The Microsurgical Management of Giant Retinal Tears with Trans-scleral Retinal Sutures JA Y L. FEDERMAN, MD, JEFFREY L. SHAKIN, MD, RICHARD C. LANNING, MD
Abstract: Eight cases of retinal detachment from giant tears were followed from four months to two years. Patients were treated with a combined procedure, including pars plana vitrectomy, rotation of the patient with air-gas fluid exchange to bring the retina into its normal anatomic position, and trans-scleral retinal sutures, using an external rather than internal approach. Seven of the eight cases were reattached successfully. Methods, materials, and complications are described. Pre- and post-operative information regarding visual acuity and results are listed in tabular form. [Key words: air-gas fluid exchange, giant retinal tear, macular pucker, massive periretinal proliferation, pars plana vitrectomy, retinal detachment, retinal fixation, rotation of patient, trans-scleral retinal sutures.] Ophthalmology 89:832-839, 1982
The surgical management of retinal detachments resulting from giant tears remains a difficult problem with a poor success rate. Various ingenious surgical techniques have been developed to reposition and reattach the retina in these cases.1- 10 This includes the use of sutures through the retinaY-15 This paper describes the use of trans-scleral retinal sutures to provide immediate anterior fixation of the retina in eight cases of giant tears.
MATERIALS AND METHODS
CASE SELECTION
Eight eyes with retinal detachment secondary to giant tear are presented. The retinal breaks in these
From the Department of Research and Retina Service, Wills Eye Hospital Philadelphia, PA.
Supported in part by the Wills Eye Hospital Research Department.
Presented at the Eighty-sixth Annual Meeting of the American Academy of Ophthalmology, Atlanta, Georgia, November 1-6, 1981
Reprint request to Jay L. Federman, MD, Department of Research, Wills Eye Hospital, 9th & Walnut Streets, Philadelphia, PA 19107.
832
patients ranged in extent from approximately 1200 to 2700 (Table 1). Three of the cases occurred after trauma, and five were in myopic eyes. Age range was from 14 to 52 years. There were two women and six men. In all cases the edge of the flap was everted. Slit-lamp biomicroscopy often revealed vitreoretinal traction on the posterior edge of the tear. In the six cases in which the retinal tear was 1500 or greater, the retina was completely folded over. In those cases in which just the edge was everted, there appeared to be marked redundancy, as the retina appeared to slide posteriorly, with folds in the posterior retina.
MICROSURGICAL TECHNIQUE
The combined microsurgical technique used in the management of these eight cases can be separated into three components. Extraocular, intraocular, and transocular microsurgical techniques are combined into the total procedure, as described in the following paragraphs.
Under the microscope the conjunctiva was opened, and traction sutures were placed under the rectus muscles for ocular rotation and stabilization. The anterior edge of the tear was localized with indirect ophthalmoscopy, because the posterior aspect had either slipped posteriorly or was folded over. A 3600
0161-6420/82/0700/0832/$1. 20 © American Academy of Ophthalmology

FEDERMAN , et al • MICROSURGICAL MANAGEMENT OF GIANT RETINAL TEARS
Table 1.
Preop Postop Postop No. of Reoperations Tear Visual Visual Retinal and Retinalinal
Case # Size Acuity Acuity Status Status
1 2700 CF 20/20 Macular pucker 1-flat 2 1550 20/60 20/20 Flat O-flat 3 1500 20/20 20/30 Flat O-flat 4 2500 20/400 20/20 Flat O-flat 5 1800 20/60 20/100 Macular pucker 1-flat 6 2400 20/30 LP MPP 3-MPP 7 1200 20/200 20/40 Flat O-flat 8 1250 20/400 CF Choroidal hemorrhage· 1-flat
Key: CF: count fingers; LP: light perception; MPP: massive peri retinal proliferation . • Occurred during reoperation.
silicone 2-mm band was placed approximately 4 mm behind the episcleral localization marks so that there would be a buckle effect posterior to the tear when the retina reattached. The band was secured either with mattress sutures or by the use of scleral tunnels.
A pars plana vitrectomy using three incisions was performed with two instruments . The third incision in the inferior temporal quadrant was for an infusion cannula (4 mm long, 1 mm in diameter). A I-mm vitrectomy instrument (SITE) and a I-mm fiberoptic probe for intraocular illumination were used to perform a lensectomy, followed by a vitrectomy. An attempt was made to remove all cortical vitreous as well as the vitreous from the posterior edge of the tear. The superior sclerotomy sites were closed, and the intraocular pressure equalized through the infusion cannula. Scleral beds were dissected anterior to the band exoplant in the quadrants that corresponded to the torn retina. Two beds per quadrant were made and diathermy was applied. In six eyes, each bed was 4 mm X 6 mm, but in two cases the beds measured 4 mm x 12 mm. A knife-needle incision was made at the limbus, usually in a quadrant containing the tear. The patient was turned to the prone position, and a 10% SF6, 90% air mixture was injected into the globe through the infusion cannula. In all of our cases the tear did not extend into the quadrant where the infusion cannula was placed. As the SF6-air mixture was instilled, the intraocular fluid was drained through the limbal knife-needle incision. When all intraocular fluid was removed, the retina was noted to be flat in all cases.
