Embed Size (px)
Citation preview

Upper Extremity Upper Extremity TraumaTrauma

2
How do fractures heal?

3
Fracture healing
Why do fractures unite?
Because the bone is broken!

4
Healing cascade: indirect healing Inflammation 0 – 5 days
– Haematoma– Necrotic material – Phagocytosis
Repair: 5 – 42 days– Granulation tissue– Acid environment– Periosteum – osteogenic
cells– Cortical osteoclasis
Remodelling– years

5
Healing cascade
Late repair:
Fibrous tissue replaced by
cartilage
Endochondral ossification
Periosteal healing »
membranous ossification

6
What is the difference between direct and indirect
bone healing?

7
Indirect healing – healing by Callus
Unstable Callus stabilises #
Direct healing between cortices

8
Direct bone healing – the response to rigid fixation Only occurs in
absolute stability of the fracture
Does not involve callus formation
Requires good blood supply

9
What are the aims of fracture treatment?

10
AIMS OF FRACTURE TREATMENT
Restore the patient to optimal functional state
Prevent fracture and soft-tissue complications
Get the fracture to heal, and in a position which will produce optimal functional recovery
Rehabilitate the patient as early as possible

11
What factors effect fracture healing?

12
FACTORS AFFECTING FRACTURE HEALING
The energy transfer of the injury
The tissue response– Two bone ends in opposition or compressed– Micro-movement or no movement– Blood Supply (scaphoid, talus, femoral and humeral
head)– Nerve Supply– No infection
The patient– smoking
The method of treatment

Upper Extremity Trauma

14
DIAGNOSING THE BONE INJURY
Clinical assessment
– History - Co-morbidities
– Exposure/systematic examination
“First-aid” reduction
Splintage and analgesia
Radiographs– Two planes including joints above and below area
of injury

TopicsTopics
ClavicleClavicle Shoulder DislocationShoulder Dislocation HumerusHumerus ElbowElbow ForearmForearm Distal RadiusDistal Radius

Clavicle FracturesClavicle Fractures

Clavicle FracturesClavicle Fractures
MechanismMechanism– Fall onto shoulder Fall onto shoulder
(87%)(87%)– Direct blow (7%)Direct blow (7%)– Fall onto outstretched Fall onto outstretched
hand (6%)hand (6%) Trimodal distributionTrimodal distribution
0
10
20
30
40
50
60
70
80
Group I(13yrs)
Group 2(47yrs)
Group 3(59yrs)
Percent
The clavicle is the last ossification
center to complete (sternal end) at about 22-25yo.

Clavicle FracturesClavicle Fractures
Clinical EvaluationClinical Evaluation– Inspect and palpate for Inspect and palpate for
deformity/abnormal motiondeformity/abnormal motion– Thorough distal neurovascular examThorough distal neurovascular exam– Auscultate the chest for the possibility Auscultate the chest for the possibility
of lung injury or pneumothoraxof lung injury or pneumothorax Radiographic ExamRadiographic Exam
– AP chest radiographs.AP chest radiographs.– Clavicular 45deg A/P oblique X-raysClavicular 45deg A/P oblique X-rays

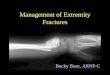
Clavicle FracturesClavicle Fractures Allman Classification of Clavicle FracturesAllman Classification of Clavicle Fractures
– Type IType I Middle Third (80%)Middle Third (80%)– Type IIType II Distal Third (15%)Distal Third (15%)
Differentiate whether ligaments Differentiate whether ligaments attached to lateral or medial fragmentattached to lateral or medial fragment
– Type IIIType III Medial Third (5%)Medial Third (5%)

Clavicle FractureClavicle Fracture
Closed TreatmentClosed Treatment– Sling immobilization for usually 3-4 weeks with Sling immobilization for usually 3-4 weeks with
early ROM encouragedearly ROM encouraged Operative interventionOperative intervention
– Fractures with neurovascular injuryFractures with neurovascular injury– Fractures with severe associated chest injuriesFractures with severe associated chest injuries– Open fracturesOpen fractures– Group II, type II fracturesGroup II, type II fractures– Cosmetic reasons, uncontrolled deformityCosmetic reasons, uncontrolled deformity– NonunionNonunion

Associated InjuriesAssociated Injuries– Brachial Plexus InjuriesBrachial Plexus Injuries
Contusions most common, penetrating Contusions most common, penetrating (rare)(rare)
– Vascular InjuryVascular Injury– Rib Fractures Rib Fractures – Scapula FracturesScapula Fractures– PneumothoraxPneumothorax
Clavicle FracturesClavicle Fractures

Shoulder DislocationsShoulder Dislocations

Shoulder DislocationsShoulder Dislocations
EpidemiologyEpidemiology– Anterior: Most commonAnterior: Most common– Posterior: UncommonPosterior: Uncommon– Inferior (Luxatio Erecta), hyperabduction injuryInferior (Luxatio Erecta), hyperabduction injury

Shoulder DislocationsShoulder Dislocations
Clinical EvaluationClinical Evaluation– Examine axillary nerve (deltoid function, not Examine axillary nerve (deltoid function, not
sensation over lateral shoulder)sensation over lateral shoulder)– Examine biceps function and anterolateral Examine biceps function and anterolateral
forearm sensationforearm sensation Radiographic EvaluationRadiographic Evaluation
– True AP shoulderTrue AP shoulder– Axillary LateralAxillary Lateral– Scapular YScapular Y– Stryker Notch View (Bony Bankart)Stryker Notch View (Bony Bankart)

Shoulder DislocationsShoulder Dislocations
Anterior Dislocation Recurrence RateAnterior Dislocation Recurrence Rate– Age 20: 80-92%Age 20: 80-92%– Age 30: 60%Age 30: 60%– > Age 40: 10-15%> Age 40: 10-15%
Look for Concomitant InjuriesLook for Concomitant Injuries– Bony:Bony: Bankart, Hill-Sachs Lesion, Glenoid Bankart, Hill-Sachs Lesion, Glenoid
Fracture, Greater Tuberosity FractureFracture, Greater Tuberosity Fracture– Soft Tissue: Soft Tissue: Subscapularis Tear, RCT (older Subscapularis Tear, RCT (older
pts with dislocation)pts with dislocation)– Vascular:Vascular: Axillary artery injury (older pts with Axillary artery injury (older pts with
atherosclerosis)atherosclerosis)– Nerve:Nerve: Axillary nerve neuropraxia Axillary nerve neuropraxia

Anterior DislocationAnterior Dislocation– TraumaticTraumatic– Atraumatic Atraumatic
(Congenital Laxity)(Congenital Laxity)– Acquired Acquired
(Repeated (Repeated Microtrauma)Microtrauma)
Shoulder DislocationsShoulder Dislocations

Posterior DislocationPosterior Dislocation– Adduction/Flexion/IR at time of Adduction/Flexion/IR at time of
injuryinjury– Look for “lightbulb sign” and Look for “lightbulb sign” and
“vacant glenoid” sign“vacant glenoid” sign– Reduce with traction and gentle Reduce with traction and gentle
anterior translation (Avoid ER anterior translation (Avoid ER arm arm Fx) Fx)
Shoulder DislocationsShoulder Dislocations

Inferior DislocationsInferior DislocationsLuxatio ErectaLuxatio Erecta– Hyperabduction injuryHyperabduction injury– Arm presents in a flexed Arm presents in a flexed
“asking a question” posture“asking a question” posture– High rate of nerve and High rate of nerve and
vascular injuryvascular injury– Reduce with in-line traction Reduce with in-line traction
and gentle adductionand gentle adduction
Shoulder DislocationsShoulder Dislocations

