________________________
Age:__________ Gender:__________
Interviewer:____________________________________
Date of interview:___/___/_____
501598-bw-deZeeuw.indd 19 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
20
References World Health Organization. (2013) World health assembly adopts resolution on all 17 neglected tropical diseases. Geneva: World Health Organization. Available: http://www.who.int/neglected_diseases/mediacentre/WHA_66.12_Eng.pdf?ua=1. Accessed 27 November 2014. van der Werf TS, Stienstra Y, Johnson RC, Phillips R, AdjeiO, et al. (2005) Mycobacterium ulcerans disease. Bull World Health Organ 83(10): 785-791.MacCallum P. (1948) A new mycobacterial infection in man. I. clinical aspects. J Pathol Bacteriol 60(1): 93-122.Ward DE. (1970) Buruli ulcer. Br Med J 3(5718): 346.Uganda Buruli Group. (1970) Clinical features and treatment of pre-ulcerative Buruli ulesions (Mycobacterium ulcerans infection). British Medical Journal 2(5706): 390-393.World Health Organization. (2013) Buruli ulcer. number of new cases of Buruli ulcer reported. Available at: http://apps.who.int/neglected_diseases/ntddata/buruli/buruli.html. Accessed 9 October, 2014. van der Graaf WT, Scherpbier RW, van der Werf TS. (1999) Buruli ulcer (Mycobacterium ulcerans infection); report from the international congress in Yamoussoukro, Ivory Coast. Ned Tijdschr Geneeskd 143(6): 312-316.World Health Organization. (2004) Resolution WHA57. 1 surveillance and control of Mycobacterium ulcerans disease (Buruli ulcer). Fifty Seventh World Health Assembly :17- 22.World Health Organization. (2013) Number of new cases of Buruli ulcer reported by country (per year). Available at: http://apps.who.int/gho/data/node.main.A1631?lang=en.Accessed 7 October, 2014. Sopoh GE, Johnson RC, Anagonou SY, Barogui YT, Dossou AD, et al. (2011) Buruli ulcer prevalence and altitude, Benin. Emerging Infectious Diseases 17(1): 153-154.Amofah G, Bonsu F, Tetteh C, Okrah J, Asamoa K, et al. (2002) Buruli ulcer in Ghana: results of a national case search. Emerg Infect Dis 8(2): 167-170.Merritt RW, Walker ED, Small PL, Wallace JR, Johnson PD, et al. (2010) Ecology and transmission of Buruli ulcer disease: a systematic review. PLoS Negl Trop Dis 4(12): e911.Silva MT, Portaels F, Pedrosa J. (2009) Pathogeneticmechanisms of the intracellular parasite Mycobacterium ulcerans leading to Buruli ulcer. Lancet Infect Dis 9(11): 699-710.Chany AC, Casarotto V, Schmitt M, Tarnus C, Guenin-Mace L, et al. (2011) A diverted total synthesis of mycolactone analogues: an insight into Buruli ulcer toxins. Chemistry 17(51): 14413-14419.Chany AC, Veyron-Churlet R, Tresse C, Mayau V, Casarotto V, et al. (2014) Synthetic variants of mycolactone bind and activate Wiskott-Aldrich syndrome proteins. J Med Chem 57(17): 7382-7395.Guenin-Mace L, Carrette F, Asperti-Boursin F, Le Bon A, Caleechurn L, et al. (2011) Mycolactone impairs T cell homing by suppressing microRNA control of L-selectin expression. Proc Natl Acad Sci U S A 108(31): 12833-12838.Johnson PD, Stinear T, Small PL, Pluschke G, Merritt RW, et al. (2005) Buruli ulcer (M. ulcerans infection): New insights, new hope for disease control. PLoS Med 2(4): e108.Lehman L, Simonet V, Saunderson P, Agbenorku P. (2006) Buruli ulcer. Prevention of disability (POD). Geneva: World Health Organization.Simonet V. (2008) Prevention of disability in Buruli ulcer: Basic rehabilitation. practical field guide. Geneva: World Health Organization.Nienhuis WA, Stienstra Y, Thompson WA, Awuah PC, Abass KM, et al. (2010) Antimicrobial treatment for early, limited Mycobacterium ulcerans infection: A randomized controlled trial. Lancet 375(9715): 664-672.Goto M, Nakanaga K, Aung T, Hamada T, Yamada N, et al. (2006) Nerve damage in Mycobacterium ulcerans-infected mice: probable cause of painlessness in Buruli ulcer. Am J Pathol 168(3): 805-811.