After the air-gas fluid exchange was completed, the infusion line was clamped so that none of the air-gas mixture would escape. The presence ofthe intraocular SF6-air bubble caused a tamponade of the retina against pigment epithelium. With the retina repositioned, the trans-scleral retinal sutures were placed. In five cases this was performed with the patient in the prone position, in three cases with the patient in the supine position. Before placing the trans-scleral retinal sutures, the retina was examined with indirect ophthalmoscopy to make sure it was reattached anatomically. The scleral beds could have been dissected
more posteriorly if the diathermy marks did not show through posterior to the edge of the tear. In no case, however, was this necessary.
The trans-scleral retinal sutures were placed, using an 8-0 monofilament nylon suture with a tapered (5/8 circle) curved needle (Fig. 1). The outside diameter of the needle was 127 microns (p,), and the outside diameter of the suture 45 p,. The proximal end of the needle was held with a curved, narrow-pointed, microneedle holder, and the sutures were placed with one rotating motion (Fig. 2A). The point was placed through the deep scleral fibers of the scleral bed, the choroid, pigment epithelium, and retina (Fig 2A); then passed across the surface of the retina (Fig 2B) and back through the retina, retinal pigment epithelium, choroid, and scleral fibers, to be tied in the scleral bed. One suture was placed for approximately every 45° of tear, or two sutures per quadrant. After the sutures
/
Fig 1. Davis and Geck suture and needle . Note 5/8 curve of needle. From tip to stem of the needle, distance is 5 mm. Outside diameter of the needle is 12711-. The outside diameter of the suture is 45 11- .
833
OPHTHALMOLOGY • JULY 1982 • VOLUME 89 • NUMBER 7
I I t-, ~I
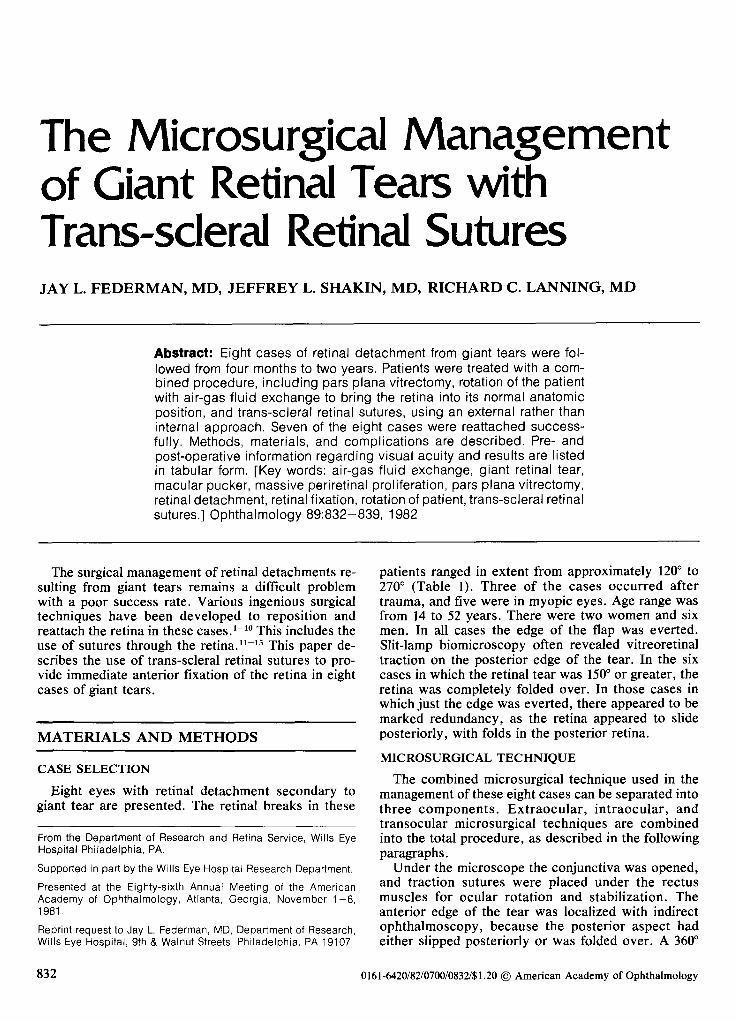
Figs 2A-B. A.left. external view showing placement of the 5/8 curved needle through the scleral bed. Notice the stem and tip of the needle protruding through the fibers of the scleral bed. B, right, internal view of needle shaft across surface of retina, piercing the retina in two places 5 mm apart.
were tied, the scleral flaps were reapproximated. The band was tightened to give a very gentle indentation. Finally, cryopexy was applied along the posterior edge of the tear (Fig 3).