Shoulder DislocationShoulder Dislocation TreatmentTreatment
– Nonoperative treatmentNonoperative treatment Closed reduction should be performed after adequate Closed reduction should be performed after adequate
clinical evaluation and appropriate sedationclinical evaluation and appropriate sedation
– Reduction Techniques:Reduction Techniques: Traction/countertraction- Generally used with a sheet Traction/countertraction- Generally used with a sheet
wrapped around the patient and one wrapped around the wrapped around the patient and one wrapped around the reducer.reducer.
Hippocratic technique- Effective for one person. One foot Hippocratic technique- Effective for one person. One foot placed across the axillary folds and onto the chest wall placed across the axillary folds and onto the chest wall then using gentle internal and external rotation with axial then using gentle internal and external rotation with axial tractiontraction
Stimson technique- Patient placed prone with the affected Stimson technique- Patient placed prone with the affected extremity allowed to hang free. Gentle traction may be extremity allowed to hang free. Gentle traction may be usedused
Milch Technique- Arm is abducted and externally rotated Milch Technique- Arm is abducted and externally rotated with thumb pressure applied to the humeral headwith thumb pressure applied to the humeral head
Scapular manipulationScapular manipulation

Shoulder DislocationsShoulder Dislocations
PostreductionPostreduction– Post reduction films are a must to confirm the Post reduction films are a must to confirm the
position of the humeral headposition of the humeral head– Pain controlPain control– Immobilization for 7-10 days then begin Immobilization for 7-10 days then begin
progressive ROMprogressive ROM Operative IndicationsOperative Indications
– Irreducible shoulder (soft tissue interposition)Irreducible shoulder (soft tissue interposition)– Displaced greater tuberosity fracturesDisplaced greater tuberosity fractures– Glenoid rim fractures bigger than 5 mmGlenoid rim fractures bigger than 5 mm– Elective repair for younger patientsElective repair for younger patients

Proximal Humerus FracturesProximal Humerus Fractures


Proximal Humerus FracturesProximal Humerus Fractures
EpidemiologyEpidemiology– Most common fracture of the humerusMost common fracture of the humerus– Higher incidence in the elderly, thought to be Higher incidence in the elderly, thought to be
related to osteoporosisrelated to osteoporosis– Females 2:1 greater incidence than malesFemales 2:1 greater incidence than males
Mechanism of InjuryMechanism of Injury– Most commonly a fall onto an outstretched arm Most commonly a fall onto an outstretched arm
from standing heightfrom standing height– Younger patient typically present after high Younger patient typically present after high
energy trauma energy trauma

Proximal Humerus FracturesProximal Humerus Fractures
Clinical EvaluationClinical Evaluation– Patients typically present with arm Patients typically present with arm
held close to chest by contralateral held close to chest by contralateral hand. Pain and crepitus detected on hand. Pain and crepitus detected on palpationpalpation
– Careful NV exam is essential, Careful NV exam is essential, particularly with regards to the axillary particularly with regards to the axillary nerve. Test sensation over the deltoid. nerve. Test sensation over the deltoid. Deltoid atony does not necessarily Deltoid atony does not necessarily confirm an axillary nerve injuryconfirm an axillary nerve injury

Proximal Humerus FracturesProximal Humerus Fractures
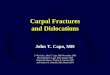
Neer ClassificationNeer Classification– Four partsFour parts
Greater and lesser Greater and lesser tuberosities, tuberosities,
Humeral shaftHumeral shaft Humeral headHumeral head
– A part is displaced if A part is displaced if >1 cm displacement >1 cm displacement or >45 degrees of or >45 degrees of angulation is seenangulation is seen

Proximal Humerus FracturesProximal Humerus Fractures TreatmentTreatment
– Minimally displaced fractures- Sling immobilization, early Minimally displaced fractures- Sling immobilization, early motionmotion
– Two-part fractures- Two-part fractures- Anatomic neck fractures likely require ORIF. High incidence Anatomic neck fractures likely require ORIF. High incidence
of osteonecrosisof osteonecrosis Surgical neck fractures that are minimally displaced can be Surgical neck fractures that are minimally displaced can be
treated conservatively. Displacement usually requires ORIFtreated conservatively. Displacement usually requires ORIF– Three-part fracturesThree-part fractures
Due to disruption of opposing muscle forces, these are Due to disruption of opposing muscle forces, these are unstable so closed treatment is difficult. Displacement unstable so closed treatment is difficult. Displacement requires ORIF. requires ORIF.
– Four-part fracturesFour-part fractures In general for displacement or unstable injuries ORIF in the In general for displacement or unstable injuries ORIF in the
young and hemiarthroplasty in the elderly and those with young and hemiarthroplasty in the elderly and those with severe comminution. High rate of AVN (13-34%)severe comminution. High rate of AVN (13-34%)

Humeral Shaft FracturesHumeral Shaft Fractures

Humeral Shaft FracturesHumeral Shaft Fractures
Mechanism of InjuryMechanism of Injury– Direct trauma is the most common especially Direct trauma is the most common especially
MVAMVA– Indirect trauma such as fall on an outstretched Indirect trauma such as fall on an outstretched
handhand– Fracture pattern depends on stress appliedFracture pattern depends on stress applied
Compressive- proximal or distal humerusCompressive- proximal or distal humerus Bending- transverse fracture of the shaftBending- transverse fracture of the shaft Torsional- spiral fracture of the shaftTorsional- spiral fracture of the shaft Torsion and bending- oblique fracture usually Torsion and bending- oblique fracture usually
associated with a butterfly fragmentassociated with a butterfly fragment

Humeral Shaft FracturesHumeral Shaft Fractures
Clinical evaluationClinical evaluation– Thorough history and Thorough history and
physicalphysical– Patients typically Patients typically
present with pain, present with pain, swelling, and deformity swelling, and deformity of the upper armof the upper arm
– Careful NV exam Careful NV exam important as the radial important as the radial nerve is in close nerve is in close proximity to the proximity to the humerus and can be humerus and can be injuredinjured

Humeral Shaft FracturesHumeral Shaft Fractures
Radiographic evaluationRadiographic evaluation– AP and lateral views of the humerus AP and lateral views of the humerus – Traction radiographs may be indicated Traction radiographs may be indicated
for hard to classify secondary to severe for hard to classify secondary to severe displacement or a lot of comminutiondisplacement or a lot of comminution

Humeral Shaft FracturesHumeral Shaft Fractures Conservative TreatmentConservative Treatment
– Goal of treatment is to Goal of treatment is to establish union with establish union with acceptable alignmentacceptable alignment
– >90% of humeral shaft >90% of humeral shaft fractures heal with fractures heal with nonsurgical managementnonsurgical management 20 degrees of anterior 20 degrees of anterior
angulation, 30 degrees of varus angulation, 30 degrees of varus angulation and up to 3 cm of angulation and up to 3 cm of shortening are acceptableshortening are acceptable
Most treatment begins with Most treatment begins with application of a coaptation spint application of a coaptation spint or a hanging arm cast followed or a hanging arm cast followed by placement of a fracture brace by placement of a fracture brace

Humeral Shaft FracturesHumeral Shaft Fractures
TreatmentTreatment– Operative TreatmentOperative Treatment
Indications for operative treatment Indications for operative treatment include inadequate reduction, include inadequate reduction, nonunion, associated injuries, open nonunion, associated injuries, open fractures, segmental fractures, fractures, segmental fractures, associated vascular or nerve injuriesassociated vascular or nerve injuries
Most commonly treated with plates Most commonly treated with plates but also IM nailsbut also IM nails

Humeral Shaft FracturesHumeral Shaft Fractures
Holstein-Lewis FracturesHolstein-Lewis Fractures– Distal 1/3 fracturesDistal 1/3 fractures– May entrap or lacerate radial nerve as the May entrap or lacerate radial nerve as the
fracture passes through the intermuscular fracture passes through the intermuscular septumseptum

