Embed Size (px)
Citation preview
+
Maryann Ryan, MSN, APN, NP-C, PMHNP-BCRamapo 2015
PSYCHIATRIC NURSING
2015
+
How do I know it’s right for me? Join the APNA or ISPMHN
Volunteer Do some volunteer work in agencies, hospitals, and/or community programs
where you encounter individuals or families with psychiatric problems.
A “rotation” on a psychiatric-mental health unit helps introduce students to the specialty and assists them with determining if they want to work in this area or even pursue a master’s degree in psychiatric-mental health nursing.
http://www.apna.org
+
Psychiatric Nursing Professional Organizations
American Psychiatric Nurses Association Membership available to nursing students $25.00 per year.
International Society of Psychiatric-Mental Health Nurses Associate Membership available to nursing students
$25.00 per year.
+ Psychiatric Nursing Credentialing
American Nurses Credentialing Center RN-BC Psychiatric – Mental Health Nurse PMHNP Psychiatric – Mental Health Nurse Practitioner
+Why is psychiatric nursing
different?
our patients are not usually confined to their beds “Walkie Talkies”
Their clinical issues primarily involve thoughts and feelings
Our nursing interventions focus on managing our patient’s behavior
+
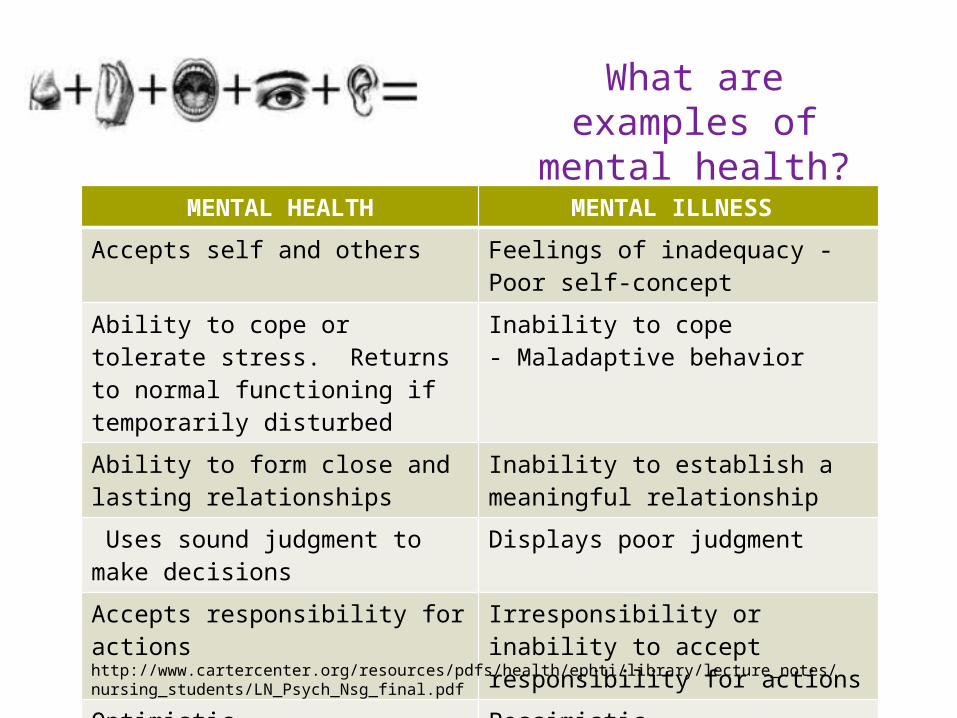
MENTAL HEALTH MENTAL ILLNESS
Accepts self and others Feelings of inadequacy - Poor self-concept
Ability to cope or tolerate stress. Returns to normal functioning if temporarily disturbed
Inability to cope- Maladaptive behavior
Ability to form close and lasting relationships
Inability to establish a meaningful relationship
Uses sound judgment to make decisions
Displays poor judgment
Accepts responsibility for actions Irresponsibility or inability to accept responsibility for actions
Optimistic Pessimistic
http://www.cartercenter.org/resources/pdfs/health/ephti/library/lecture_notes/nursing_students/LN_Psych_Nsg_final.pdf
What are examples of mental health?
+
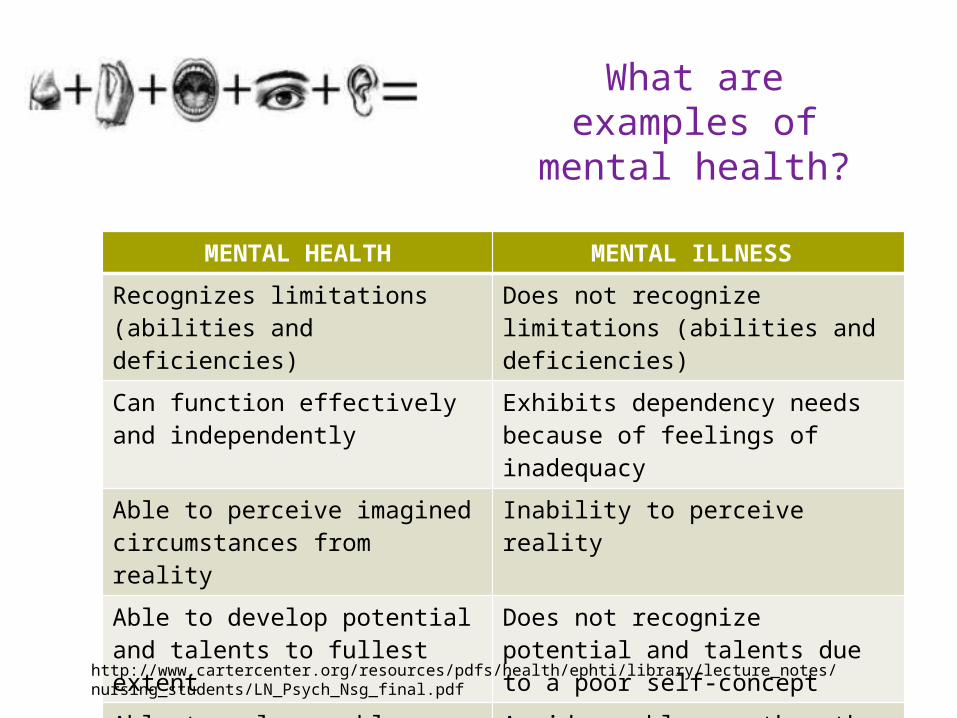
MENTAL HEALTH MENTAL ILLNESS
Recognizes limitations (abilities and deficiencies)
Does not recognize limitations (abilities and deficiencies)
Can function effectively and independently
Exhibits dependency needs because of feelings of inadequacy
Able to perceive imagined circumstances from reality
Inability to perceive reality
Able to develop potential and talents to fullest extent
Does not recognize potential and talents due to a poor self-concept
Able to solve problems Avoids problems rather than handling them or attempting to solve them
http://www.cartercenter.org/resources/pdfs/health/ephti/library/lecture_notes/nursing_students/LN_Psych_Nsg_final.pdf
What are examples of mental health?
+
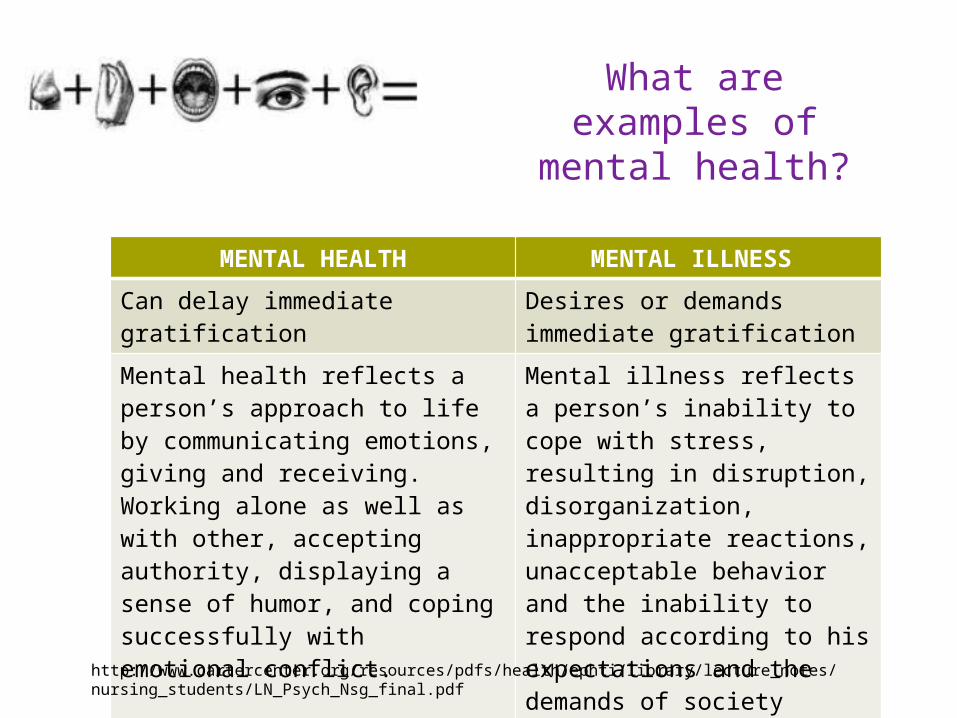
MENTAL HEALTH MENTAL ILLNESS
Can delay immediate gratification Desires or demands immediate gratification
Mental health reflects a person’s approach to life by communicating emotions, giving and receiving. Working alone as well as with other, accepting authority, displaying a sense of humor, and coping successfully with emotional conflict.
Mental illness reflects a person’s inability to cope with stress, resulting in disruption, disorganization, inappropriate reactions, unacceptable behavior and the inability to respond according to his expectations and the demands of society
http://www.cartercenter.org/resources/pdfs/health/ephti/library/lecture_notes/nursing_students/LN_Psych_Nsg_final.pdf
What are examples of mental health?