ANIMAL STUDIES
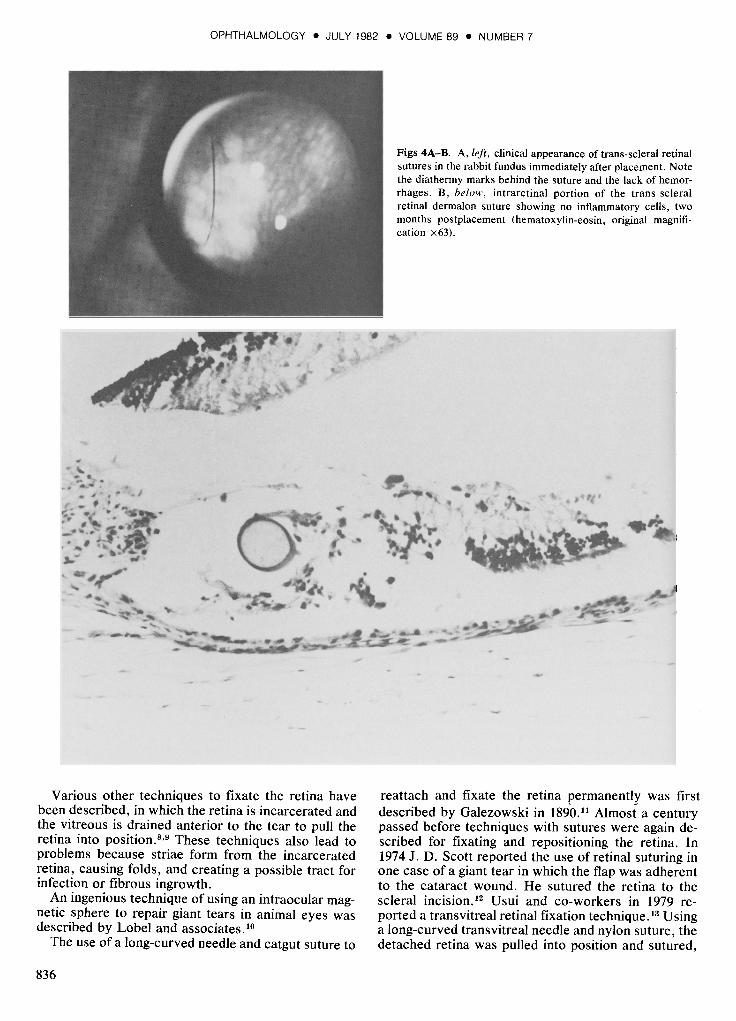
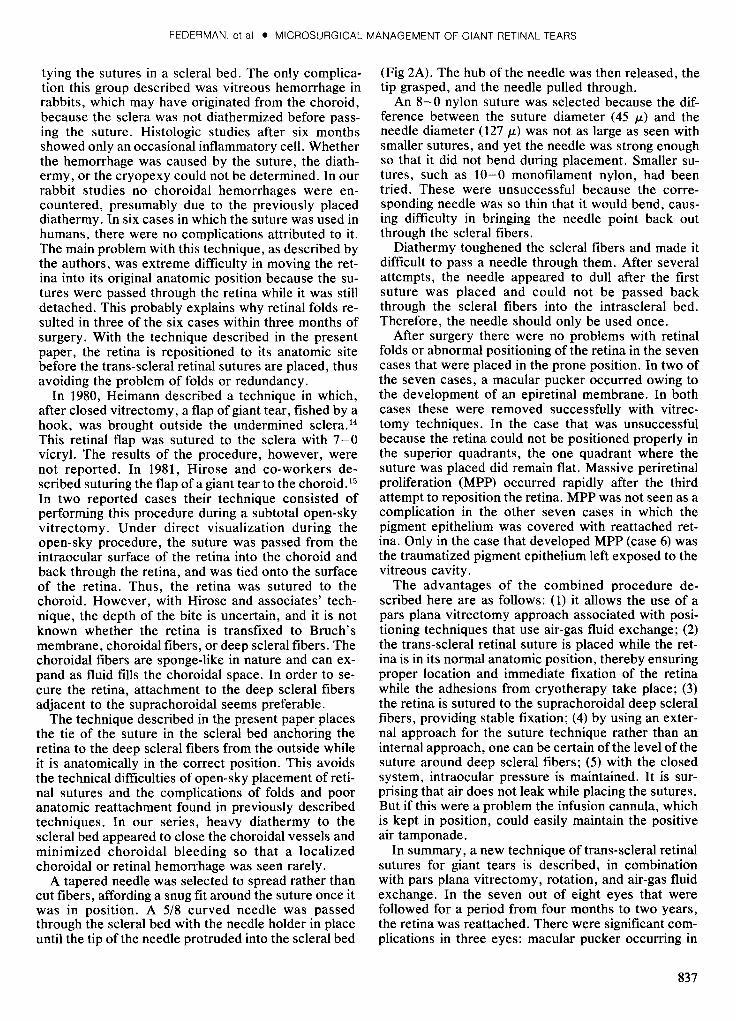
Trans-scleral retinal sutures were studied in 12 eyes of six albino rabbits. The sutures were placed via an external approach as described above. Rabbit sclera is very thin. Therefore, scleral beds were not dissected (Fig 4A). Diathermy was applied directly to the surface of the sclera before the trans-scleral retinal sutures were placed. These trans-scleral retinal suture sites were studied histologically in eyes enucleated at one, two, and three weeks and then monthly for up to six months (Fig 4B).
