
1998;66:733-739 Ann Thorac SurgTerri-Ann Wattsman, Robert C. King, Curtis G. Tribble and Irving L. Kron
Patrick E. Parrino, Victor E. Laubach, John R. Gaughen, Jr, Kimberly S. Shockey, coronary flow
Inhibition of inducible nitric oxide synthase after myocardial ischemia increases
http://ats.ctsnetjournals.org/cgi/content/full/66/3/733on the World Wide Web at:
The online version of this article, along with updated information and services, is located
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 1998 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from

Inhibition of Inducible Nitric Oxide Synthase AfterMyocardial Ischemia Increases Coronary FlowPatrick E. Parrino, MD, Victor E. Laubach, PhD, John R. Gaughen, Jr, BA,Kimberly S. Shockey, MS, Terri-Ann Wattsman, MD, Robert C. King, MD,Curtis G. Tribble, MD, and Irving L. Kron, MDDivision of Thoracic and Cardiovascular Surgery, Department of Surgery, University of Virginia Health Sciences Center,Charlottesville, Virginia
Background. The role of nitric oxide synthase in myo-cardial ischemia–reperfusion injury is complex. Our hy-pothesis was that inducible nitric oxide synthase has arole in the regulation of coronary flow after ischemia.
Methods. Four groups of isolated blood-perfused rab-bit hearts underwent sequential periods of perfusion,ischemia, and reperfusion (20, 30, and 20 minutes). Twogroups underwent 40 minutes of perfusion. Ischemicgroups received saline vehicle, Nv-nitro-L-argininemethyl ester (L-NAME) or the highly specific induciblenitric oxide synthase inhibitor 1400W in low or highdoses during reperfusion. Two nonischemic groups weretreated with saline vehicle or 1400W during the last 20minutes of perfusion. Left ventricular developed pres-sure and coronary flow were measured after each perfu-sion period. Ventricular levels of myeloperoxidase andcyclic guanosine monophosphate were measured at theend of the second perfusion period.
Results. Coronary flow was significantly increased in
both 1400W groups versus L-NAME (p < 0.001) and inhigh-dose 1400W versus control (p < 0.001). Coronaryflow was not significantly different between the nonisch-emic groups. Left ventricular developed pressure was notsignificantly different among the ischemic groups orbetween the two nonischemic groups. There were nodifferences in cyclic guanosine monophosphate levels inany of the ischemic hearts. Myeloperoxidase levels weresignificantly elevated in L-NAME versus high-dose1400W, nonischemic 1400W, and nonischemic salinegroups (p < 0.02).
Conclusions. Highly selective inhibition of induciblenitric oxide synthase results in increased coronary flowafter ischemia but not after continuous perfusion. Thisoccurs with decreased neutrophil accumulation and atrend toward increased contractility without elevation ofcyclic guanosine monophosphate levels.
(Ann Thorac Surg 1998;66:733–9)© 1998 by The Society of Thoracic Surgeons
The role of nitric oxide synthase (NOS) and its prod-uct, nitric oxide (NO), in myocardial ischemia–
reperfusion injury is complex and has not been clearlydefined. Many studies that demonstrate a beneficial rolefor NO after ischemia–reperfusion use either the sub-strate for NOS (l-arginine), a NOS inhibitor, or both[1–5]. Other studies use the same substrate or inhibitorand report a contrary response [6–9]. Data from differentstudies that often seems contradictory may be explained,in part, by a bimodal effect of NO that is the result of thetiming of administration of either inhibitors or substrate.Defining a clear role for NOS has been further compli-cated by the elucidation of three different isoforms ofNOS: endothelial NOS (eNOS), inducible NOS (iNOS),and neuronal NOS. In the heart, NO is produced underbasal conditions predominantly by eNOS. After appro-
priate stimulus (lipopolysaccharide, interleukin-1b, tu-mor necrosis factor-a, interferon-g, interleukin-6, andischemia) cardiac myocytes, microvascular endothelium,endocardial endothelial cells, and vascular smooth mus-cle cells, as well as certain inflammatory cells (macro-phages, neutrophils), may also express iNOS in a time-dependent fashion [10, 11]. Neuronal NOS is thought toplay a relatively minor role in the generation of NO in theheart [10].
An additional factor that has made the role of NOSafter ischemia–reperfusion difficult to sort out is the lackof specific inhibitors for the various isoforms. Commonlyused inhibitors of NOS such as L-NAME (Nv-nitro-l-arginine methyl ester) and L-NMMA (NG-monomethyl-l-arginine) are l-arginine analogs that compete for bind-ing with l-arginine and lack specificity for any of theknown NOS variants.