1
2
3
45
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
1
501598-bw-deZeeuw.indd 20 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
21
En J, Goto M, Nakanaga K, Higashi M, Ishii N, et al. (2008) Mycolactone is responsible for the painlessness of Mycobacterium ulcerans infection (Buruli ulcer) in a murine study. Infect Immun 76(5): 2002-2007.Marion E, Song OR, Christophe T, Babonneau J, FenisteinD, et al. (2014) Mycobacterial toxin induces analgesia in Buruli ulcer by targeting the angiotensin pathways. Cell 157(7): 1565-1576.Ackumey MM, Gyapong M, Pappoe M, Weiss MG. (2011) Help-seeking for pre-ulcer and ulcer conditions of Mycobacterium ulcerans disease (Buruli ulcer) in Ghana. Am J Trop Med Hyg 85(6): 1106-1113.Onoe H, Yotsu RR, Nakanaga K, Hoshino Y, Ishii N, et al. (2012) Buruli ulcer accompanied by pain in a Japanese patient. J Dermatol 39(10): 869-870.Nienhuis WA, Stienstra Y, Abass KM, Tuah W, Thompson WA, et al. (2012) Paradoxical responses after start of antimicrobial treatment in Mycobacterium ulcerans infection. Clin Infect Dis 54(4): 519-526.Woo KY. (2010) Wound-related pain: Anxiety, stress and wound healing. Wounds 6(4): 92- 98.Velding K, Klis SA, Abass KM, Tuah W, Stienstra Y, et al. (2014) Wound care in Buruli ulcer disease in Ghana and Benin. Am J Trop Med Hyg 91(2): 313-318.Sen S, Greenhalgh D, Palmieri T. (2013) Review of burn research for the year 2011. J Burn Care Res 34(2): 211-218.Faucher L, Furukawa K. (2006) Practice guidelines for the management of pain. J Burn Care Res 27(5): 659-668.Swieboda P, Filip R, Prystupa A, Drozd M. (2013) Assessment of pain: types, mechanism and treatment. Ann Agric Environ Med Spec no. 1: 2-7.Marchand S. (2008) The physiology of pain mechanisms: from the periphery to the brain. Rheum Dis Clin North Am 34(2): 285-309.Tracey I, Mantyh PW. (2007) The cerebral signature for pain perception and its modulation. Neuron 55(3): 377-391.Zborowski M. (1952) Cultural components in responses to pain. Journal of Social Issues 8(14): 16-30.Rahim-Williams B, Riley JL,3rd, Williams AK, FillingimRB. (2012) A quantitative review of ethnic group differences in experimental pain response: do biology, psychology, and culture matter? Pain Med 13(4): 522-540.Lovering S. (2006) Cultural attitudes and beliefs about pain. J Transcult Nurs 17(4): 389-395.Latimer M, Finley GA, Rudderham S, Inglis S, Francis J, et al. (2014) Expression of pain among Mi’kmaq children in one Atlantic Canadian community: A qualitative study. CMAJ Open 2(3): E133-8.Sargent C. (1984) Between death and shame: Dimensions of pain in Bariba culture. Soc Sci Med 19(12): 1299-1304.Beck SL. (2000) An ethnographic study of factors influencing cancer pain management in South Africa. Cancer Nurs 23(2): 91-9; quiz 99-100.von Baeyer CL, Spagrud LJ. (2007) Systematic review of observational (behavioral) measures of pain for children and adolescents aged 3 to 18 years. Pain 127(1-2): 140-150.Tomlinson D, von Baeyer CL, Stinson JN, Sung L. (2010) A systematic review of faces scales for the self-report of pain intensity in children. Pediatrics 126(5): e1168-98.Brennan F, Carr DB, Cousins M. (2007) Pain management: a fundamental human right. Anesth Analg 105(1): 205-221.World Health Organization. (2007) Normative guidelines on pain management. report of a delphi study to determine the need for guidelines and to identify the number and topics of guidelines that should be developed by WHO. Geneva: World Health Organization.World Health Organization. (1986) Cancer pain relief. Geneva: World Health Organization.Brolmann FE, Vermeulen H, Go P, Ubbink D. (2013) Guideline ‘wound care’: Recommendations for 5 challenging areas. Ned Tijdschr Geneeskd 157(29): A6086.