Elbow Fracture/DislocationsElbow Fracture/Dislocations

Elbow DislocationsElbow Dislocations EpidemiologyEpidemiology
– Accounts for 11-28% of injuries to the elbowAccounts for 11-28% of injuries to the elbow– Posterior dislocations most commonPosterior dislocations most common– Highest incidence in the young 10-20 years and Highest incidence in the young 10-20 years and
usually sports injuriesusually sports injuries Mechanism of injuryMechanism of injury
– Most commonly due to fall on outstretched hand Most commonly due to fall on outstretched hand or elbow resulting in force to unlock the or elbow resulting in force to unlock the olecranon from the trochleaolecranon from the trochlea
– Posterior dislocation following hyperextension, Posterior dislocation following hyperextension, valgus stress, arm abduction, and forearm valgus stress, arm abduction, and forearm supinationsupination
– Anterior dislocation ensuing from direct force to Anterior dislocation ensuing from direct force to the posterior forearm with elbow flexedthe posterior forearm with elbow flexed

Elbow DislocationsElbow Dislocations
Clinical EvaluationClinical Evaluation– Patients typically present guarding the injured Patients typically present guarding the injured
extremityextremity– Usually has gross deformity and swellingUsually has gross deformity and swelling– Careful NV exam in important and should be Careful NV exam in important and should be
done prior to radiographs or manipulationdone prior to radiographs or manipulation– Repeat after reductionRepeat after reduction
Radiographic EvaluationRadiographic Evaluation– AP and lateral elbow films should be obtained AP and lateral elbow films should be obtained
both pre and post reductionboth pre and post reduction– Careful examination for associated fracturesCareful examination for associated fractures

Elbow Fracture/DislocationsElbow Fracture/Dislocations TreatmentTreatment
– Posterior DislocationPosterior Dislocation Closed reduction under sedationClosed reduction under sedation Reduction should be performed with the elbow flexed Reduction should be performed with the elbow flexed
while providing distal tractionwhile providing distal traction Post reduction management includes a posterior Post reduction management includes a posterior
splint with the elbow at 90 degreessplint with the elbow at 90 degrees Open reduciton for severe soft tissue injuries or bony Open reduciton for severe soft tissue injuries or bony
entrapmententrapment– Anterior DislocationAnterior Dislocation
Closed reduction under sedationClosed reduction under sedation Distal traction to the flexed forearm followed by Distal traction to the flexed forearm followed by
dorsally direct pressure on the volar forearm with dorsally direct pressure on the volar forearm with anterior pressure on the humerusanterior pressure on the humerus

Elbow DislocationsElbow Dislocations
Associated injuriesAssociated injuries– Radial head fx (5-Radial head fx (5-
11%)11%)– TreatmentTreatment
Type I- ConservativeType I- Conservative Type II/III- Attempt Type II/III- Attempt
ORIF vs. radial head ORIF vs. radial head replacementreplacement

Elbow DislocationsElbow Dislocations
Associated Associated injuriesinjuries– Coronoid process Coronoid process
fractures (5-10%)fractures (5-10%)

Elbow DislocationsElbow Dislocations
Associated injuriesAssociated injuries– Medial or lateral epicondylar fx (12-Medial or lateral epicondylar fx (12-
34%)34%)

Elbow DislocationsElbow Dislocations Instability ScaleInstability Scale
– Type IType I Posterolateral rotary Posterolateral rotary
instability, lateral ulnar instability, lateral ulnar collateral ligament disruptedcollateral ligament disrupted
– Type IIType II Perched condyles, varus Perched condyles, varus
instability, ant and post instability, ant and post capsule disruptedcapsule disrupted
– Type IIIType III A: posterior dislocation with A: posterior dislocation with
valgus instability, medial valgus instability, medial collateral ligament disruptioncollateral ligament disruption
B: posterior dislocation, B: posterior dislocation, grossly unstable, lateral, grossly unstable, lateral, medial, anterior, and medial, anterior, and posterior disruptionposterior disruption

Forearm FracturesForearm Fractures

Forearm FracturesForearm Fractures
EpidemiologyEpidemiology– Highest ratio of open to closed than any Highest ratio of open to closed than any
other fracture except the tibiaother fracture except the tibia– More common in males than females, More common in males than females,
most likely secondary mva, contact most likely secondary mva, contact sports, altercations, and fallssports, altercations, and falls
Mechanism of InjuryMechanism of Injury– Commonly associated with mva, direct Commonly associated with mva, direct
trauma and fallstrauma and falls

Forearm FracturesForearm Fractures Clinical EvaluationClinical Evaluation
– Patients typically present with gross deformity of Patients typically present with gross deformity of the forearm and with pain, swelling, and loss of the forearm and with pain, swelling, and loss of function at the handfunction at the hand
– Careful exam is essential, with specific Careful exam is essential, with specific assessment of radial, ulnar, and median nerves assessment of radial, ulnar, and median nerves and radial and ulnar pulsesand radial and ulnar pulses
– Tense compartments, unremitting pain, and pain Tense compartments, unremitting pain, and pain with passive motion should raise suspicion for with passive motion should raise suspicion for compartment syndromecompartment syndrome
Radiographic EvaluationRadiographic Evaluation– AP and lateral radiographs of the forearmAP and lateral radiographs of the forearm– Don’t forget to examine and x-ray the elbow and Don’t forget to examine and x-ray the elbow and
wristwrist

Forearm FracturesForearm Fractures Ulna FracturesUlna Fractures
– These include nightstick and Monteggia fracturesThese include nightstick and Monteggia fractures– Monteggia denotes a fracture of the proximal Monteggia denotes a fracture of the proximal
ulna with an associated radial head dislocationulna with an associated radial head dislocation Monteggia fractures classification- BadoMonteggia fractures classification- Bado Type I- Anterior Dislocation of the radial head with Type I- Anterior Dislocation of the radial head with
fracture of ulna at any level- produced by forced fracture of ulna at any level- produced by forced pronationpronation
Type II- Posterior/posterolateral dislocation of the radial Type II- Posterior/posterolateral dislocation of the radial head- produced by axial loading with the forearm flexedhead- produced by axial loading with the forearm flexed
Type III- Lateral/anterolateral dislocation of the radial Type III- Lateral/anterolateral dislocation of the radial head with fracture of the ulnar metaphysis- forced head with fracture of the ulnar metaphysis- forced abduction of the elbowabduction of the elbow
Type IV- anterior dislocation of the radial head with Type IV- anterior dislocation of the radial head with fracture of radius and ulna at the same level- forced fracture of radius and ulna at the same level- forced pronation with radial shaft failurepronation with radial shaft failure

Monteggia fractures Monteggia fractures

Forearm FracturesForearm Fractures Radial Diaphysis FracturesRadial Diaphysis Fractures
– Fractures of the proximal two-thirds can be Fractures of the proximal two-thirds can be considered truly isolatedconsidered truly isolated
– Galeazzi or Piedmont fractures refer to fracture Galeazzi or Piedmont fractures refer to fracture of the radius with disruption of the distal radial of the radius with disruption of the distal radial ulnar jointulnar joint
MechanismMechanism– Usually caused by direct or indirect trauma, Usually caused by direct or indirect trauma,
such as fall onto outstretched handsuch as fall onto outstretched hand– Galeazzi fractures may result from direct trauma Galeazzi fractures may result from direct trauma
to the wrist, typically on the dorsolateral aspect, to the wrist, typically on the dorsolateral aspect, or fall onto outstretched hand with pronationor fall onto outstretched hand with pronation

Galeazzi fractureGaleazzi fracture

Distal Radius FracturesDistal Radius Fractures

Distal Radius FracturesDistal Radius Fractures

Distal Radius FracturesDistal Radius Fractures
EpidemiologyEpidemiology– Most common fractures of the upper extremityMost common fractures of the upper extremity– Common in older patients. Usually a result of Common in older patients. Usually a result of
direct trauma such as fall on out stretched handdirect trauma such as fall on out stretched hand– Increasing incidence due to aging populationIncreasing incidence due to aging population
Mechanism of InjuryMechanism of Injury– Most commonly a fall on an outstretched Most commonly a fall on an outstretched
extremity with the wrist in dorsiflexionextremity with the wrist in dorsiflexion– High energy injuries may result in significantly High energy injuries may result in significantly
displaced, highly unstable fracturesdisplaced, highly unstable fractures

Distal Radius FracturesDistal Radius Fractures
A severe Colles fracture may assume a bayonet-like displacement.