+
Teamwork Effective teamwork includes the active participation in
team decision making by all staff, including unlicensed mental health workers
Difference in treatment modalities
Mental health workers are often the ones who first recognize the need for intervention
+
Thoughtful communicationPositive feedback can be effective when communicating with patients about their behavior
Difference in tx modalities
Thoughtful communicationPatient are often used to negative feedback. At times patients will behave in ways to illicit negative feedback
+
Methodical observation Observation in psychiatry has at least two functions --
safety and assessment Three types of observation are common in psychiatry:
unit rounds observation of individual patients observation of the milieu as a whole
Difference in treatment modalities
+
Supportive interventions Help our patients learn effective ways of managing
their own behavior by acquiring skills that will be critical to their success when they return to the community
Difference in treatment modalities
+
Reference
Stanton, K., (2014) Psychiatric Nursing. Retrieved 9/6/14 https://nursing.advanceweb.com/CE/TestCenter/Content.aspx?CourseID=983&CreditID=1&CC=259047&sid=3415
+ S
Subjective
Mood How did patient cope? Exercise Medicine taken Sleep and appetite
?? ??
Maryann Ryan, MSN, APN, NP-C, PMHNP-BC
+ Subjective Triggers
Stress at work Stress at home Lack of sleep Negative Self Talk Relationship Problem Arguing Alcohol Consumption Poor diet Medicine not taken Ill health or pain Difficult life changes Workplace changes Change in treatment Change in General
Strategies for Wellness Adequate sleep Water Minimal Caffeine Minimal Alcohol Professional support Social Support Routine Day Managing Conflict Enjoyable activities Activities with others Time outside Positive thinking Looking outward
+Suicidal/Homicidal
Ideation
Suicide“Have you had thoughts that you would be better off dead, or that life is not worth living, of of hurting yourself, or ending your life?”Assess: Plan, Means and Duration
Asking about suicidal ideation does not increase the risk of an attempt.
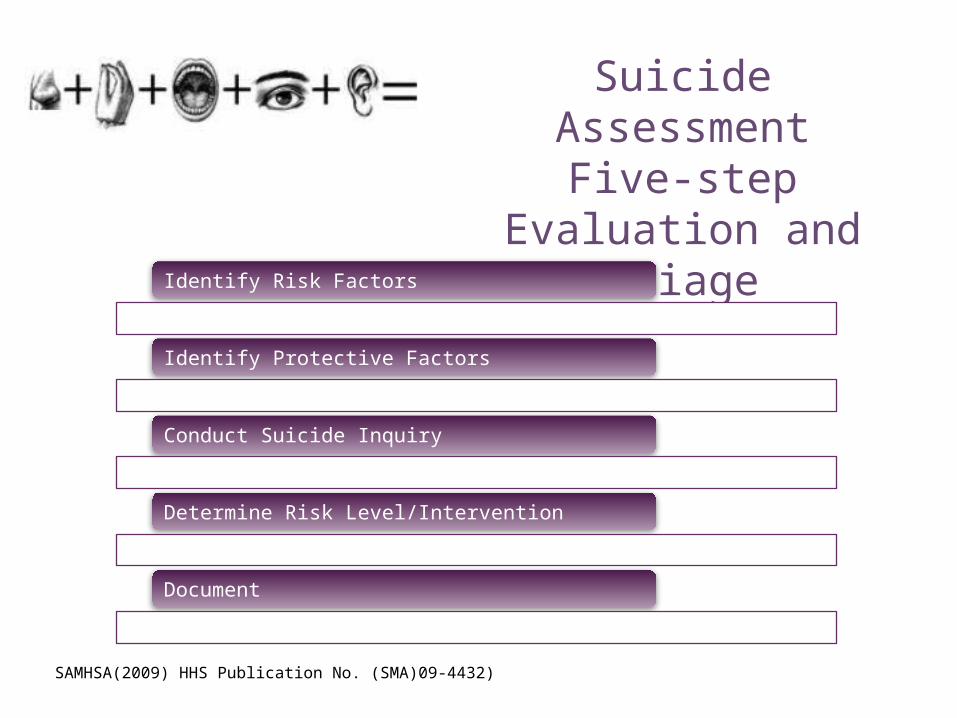
+ Suicide Assessment Five-step Evaluation
and Triage
Identify Risk Factors
Identify Protective Factors
Conduct Suicide Inquiry
Determine Risk Level/Intervention
Document
SAMHSA(2009) HHS Publication No. (SMA)09-4432)
+Suicide Severity Information/Trai
ningColumbia-Suicide Severity Rating Scale (C-SSRS)
Columbia University Medical Center
Center for Suicide Risk Assessment
Available at:
http://www.cssrs.columbia.edu/scales_practice_cssrs.html
+ O
Objective
Mental Exam
Maryann Ryan, MSN, APN, NP-C, PMHNP-BC
+ Consciousness
Disturbances of consciousness usually indicate organic brain impairment
Clouding
Stupor
LethargyComa
Alert A patient usually has fluctuations in the level of awareness of the enviornment with delirium
+ Appearance
Items
•Body Type•Grooming•Posture•Clothes•Hair•Nales
Ter
ms
•Healthy•Sick•Ill at ease•Poised•Old looking•Young looking•Disheveled•Childlike•Bizarre
Sig
ns of A
nxiety
•Moist hands•Perspiring•Tense posture•Wringing hands•Wide eyes
+ Speech
Qu
ality
•Talkative•Nonverbal•Unspontaneous•Normally responsive to cues
Rate
•Rapid •Slow•Pressured•Hesitant
Qu
ality
•Emotional•Dramatic•Monotonous•Mumbled•Whispered•Slurred
+ Mood/Affect
Mood•Depressed, sad, agitated, angry, irritable, euphoric, happy, guilty, hopeless
Affect•Flat•Constricted•Blunted•Appropriate or Not?
+
Mental Status Exam Elements
Available at: http://aitlvideo.uc.edu/aitl/MSE/msekm.swf
+
Thought Process
• Logical• Coherent• Incomprehensible
Thought Content
• Ideas• Beliefs• Preoccupations• Obsessions
AbnormalDelusions• Grandiose• Paranoid• SexualIllusions
+ Orientation
Pers
on • What’s your name? Pl
ace • Do you
know where you are?
• What kind of place is this?
Tim
e • Do you know what day it is? What season? What time it is?
• What year is it?
Impairment usually appears in this order (i.e., sense of time is impaired before sense of place); as the patient improves, the impairment clears in the reverse order.
+ Perception
HalluctionationsAuditory
VisualTasteSmell Tactile
When falling asleepWhen waking
up
Stressors involved
Have you heard voices or other sounds that no one else hears?
Have you experienced any strange sensations in your body that no one else sees?
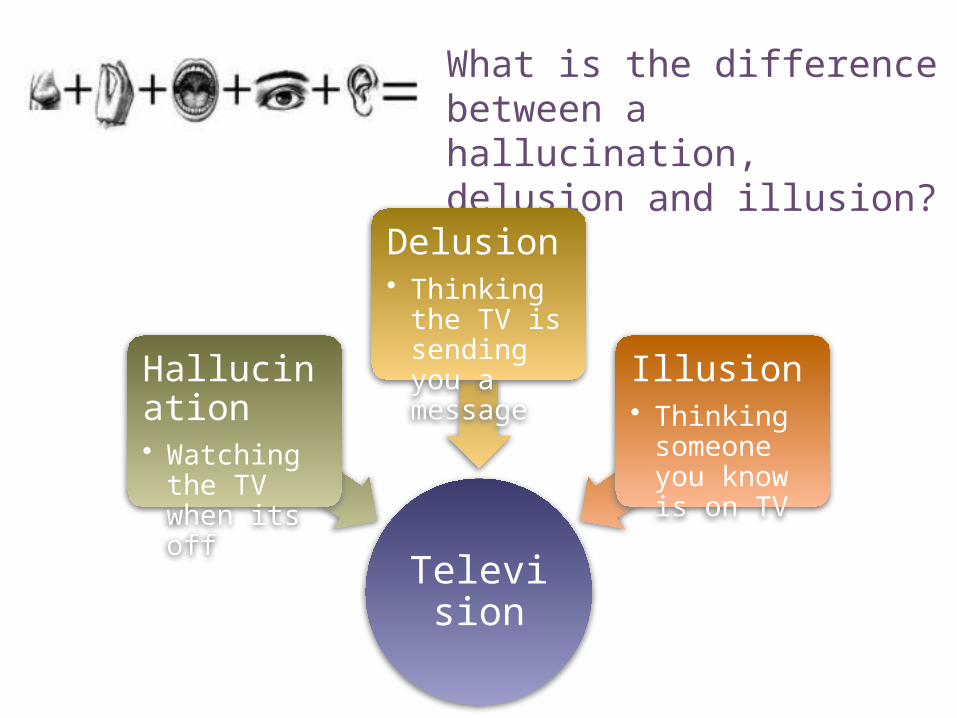
+ What is the difference between a hallucination, delusion and illusion?
Television
Hallucination• Watching the
TV when its off
Delusion• Thinking the
TV is sending you a message Illusion
• Thinking someone you know is on TV
+
When asked what she would do if she found a stamped, addressed envelope on the street, the patient replied, “Well I would open it of course and read what it said. Maybe there would be money in it.”
Does the patient understand the likely outcome of their
Behavior? Are they influence by this understanding?
Can the patient imagine what she would do in imaginary
situations?