22
23
24
25
26
2728
29
30
31
32
33
3435
3637
38
39
40
41
42
43
4445
Introduction on Buruli ulcer - a neglected tropical disease
501598-bw-deZeeuw.indd 21 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
22
Albertyn R, Rode H, Millar AJ, Thomas J. (2009) Challenges associated with pediatric pain management in sub-Saharan Africa. Int J Surg 7(2): 91-93.Rampanjato RM, Florence M, Patrick NC, Finucane BT.(2007) Factors influencing pain management by nurses in emergency departments in Central Africa. Emerg Med J 24(7): 475- 476.Ruf MT, Chauty A, Adeye A, Ardant MF, Koussemou H, et al. (2011) Secondary Buruli ulcer skin lesions emerging several months after completion of chemotherapy: Paradoxical reaction or evidence for immune protection? PLoS NeglTrop Dis 5(8): e1252.O’Brien DP, Robson M, Friedman ND, Walton A, McDonald A, et al. (2013) Incidence, clinical spectrum, diagnostic features, treatment and predictors of paradoxical reactions during antibiotic treatment of Mycobacterium ulcerans infections. BMC Infect Dis 13: 416-2334-13- 416.Breen RA, Smith CJ, Bettinson H, Dart S, Bannister B, et al. (2004) Paradoxical reactions during tuberculosis treatment in patients with and without HIV co-infection. Thorax 59(8): 704-707.Hawkey CR, Yap T, Pereira J, Moore DA, Davidson RN, et al. (2005) Characterization and management of paradoxical upgrading reactions in HIV-uninfected patients with lymph node tuberculosis. Clin Infect Dis 40(9): 1368-1371.Carvalho AC, De Iaco G, Saleri N, Pini A, Capone S, et al. (2006) Paradoxical reaction during tuberculosis treatment in HIV-seronegative patients. Clin Infect Dis 42(6): 893-895.Kamath S, Vaccaro SA, Rea TH, Ochoa MT. (2014) Recognizing and managing the immunologic reactions in leprosy. J Am Acad Dermatol 71(4): 795-803.Hoffmann G, Wirleitner B, Fuchs D. (2003) Potential role of immune system activation- associated production of neopterin derivatives in humans. Inflamm Res 52(8): 313-321.Hamerlinck FF, Klatser PR, Walsh DS, Bos JD, Walsh GP, et al. (1999) Serum neopterin as a marker for reactional states in leprosy. FEMS Immunol Med Microbiol 24(4): 405-409.Faber WR, Iyer AM, Fajardo TT, Dekker T, Villahermosa LG, et al. (2004) Serial measurement of serum cytokines, cytokine receptors and neopterin in leprosy patients with reversal reactions. Lepr Rev 75(3): 274-281.World Health Organization. (2015) Buruli ulcer. (Mycobacterium ulcerans infection).Barogui Y, Johnson RC, van der Werf TS, Sopoh G, DossouA, et al. (2009) Functional limitations after surgical or antibiotic treatment for Buruli ulcer in Benin. Am J Trop Med Hyg 81(1): 82-87.World Health Organization. (2001) International classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization. World Health Organization. (2002) Towards a common language for Functioning, Disability and Health; ICF.Geneva: World Health Organization.Leonardi M, Bickenbach J, Ustun TB, Kostanjsek N, Chatterji S. (2006) The definition of disability: what is in a name? Lancet 368(9543): 1219-1221.Schunk M, Thompson W, Klutse E, Nitschke J, Opare-Asamoah K, et al. (2009) Outcome of patients with Buruliulcer after surgical treatment