Distal Radius FracturesDistal Radius Fractures
Clinical EvaluationClinical Evaluation– Patients typically present with gross Patients typically present with gross
deformity of the wrist with variable deformity of the wrist with variable displacement of the hand in relation to the displacement of the hand in relation to the wrist. Typically swollen with painful ROMwrist. Typically swollen with painful ROM
– Ipsilateral shoulder and elbow must be Ipsilateral shoulder and elbow must be examinedexamined
– NV exam including specifically median NV exam including specifically median nerve for acute carpal tunnel compression nerve for acute carpal tunnel compression syndromesyndrome

Radiographic EvaluationRadiographic Evaluation
3 view of the wrist including AP, Lat, 3 view of the wrist including AP, Lat, and Obliqueand Oblique– Normal RelationshipsNormal Relationships
23 Deg
11 mm
11 Deg

Distal Radius FracturesDistal Radius Fractures EponymsEponyms
– Colles FractureColles Fracture Combination of intra and extra articular fractures of the distal Combination of intra and extra articular fractures of the distal
radius with dorsal angulation (apex volar), dorsal radius with dorsal angulation (apex volar), dorsal displacement, radial shift, and radial shortentingdisplacement, radial shift, and radial shortenting
Most common distal radius fracture caused by fall on Most common distal radius fracture caused by fall on outstretched handoutstretched hand
– Smith Fracture (Reverse Colles)Smith Fracture (Reverse Colles) Fracture with volar angulation (apex dorsal) from a fall on a Fracture with volar angulation (apex dorsal) from a fall on a
flexed wristflexed wrist– Barton FractureBarton Fracture
Fracture with dorsal or volar rim displaced with the hand and Fracture with dorsal or volar rim displaced with the hand and carpuscarpus
– Radial Styloid Fracture (Chauffeur Fracture)Radial Styloid Fracture (Chauffeur Fracture) Avulsion fracture with extrinsic ligaments attached to the Avulsion fracture with extrinsic ligaments attached to the
fragmentfragment Mechanism of injury is compression of the scaphoid against Mechanism of injury is compression of the scaphoid against
the styloidthe styloid

Distal Radius FracturesDistal Radius Fractures
TreatmentTreatment– Displaced fractures require and attempt at Displaced fractures require and attempt at
reduction.reduction. Hematoma block-10ccs of lidocaine or a mix of lidocaine Hematoma block-10ccs of lidocaine or a mix of lidocaine
and marcaine in the fracture siteand marcaine in the fracture site Hang the wrist in fingertraps with a traction weightHang the wrist in fingertraps with a traction weight Reproduce the fracture mechanism and reduce the Reproduce the fracture mechanism and reduce the
fracturefracture Place in sugar tong splintPlace in sugar tong splint
– Operative ManagementOperative Management For the treatment of intraarticular, unstable, malreduced For the treatment of intraarticular, unstable, malreduced
fractures.fractures. As always, open fractures must go to the OR.As always, open fractures must go to the OR.


Spinal TraumaSpinal Trauma

TopicsTopics
Introduction to Spinal InjuriesIntroduction to Spinal Injuries Spinal Anatomy and PhysiologySpinal Anatomy and Physiology Pathophysiology of Spinal InjuryPathophysiology of Spinal Injury Assessment of the Spinal Injury Assessment of the Spinal Injury
PatientPatient Management of the Spinal Injury Management of the Spinal Injury
PatientPatient

Introduction to Spinal Introduction to Spinal InjuriesInjuries
Annually 15,000 permanent spinal cord injuriesAnnually 15,000 permanent spinal cord injuries Commonly men 16Commonly men 16––30 years old30 years old Mechanism of InjuryMechanism of Injury
– Vehicle crashes: 48%Vehicle crashes: 48%– Falls: 21%Falls: 21%– Penetrating trauma: 15%Penetrating trauma: 15%– Sports injury: 14%Sports injury: 14%
25% of all spinal cord injuries occur from improper handling 25% of all spinal cord injuries occur from improper handling of the spine and patient after injury.of the spine and patient after injury.– ASSUME based upon MOI that patients have a spinal injury.ASSUME based upon MOI that patients have a spinal injury.– MANAGE ALL spinal injuries with immediate and continued MANAGE ALL spinal injuries with immediate and continued
care.care. Lifelong care for spinal cord injury victim exceeds $1 Lifelong care for spinal cord injury victim exceeds $1
million.million. Best form of care is public safety and prevention programs.Best form of care is public safety and prevention programs.

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologyVertebral Column Vertebral Column
33 bones comprise the spine.33 bones comprise the spine. Function:Function:
– Skeletal support structureSkeletal support structure– Major portion of axial skeletonMajor portion of axial skeleton– Protective container for spinal cordProtective container for spinal cord
Vertebral Body:Vertebral Body:– Major weight-bearing componentMajor weight-bearing component– Anterior to other vertebrae componentsAnterior to other vertebrae components

Spinal Anatomy and Spinal Anatomy and PhysiologyPhysiology
Vertebral Column Vertebral Column

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologyVertebral Column Vertebral Column
Size of VertebraeSize of Vertebrae– C-1 and C-2:C-1 and C-2:
No vertebral bodyNo vertebral body Support headSupport head Allow for turning of headAllow for turning of head
– Vertebral body size increases the more inferior Vertebral body size increases the more inferior they become.they become. Lumbar spine strongest and largestLumbar spine strongest and largest
– Bear weight of the bodyBear weight of the body
– Sacral and coccyx vertebrae are fused.Sacral and coccyx vertebrae are fused. No vertebral bodyNo vertebral body

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologyVertebral Column Vertebral Column
Components of VertebraeComponents of Vertebrae– Spinal CanalSpinal Canal
Opening in the vertebrae that the spinal cord passes Opening in the vertebrae that the spinal cord passes throughthrough
– PediclesPedicles Thick, bony structures that connect the vertebral body Thick, bony structures that connect the vertebral body
to the spinous and transverse processesto the spinous and transverse processes
– LaminaeLaminae Posterior bones of vertebrae that make up foramenPosterior bones of vertebrae that make up foramen
– Transverse ProcessTransverse Process Bilateral projections from vertebraeBilateral projections from vertebrae Muscle attachment and articulation location with ribsMuscle attachment and articulation location with ribs

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologyVertebral ColumnVertebral Column
Components of VertebraeComponents of Vertebrae– Spinous ProcessSpinous Process
Posterior prominence on vertebraePosterior prominence on vertebrae
– Intervertebral DiskIntervertebral Disk Cartilaginous pad between vertebraeCartilaginous pad between vertebrae Serves as shock absorberServes as shock absorber

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologyVertebral Column Vertebral Column
Vertebral LigamentsVertebral Ligaments– Anterior LongitudinalAnterior Longitudinal
Anterior surface of vertebral bodiesAnterior surface of vertebral bodies Provides major stability of the spinal columnProvides major stability of the spinal column Resists hyperextensionResists hyperextension
– Posterior LongitudinalPosterior Longitudinal Posterior surface of vertebral bodies in Posterior surface of vertebral bodies in
spinal canalspinal canal Prevents hyperflexionPrevents hyperflexion

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologyVertebral Column Vertebral Column
Cervical SpineCervical Spine– 7 vertebrae7 vertebrae– Sole support for headSole support for head
Head weighs 16Head weighs 16––22 pounds22 pounds– C-1 (Atlas)C-1 (Atlas)
Supports headSupports head Securely affixed to the occiputSecurely affixed to the occiput Permits noddingPermits nodding
– C-2 (Axis)C-2 (Axis) Odontoid process (dens)Odontoid process (dens)
– Projects upwardProjects upward– Provides pivot point so head can rotateProvides pivot point so head can rotate
– C-7C-7 Prominent spinous process (vertebra prominens)Prominent spinous process (vertebra prominens)