Judgement
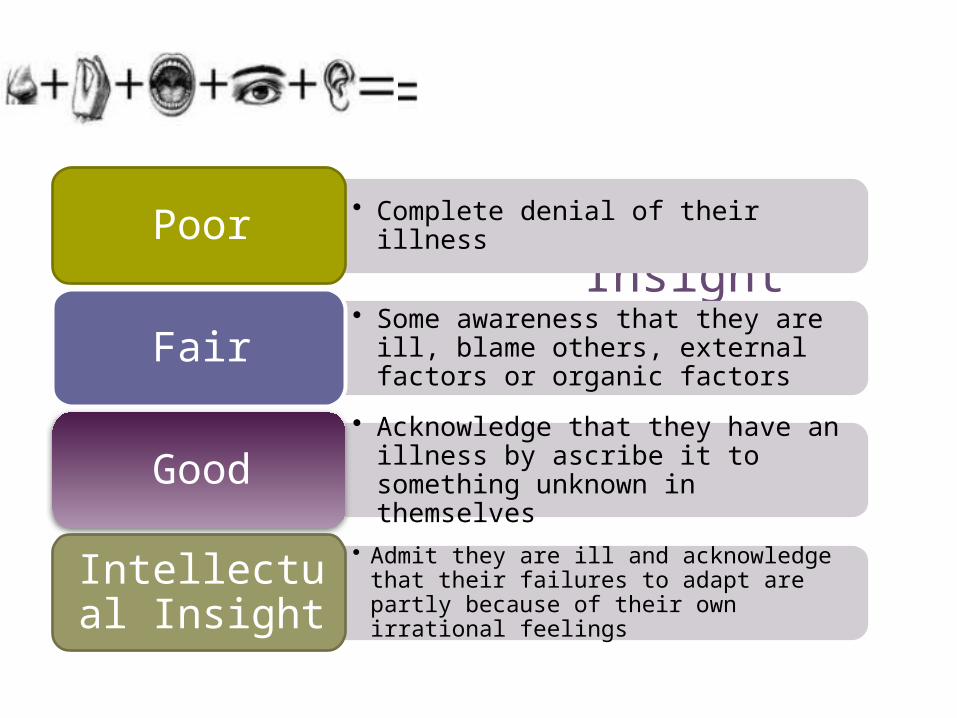
+ Insight
• Complete denial of their illnessPoor
• Some awareness that they are ill, blame others, external factors or organic factorsFair
• Acknowledge that they have an illness by ascribe it to something unknown in themselves
Good
• Admit they are ill and acknowledge that their failures to adapt are partly because of their own irrational feelings
Intellectual Insight
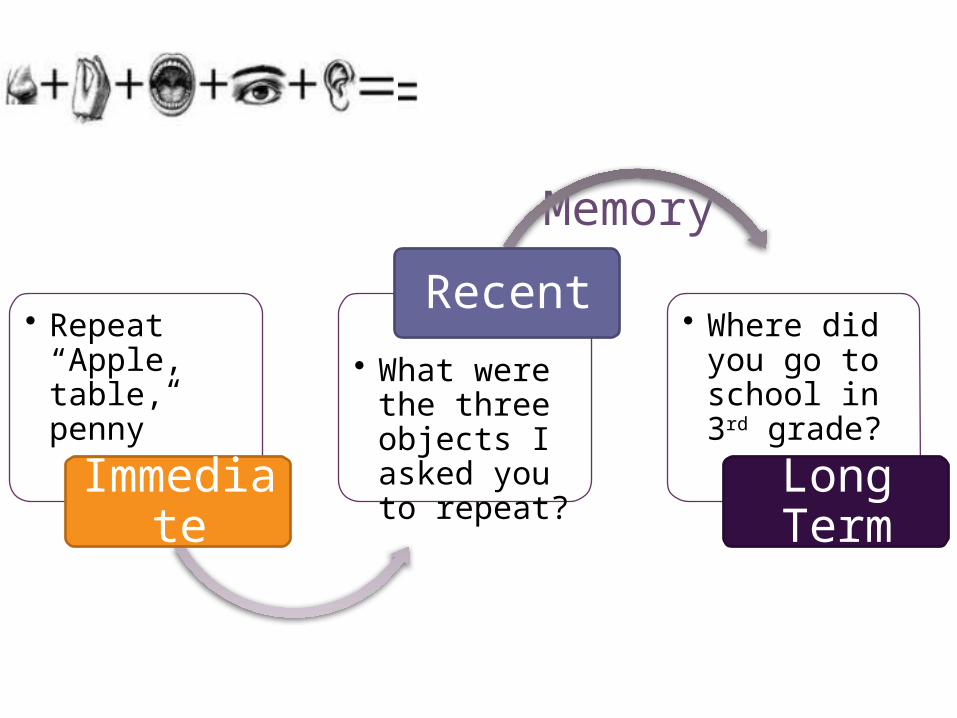
+ Memory
• Repeat “Apple, table, penny”
Immediate
• What were the three objects I asked you to repeat?
Recent• Where did you
go to school in 3rd grade?
Long Term
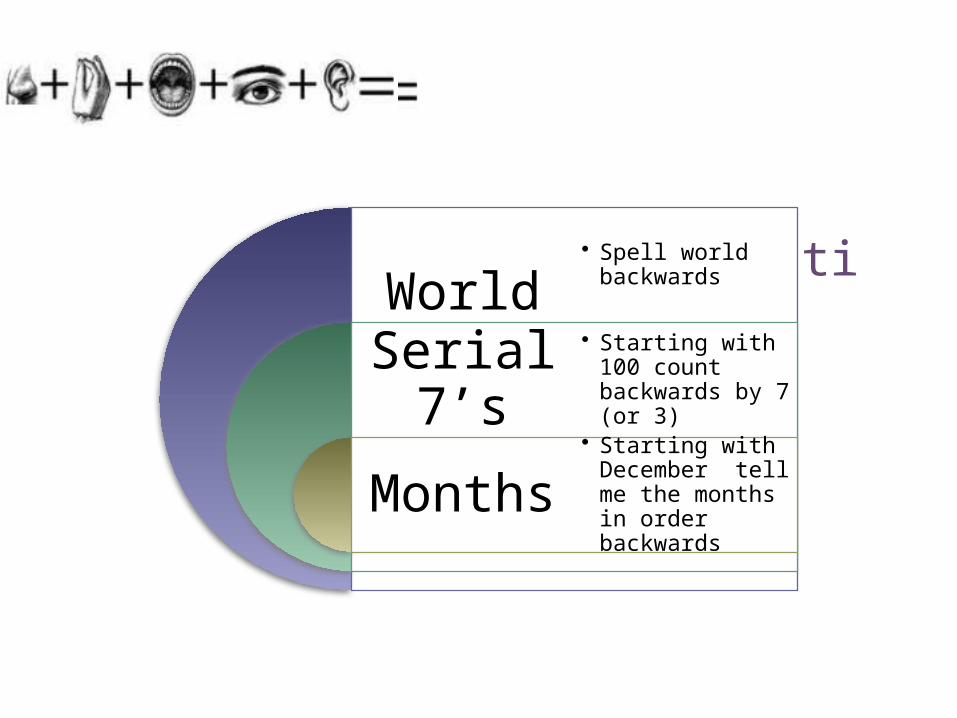
+ Concentration
World
Serial 7’s
Months
• Spell world backwards
• Starting with 100 count backwards by 7 (or 3)
• Starting with December tell me the months in order backwards
+
Read this Sentence.
+ Abstract Thinking
Very Concrete“Glass can
break easily”
Overly abstract“houses are a good thing for
anyone”
What does People who live in Glass houses should not throw stones mean?
+ Write a sentence
+
References Sadock, B. J., & Sadock, V. A. (2007). Kaplan and Sadock's: Synopsis of
psychiatry (10th ed.). Philadelphia: Lippincott, Williams, & Wilkins.
+
Maryann Ryan, MSN, APN, NP-C, PMHNP-C
Therapeutic Communication
+
Hildagard Peplau
Known as the mother of psychiatric nursing, Peplau introduced the "nurse-patient relationship" idea 40 years ago. This was at a time when patients did not actively participate in their own care.
http://media01.commpartners.com/PCNA/pcna_hilda_peplau.html
Nurse Patient Relationship
+
The nurse-client relationship is the foundation on which psychiatric
nursing is established.
The therapeutic interpersonal relationship is the process by which
nurses provide care for clients in need of psychosocial intervention.

+
Therapeutic relationships are:• goal- oriented • directed at learning
and growth promotion.
• patient is the primary focus of the interaction
+
Nurses must possess:
self-awareness
• Beliefs• Thoughts• Motivations• Biases• Limitations • recognizing how they
affect others.
Therapeutic Use of Self
The ability to use one’s personality consciously and in full awareness in an attempt to establish relatedness and to structure nursing interventions.
+
Requirements for Therapeutic Relationship
+
In analyzing patient-nurse communication, nonverbal behaviors and gestures are communicated first. If a patient’s verbal and nonverbal communications are contradictory, priority should be given to the nonverbal behavior and gestures.
