1698
for the existence of complete aphasia to be observed.The meningeal symptoms gradually diminished.On several occasions lumbar puncture was per-formed with similar results. On the 9th the cerebro-spinal fluid was found under increased tension,of an amber colour and turbid. It contained 688leucocytes per cubic millimetre, which consisted of88’3 per cent. of polynuclears, 9’3 of lymphocytes,and 2’3 of mononuclears. Cultures of the fluidwere sterile and inoculation of a rabbit negative.Recovery ensued. In the second case a man, aged30 years, the subject of plumbism, was taken to
hospital comatose on Sept. 26th, 1912. There wasright hemiplegia. He had had a
" stroke " during
his work. He remained in this state for 48 hours,and on the morning of the 28th, when he becameconscious, he was found to be aphasic. In theevening he again became comatose, and in additionto the hemiplegia meningeal symptoms were found.The neck was rigid and Kernig’s sign was presenton the left side. There was optic neuritis and theurine contained albumin. Lumbar puncture wasperformed several times. On the 26th the cerebro-
spinal fluid bad the rose-colour of haemorrhage. Onthe 28th it was of an amber colour and contained
leucocytes in abundance. They were almost allintact polynuclears. There were no red corpuscles.Death occurred on the 30th. The necropsy showedan encysted heamorrhage which had destroyed theleft internal capsule and part of the grey nuclei.
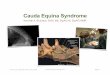
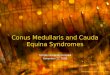
LESIONS OF THE CAUDA EQUINA.
HIDDEN away as it is from most investigators,even from the enterprising surgeon of the twentiethcentury (whose researches lead him into districtsthat the pathologists of past generations were
content to leave unexplored unless there were specialreasons for going there), the cauda equina hashitherto received something less than its due shareof attention. However, this is going to be changed,as two papers in the April and May numbers of theAmerican Joul’nal of the Jledical Sciences show.The first, by Dr. Joseph Collins and Dr. C. A. Elsberg,describes recently observed cases of giant tumoursencountered in this area. These tumours, theysay, seem to originate in the pia over the rootsor from the roots themselves ; they grow slowly,causing few symptoms until they have attainedsuch a size that they fill the entire lower part ofthe spinal canal, extending upwards over the conusand the lumbo-sacral cord. Three such cases aredescribed, in the first of which the diagnosis was sus-pected, while in the other two a correct diagnosisof giant tumour of the cauda equina was made beforethe operation. In spite of this diagnostic accuracythe results of operation were not very good; twoof the patients were considerably relieved, but itwas impossible to effect a complete removal of thegrowth. The writers think that an earlier dia-
gnosis would offer some hope of a radical success.As they point out, their patients’ histories pre-sented a long period of premonitory symptoms,chief among which were pain in the small of theback, extending sooner or later into one and thenthe other lower limb, and leading to a diagnosis ofsciatica, stiffness of the lumbar back, increasingstiffness and weakness in the lower limbs, withdrop-foot, and slight sphincter disturbances. Tothese data objective examination added the dis-covery of paralysis of the peronei and sometimes ofthe anterior tibial group, absence of the knee- andankle-jerks, tenderness of the lower lumbar spines,
irregular and asymmetrical sensory disturbances,and absence of cerebro-spinal fluid or of charac-teristic changes on lumbar puncture. The tumoursremoved were endotheliomata or endothelial sarco.mata; they were relatively benign and did nottend to extend through the dura. The secondpaper, by Dr. Foster Kennedy, Dr. C. A. Elsberg,and Dr. C. I. Lambert, emanates from the samesource, the New York Neurological Institute. Init the authors describe what they regard as a newmorbid entity. This belief is based on observa-tion of five cases so closely resembling one
another, and so different from anything hithertodescribed, that it seems to be well founded. Thesymptoms were pain in the lower limbs, especiallyin the backs of the thighs and the calves; atrophyof the anterior tibial muscles, with drop foot;objective sensory phenomena most marked andsevere in the areas supplied by the sacral roots;loss of knee-jerks, and (in three cases) a plantarextensor response. At the laminectomies whichwere performed in every instance the caudal rootswere found to be swollen, congested, and bluish-redin colour. Pathological examination showed theseappearances to be due to a meningo-radiculitiswhich was not syphilitic or tuberculous in character,but which is very suggestively compared by theauthors to a similar condition found in horses, andto the phenomena produced experimentally inthese and other nerve roots by bacterial toxins
ascending from the periphery into the centralnervous system along the nerve trunks. In thesehuman cases, however, no source of infection ofthis kind appears to have been discoverable.
SEASONAL CHANGES IN THE HEALTH OF THECONSUMPTIVE.
THE popular belief that the summer months arethe most favourable for the consumptive is, nodoubt, largely founded on the observation thatcoughs and colds are so much more frequent in thewinter than in the summer. But even when thenon-tuberculous conditions are excluded it wouldseem that the prevailing belief in the salubrity ofthe summer months is founded on fact as far asconsumption is concerned. This view has latelybeen confirmed and amplified by Dr. N. J.
Strandgaard, whose investigations, communicatedat a meeting of the Medical Society of Copenhagen,have been published in Hospitalstidende ofApril lst. It is the practice for patients in theDanish sanatoriums to be weighed every Saturdaymorning, and the average gain of weight isbetween 200 and 300 grammes. To be exact,the average is 270 grammes, which is the figuregiven for eight sanatoriums with an averagetotal of 800 patients during a period of 10 years.The average gain of weight varies much with theseason of the year. From December to May it is
fairly uniform but low, being 225 to 250 grammes.It rises rapidly and steadily from May to September,during which month it reaches the maximum of380 grammes. It falls from October to December,which is the month showing the smallest gain ofweight. The average gain of weight in Septemberis almost double that in December, and there canbe little doubt that gain in weight is, as a rule,accompanied with improvement in the patient’shealth. Thus at Boserup, one of the Danish sana-toriums, it was noted during an observation periodof 10 years, that the proportion of febrile patientsconfined to bed was about twice as great in the
Recommended