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologyVertebral Column Vertebral Column
Thoracic SpineThoracic Spine– 12 vertebrae12 vertebrae– 1st rib articulates with T-11st rib articulates with T-1
Attaches to transverse process and vertebral bodyAttaches to transverse process and vertebral body
– Next nine ribs attach to the inferior and superior Next nine ribs attach to the inferior and superior portion of adjacent vertebral bodiesportion of adjacent vertebral bodies Limits rib movement and provides increased rigidityLimits rib movement and provides increased rigidity
– Larger and stronger than cervical spineLarger and stronger than cervical spine Larger muscles help to ensure that the body stays Larger muscles help to ensure that the body stays
erecterect Supports movement of the thoracic cage during Supports movement of the thoracic cage during
respirationsrespirations

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologyVertebral Column Vertebral Column
Lumbar SpineLumbar Spine– 5 vertebrae5 vertebrae– Bear forces of bending and lifting above Bear forces of bending and lifting above
the pelvisthe pelvis– Largest and thickest vertebral bodies Largest and thickest vertebral bodies
and intervertebral disksand intervertebral disks

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologyVertebral Column Vertebral Column
Sacral SpineSacral Spine– 5 fused vertebrae5 fused vertebrae– Form posterior plate of pelvisForm posterior plate of pelvis– Help protect urinary and reproductive Help protect urinary and reproductive
organsorgans– Attach pelvis and lower extremities to Attach pelvis and lower extremities to
axial skeletonaxial skeleton Coccygeal SpineCoccygeal Spine
– 33––5 fused vertebrae5 fused vertebrae– Residual elements of a tailResidual elements of a tail

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal MeningesSpinal Meninges
LayersLayers– Dura materDura mater– ArachnoidArachnoid– Pia materPia mater
Cover entire spinal cord and peripheral Cover entire spinal cord and peripheral nerve roots that exitnerve roots that exit
Cerebrospinal fluid bathes spinal cord by Cerebrospinal fluid bathes spinal cord by filling the subarachnoid spacefilling the subarachnoid space– Exchange of nutrients and waste productsExchange of nutrients and waste products– Absorbs shocks of sudden movementAbsorbs shocks of sudden movement

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal Cord Spinal Cord
FunctionFunction– Transmits sensory input from body to the brainTransmits sensory input from body to the brain– Conducts motor impulses from brain to muscles Conducts motor impulses from brain to muscles
and organsand organs– Reflex centerReflex center
Intercepts sensory signals and initiates a reflex signalIntercepts sensory signals and initiates a reflex signal
GrowthGrowth– FetusFetus
Entire cord fills entire spinal foramenEntire cord fills entire spinal foramen
– AdultAdult Base of brain to L-1 or L-2 levelBase of brain to L-1 or L-2 level Peripheral nerve roots pulled into spinal foramen at the Peripheral nerve roots pulled into spinal foramen at the
distal end (cauda equina)distal end (cauda equina)

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal Cord Spinal Cord
Blood SupplyBlood Supply– Paired spinal arteriesPaired spinal arteries
Branch off the vertebral, cervical, thoracic, Branch off the vertebral, cervical, thoracic, and lumbar arteriesand lumbar arteries
Travel through intervertebral foraminaTravel through intervertebral foramina– Split into anterior and posterior arteriesSplit into anterior and posterior arteries

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal Cord Spinal Cord
General Cord AnatomyGeneral Cord Anatomy– Anterior Medial FissureAnterior Medial Fissure
Deep crease along the ventral surface of the spinal Deep crease along the ventral surface of the spinal cord that divides cord into left and right halvescord that divides cord into left and right halves
– Posterior Medial FissurePosterior Medial Fissure Shallow longitudinal groove along the dorsal surfaceShallow longitudinal groove along the dorsal surface
– Gray MatterGray Matter Area of the CNS dominated by nerve cell bodiesArea of the CNS dominated by nerve cell bodies Central portion of the spinal cordCentral portion of the spinal cord
– White MatterWhite Matter Surrounds gray matterSurrounds gray matter Comprised of axonsComprised of axons

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal Cord Spinal Cord
General Cord AnatomyGeneral Cord Anatomy– AxonsAxons
Transmit signals upward to the brain and Transmit signals upward to the brain and down to the bodydown to the body
Ascending tractsAscending tracts– Axons that transmit signals to the brainAxons that transmit signals to the brain– Sensory tractsSensory tracts
Descending tractsDescending tracts– Axons that transmit signals to the bodyAxons that transmit signals to the body– Motor tractsMotor tracts
Voluntary and fine muscle movementVoluntary and fine muscle movement


Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal NervesSpinal Nerves
31 pairs of nerves that originate along the 31 pairs of nerves that originate along the spinal cord from anterior and posterior nerve spinal cord from anterior and posterior nerve rootsroots– Sensory and motor functionsSensory and motor functions– Travel through intervertebral foraminaTravel through intervertebral foramina
1st pair exit between the skull and C-11st pair exit between the skull and C-1 Remainder of pairs exit below the vertebraeRemainder of pairs exit below the vertebrae Each pair has 2 dorsal and 2 ventral rootsEach pair has 2 dorsal and 2 ventral roots
– Ventral roots: motor impulses from cord to bodyVentral roots: motor impulses from cord to body– Dorsal roots: sensory impulses from body to cordDorsal roots: sensory impulses from body to cord– C-1 and Co-1 do not have dorsal rootsC-1 and Co-1 do not have dorsal roots

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal Nerves Spinal Nerves
PlexusPlexus– Nerve roots that converge in a cluster of Nerve roots that converge in a cluster of
nervesnerves Cervical plexusCervical plexus
– 5 cervical nerve roots5 cervical nerve roots– Innervates the neckInnervates the neck– Produces the phrenic nerveProduces the phrenic nerve
Peripheral nerve roots C-3 through C-5Peripheral nerve roots C-3 through C-5 Responsible for diaphragm controlResponsible for diaphragm control ““C3, 4, and 5 keep the diaphragm alive”C3, 4, and 5 keep the diaphragm alive”

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal NervesSpinal Nerves
Brachial PlexusBrachial Plexus– C-5 through T-1C-5 through T-1– Controls the upper extremityControls the upper extremity
Lumbar and Sacral PlexusesLumbar and Sacral Plexuses– Innervation of the lower extremityInnervation of the lower extremity

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal NervesSpinal Nerves

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal Nerves Spinal Nerves
DermatomesDermatomes– Topographical region of the body Topographical region of the body
surface innervated by one nerve rootsurface innervated by one nerve root– Key locationsKey locations
Collar region: C-3Collar region: C-3 Little finger: C-7Little finger: C-7 Nipple line: T-4Nipple line: T-4 Umbilicus: T-10Umbilicus: T-10 Small toe: S-1Small toe: S-1

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal Nerves Spinal Nerves

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal Nerves Spinal Nerves
MyotomesMyotomes– Muscle and tissue of the body Muscle and tissue of the body
innervated by spinal nerve rootsinnervated by spinal nerve roots– Key myotomesKey myotomes
Arm extension: C-5Arm extension: C-5 Elbow extension: C-7Elbow extension: C-7 Small finger abduction: T-1Small finger abduction: T-1 Knee extension: L-3Knee extension: L-3 Ankle flexion: S-1Ankle flexion: S-1

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal Nerves Spinal Nerves
Reflex PathwaysReflex Pathways– FunctionFunction
Speed body’s response to stressorsSpeed body’s response to stressors Reduce seriousness of injuryReduce seriousness of injury Body stabilizationBody stabilization
– Occur in special neuronsOccur in special neurons InterneuronsInterneurons ExampleExample
– Touch hot stove.Touch hot stove.– Severe pain sends intense impulse to brain.Severe pain sends intense impulse to brain.– Strong signal triggers interneuron in the spinal cord to Strong signal triggers interneuron in the spinal cord to
direct a signal to the flexor muscle.direct a signal to the flexor muscle.– Limb withdraws without waiting for a signal from the Limb withdraws without waiting for a signal from the
brain.brain.