TYPES OF COMMUNICATION
Nonverbal
Verbal
+
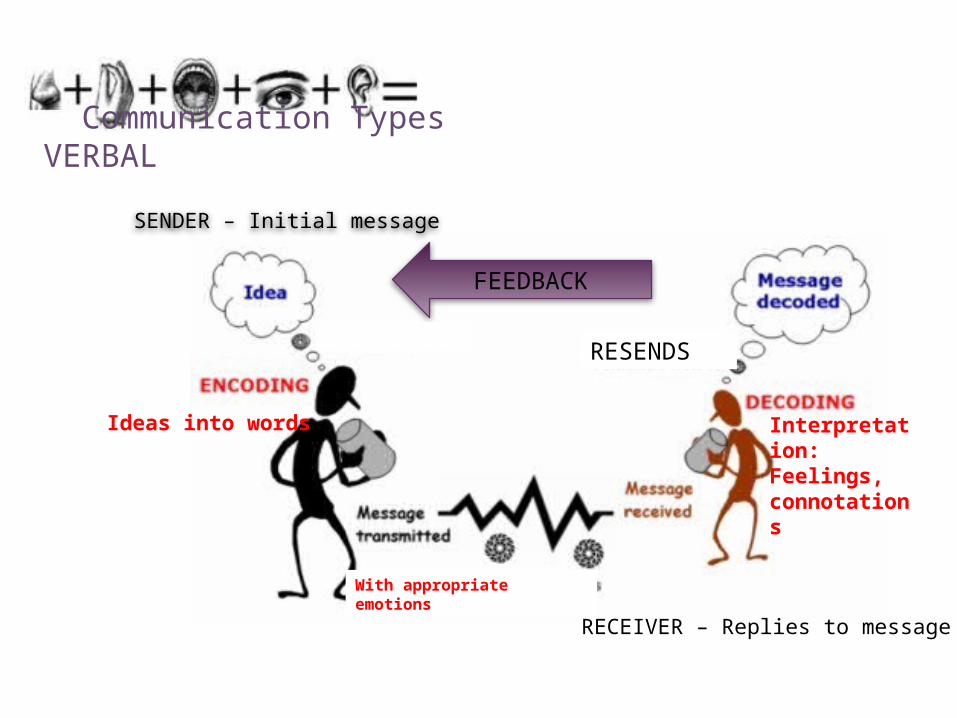
Communication Types VERBAL
SENDER – Initial message
FEEDBACK
RECEIVER – Replies to message
Ideas into words Interpretation:Feelings, connotations
With appropriate emotions
RESENDSRESENDS
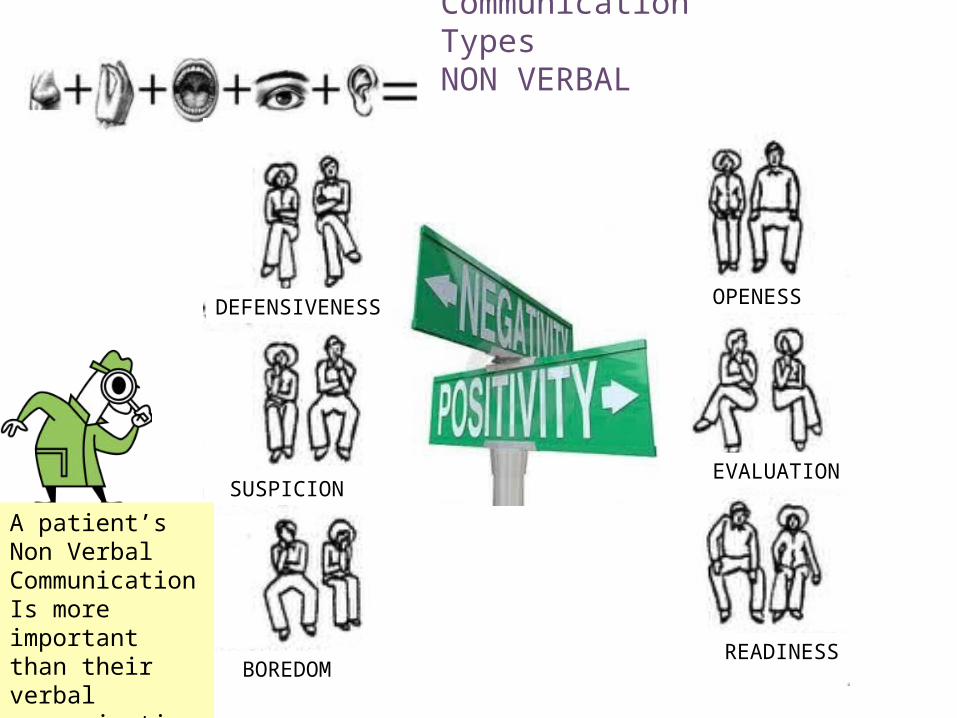
+ Communication Types NON VERBAL
SUSPICION
DEFENSIVENESS
BOREDOM
OPENESS
EVALUATION
READINESS
A patient’s Non VerbalCommunicationIs more important than their verbal communication
+
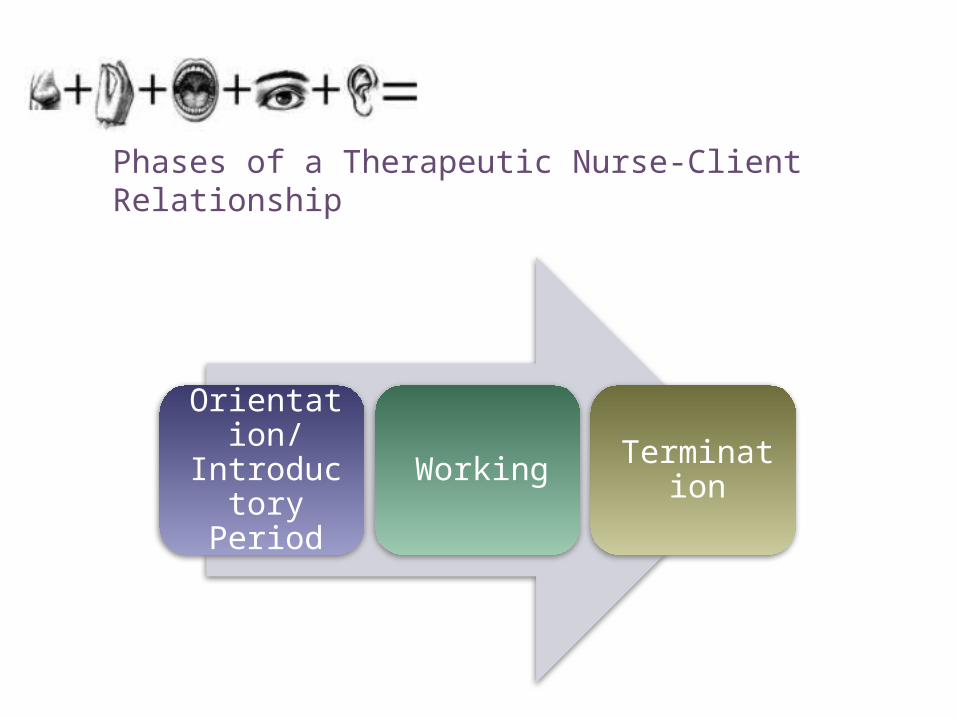
Phases of a Therapeutic Nurse-Client Relationship
Orientation/Introductor
y PeriodWorking Termination
+
Nontherapeutic Communication Techniques
Giving reassurance
Rejecting
Approving or disapproving
Agreeing or disagreeing
Using denial
Interpreting
Introducing an unrelated topic
+
Nontherapeutic Communication Techniques
Giving advice
Probing
Defending
Requesting an explanation
Indicating the existence of an external source of power “not their fault”
Belittling feelings expressed
Making stereotyped comments, clichés, and trite expressions
+ Example Non Therapeutic Communication
http://www.youtube.com/watch?v=ZarN-cEkrRs
+
Therapeutic Communication Techniques
+
Therapeutic Communication Techniques
Offering general leads - encourages client to continue
Placing the event in time or sequence - clarifies the relationship of events in time
Making observations - verbalizing what is observed or perceived
Encouraging description of perceptions - asking client to verbalize what is being perceived
Encouraging comparison - asking client to compare similarities and differences in ideas, experiences, or interpersonal relationships
+
Therapeutic Communication Techniques
Restating - lets client know whether an expressed statement has or has not been understood
Reflecting - directs questions or feelings back to client so that they may be recognized and accepted
Focusing - taking notice of a single idea or even a single word
Exploring - delving further into a subject, idea, experience, or relationship
Seeking clarification and validation - striving to explain what is vague and searching for mutual understanding
+
Therapeutic Communication Techniques
Presenting reality - clarifying misconceptions that client may be expressing
Voicing doubt - expressing uncertainty as to the reality of client’s perception
Verbalizing the implied - putting into words what client has only implied
Attempting to translate words into feelings - putting into words the feelings the client has expressed only indirectly
Formulating plan of action - striving to prevent anger or anxiety escalating to unmanageable level when stressor recurs
+ Example Therapeutic Communication
http://www.youtube.com/watch?v=AlFDgEFYcVw
+Listening to the Patient
Sit squarely facing the client
Observe an open posture
Lean forward toward the client
Establish eye contact
Relax
+
References Epstein RM, Borrell F, Caterina M . Communication and mental health in primary care. In New
Oxford Textbook of Psychiatry (Edrs. Gelder MG, López-Ibor JJ, Andreasen NC), Oxford University Press, 2000.
+
Maryann Ryan, MSN, APN, NP-C, PMHNP-C
Cultural Considerations
Therapeutic Communication
+DID YOU KNOW?
Writing a persons name in red ink means you are dead in the Korean culture?
Some Asian cultures may think you are trying to kill them if you offer a cold glass of water?
IKEA somehow agreed upon the Name “FARTFULL” for one of its new desks?
Pepsodent tried to sell its toothpaste in southeast Asia by emphasizing that it “whitens your teeth.” They found out that the local natives chew betel nuts to blacken their teeth, which they find attractive.
Kellogg had to rename its Bran Buds cereal in Sweden when it discovered that the name roughly translated to “Burned farmer”
When Pepsico advertised Pepsi in Taiwan with the ad “Come Alive With Pepsi” they had no idea that it would be translated into Chinese as “Pepsi brings your ancestors back from the dead.”
In Italy, a campaign for Schweppes Tonic Water translated the name into “Schweppes Toilet Water”.
+Rule #1 Guard against perceived similarities
Always observe closely
When we perceive others to be similar to us, we lack the sensitivity required to see differences that may exist.
Adjust your communication , both verbal and nonverbal, to better align with individuals in which you are communicating.
Treating people from different cultures the same as we treat others from our own culture may be inappropriate.
Our perceptions will blind us to cultural differences that we must adapt to in order to be effective in our communication.
+ Rule #2Guard against stereotypes
Stereotypes lock us into a way of thinking and treating others in a certain way.
Stereotypes alter our communication and may cause inappropriate behaviors.
Stereotypes cause us to behave in a certain way.
When we do this, we are unable to adjust our thinking and are not able to adjust our our behavior in a manner that would best “fit” the
situation.
Guard against unacceptable behavior that will stifle and hinder the opportunity to build positive cross cultural relationships.
+Rule #3 Recognize that Cultural Differences Exist
Recognize and adapt.
We then are able to monitor our own behavior in relation to what is most effective cross culturally.
Recognizing that people have different values and belief structures leads to a better understanding of those differences.
Recognition improves awareness, improved awareness improves our ability to adjust our behavior.
When we recognize that differences exist, adaptation can be made to improve communication.
Our ability to recognize cultural differences impacts our communication.
+Rule #4 Guard Against Judging Others
Judging impedes health interaction and is unproductive for all.
Judging diminishes our ability to understand and accept differences.
Therefore, take a non-judgemental approch in order to improve communication.
Judging others locks us into patterns of interaction based on what we think, in stead of what can be learned about others.
Recognizing cultural differences in adaptive and productive.
+Rule #5 Describe, evaluate, adjust
After describing what is around us, we can evaluate our plan of action.
By describing the culture around us, we begin to extend ourselves culturally.
By doing so we are more likely to adjust our communication activities to match those with whom we are communicating.
In order to communicate effectively cross culturally, we must first describe the culture.
This is part of “figuring things out” before we act in an unacceptable manner.
+HIPPA, Privacy, Confidentiality
and Social Media
Maryann Ryan, MSN, APN, NP-C, PMHNP-BC
+
Gossiping about something you’ve
overheard is rarely a good idea in healthcare.
+
Special Considerations in Mental Health
Staff/students are prohibited from confirming or denying
that a patient is on the psychiatric unit.