RESULTS
An anatomic reattachment of the retina at the time of surgery was accomplished in seven of the eight
834
cases (Table 1, Fig 3). An anatomic reattachment was not possible at the time of surgery in a patient (case 6) who had a 2400 (left eye) tear from the 2-0'clock posi:tion counterclockwise to the 6-0'clock position. This was the only case that could not be placed in a prone position and, after several attempts at air-gas fluid exchange, the retina could not be reattached. With each attempt, folds persisted superiorly. One suture was placed in the inferior nasal quadrant that held the retina flat only in that position after surgery. In the postoperative period, the retina redetached with marked posterior redundancy and a folded retina. A second and third operation were performed without success, and massive periretinal proliferation (MPP) developed so that the patient had only light perception. Of the seven cases in which an anatomic reattachment was accomplished successfully at the time of surgery, two patients developed a macular pucker after surgery within six weeks. These epiretinal membranes were successfully removed surgically (cases 1 and 5). A redetachment of the retina occurred three weeks after surgery in one of the seven cases (case 8), necessitat-
FEDERMAN, et al • MICROSURGICAL MANAGEMENT OF GIANT RETINAL TEARS
ing a second operation. During the air-gas fluid exchange an expulsive choroidal hemorrhage occurred. This patient had a 125° tear superiorly , and only one suture had been placed during the original operation. The choroidal hemorrhage cleared, and the retina has remained flat following the second operation. Unfortunately, this pateint' s vision remains at the finger counting level. The postoperative visual acuities otherwise range from 20/20 to light perception (Table 1).
The trans-scleral retinal sutures placed in the 12 rabbit eyes showed minimal inflammatory reaction after one month. The initial inflammatory response was most probably due to the diathermy. By two months postplacement, the intraretinal portion of the suture showed no inflammatory cells (Fig 4B) . Once this initial inflammation subsided , inflammatory cells were not seen around the sutures for up to six months. There was no evidence of fibrovascularization at the suture sites during the six-month follow-up. Occasionally a small retinal hemorrhage (which resorbed within one month) was seen where the suture pierced the retina. Choroidal hemorrhages were not observed.
DISCUSSION
The management of retinal detachments resulting from giant retinal breaks remains one of the most difficult challenges in ophthalmology. Various elaborate
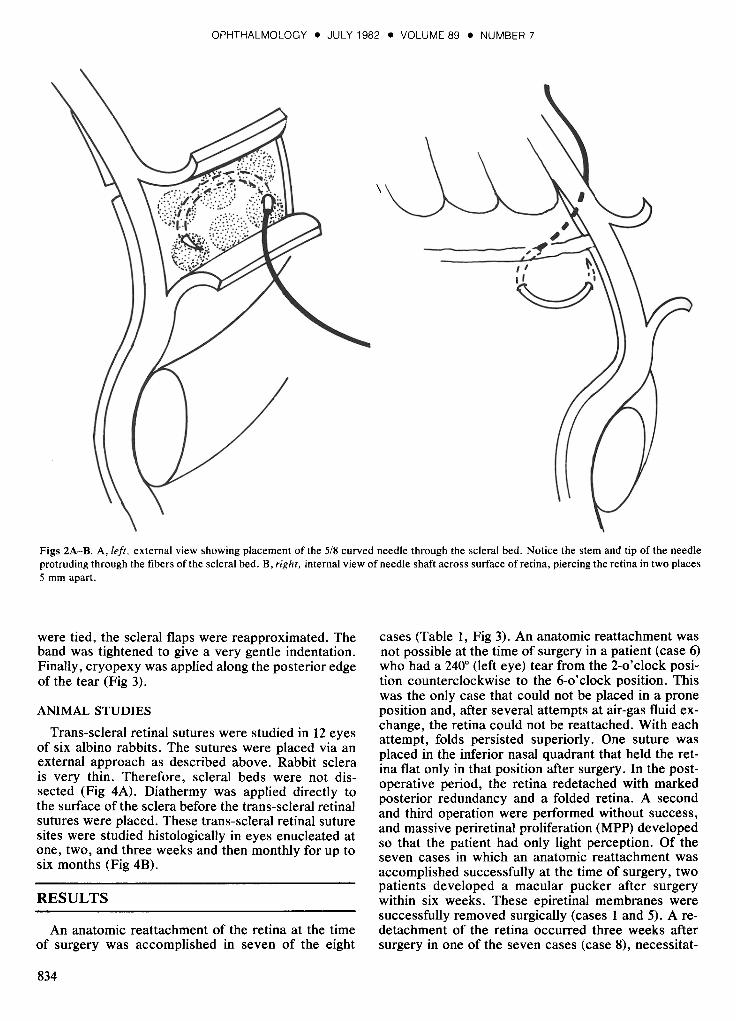
Fig 3. The reattached ret-' tina with mottled pigmen- ntation secondary to cryo '0
with six sutures . The blow- ,ups each show one suture'e crossing the area of cryo- )reaction.