Spinal Anatomy and Spinal Anatomy and PhysiologyPhysiology
Spinal Nerves Spinal Nerves

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal Nerves Spinal Nerves
Subdivision of ANSSubdivision of ANS– Parasympathetic, “Feed and Breed”Parasympathetic, “Feed and Breed”
Controls rest and regenerationControls rest and regeneration Peripheral nerve roots from the sacral and Peripheral nerve roots from the sacral and
cranial nervescranial nerves Major FunctionsMajor Functions
– Slows heart rateSlows heart rate– Increases digestive system activityIncreases digestive system activity– Plays a role in sexual stimulationPlays a role in sexual stimulation

Spinal Anatomy and PhysiologySpinal Anatomy and PhysiologySpinal Nerves Spinal Nerves
Subdivision of ANS Subdivision of ANS – Sympathetic, “Fight or Flight”Sympathetic, “Fight or Flight”
Increases metabolic rateIncreases metabolic rate Branches from nerves in the thoracic and lumbar Branches from nerves in the thoracic and lumbar
regionsregions Major FunctionsMajor Functions
– Decreases organ and digestive system activityDecreases organ and digestive system activity VasoconstrictionVasoconstriction
– Release of epinephrine and norepinephrineRelease of epinephrine and norepinephrine– Systemic vascular resistanceSystemic vascular resistance
Reduces venous blood volumeReduces venous blood volume Increases peripheral vascular resistanceIncreases peripheral vascular resistance
– Increases heart rateIncreases heart rate– Increases cardiac outputIncreases cardiac output

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury
Mechanisms of Spinal InjuryMechanisms of Spinal Injury
– Extremes of MotionExtremes of Motion HyperextensionHyperextension Hyperflexion: “Kiss the Chest”Hyperflexion: “Kiss the Chest” Excessive rotationExcessive rotation Lateral bendingLateral bending

Pathophysiology of Spinal Pathophysiology of Spinal InjuryInjury
Mechanisms of Spinal InjuryMechanisms of Spinal Injury
– Axial StressAxial Stress Axial loadingAxial loading
– Compression common between T-12 and L-2Compression common between T-12 and L-2
DistractionDistraction CombinationCombination
– Distraction/rotation or compression/flexionDistraction/rotation or compression/flexion
– Other MOIOther MOI Direct, blunt, or penetrating traumaDirect, blunt, or penetrating trauma ElectrocutionElectrocution

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury







Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury
(4 of 14)(4 of 14) Column InjuryColumn Injury
– Movement of vertebrae from normal positionMovement of vertebrae from normal position– Subluxation or dislocationSubluxation or dislocation– FracturesFractures
Spinous process and transverse processSpinous process and transverse process Pedicle and laminaePedicle and laminae Vertebral bodyVertebral body
– Ruptured intervertebral disksRuptured intervertebral disks– Common sites of injuryCommon sites of injury
C-1/C-2: Delicate vertebraeC-1/C-2: Delicate vertebrae C-7: Transition from flexible cervical spine to thoraxC-7: Transition from flexible cervical spine to thorax T-12/L-1: Different flexibility between thoracic and T-12/L-1: Different flexibility between thoracic and
lumbar regionslumbar regions

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury
(5 of 14)(5 of 14) Cord InjuryCord Injury– ConcussionConcussion
Similar to cerebral concussionSimilar to cerebral concussion Temporary and transient disruption of cord Temporary and transient disruption of cord
functionfunction– ContusionContusion
Bruising of the cordBruising of the cord Tissue damage, vascular leakage, and swellingTissue damage, vascular leakage, and swelling
– CompressionCompression Secondary to:Secondary to:
– Displacement of the vertebraeDisplacement of the vertebrae– Herniation of intervertebral diskHerniation of intervertebral disk– Displacement of vertebral bone fragmentDisplacement of vertebral bone fragment– Swelling from adjacent tissueSwelling from adjacent tissue

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury
(6 of 14)(6 of 14) Cord InjuryCord Injury
– LacerationLaceration CausesCauses
– Bony fragments driven into the vertebral foramenBony fragments driven into the vertebral foramen– Cord may be stretched to the point of tearingCord may be stretched to the point of tearing
Hemorrhage into cord tissue, swelling, and Hemorrhage into cord tissue, swelling, and disruption of impulsesdisruption of impulses
– HemorrhageHemorrhage Associated with contusion, laceration, or Associated with contusion, laceration, or
stretchingstretching

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury
(7 of 14)(7 of 14) Transection Cord InjuryTransection Cord Injury
– Injury that partially or completely severs Injury that partially or completely severs the spinal cordthe spinal cord CompleteComplete
– Cervical SpineCervical Spine QuadriplegiaQuadriplegia IncontinenceIncontinence Respiratory paralysisRespiratory paralysis
– Below T-1Below T-1 IncontinenceIncontinence ParaplegiaParaplegia
IncompleteIncomplete

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury
(8 of 14)(8 of 14) Incomplete Transection Cord InjuryIncomplete Transection Cord Injury– Anterior Cord SyndromeAnterior Cord Syndrome
Anterior vascular disruptionAnterior vascular disruption Loss of motor function and sensation of pain, light Loss of motor function and sensation of pain, light
touch, and temperature below injury sitetouch, and temperature below injury site Retain motor, positional, and vibration sensationRetain motor, positional, and vibration sensation
– Central Cord SyndromeCentral Cord Syndrome Hyperextension of cervical spineHyperextension of cervical spine Motor weakness affecting upper extremitiesMotor weakness affecting upper extremities Bladder dysfunctionBladder dysfunction
– Brown-Sequard’s SyndromeBrown-Sequard’s Syndrome Penetrating injury that affects one side of the cordPenetrating injury that affects one side of the cord Ipsilateral sensory and motor lossIpsilateral sensory and motor loss Contralateral pain and temperature sensation lossContralateral pain and temperature sensation loss

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury
(9 of 14)(9 of 14) General Signs and SymptomsGeneral Signs and Symptoms
– Extremity paralysisExtremity paralysis– Pain with and without movementPain with and without movement– Tenderness along spineTenderness along spine– Impaired breathingImpaired breathing– Spinal deformitySpinal deformity– PriapismPriapism– PosturingPosturing– Loss of bowel or bladder controlLoss of bowel or bladder control– Nerve impairment to extremitiesNerve impairment to extremities

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury (10 of 14)(10 of 14)
Spinal ShockSpinal Shock– Temporary insult to the cordTemporary insult to the cord– Affects body below the level of injuryAffects body below the level of injury– Affected areaAffected area
FlaccidFlaccid Without feelingWithout feeling Loss of movement (flaccid paralysis)Loss of movement (flaccid paralysis) Frequent loss of bowel and bladder controlFrequent loss of bowel and bladder control PriapismPriapism Hypotension secondary to vasodilationHypotension secondary to vasodilation

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury (11 of 14)(11 of 14) Neurogenic ShockNeurogenic Shock
– Spinal-Vascular ShockSpinal-Vascular Shock– Occurs when injury to the spinal cord disrupts Occurs when injury to the spinal cord disrupts
the brain’s ability to control the bodythe brain’s ability to control the body Loss of sympathetic toneLoss of sympathetic tone
– Dilation of arteries and veinsDilation of arteries and veins Expands vascular spaceExpands vascular space Results in relative hypotensionResults in relative hypotension
– Reduced cardiac preloadReduced cardiac preload– Reduction of the strength of contractionReduction of the strength of contraction
Frank-Starling reflexFrank-Starling reflex ANS loses sympathetic control over adrenal medullaANS loses sympathetic control over adrenal medulla
– Unable to control release of epinephrine and Unable to control release of epinephrine and norepinephrinenorepinephrine
Loss of positive inotropic and chronotropic effectsLoss of positive inotropic and chronotropic effects