In public, staff/students are not allowed to acknowledge a
patient. If a patient approaches staff, it is okay to
engage in an appropriate conversation.
Engaging in a relationship with a mental health patient
can put you at risk for a conflict of interest, even if the patient initiates the contact.
+
Common Myths and Misunderstandings of Social Media
A mistaken belief that the communication or post is private and accessible only to the intended recipient.
A mistaken belief that content that has been deleted from a site is no longer accessible.
+How to Avoid Problems
Nurses are strictly prohibited from transmitting any information that may be reasonably anticipated to violate patient rights to confidentiality or privacy, or otherwise degrade or embarrass the patient.
Do not refer to patients in a disparaging manner, even if the
patient is not identified
Do not identify patients by name or post or publish information that may lead to the identification of a patient.
Do not take photos or videos of patients on personal devices,
including cell phones.
Nurses have an ethical and legal obligation to
maintain patient privacy and
confidentiality at all times.
+How to Avoid Problems
Use caution when having online social contact with patients or former patients.
Do not share information given by patients on line.
The nurse has the obligation to establish, communicate and enforce professional boundaries with patients in the online environment.
The fact that a patient may initiate contact with the nurse does not permit the nurse to engage in a
personal relationship with the patient.
Maintain professional boundaries in the use of
electronic media
+
Maryann Ryan, MSN, APN, NP-C, PMHNP-BC
Additional Legal Issues in
Mental Health
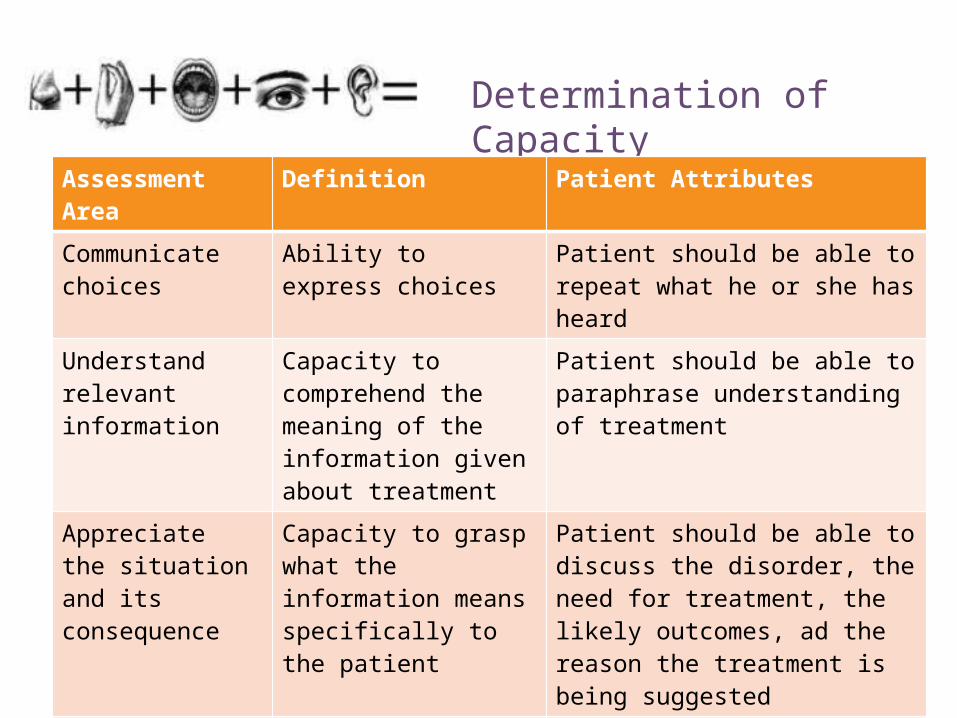
+Determination of Capacity
Assessment Area Definition Patient Attributes
Communicate choices
Ability to express choices Patient should be able to repeat what he or she has heard
Understand relevant information
Capacity to comprehend the meaning of the information given about treatment
Patient should be able to paraphrase understanding of treatment
Appreciate the situation and its consequence
Capacity to grasp what the information means specifically to the patient
Patient should be able to discuss the disorder, the need for treatment, the likely outcomes, ad the reason the treatment is being suggested
Use a logical thought process to compare the risks and benefits of treatment options
Capacity to reach a logical conclusion consistent with the starting premise
Patient should be able to discuss logical reasons for the choice of treatment
+
Duty to Warn
Health care providers are legally obligated to breach confidentiality. When there is a judgment that the patient has harmed any person or is about to injure someone, professional are mandated by law to report it to authorities.
+
Involuntary Commitment
Involuntary commitment Is the confined hospitalization of a person without the
person’s consent but with a court order. There are three common elements:
1. Mentally disordered2. Dangerous to self or others3. Unable to provide for basic needs “gravely disabled”
+Least restrictive environment
Least restrictive environmentAn individual cannot be restricted to an institution when
they can be treated in the community.Medication cannot be given unnecessarily.An individual cannot be restrained or locked in a room
unless ALL other “less restrictive” interventions have been tried first.
+
Maryann Ryan, MSN, APN, NP-C, PMHNP-BC
Behavioral Management of
Aggression
+
Management of Agitation and Aggression
•Most patients with mental disorders are not aggressive.
•Evidence does point to increased risk for violence among individuals with a
mental disorder as compared to the general
population.
+
Anger, Agitation, and Aggression
Anger is the emotional response to a perceived grievance which may be real or imagined.
Agitation refers to the unpleasant state of arousal with increased tension and irritability which can lead to hyperactivity, confusion and outright hostility
The spiral of anger and escalating agitation can lead to aggressive behavior.
+What are the risk factors?
History of violence Chemical Withdrawal
Pain Chronic fatigue
Diagnoses• Delirium• Dementia• personality
disorders• mania• substance abuse
What is the most important Risk factor to assess for?
History of violence
+ What are the risk factors?
Response to internal stimuli
• Psychosis• delusions
• hallucinations
Medication issues • Frequent changes• Non-compliance
Changes in environment Long waiting and feelings that no one is paying to attention to one’s needs
Psychosocial stressors• Illness
• Financial• health concerns
• relationship issues• feelings of intimidation
and loss of control
+ What are the risk factors?
Response to internal stimuli • Psychosis• delusions
• hallucinations
Medication issues • Frequent changes• Non-compliance
Long waiting and feelings that no one is paying to attention to one’s
needs
Psychosocial stressors• Illness
• Financial• health concerns
• relationship issues• feelings of intimidation and loss
of control
+ Recognize and prevent through awareness and assessment…
Facial expressions
• Glaring eyes• Clenched
teeth• Red face
Body Stance
• Tensed muscles
• Clenched fists
Physiologic Changes:
• Sweating• Shallow or
heavy breathing
• Tremors
Observational cues and behaviors associated with anxiety/tension
+ Recognize and prevent through awareness and
assessment…
Speech:
• Loud• Forceful• Cursing• Threatening• repetitive questions• Sarcastic• Challenging
Actions:
• Restlessness• Pacing• Fist Pounding• Refusal to follow
direction
Observational cues and behaviors associated with anxiety/tension
+
Understand the underlying issues motivating anger
Fear Frustration Feelings of Intimidation
Feelings of loss of control
Feelings of intolerable
anxiety
+
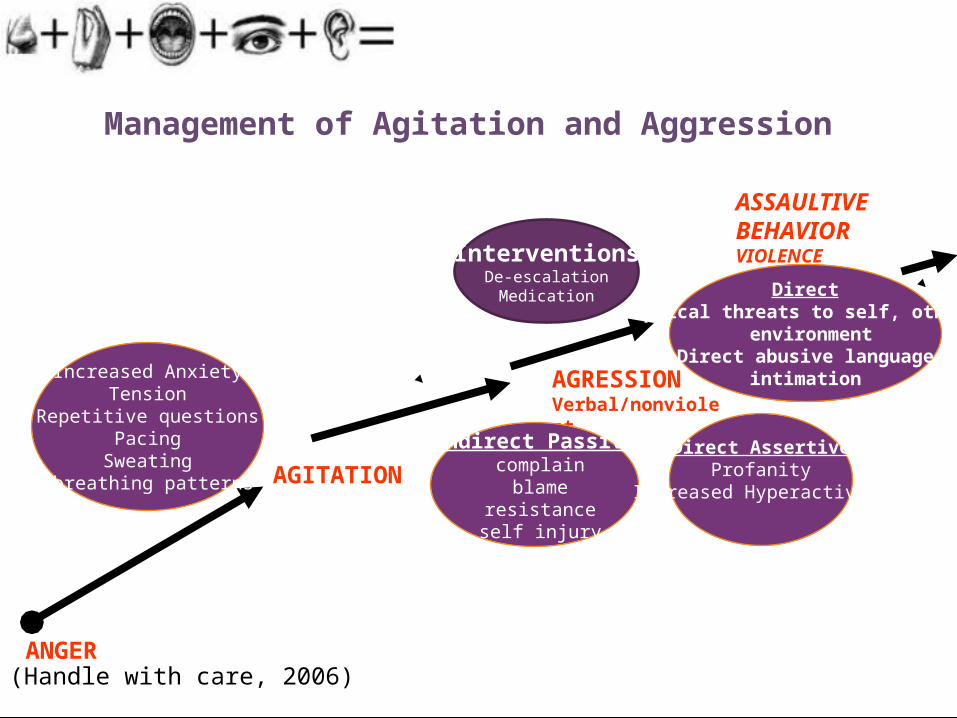
(Handle with care, 2006)
Management of Agitation and Aggression
ANGER
AGITATION
InterventionsDe-escalation
Medication
Increased AnxietyTension
Repetitive questionsPacing
Sweating breathing patterns
AGRESSION Verbal/nonviolent
Indirect Passive complain
blame resistance self injury
Direct AssertiveProfanity
Increased Hyperactivity
ASSAULTIVE BEHAVIOR VIOLENCE
DirectPhysical threats to self, others,
environmentDirect abusive language
intimation
+
Separate agitated person from other patients
Allow the patient to see staff presence
Minimize environmental stimuli
Maintain a safe distance • At least two arm’s
length• Off to the side
Assume a non-threatening stance Maintain eye contact
Safety, Safety, Safety…….
+
Aggression and Violence in Health Care
Although workplace violence occurs in all work environments, the health industry is particularly prone, especially in the areas of behavioral health and emergency departments.