techniques have been described, most of which address two specific problems: repositioning the retina, and fixation once it has been repositioned. Schepens and Freeman developed a rotating table that allowed the inverted retina to be repositioned by changing the head position of the patient after an encircling procedure, diathermy, and intravitreous fluid injection. This group reported some success .1
Freeman and co-workers described the use of an intraocular balloon to help unfold the retina. 2 Amoils described the use of cryopexy to fixate the edge of the retina,3 while Wessing and associates used an encircling band to reattach the retina through evacuation of subretinal fluid and intraocular injection of Ringer's solution followed by photocoagulation.4
•5 Norton and co-workers described intravitreous air injection with adjustment of the patient' s head in order to reposition the retina, using the air bubble to fixate the retina while adhesion formation took place. 6
Machemer and Allen and co-workers devised a technique employing vitrectomy and a rotating table, and a mixture of SF6-air to tamponade the retina7
while the chorioretinal adhesion formation took place. Even with these elaborate and sophisticated techniques of repositioning the retina, the procedure was often unsuccessful because the posterior edge of the tear would slide posteriorly or the retina would float free again after surgery, before the adhesions had become permanent.
835
OPHTHALMOLOGY. JULY 1982 • VOLUME 89 • NUMBER 7
-. .. .. ...
Various other techniques to fixate the retina have been described, in which the retina is incarcerated and the vitreous is drained anterior to the tear to pull the retina into position.8
,9 These techniques also lead to problems because striae form from the incarcerated retina, causing folds, and creating a possible tract for infection or fibrous ingrowth.
An ingenious technique of using an intraocular magnetic sphere to repair giant tears in animal eyes was described by Lobel and associates. 1o
The use of a long-curved needle and catgut suture to
836
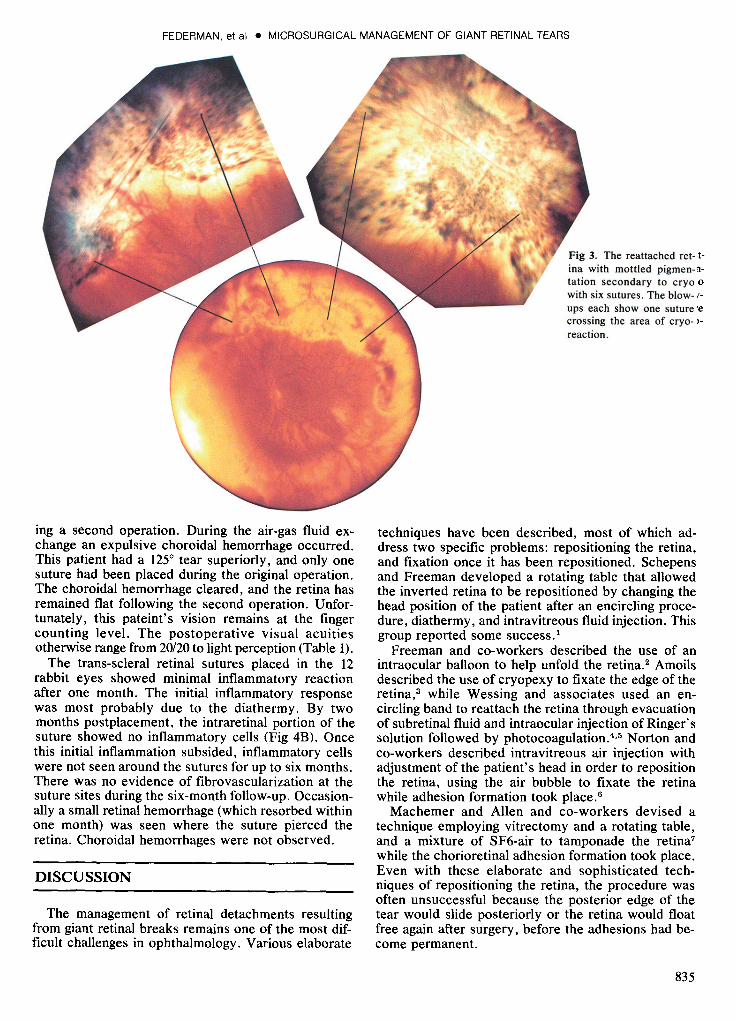
Figs 4A-B. A, left, clinical appearance of trans-scleral retinal sutures in the rabbit fundus immediately after placement. Note the diathermy marks behind the suture and the lack of hemorrhages. B, below, intraretinal portion of the trans-scleral retinal dermalon suture showing no inflammatory cells, two months postplacement <hematoxylin-eosin, original magnification x63) .