We developed the hypothesis that both eNOS andiNOS have a role in the regulation of coronary flow afterischemia, and that selective inhibition of iNOS mightimprove postischemic myocardial function without com-promising the ability of the endothelium to synthesizeappropriate amounts of NO.
Presented at the Forty-fourth Annual Meeting of the Southern ThoracicSurgical Association, Naples, FL, Nov 6–8, 1997.
Address reprint requests to Dr Kron, Department of Surgery, Box 310,University of Virginia Health Sciences Center, Charlottesville, VA 22908(e-mail: [email protected]).
© 1998 by The Society of Thoracic Surgeons 0003-4975/98/$19.00Published by Elsevier Science Inc PII S0003-4975(98)00605-5
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from

Material and Methods
All protocols in this study were reviewed and approvedby the Animal Review Committee of the University ofVirginia. All animals received humane care in compli-ance with the “Principles of Laboratory Animal Care” asdescribed by the National Society for Medical Researchand the “Guide for the Care and Use of LaboratoryAnimals” (NIH publication 85-23, revised 1985). AdultNew Zealand white rabbits of either sex were usedthroughout this study.
Preparation of Donor Animal and Organ HarvestNew Zealand white rabbits (2.8 to 3.0 kg) were anesthe-tized with an intramuscular injection of xylazine (10 mg)and ketamine (100 mg); this was followed by placementof an ear vein catheter and a tracheostomy, and volumeventilation (12 mL/kg) with 100% oxygen was begun.Vecuronium bromide (0.2 mg) and 2,000 units of heparinsodium were administered intravenously. A sternotomywas performed and the aorta isolated. The inferior venacava was then transected, followed by a rapid aortotomyand insertion of a saline-filled stainless steel cannula,which was secured in place. The hearts were then quicklyexcised and immediately reperfused ex vivo in the Lan-gendorff mode.
Establishment of Perfusion and Baseline DataAll hearts were reperfused with oxygenated whole bloodfrom a support animal as described in detail by Mauneyand coworkers [12] (Fig 1). In brief, a support rabbit wasused to provide oxygenated blood through a perfusioncircuit to the isolated heart. This blood was filtered andwarmed (37°C) before passing an ultrasonic flow probe(Transonic Systems, Inc, Ithaca, NY) and entering thecannula. The perfusion pressure was a constant80 mm Hg, which is the normal physiologic perfusionpressure of the rabbit heart. Transfusion of blood from ablood-donor rabbit was used as needed to maintainadequate circulating blood volume in the support animal.All hearts were allowed to equilibrate during the first 10minutes of perfusion. At 10 minutes, pacing leads were
attached to the right ventricular free wall and the heartswere paced at 150 Hz. Subsequently, a left atriotomy wasmade and the mitral valve was gently disrupted. Asaline-filled latex balloon was then placed into the leftventricle for continuous measurement of left ventriculardeveloped pressure. Baseline data were collected for anadditional 10 minutes.
Experimental DesignSix groups of rabbits were studied. All groups underwentharvest, equilibration, and baseline data collection asdescribed above. Four groups were subjected to a 30-minute period of warm ischemia by occlusion of theaortic cannula and immersion in a warm saline bath(37°C). Hearts were not paced during this time. After thisinterval, the saline bath was drained, perfusion wasrestarted, and the hearts were again paced at 150 Hz.Simultaneously, infusion of drug or saline vehicle wasbegun. An infusion pump (syringe infusion pump 22;Harvard Apparatus, South Natick, MA) was connected toa side port in the aortic cannula and was used toadminister drug directly into the coronary circulation.The infusate was given at a constant rate of 0.25 mL/min.The hearts were reperfused for 20 minutes before re-moval from the apparatus. During reperfusion, effluentblood from the isolated heart was discarded and notreturned to the support animal, thus limiting drug expo-sure to the isolated heart only. After removal from theapparatus, the hearts were gently flushed with 20 mL ofnormal saline solution through the cannula, the rightventricular free wall and atria were dissected away, andthe left ventricle was immersed in liquid nitrogen. Thefrozen hearts were then stored at 280°C for later assay.Two groups of animals did not undergo warm ischemia;rather, after 20 minutes of equilibration, infusion of drugor vehicle was begun at the aforementioned rate. As inthe other four groups, 20 minutes of data were collectedbefore removal, flushing, trimming, and freezing. Theinfusates in the four ischemic groups consisted of salinevehicle, L-NAME (1 mg/min, Sigma Chemical Co, St.Louis, MO), low-dose 1400W (N-[3-(aminomethyl)ben-zyl] acetamidine, 5 mg/min, provided by Glaxo-WellcomeResearch, Hertfordshire, UK), and high-dose 1400W (50mg/min). Drugs were prepared in appropriate concentra-tions to allow a uniform infusion rate in all groups. Thedose of L-NAME was selected based on a previous studyin which a rabbit model was used to study the effect ofL-NAME on regional myocardial ischemia–reperfusion[13]. The dose of 1400W was chosen based on previouswork that examined the efficacy of 1400W in preventingvascular leakage caused by endotoxin [14]. In that study,the authors found a median effective dose ED50 of0.3 mg/kg in their study animals. In the present study, themass of the typical rabbit heart was approximately 10 g,resulting in a dose of 0.005 mg/heart. However, becausethe blood was not recirculated, this dose was used on aper minute basis to approximate the in vivo exposure ofthe heart to 1400W. The two nonischemic groups re-ceived saline vehicle or low-dose 1400W. Groups were
Fig 1. Schematic of the isolated, blood-perfused heart circuit. (Vent5 ventilator.)