Nurses and healthcare professionals need to recognize the behaviors of both the perpetrators and themselves in order to effectively de-escalate potential patient aggression and violence.
+
Elements of Supportive Interventions
• Allow person to vent feelingsListen
• And consider the validity of the feelingsAccept
• On one issue at a timeFocus
• AssertivenessEncourage
• Choices that the patient can makeOffer Alternatives
• With and persuade the individual to agree on course of appropriate action.Contract
+ References
Chapman, R., Perry, L., Styles, I., & Combs, S. (2009, March). Predicting patient aggression against nurses in all hospital areas. British Journal of Nursing, 18, (8) 476, 478 – 83.
Cowin, L., Davies, R., Berlin, T., Fitzgerald, M, & Hoot, S. (2003). De-escalating aggression and violence in the mental health setting. International Journal of Mental Health Nursing, 12 (64-73).
Handle with Care® (2006). Instructor Manual: Gardiner, NY.
Rippon, T. J. (2000). Aggression and violence in health care professions. Journal of Advanced Nursing, 31 (2), 452-460.
Zernicke, W. (1998). Patient aggression in general hospital setting: do nurses perceive it to be a problem? International Journal of Nursing Practice.
+Safety Tips
Be aware of your environment
Always know where the exit is
Keep your eyes on the patient
Know your patient: History of violence? Recent threats? Recent problems with patient on unit? Incarceration? Command hallucinations?
Keep more than an arms length between yourself and a patient
Call for help if a situation begins to escalate
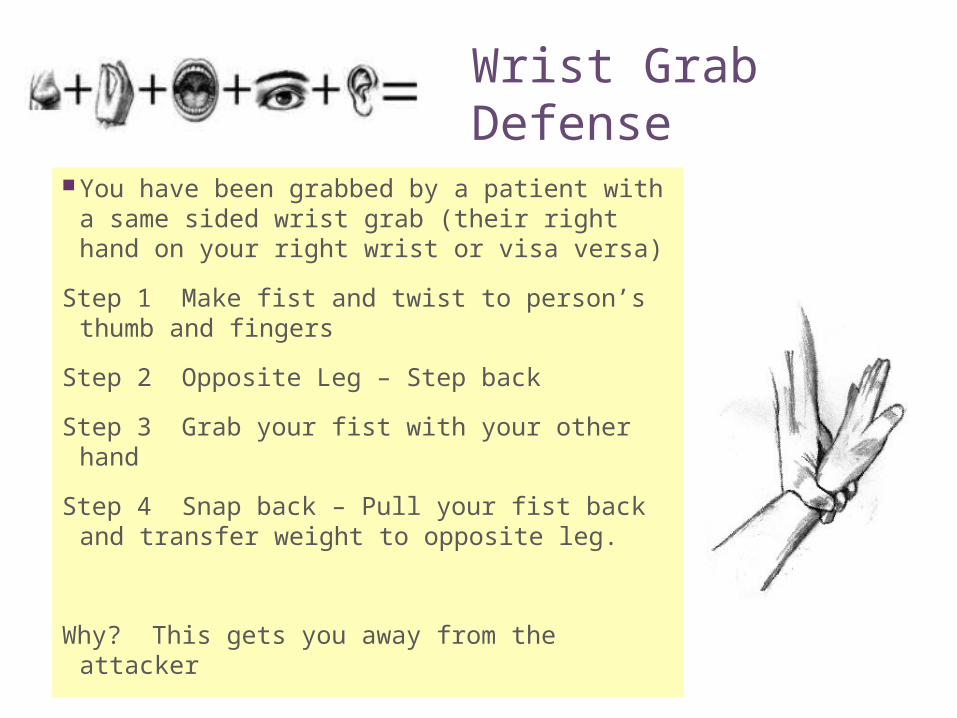
+ Wrist Grab Defense
You have been grabbed by a patient with a same sided wrist grab (their right hand on your right wrist or visa versa)
Step 1 Make fist and twist to person’s thumb and fingers
Step 2 Opposite Leg – Step back
Step 3 Grab your fist with your other hand
Step 4 Snap back – Pull your fist back and transfer weight to opposite leg.
Why? This gets you away from the attacker
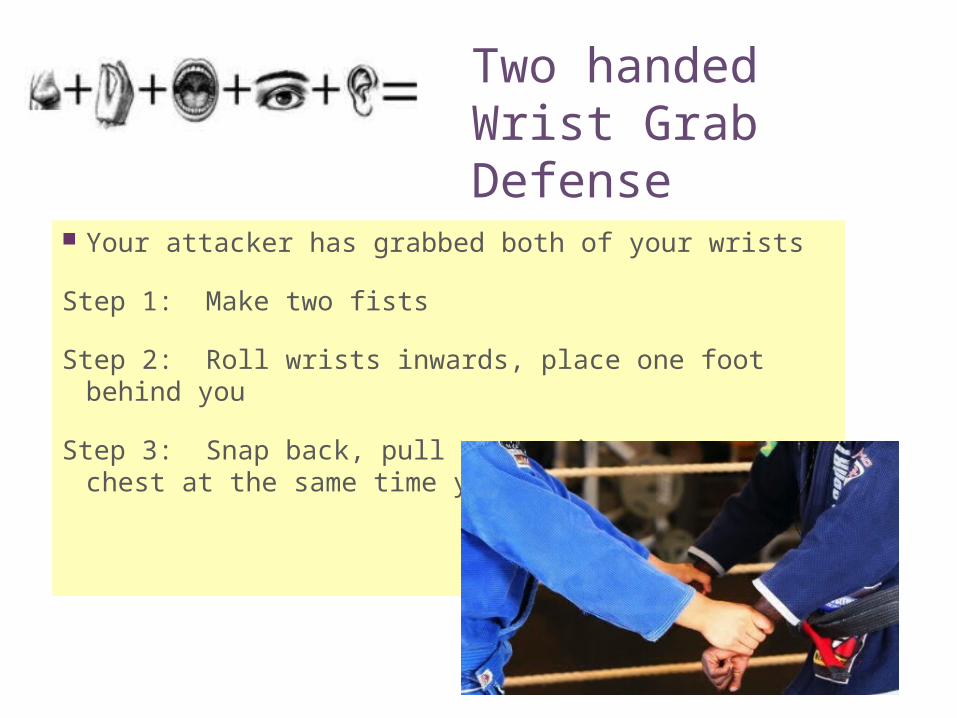
+ Two handed Wrist Grab Defense
Your attacker has grabbed both of your wrists
Step 1: Make two fists
Step 2: Roll wrists inwards, place one foot behind you
Step 3: Snap back, pull your wrists to your chest at the same time you step back
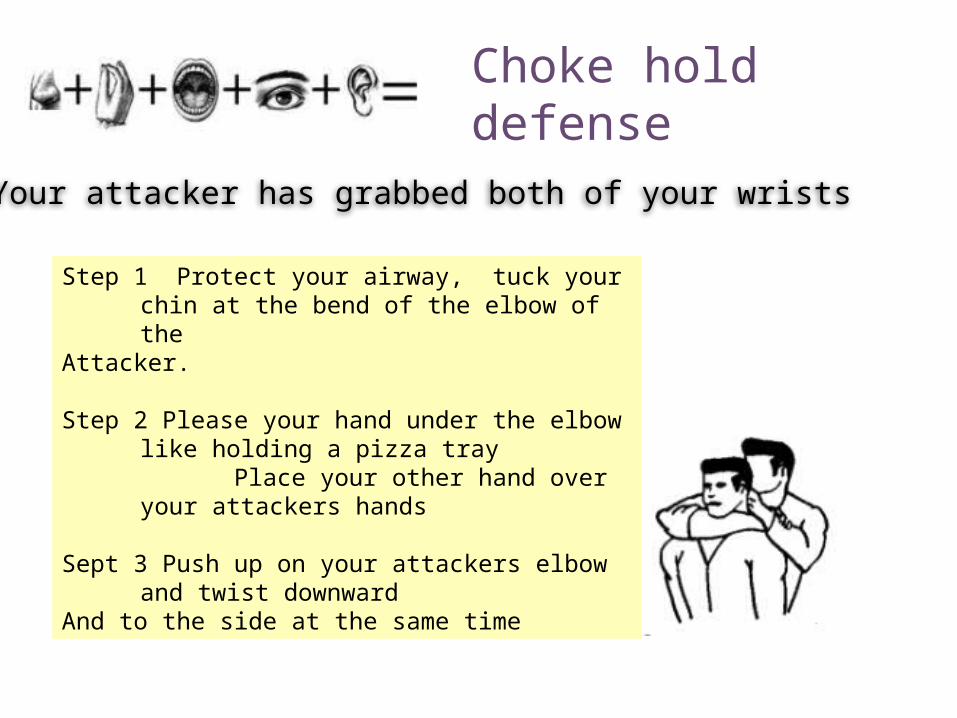
+ Choke hold defense
Your attacker has grabbed both of your wrists
Step 1 Protect your airway, tuck your chin at the bend of the elbow of the
Attacker.