reattach and fixate the retina permanently was first described by Galezowski in 1890. 11 Almost a century passed before techniques with sutures were again described for fixating and repositioning the retina. In 1974 J. D. Scott reported the use of retinal suturing in one case of a giant tear in which the flap was adherent to the cataract wound. He sutured the retina to the scleral incision. 12 Usui and co-workers in 1979 reported a transvitreal retinal fixation technique. 13 Using a long-curved transvitreal needle and nylon suture, the detached retina was pulled into position and sutured,
FEDERMAN, et al • MICROSURGICAL MANAGEMENT OF GIANT RETINAL TEARS
tying the sutures in a scleral bed. The only complication this group described was vitreous hemorrhage in rabbits, which may have originated from the choroid, because the sclera was not diathermized before passing the suture. Histologic studies after six months showed only an occasional inflammatory cell. Whether the hemorrhage was caused by the suture, the diathermy, or the cryopexy could not be determined. In our rabbit studies no choroidal hemorrhages were encountered, presumably due to the previously placed diathermy. In six cases in which the suture was used in humans, there were no complications attributed to it. The main problem with this technique, as described by the authors, was extreme difficulty in moving the retina into its original anatomic position because the sutures were passed through the retina while it was still detached. This probably explains why retinal folds resulted in three of the six cases within three months of surgery. With the technique described in the present paper, the retina is repositioned to its anatomic site before the trans-scleral retinal sutures are placed, thus avoiding the problem of folds or redundancy.
In 1980, Heimann described a technique in which, after closed vitrectomy, a flap of giant tear, fished by a hook, was brought outside the undermined sclera. 14
This retinal flap was sutured to the sclera with 7-0 vicryl. The results of the procedure, however, were not reported. In 1981, Hirose and co-workers described suturing the flap of a giant tear to the choroid. I; In two reported cases their technique consisted of performing this procedure during a subtotal open-sky vitrectomy. Under direct visualization during the open-sky procedure, the suture was passed from the intraocular surface of the retina into the choroid and back through the retina, and was tied onto the surface of the retina. Thus, the retina was sutured to the choroid. However, with Hirose and associates' technique, the depth of the bite is uncertain, and it is not known whether the retina is transfixed to Bruch's membrane, choroidal fibers, or deep scleral fibers. The choroidal fibers are sponge-like in nature and can expand as fluid fills the choroidal space. In order to secure the retina, attachment to the deep scleral fibers adjacent to the suprachoroidal seems preferable.
The technique described in the present paper places the tie of the suture in the scleral bed anchoring the retina to the deep scleral fibers from the outside while it is anatomically in the correct position. This avoids the technical difficulties of open-sky placement of retinal sutures and the complications of folds and poor anatomic reattachment found in previously described techniques. In our series, heavy diathermy to the scleral bed appeared to close the choroidal vessels and minimized choroidal bleeding so that a localized choroidal or retinal hemorrhage was seen rarely.
A tapered needle was selected to spread rather than cut fibers, affording a snug fit around the suture once it was in position. A 5/8 curved needle was passed through the scleral bed with the needle holder in place until the tip of the needle protruded into the scleral bed
(Fig 2A). The hub of the needle was then released, the tip grasped, and the needle pulled through.
An 8-0 nylon suture was selected because the difference between the suture diameter (45 /L) and the needle diameter (127 /L) was not as large as seen with smaller sutures, and yet the needle was strong enough so that it did not bend during placement. Smaller sutures, such as 10-0 monofilament nylon, had been tried. These were unsuccessful because the corresponding needle was so thin that it would bend, causing difficulty in bringing the needle point back out through the scleral fibers.
Diathermy toughened the scleral fibers and made it difficult to pass a needle through them. After several attempts, the needle appeared to dull after the first suture was placed and could not be passed back through the scleral fibers into the intrascleral bed. Therefore, the needle should only be used once.
After surgery there were no problems with retinal folds or abnormal positioning of the retina in the seven cases that were placed in the prone position. In two of the seven cases, a macular pucker occurred owing to the development of an epiretinal membrane. In both cases these were removed successfully with vitrectomy techniques. In the case that was unsuccessful because the retina could not be positioned properly in the superior quadrants, the one quadrant where the suture was placed did remain flat. Massive periretinal proliferation (MPP) occurred rapidly after the third attempt to reposition the retina. MPP was not seen as a complication in the other seven cases in which the pigment epithelium was covered with reattached retina. Only in the case that developed MPP (case 6) was the traumatized pigment epithelium left exposed to the vitreous cavity.