with or without antimycobacterial treatment in Ghana. Am J Trop Med Hyg 81(1): 75-81.Vincent QB, Ardant MF, Adeye A, Goundote A, Saint-Andre JP, et al. (2014) Clinical epidemiology of laboratory-confirmed Buruli ulcer in Benin: a cohort study. Lancet Glob Health 2(7): e422-30.Stienstra Y, van der Graaf WT, Asamoa K, van der WerfTS. (2002) Beliefs and attitudes toward Buruli ulcer in Ghana. Am J Trop Med Hyg 67(2): 207-213.Mulder AA, Boerma RP, Barogui Y, Zinsou C, Johnson RC, et al. (2008) Healthcare seeking behaviour for Buruli ulcer in Benin: A model to capture therapy choice of patients and healthy community members. Trans R Soc Trop Med Hyg102(9): 912-920.
46
47
48
49
50
51
52
53
54
55
56
5758
59
60
61
62
63
64
65
1
501598-bw-deZeeuw.indd 22 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
23
Mak WW, Mo PK, Cheung RY, Woo J, Cheung FM, et al. (2006) Comparative stigma of HIV/AIDS, SARS, and tuberculosis in Hong Kong. Soc Sci Med 63(7): 1912-1922.Van Brakel WH. (2006) Measuring health-related stigma-a literature review. Psychol Health Med 11(3): 307-334.Weiss MG. (2008) Stigma and the social burden of neglected tropical diseases. PLoS Negl Trop Dis 2(5): e237.Amosun SL, Nyante GG, Wiredu EK. (2013) Perceived and experienced restrictions in participation and autonomy among adult survivors of stroke in Ghana. Afr Health Sci 13(1): 24-31.Stevelink SA, van Brakel WH, Augustine V. (2011) Stigma and social participation in Southern India: differences and commonalities among persons affected by leprosy and persons living with HIV/AIDS. Psychol Health Med : 1-13.Ebenso B, Fashona A, Ayuba M, Idah M, Adeyemi G, et al. (2007) Impact of socio-economic rehabilitation on leprosy stigma in Northern Nigeria: findings of a retrospective study. Asia Pacific Disability Rehabilitation Journal 18(2): 98-119.Rensen C, Bandyopadhyay S, Gopal PK, Van Brakel WH. (2011) Measuring leprosy-related stigma - a pilot study to validate a toolkit of instruments. Disabil Rehabil 33(9): 711-719.van Brakel WH, Sihombing B, Djarir H, Beise K, Kusumawardhani L, et al. (2012) Disability in people affected by leprosy: the role of impairment, activity, social participation, stigma and discrimination. Glob Health Action 5: Epub 2012 Jul 20.Whiteneck G, Dijkers MP. (2009) Difficult to measure constructs: Conceptual and methodological issues concerning participation and environmental factors. Arch PhysMed Rehabil 90(11 SUPPL. 1): S22-S35.Chang FH, Coster WJ. (2014) Conceptualizing the construct of participation in adults with disabilities. Arch Phys Med Rehabil 95(9): 1791-1798.Whiteneck GG. (2010) Issues affecting the selection of participation measurement in outcomes research and clinical trials. Arch Phys Med Rehabil 91(9 SUPPL.): S54-S59.Magasi S, Post MW. (2010) A comparative review of contemporary participation measures’ psychometric properties and content coverage. Arch Phys Med Rehabil 91(9 Suppl): S17-28.Stevelink SA, van Brakel WH. (2013) The cross-cultural equivalence of participation instruments: a systematic review. Disabil Rehabil 35(15): 1256-1268.Rainey L, van Nispen R, van der Zee C, van Rens G. (2014) Measurement