Step 2 Please your hand under the elbow like holding a pizza tray
Place your other hand over your attackers hands
Sept 3 Push up on your attackers elbow and twist downward
And to the side at the same time
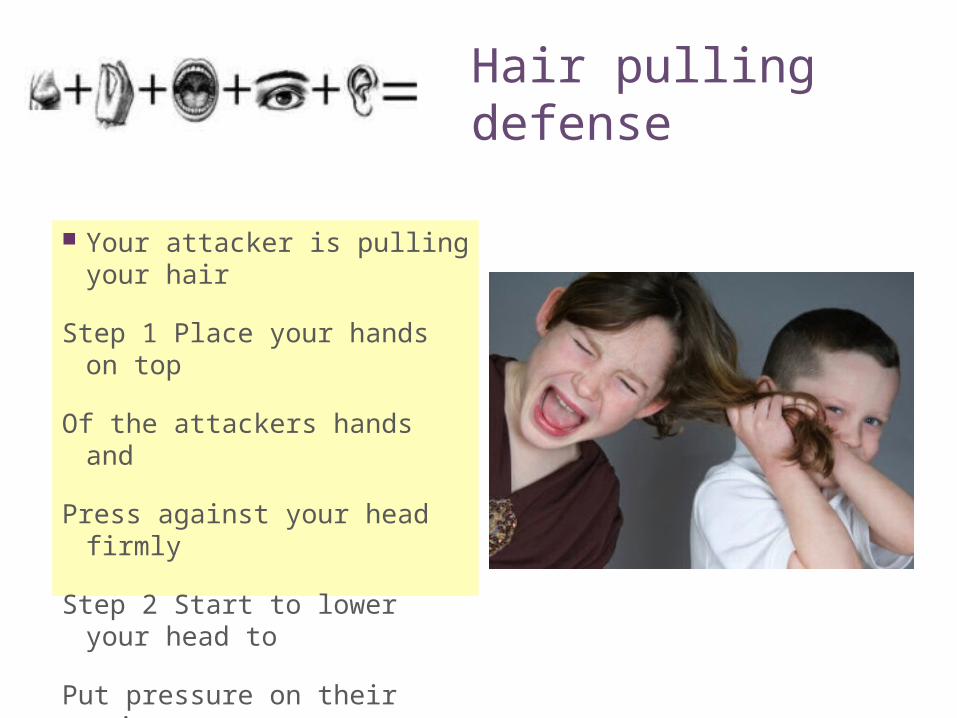
+ Hair pulling defense
Your attacker is pulling your hair
Step 1 Place your hands on top
Of the attackers hands and
Press against your head firmly
Step 2 Start to lower your head to
Put pressure on their wrist
+ Bite defense
An Attacker is biting you
Step 1 hold head to your bodyDon’t pull away
Step 2 Use the side of your handTo push up under the attacker’s nose
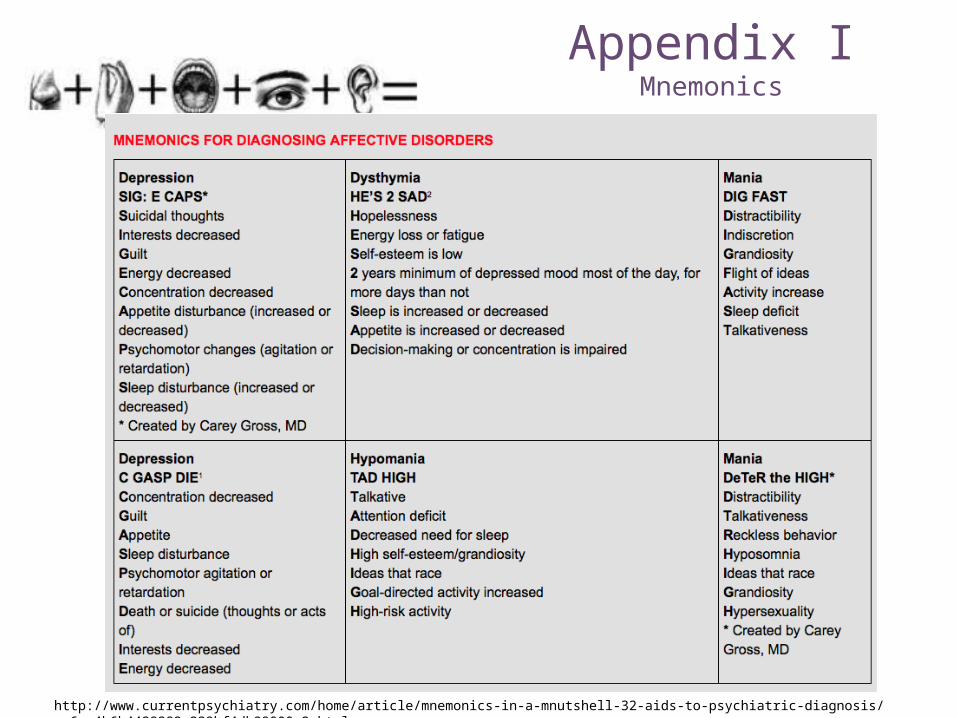
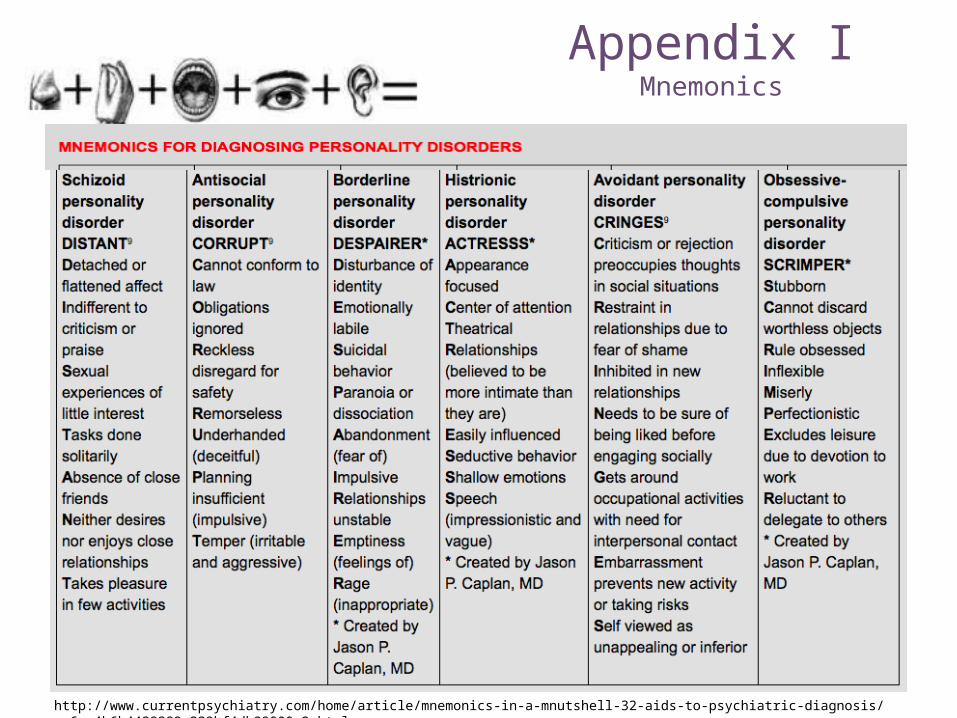
+ Appendix IMnemonics
http://www.currentpsychiatry.com/home/article/mnemonics-in-a-mnutshell-32-aids-to-psychiatric-diagnosis/ce6ce4b6b4429382a239bf4db99000c2.html
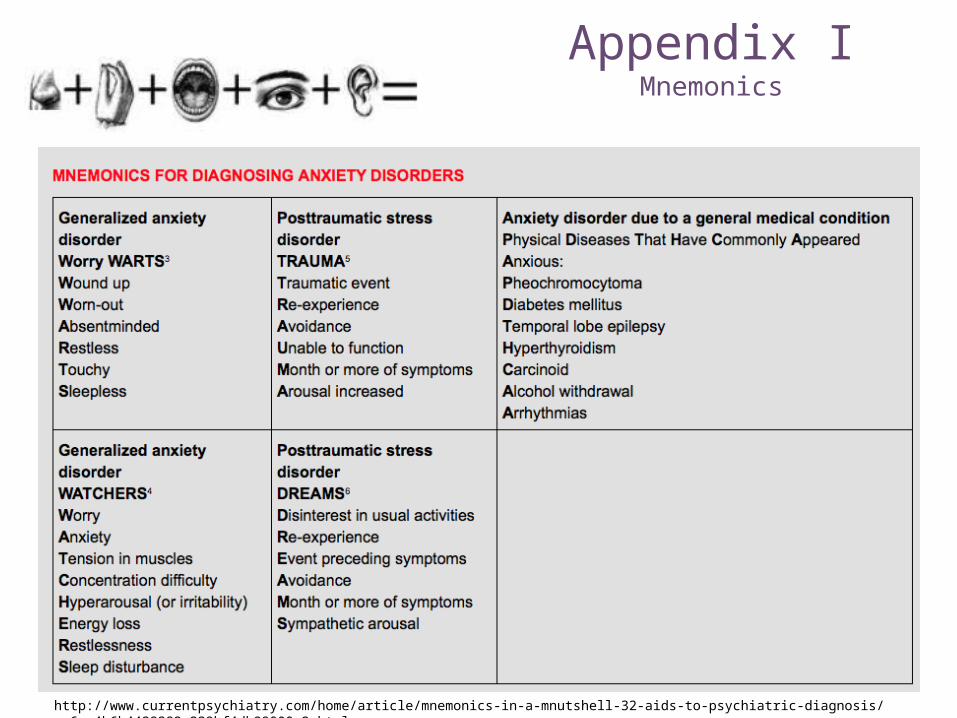
+ Appendix IMnemonics
http://www.currentpsychiatry.com/home/article/mnemonics-in-a-mnutshell-32-aids-to-psychiatric-diagnosis/ce6ce4b6b4429382a239bf4db99000c2.html
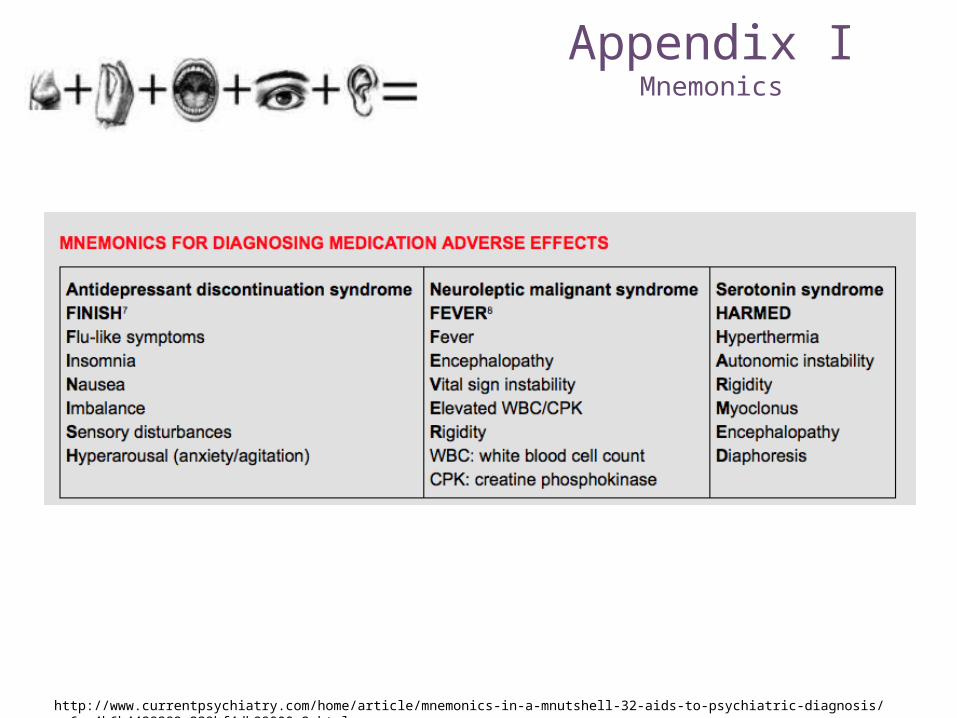
+ Appendix IMnemonics
http://www.currentpsychiatry.com/home/article/mnemonics-in-a-mnutshell-32-aids-to-psychiatric-diagnosis/ce6ce4b6b4429382a239bf4db99000c2.html
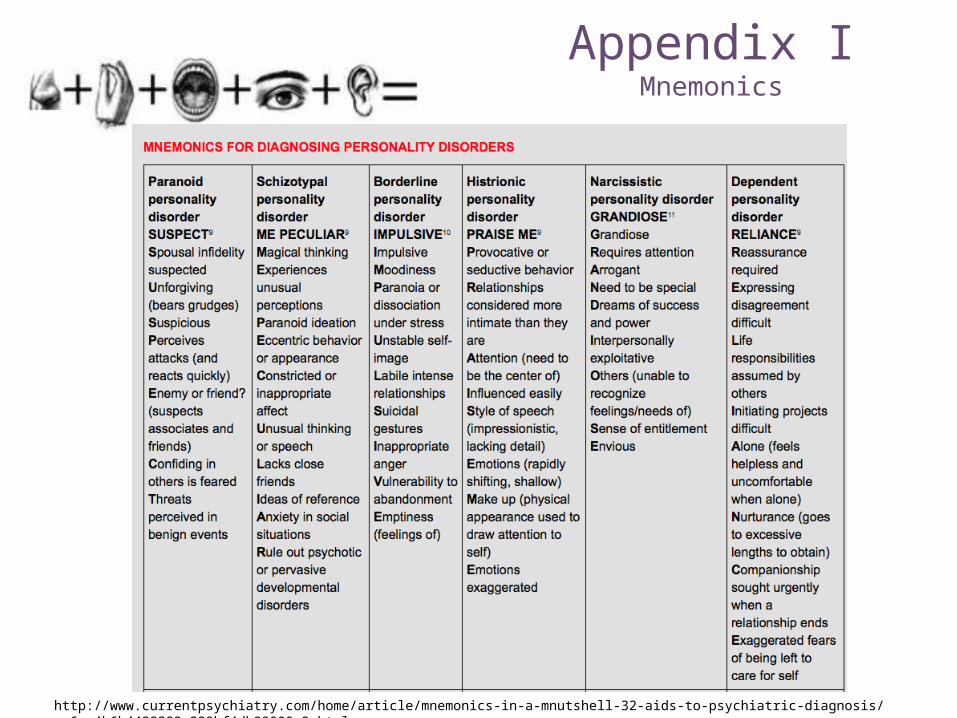
+ Appendix IMnemonics
http://www.currentpsychiatry.com/home/article/mnemonics-in-a-mnutshell-32-aids-to-psychiatric-diagnosis/ce6ce4b6b4429382a239bf4db99000c2.html
+ Appendix IMnemonics
http://www.currentpsychiatry.com/home/article/mnemonics-in-a-mnutshell-32-aids-to-psychiatric-diagnosis/ce6ce4b6b4429382a239bf4db99000c2.html
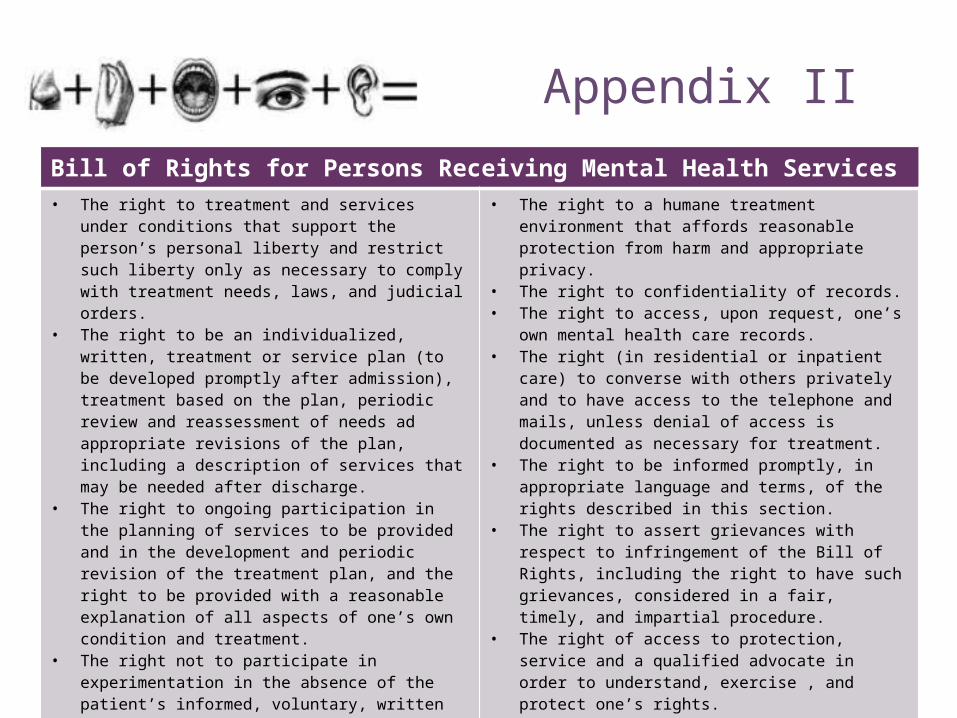
+Appendix II
Bill of Rights for Persons Receiving Mental Health Services• The right to treatment and services under conditions that
support the person’s personal liberty and restrict such liberty only as necessary to comply with treatment needs, laws, and judicial orders.
• The right to be an individualized, written, treatment or service plan (to be developed promptly after admission), treatment based on the plan, periodic review and reassessment of needs ad appropriate revisions of the plan, including a description of services that may be needed after discharge.
