INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 26 No.1, 2005 47
Department of Radiation Oncology & PathologyAll India Institute of Medical Sciences, New Delhi-110 029.Correspondence to : SUSHMITA PATHYE-mail : [email protected]
ABSTRACTXeroderma pigmentosa with squamous cellcarcinoma of skin has been infrequentlyreported. A nine year old boy havingxeroderma pigmentosa presented withextensive ulceration in the face. Oninvestigations, the ulceration was found to besquamous cell carcinoma. The details of thiscase are presented and management with ashort course of palliative radiotherapy isdiscussed.
INTRODUCTION
Xeroderma pigmentosum (XP) is a heterogenousgroup of genetic diseases which result fromfaulty DNA repair mechanism. I t is a rareautosomal recessive disease characterized byphotosensit iv i ty, pigmentary changes,premature skin aging, neoplasia and abnormalDNA repair. Xeroderma pigmentosa wasrecognised in late 1800 by Maritz Kaposi.1 XPhas been reported world wide in all races withan over al l prevalence of 1--4 per mi l l ionpopulation. Basal cell carcinoma is found to beassociated with XP in majority of the reportedcases in Indian l i terature.2- 3Very few adultpatients revealed squamous cell lesions.
Here we report a case of squamous cellcarcinoma of the face in a young boy co-existingwith xeroderma pigmentosa. A signif icantfamily history was also elicited.
CASE
A 9 year old boy presented to our tumour clinicwith history of skin pigmentation over face,
Squamous Cell Carcinoma of Face With XerodermaPigmentosa – A Case Report
S. PATHY, K.K. NAIK, SUMAN BHASKER, M.C. SHARMA, P.K. JULKA,AND G.K. RATH
neck and trunk, freckles over face andphotophobia since 6 months of age. Ulcerationon the left side of face was present for 8 months.The pigmentation was progressive and more soafter exposure to sunlight and over exposedareas.
A detai led history revealed simi larsymptoms in his sibling aged 12 years with non-progressive lesion. The child was immunizedwith no signif icant perinatal history.Development of milestones was normal.
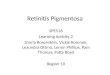
Local examinat ion revealed extensiveulcero-proliferative lesion on left side of faceinvolving left eye, temporal region, 7x7 cmextending from supraorbital ridge above, toangle of mouth below with purulent discharge,areas of haemorrhage and everted margins, andanother lesion measuring 4 x 3cm on the rightside of the face with crusting and haemorrhage(Figure 1a and 1b). Small papular lesion was seenon the rest of the face. Mult iple pigmentedlesions and skin freckles were noticed all overthe body. There was no signif icant cervicallymphadenopathy. Systemic examinat ionincluding neurological functions was essentiallynormal. Haemogram and serum biochemistrywas within normal l imits. Chest radiographyand ultrasonography of abdomen were normal.
Biopsy of the skin lesion revealedsquamous cell carcinoma with keratin pearls(Fig 2). The patient was offered conservativetreatment with ant ibiot ics and wound carefol lowed by pal l iat ive radiotherapy to theprimary lesion as surgical excision was notfeasible. A dose of 30Gy in 15 fractions over 3weeks was planned by direct field on Co60 unit.Subsequently there was adequate symptom
Case Report-III

INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 26 No.1, 2005 48
DISCUSSION
The incidence of xeroderma pigmentosa isapproximately 1 in 250,000 population.4 Theexact genet ic defects are st i l l not ful lyunderstood in al l forms of xerodermapigmentosa, but defective excision repair of UVinduced DNA damage is found in mostindividuals. Defective repair replication waslater reported with dermal f ibroblasts,lymphocytes and conjunctival cells.5
There are 10 genetic complementationgroups; while one group exhibits defective, postrepl icat ion repair (XP variant), nine aredeficient in excision repair (XP group A-I) .Owing to impaired ability to repair, defective ordamaged DNA is retained. Retention of thedamaged DNA leads to heritable chromosomalmutation and cell death, which possibly causeneoplastic and atrophic clinical abnormalities.
Skin changes are noticed between 12-36months in 75% cases, in the case reported initialsymptoms were noticed at 6 months of age.
The cutaneous stages are well defined andsimilar cutaneous changes are also observed inporphyria and aminoaciduria, however nohumoral substances have been demonstrated inxeroderma pigmentosa.
Ocular manifestat ions include-photo-phobia as the earl iest symptom which is afeature of keratitis. This was also seen in thepresent case study. Other ocular complicationsinclude exposure kerat i t is, vascular izat ion,ulcerat ion, nodular dystrophy and uveit is.Neurologic defects are detected in 20-30% ofpatients with XP. Microcephaly, delayed motordevelopment, dementia, sensorineural deafnessare common disorders.6
The disease is a progressive andaccelerated degeneration of skin, eyes andnervous system take place. If left untreated most
Figure 1b : Ulceroproliferative lesion on right side of theface 4 x 3 cm with crusting and haemorrhage.
Figure 1a : Ulceroprol i ferative lesion left side of faceinvolving left eye, temporal region,
Figure 2 : Photograph showing rests of squamous cellcarcinoma with keratin pearls (H&E x 100)
control. The patient was then continued onsymptomatic treatment. Appropriate counsellingwas offered to both the parents emphasizing theneed for early recognition of malignancy.

INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 26 No.1, 2005 49
of the patients die before the completion ofsecond decade. The course of the disease can bemodified by appropriate preventive measuresagainst exposure to sunl ight. Prophylact ictreatment with topical appl icat ion (t i taniumdioxide cream, para-amino benzoic acid inalcohol) may be administered early.
Amniocentesis and in vitro cell cultureand detect ion of defect ive DNA repair maysuggest prenatal diagnosis. 7
Cutaneous neoplasia are generally treatedwith electrodesiccation and curettage or byexcision. In the case reported above excisionwas not feasible due to the extensive lesion,mult iple satel l i te lesions and poor generalcondition. Therefore palliative radiotherapy wasoffered and the pat ient achieved adequatepall iation.
REFERENCES :
1. Hebra F, Kaposi M. On diseases of the skin includingthe exanthemata 3rd ed. London. The Men SydenhamSociety 1874;pp.252-58.
2. Saroj in i PA, Malhotra YK, Bhutani LK, Kandhar i KC.The de-sanctis cacchione syndrome. Indian J Derm Vener1969;35:247.
3. Kunwar KB, Kumar S. Xeroderma pigmentosa with basalcell carcinoma. J Indian Med Assoc 1967;48:273.
4. Knaemer KH, Lee MM, Scotto J Xeroderma pigmentosum– cutaneous, ocular and neurologic abnormalities in 830published cases. Arch Dermatol 1987;123:241-50.
5. Newsome DA, Kraemer KH, Robbins JH. Repair of DNAin xeroderma pigmentosum conjunct iva. ArchOphthalmol 1975;93:660-2.
6. Lambert WC, Kno HR, Lambert MW. XP (Review)Dermatol Clin 1995;13:169-209.
7. Ramsay CA, Cul tar t TM, Blunt S, Pawsey SA andGiannel l i F. Prenatal d iagnosis of xerodermapigmentosum : Report of f irst successful case. Lancet1974;2:1109-1112.
�
IJMPO would like to publish ‘Profile of a Cancer Centre’ or anOncology department in a major teaching institute/hospital inIndia outlining its history, facilities available, and achievementsin the field of research, teaching and patient care. Please sendyour write-up (up to 2000 words) with 2-3 photographs.
Recommended