The advantages of the combined procedure described here are as follows: (1) it allows the use of a pars plana vitrectomy approach associated with positioning techniques that use air-gas fluid exchange; (2) the trans-scleral retinal suture is placed while the retina is in its normal anatomic position, thereby ensuring proper location and immediate fixation of the retina while the adhesions from cryotherapy take place; (3) the retina is sutured to the suprachoroidal deep scleral fibers, providing stable fixation; (4) by using an external approach for the suture technique rather than an internal approach, one can be certain ofthe level ofthe suture around deep scleral fibers; (5) with the closed system, intraocular pressure is maintained. It is surprising that air does not leak while placing the sutures. But if this were a problem the infusion cannula, which is kept in position, could easily maintain the positive air tamponade.
In summary, a new technique of trans-scleral retinal sutures for giant tears is described, in combination with pars plana vitrectomy, rotation, and air-gas fluid exchange. In the seven out of eight eyes that were followed for a period from four months to two years, the retina was reattached. There were significant complications in three eyes: macular pucker occurring in
837

OPHTHALMOLOGY. JULY 1982 • VOLUME 89 • NUMBER 7
two eyes and an expulsive choroidal hemorrhage during a second procedure in one eye. The complication of MPP was seen only in the case that was not reattached successfully, even after three operations. It is possible that the expulsive choroidal hemorrhage that occurred during the second procedure (case 8) may have been related to the presence of a suture passing through the choroid.
ACKNOWLEDGMENTS
The authors wish to thank Drs. D. Fischer, M. Ridley, and J. Gonder for their assistance during these procedures; Drs. F. Deglin, A. Lucier, and L. K. Sarin, for referring their patient for these procedures.
REFERENCES
1. Schepens CL, Freeman HM. Current management of giant retinal breaks. Trans Am Acad Ophthalmol Otolaryngol 1967; 71:474-87.
2. Freeman HM, Couvillion GC, Schepens CL. Vitreous surgery. IV. Intraocular balloon: clinical application. Arch Ophthalmol 1970; 83:715-21.
3. Amoils SP. Cryosurgery in Ophthalmology. Chicago: Year Book Medical Publishers Inc, 1975; 162-5.
4. Wessing A, Spitznas M, Palomar A. Management of retinal detachments due to giant tears. Albrecht von Graefes Arch Klin Exp Ophthalmol 1974; 192,277-84.
5. Wessing A, Spitznas M, Palomar A Jr. The surgical treatment of retinal detachment due to equatorial giant tears. Mod Probl Ophthalmol 1975; 15:328-31.
6. Norton EWD, Aaberg T, Fung W, Curtin VT. Giant retinal tears. I. Clinical management with intravitreal air. Am J Ophthalmol 1969; 68:1011-21.
7. Machemer R, Allen AW. Retinal tears 1800 and greater. Management with vitrectomy and intravitreal gas. Arch Ophthalmol 1976; 94:1340-6.
8. Freeman HM, Schepens CL, Couvillion GC. Current management of giant retinal breaks. Part II. Trans Am Acad Ophthalmol Otololaryngol 1970; 74:59-74.
9. Howard RO, Gaasterland DE. Giant retinal dialysis and tear. Surgical repair .. Arch Ophthalmol 1970; 84:312-5.
10. Lobel D, Hale JR, Montgomery DB. A new magnetic technique for the treatment of giant retinal tears. Am J Ophthalmol 1978; 85:699-703.
11. Galezowski X. Du decollement de la retine et de son traitement. Bull Mem Soc Fr Ophtalmol 1889; 7:200-2.
12. Scott JD. A new approach to the vitreous base. Mod Probl Ophthalmol 1974; 12:407-10.
13. Usui M, Hamazaki S, Takano S, Matsuo H. A new surgical technique for the treatment of giant tear: transvitreoretinal fixation. Jpn J Ophthalmol 1979; 23:206-15.
14. Heimann K. Zur Behandlung komplizierter Riesenrisse der Netzhaut. Klin Monatsbl Augenheikd 1980; 176:491-2.
15. Hirose T, Schepens CL, Lopansri C. Subtotal open-sky vitrectomy for severe retinal detachment occurring as a late complication of ocular trauma. Ophthalmology 1981; 88: 1-9.
Discussion by
H. MacKenzie Freeman, MD
Results in giant tears continue to improve as a result of prone positioning of the patient as initiated by Schepens, 1 air injection to tamponade the tear as advocated by Norton,2 vitrectomy pioneered by Machemer,4 suturing of the torn retina using an open-sky approach as reported two years ago by Hirose,4 and trans-scleral suturing first described by Usui5 in 1979 and reported here by Federman.