• The right to ongoing participation in the planning of services to be provided and in the development and periodic revision of the treatment plan, and the right to be provided with a reasonable explanation of all aspects of one’s own condition and treatment.
• The right not to participate in experimentation in the absence of the patient’s informed, voluntary, written consent, the right to appropriate protections associated with such participation, the right to an opportunity to revoke such consent.
• The right to freedom from restraints or seclusion, other than during an emergency situation.
• The right to a humane treatment environment that affords reasonable protection from harm and appropriate privacy.
• The right to confidentiality of records.• The right to access, upon request, one’s own mental health
care records.• The right (in residential or inpatient care) to converse with
others privately and to have access to the telephone and mails, unless denial of access is documented as necessary for treatment.
• The right to be informed promptly, in appropriate language and terms, of the rights described in this section.
• The right to assert grievances with respect to infringement of the Bill of Rights, including the right to have such grievances, considered in a fair, timely, and impartial procedure.
• The right of access to protection, service and a qualified advocate in order to understand, exercise , and protect one’s rights.
• The right to exercise the rights described in this section without reprisal, including reprisal in the form of denial of any appropriate, available treatment.
• The right to referral as appropriate to other providers of mental health services upon discharge.
From Title V of the Mental Health Systems Act [42 U.S.C. 9501 et seq.] Retrieved from http://www4.law.cornell.edu/uscode/42/10841.html
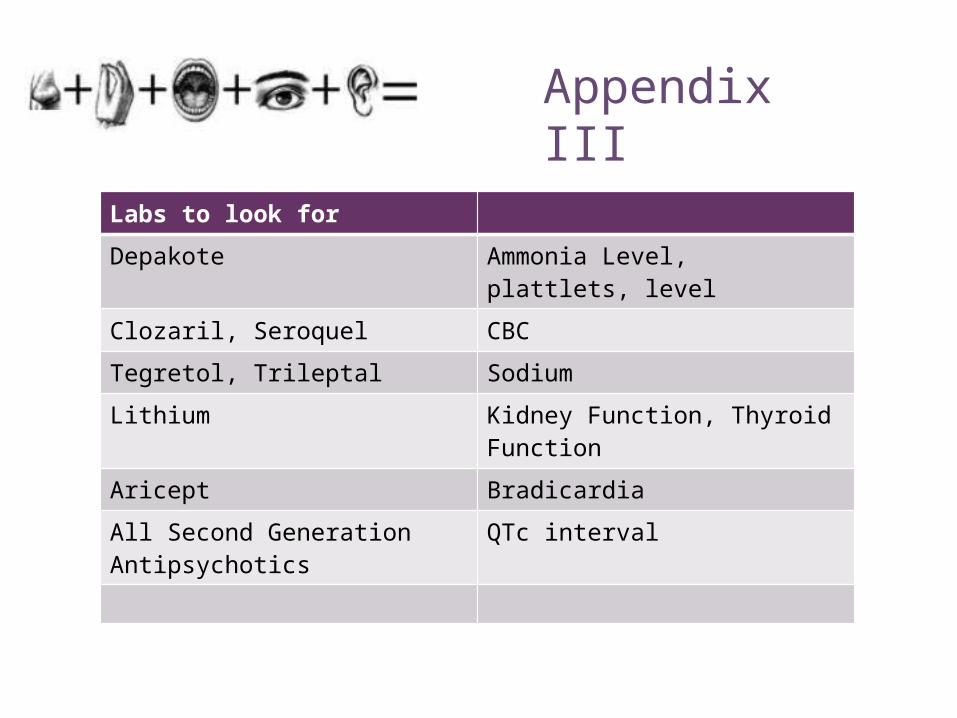
+Appendix III
Labs to look for
Depakote Ammonia Level, plattlets, level
Clozaril, Seroquel CBC
Tegretol, Trileptal Sodium
Lithium Kidney Function, Thyroid Function
Aricept Bradicardia
All Second Generation Antipsychotics
QTc interval