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury (12 of 14)(12 of 14)
Neurogenic ShockNeurogenic Shock– Signs and SymptomsSigns and Symptoms
BradycardiaBradycardia HypotensionHypotension Cool, moist, and pale skin above the injuryCool, moist, and pale skin above the injury Warm, dry, and flushed skin below the injuryWarm, dry, and flushed skin below the injury Male: priapismMale: priapism

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury (13 of 14)(13 of 14)
Autonomic Hyperreflexia SyndromeAutonomic Hyperreflexia Syndrome– Associated with the body’s resolution of the Associated with the body’s resolution of the
effects of spinal shockeffects of spinal shock– Commonly associated with injuries at or above Commonly associated with injuries at or above
T-6T-6– PresentationPresentation
Sudden hypertensionSudden hypertension BradycardiaBradycardia Pounding headachePounding headache Blurred visionBlurred vision Sweating and flushing of skin above the point of injurySweating and flushing of skin above the point of injury

Pathophysiology of Spinal Pathophysiology of Spinal Injury Injury (14 of 14)(14 of 14)
Other Causes of Neurologic Other Causes of Neurologic DysfunctionDysfunction– Any injury that affects the nerve Any injury that affects the nerve
impulse’s path of travelimpulse’s path of travel SwellingSwelling DislocationDislocation FractureFracture Compartment syndromeCompartment syndrome

Assessment of the Spinal Injury Assessment of the Spinal Injury Patient Patient (1 of 4)(1 of 4)
Scene Size-upScene Size-up– Evaluate MOI.Evaluate MOI.– Consider spinal clearance protocol.Consider spinal clearance protocol.– Determine type of spinal trauma.Determine type of spinal trauma.– Maintain suspicion with sports injuries.Maintain suspicion with sports injuries.– If unclear about MOI, take spinal If unclear about MOI, take spinal
precautions.precautions.

Assessment of the Spinal Injury Assessment of the Spinal Injury Patient Patient (2 of 4)(2 of 4)
Initial AssessmentInitial Assessment– Consider spinal clearance protocol.Consider spinal clearance protocol.– Consider spinal precautions.Consider spinal precautions.
Head injuryHead injury Intoxicated patientsIntoxicated patients Injuries above the shouldersInjuries above the shoulders Distracting injuriesDistracting injuries
– Maintain manual stabilization.Maintain manual stabilization. Vest style versus rapid extricationVest style versus rapid extrication Maintain neutral alignmentMaintain neutral alignment Increase of pain or resistance, restrict movement in Increase of pain or resistance, restrict movement in
position foundposition found

Assessment of the Spinal Injury Assessment of the Spinal Injury Patient Patient (3 of 4)(3 of 4)
Initial AssessmentInitial Assessment– ABCs.ABCs.– Suction.Suction.– Consider oral or digital intubation if Consider oral or digital intubation if
required.required. Maintain in-line manual c-spine control.Maintain in-line manual c-spine control.

Assessment of the Spinal Injury Assessment of the Spinal Injury Patient Patient (4 of 4)(4 of 4)
Rapid Trauma AssessmentRapid Trauma Assessment– Focused versus rapid assessmentFocused versus rapid assessment– Rapid AssessmentRapid Assessment
Suspected or likely spinal cord/column injurySuspected or likely spinal cord/column injury Multi-system trauma patientMulti-system trauma patient Evaluate forEvaluate for
– NeckNeck Deformity, pain, crepitus, warmth, tendernessDeformity, pain, crepitus, warmth, tenderness
– Bilateral extremitiesBilateral extremities Finger abduction/adductionFinger abduction/adduction Push, pull, gripsPush, pull, grips
– Motor and sensory functionMotor and sensory function– Dermatome and myotome evaluationDermatome and myotome evaluation– Babinski’s sign testBabinski’s sign test– Hold-up positionHold-up position

Babinski’s Sign TestBabinski’s Sign Test
Stroke lateral aspect of the bottom of Stroke lateral aspect of the bottom of the foot.the foot.
Evaluate for movement of the toes.Evaluate for movement of the toes.– Fanning and flexing (lifting)Fanning and flexing (lifting)
Positive signPositive sign– Injury along the pyramidal (descending spinal) Injury along the pyramidal (descending spinal)
tracttract

Assessment of the Assessment of the Spinal Injury PatientSpinal Injury Patient
Vital SignsVital Signs– Body temperatureBody temperature
Above and below site of injuryAbove and below site of injury
– PulsePulse– Blood pressureBlood pressure– RespirationsRespirations
Ongoing AssessmentOngoing Assessment– Recheck elements of initial assessment.Recheck elements of initial assessment.– Recheck vital signs.Recheck vital signs.– Recheck interventions.Recheck interventions.– Recheck any neurological deviations.Recheck any neurological deviations.

Spinal Clearance ProtocolSpinal Clearance Protocol

Spinal Integrity TerminologySpinal Integrity Terminology StabilizeStabilize is a word commonly used to describe is a word commonly used to describe
protecting the spinal cord from possible injury (or protecting the spinal cord from possible injury (or further injury) when vertebral column integrity is further injury) when vertebral column integrity is disrupted. disrupted.
ImmobilizeImmobilize refers to the “splinting” of the head, refers to the “splinting” of the head, neck, and torso to limit any transmission of neck, and torso to limit any transmission of motion to the spine. motion to the spine.
SpinalSpinal motion restrictionmotion restriction (SMR) is now (SMR) is now suggested as a more accurate description of suggested as a more accurate description of modern spinal injury care. However, this phrase modern spinal injury care. However, this phrase could be misunderstood to indicate a more could be misunderstood to indicate a more limited “immobilization” of the spine than is limited “immobilization” of the spine than is currently practiced. currently practiced.

Management of the Management of the Spinal Injury Patient Spinal Injury Patient (1 of 7)(1 of 7)
Spinal AlignmentSpinal Alignment– Move patient to a neutral, in-line position.Move patient to a neutral, in-line position.
Position of function.Position of function.– Hips and knees should be slightly flexed for maximum Hips and knees should be slightly flexed for maximum
comfort and minimum stress on muscles, joints, and comfort and minimum stress on muscles, joints, and spine.spine. Place a rolled blanket under the knees.Place a rolled blanket under the knees.
– ALWAYS support the head and neck.ALWAYS support the head and neck.– Contraindications to neutral position:Contraindications to neutral position:
Movement causes a noticeable increase in pain.Movement causes a noticeable increase in pain. Noticeable resistance met during procedure.Noticeable resistance met during procedure. Increase in neurological deficits occurs during movement.Increase in neurological deficits occurs during movement. Gross deformity of spine.Gross deformity of spine.
– LESS MOVEMENT IS BEST.LESS MOVEMENT IS BEST.

Management of the Management of the Spinal Injury Patient Spinal Injury Patient (2 of 7)(2 of 7)
Manual Cervical ImmobilizationManual Cervical Immobilization– Seated PatientSeated Patient
Approach from front.Approach from front. Assign a caregiver to hold GENTLE manual traction.Assign a caregiver to hold GENTLE manual traction.
– Reduce axial loading.Reduce axial loading.– Evaluate posterior cervical spine.Evaluate posterior cervical spine.
Position patient’s head slowly to a neutral, in-line Position patient’s head slowly to a neutral, in-line position.position.
– Supine PatientSupine Patient Assign a caregiver to hold GENTLE manual traction.Assign a caregiver to hold GENTLE manual traction. AdultAdult
– Lift head off ground 1–2”: neutral, in-line position.Lift head off ground 1–2”: neutral, in-line position. ChildChild
– Position head at ground level: avoid flexion.Position head at ground level: avoid flexion.