I believe there is a role for all of these techniques in our armamentarium in the management of giant tears. What we must continue to do is put each technique to its optimum use while minimizing the risks in those cases that are often monocular. It is not a question of which suturing technique is better; I believe that both have a definite place in very carefully selected cases.
Trans-scleral suturing is technically easier and has less morbidity than open-sky suturing-providing the retinal flap is mobile, so that it unfolds well anteriorly. Open-sky retinal suturing is preferable when the retinal flap unfolds poorly or becomes immobilized by preretinal organization that causes
From the Retinal Associates, Boston, Massachusetts.
838
the posterior edge to become rolled like a scroll or wrinkled or shortened in a pursestring contraction. In such cases the wide exposure of the open-sky approach makes it possible to peel the extensive preretinal membranes, then handle the retina directly using a spatula to unwrinkle it, then unfold it so that it can be sutured to the choroid.
An expulsive hemorrhage in one of eight cases with its devastating effect on vision bears further consideration. In placing two sutures per quadrant in a 2700 tear, the choroid will be perforated 12 times. Transillumination may be helpful to detect anterior tributaries of the choroidal veins so as to avoid them during suture placement. 6
The failure of case 6 emphasizes the importance of having the patient in the prone position if an air fluid exchange is to be done. I have had the same bitter experience of being unable to flatten the tear when attempting the exchange in the supine position because the air bubbles rise first toward the cornea, later passing behind the retinal flap, pushing the retina posteriorly to cause the tear to gape open. Therefore, I feel it is mandatory to perform the exchange with the patient in the prone position. In the case of a 2250 giant tear in a patient that could not be placed in the prone position, I be-

lieve that open-sky retinal suturing, which is done with the patient supine, offered a better chance of success.
Dr. Federman injects the gas through a 4-mm cannula inserted temporally. With such short penetration in the posterior segment, I have had the experience in tears over 2700 of some air bubbles passing behind the flap. I suggest using a long 30-gauge needle that makes it possible to penetrate more deeply and, under indirect ophthalmoscopic control, direct those all important initial bubbles to collect over the posterior pole, and as they enlarge, the flap unfolds smoothly, uniformly, without creating folds. 7
Giant retinal breaks have been defined as retinal breaks extending over 900 or more over the circumference of the fundus. s In my experience in operating approximately 650 retinal breaks according this definition, I have found a significant variation in the severity of giant breaks and, therefore, a similar variation in the technique best suited for each case. The inferior temporal dialysis or the traumatic dialysis that have no tendency to invert are best treated by scleral buckling alone-Hagler reports over 98% success.9 In giant retinal tears extending from 90 to 1500
, with only a slight inversion of the posterior scleral flap, I advocate vitrectomy, lensectomy, air fluid exchange, and a 3600 scleral buckling, without the risks associated with retinal suturing. In such cases we have a reattachment rate of 64%, with no operative choroidal hemorrhages. We are currently investigating the use of trans-scleral suturing in tears over 1500 with an inverted flap that unfolds well and is uncomplicated by preretinal organization. When preretinal organization causes fixed folds, a curled, retracted, or immobilized flap, then open-sky suturing has been successful in these otherwise near hopeless cases.
REFERENCES
1. Schepens CL, Freeman HM. Current management of giant retinal breaks. Trans Am Acad Ophthalmol Otolaryngol 1967; 71:474-87.
2. Norton EWD, Aaberg T, Fung W, Curtin VT. Giant retinal tear. I. Clinical management with intravitreal air. Am J Ophthalmol, 1969; 68:1011-21.
3. Machemer R, Allen AW. Retinal tears 1800 and greater. Management with vitrectomy and intravitreal gas. Arch Ophthalmol, 1976; 94:1340-6.
4. Hirose T, Schepens CL, Lopansri C. Subtotal open-sky vitrectomy for severe retinal detachment occurring as a late complication of ocular trauma. Ophthalmology 1981; 88:1-9.
5. Usui M, Hamazaki S, Takano S, Matsuo H. A new surgical technique for the treatment of giant tear: transvitreoretinal fixation. Jpn J Ophthalmol; 1979, 23:206-15.
6. Freeman HM, Castillejos ME, Schepens CL. Innovations in the technique for drainage of subretinal fluid: transillumination and choroidal diathermy. Trans Am Acad Ophthalmol Otolaryngol 1974; 78:829-36.
7. Freeman HM. Current management of giant retinal breaks: results with vitrectomy and total air fluid exchange in 95 cases. Trans Am Ophthalmol Soc 1981; 79:89-100.
8. Freeman HM, Schepens CL, Couvillion GC. Current management of giant retinal breaks. Part II. Trans Am Acad Ophthalmol Otolaryngol1970; 74:59-74.
9. Hagler WS. Discussion of article by Freeman HM, Castillejos ME: Current management of giant retinal breaks: results with vitrectomy and total air fluid exchange in 95 cases. Trans Am Ophthalmol Soc 1981; 79:100-2.
839
Recommended