properties of questionnaires assessing participation in children and adolescents with a disability: a systematic review. Qual Life Res 23(10): 2793-2808.Van Brakel WH, Anderson AM, Mutatkar RK, Bakirtzief Z, Nicholls PG, et al. (2006) The Participation Scale: measuring a key concept in public health. Disabil Rehabil28(4): 193-203.Nicholls PG, Bakirtzief Z, Van Brakel WH, Das-PattanayaRK, Raju MS, et al. (2005) Risk factors for participation restriction in leprosy and development of a screening tool to identify individuals at risk. Lepr Rev 76(4): 305-315.Cross H, Choudhary R. (2005) STEP: An intervention to address the issue of stigma related to leprosy in Southern Nepal. Lepr Rev 76(4): 316-324.Brouwers C, van Brakel WH, Cornielje H, Pokhrel P, Dhakal KP, et al. (2011) Quality of life, perceived stigma, activity and participation of people with leprosy-related disabilities in South-East Nepal. Disability, CBR and Inclusive Development 22(1).Ebenso B, Idah M, Anyor T, Opakunmi F. (2010) Lessons from the evolution of a CBR programme for people affected by leprosy in Northern Nigeria. Lepr Rev 81(4): 318-331.
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
Introduction on Buruli ulcer - a neglected tropical disease
501598-bw-deZeeuw.indd 23 05-01-16 14:30

501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw501598-L-bw-deZeeuw
24
1
Nardi SM, Paschoal VD, Zanetta DM. (2011) Social participation of people affected by leprosy after discontinuation of multidrug therapy. Lepr Rev 82(1): 55-64.Stevelink SA, Hoekstra T, Nardi SM, van der Zee CH, Banstola N, et al. (2012) Development and structural validation of a shortened version of the Participation Scale. Disabil Rehabil; 34(19):1596-607.Kelders R, van Brakel W, Beise K, Irwanto. (2012) Testing and validating a simplified scale to measure social participation of people with disabilities in Indonesia. Disabil Rehabil 34(8): 638-646.Stevelink SA, Terwee CB, Banstola N, van Brakel WH. (2013) Testing the psychometric properties of the Participation Scale in Eastern Nepal. Qual Life Res 22(1): 137-144.van Veen NH, Hemo DA, Bowers RL, Pahan D, Negrini JF, et al. (2011) Evaluation of activity limitation and social participation, and the effects of reconstructive surgery in people with disability due to leprosy: a prospective cohort study. Disabil Rehabil 33(8): 667-674.de Vet HCW, Terwee CB, Mokkink LB, Knol DL. (2011) Measurement in medicine: a practical guide. Cambridge: Cambridge University Press.Vouking MZ, Takougang I, Mbam LM, Mbuagbaw L, Tadenfok CN, et al. (2013) The contribution of community health workers to the control of Buruli ulcer in the Ngoantet area, Cameroon. Pan Afr Med J 16: 63.Abass KM, van der Werf TS, Phillips RO, Sarfo FS, AbotsiJ, et al. (2015) Buruli ulcer control in a highly endemic district in Ghana: role of community-based surveillance volunteers. Am J Trop Med Hyg 92(1): 115-117.Vouking MZ, Tamo VC, Mbuagbaw L. (2013) The impact of community health workers (CHWs) on Buruli ulcer in sub-Saharan Africa: A systematic review. Pan Afr Med J 15: 19.
85
86
87
48
89
90
91
92
93
501598-bw-deZeeuw.indd 24 05-01-16 14:30