Management of the Management of the Spinal Injury Patient Spinal Injury Patient (3 of 7)(3 of 7)

Management of the Management of the Spinal Injury Patient Spinal Injury Patient (4 of 7)(4 of 7)
Cervical Collar ApplicationCervical Collar Application– Apply the C-collar as soon as possible.Apply the C-collar as soon as possible.– Assess neck prior to placing.Assess neck prior to placing.– C-collar limits some movement and reduces axial loading.C-collar limits some movement and reduces axial loading.– DOES NOT completely prevent movement of the neck.DOES NOT completely prevent movement of the neck.– Size and Apply according to the manufacturer’s Size and Apply according to the manufacturer’s
recommendation.recommendation. Collar should fit snugly.Collar should fit snugly. Collar should NOT impede respirations.Collar should NOT impede respirations. Head should continue to be in neutral position.Head should continue to be in neutral position. SIZE IT, SIZE IT, SIZE IT!!!SIZE IT, SIZE IT, SIZE IT!!!
– DO NOT RELEASE manual control until the patient is fully DO NOT RELEASE manual control until the patient is fully secured in a spinal restriction device.secured in a spinal restriction device.

Management of the Management of the Spinal Injury Patient Spinal Injury Patient (5 of 7)(5 of 7)
Standing TakedownStanding Takedown– Minimum 3 rescuers.Minimum 3 rescuers.– Have patient remain immobile.Have patient remain immobile.– Rescuer provides manual stabilization from behind.Rescuer provides manual stabilization from behind.– Assess neck.Assess neck.– Size and place c-collar.Size and place c-collar.– Position board behind patient.Position board behind patient.– Grasp board under patient’s shoulders.Grasp board under patient’s shoulders.– Lower board to ground.Lower board to ground.– Secure patient.Secure patient.
COMMUNICATE WITH PARTNERS AND PATIENT.COMMUNICATE WITH PARTNERS AND PATIENT.

Management of the Management of the Spinal Injury Patient Spinal Injury Patient (6 of 7)(6 of 7)
Helmet RemovalHelmet Removal– When to remove:When to remove:
Helmet does not immobilize the patient’s head Helmet does not immobilize the patient’s head within.within.
Cannot securely immobilize the helmet to the long Cannot securely immobilize the helmet to the long spine board.spine board.
Helmet prevents airway care.Helmet prevents airway care. Helmet prevents assessment of anticipated injuries.Helmet prevents assessment of anticipated injuries. Present or anticipated airway or breathing problems.Present or anticipated airway or breathing problems. Removal will not cause further injury.Removal will not cause further injury.

Management of the Management of the Spinal Injury Patient Spinal Injury Patient (7 of 7)(7 of 7)
Helmet RemovalHelmet Removal– Technique:Technique:
2 Rescuers.2 Rescuers. Have a plan.Have a plan. Remove face mask and chin strap.Remove face mask and chin strap. Immobilize head.Immobilize head.
– Slide one hand under back of neck and head.Slide one hand under back of neck and head.– Other hand supports anterior neck and jaw.Other hand supports anterior neck and jaw.
Remove helmet.Remove helmet.– Gently rock head to clear occiput.Gently rock head to clear occiput.
All actions should be slow and deliberate.All actions should be slow and deliberate.
– TRANSPORT HELMET with patient.TRANSPORT HELMET with patient.– COMMUNICATION is the KEY.COMMUNICATION is the KEY.

Bledsoe et al., Bledsoe et al., Paramedic Care Paramedic Care Principles & Practice Volume Principles & Practice Volume 4: Trauma4: Trauma© 2006 by Pearson Education, © 2006 by Pearson Education, Inc. Upper Saddle River, NJInc. Upper Saddle River, NJ
Movement of the Movement of the Spinal Injury Patient Spinal Injury Patient (1 of 2)(1 of 2)
Any movement MUST be coordinated.Any movement MUST be coordinated. Move patient as a unit.Move patient as a unit. NO LATERAL PUSHING.NO LATERAL PUSHING.
– Move patient up and down to prevent lateral Move patient up and down to prevent lateral bending.bending.
Rescuer at the head “CALLS” all moves.Rescuer at the head “CALLS” all moves. ALL MOVES MUST be slowly executed and ALL MOVES MUST be slowly executed and
well coordinated.well coordinated. Consider the final positioning of the patient Consider the final positioning of the patient
prior to beginning move.prior to beginning move.

Bledsoe et al., Bledsoe et al., Paramedic Care Paramedic Care Principles & Practice Volume Principles & Practice Volume 4: Trauma4: Trauma© 2006 by Pearson Education, © 2006 by Pearson Education, Inc. Upper Saddle River, NJInc. Upper Saddle River, NJ
Movement of the Movement of the Spinal Injury Patient Spinal Injury Patient (2 of 2)(2 of 2)
Types of MovesTypes of Moves– Log rollLog roll– Straddle slideStraddle slide– Rope-Sling slideRope-Sling slide– Orthopedic stretcherOrthopedic stretcher– Vest-type immobilizationVest-type immobilization– Rapid extricationRapid extrication– Final patient positioningFinal patient positioning– Long spine boardLong spine board– Full-body vacuum mattressFull-body vacuum mattress– Diving injury immobilizationDiving injury immobilization

Management of the Management of the Spinal Injury Patient Spinal Injury Patient (1 of 3)(1 of 3)
Medications and Spinal Cord InjuryMedications and Spinal Cord Injury– Steroids if neuro-deficit is identifiedSteroids if neuro-deficit is identified
Reduce the body’s response to injuryReduce the body’s response to injury Reduce swelling and pressure on cordReduce swelling and pressure on cord Administered within 1st 8 hours of injuryAdministered within 1st 8 hours of injury

Management of the Management of the Spinal Injury Patient Spinal Injury Patient (2 of 3)(2 of 3)
Medications and Neurogenic ShockMedications and Neurogenic Shock– Fluid ChallengeFluid Challenge
Isotonic solution: 20 mL/kgIsotonic solution: 20 mL/kg– 250 mL initially250 mL initially– Monitor response and repeat as neededMonitor response and repeat as needed
– PASGPASG ControversialControversial
– Research shows no positive outcomeResearch shows no positive outcome
– DopamineDopamine 22––20 mcg/kg/min titrated to blood pressure20 mcg/kg/min titrated to blood pressure
– AtropineAtropine 0.50.5––1.0 mg q 31.0 mg q 3––5 min (maximum of 2.0 mg)5 min (maximum of 2.0 mg)

Management of the Management of the Spinal Injury Patient Spinal Injury Patient (3 of 3)(3 of 3)
Medications and the Combative Medications and the Combative PatientPatient– Consider sedatives to reduce anxiety Consider sedatives to reduce anxiety
and calm patient.and calm patient. Prevents spinal injury aggravationPrevents spinal injury aggravation
– Medications:Medications: Meperidine (Demerol)Meperidine (Demerol) Diazepam (Valium)Diazepam (Valium) Consider paralytics with airway controlConsider paralytics with airway control

SummarySummary
Introduction to Spinal InjuriesIntroduction to Spinal Injuries Spinal Anatomy and PhysiologySpinal Anatomy and Physiology Pathophysiology of Spinal InjuryPathophysiology of Spinal Injury Assessment of the Spinal Injury Assessment of the Spinal Injury
PatientPatient Management of the Spinal Injury Management of the Spinal Injury
PatientPatient

The End











![Overlooked extremity fractures in the emergency …Overlooked extremity fractures in the emergency department in the ED can also have significant clinical and legal consequences.[13]](https://img.pdfslide.net/doc/110x75/5ec79238ebc8e14ea5068f93/overlooked-extremity-fractures-in-the-emergency-overlooked-extremity-fractures-in.jpg)