734 PARRINO ET AL Ann Thorac SurgROLE OF iNOS IN POSTISCHEMIC CORONARY FLOW 1998;66:733–9
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from

defined according to the specific interventions that weremade (Table 1).
Data Acquisition During Reperfusion of IsolatedHeartsThroughout the 20-minute reperfusion period, data wereobtained from the in-line ultrasonic flow probe and theleft ventricular balloon. These continuous data werecollected and recorded by customized digital data acqui-sition software (Workbench PC; Strawberry Tree, Inc,Sunnyvale, CA) and allowed analysis of coronary flow(CF), left ventricular developed pressure, and the firstderivative of the left ventricular pressure.
Biochemical AssaysThe test hearts, which had been reduced to the leftventricle and quickly frozen in liquid nitrogen at the endof reperfusion, were stored at 280°C for later assay.Before assay, the hearts were removed from the freezer,crushed using a mortar and pestle on a bed of dry ice,and separated into 0.45- to 0.55-g samples. These sampleswere used to measure myeloperoxidase (MPO) activity andcyclic guanosine 39, 59 monophosphate (cGMP) levels.
Myeloperoxidase AssayTo elucidate the role of neutrophils in ischemia–reperfusion injury, MPO was studied as a marker ofneutrophil accumulation. Samples from all hearts wereused to determine MPO activity. The samples wereallowed to thaw and then were homogenized (Polytronmodel PCV 11, Kinnematica AG, Littau, Switzerland) in2.5 mL of 0.05 mol/L Na2PO4 at 4°C for 30 seconds. Thesamples were then centrifuged (Sorvall RC-5B refriger-ated superspeed centrifuge, DuPont Instruments, New-town, CT) at 4°C, the supernatant was discarded, and thepellet was resuspended in 2.5 mL of 0.5% HTAB (hexa-decyltrimethylammonium bromide). This solution washomogenized (Polytron model PCV 11) and sonicated(Bransonic ultrasonic cleaner 3210, Branson UltrasonicsCo, Danbury, CT) for 2 minutes at room temperature.The sample was then centrifuged (Sorvall RC-5B) at 4°Cfor 10 minutes and the supernatant removed. One tenthof a milliliter of the supernatant was then added to astock solution of H2O2 and ODD (o-dianisidine dihydro-chloride, Sigma) and placed immediately into the spec-trophotometer (LKB Biochrom model 4050, Cambridge,England), and the change in absorbance at 460 nmmeasured over 2 minutes. Myeloperoxidase activity isreported as change in absorbance per gram tissue (wetweight) per minute.
Determination of Myocardial cGMP ContentNitric oxide is known to activate the enzyme guanylylcyclase, which then catalyzes the production of cGMP[15]. As a second messenger for NO, cGMP exerts effectsdirectly on cGMP-sensitive ion channels and on cGMP-regulated cyclic adenosine 39, 59 monophosphate (cAMP)phosphodiesterases [16]. To evaluate tissue levels ofcGMP, samples from hearts in all six groups were ho-mogenized (Polytron model PCV 11) at 4°C in 5 mL of 6%trichloroacetic acid (J.T. Baker, Phillipsburg, NJ). Theywere then centrifuged (Sorvall RC-5B) for 15 minutes at4°C. The supernatant was then removed and washed fourtimes with ethyl ether (Fisher Scientific, Fair Lawn, NJ).The samples were then vacuum-dried at 60°C for 3 to 4hours. The resulting pellet was then resuspended in 1 mLof 0.1 N HCl, and the solution was subjected to radioim-
Table 1. Experimental Groups
Group Infusate
30-MinIschemicInterval
Control(n 5 7)
Saline vehicle Yes
L-NAME(n 5 8)
L-NAME (1 mg/min) Yes
LD 1400W(n 5 7)
Low-dose 1400W (5 mg/min) Yes
HD 1400W(n 5 7)
High-dose 1400W (50 mg/min) Yes
Non I 1400W(n 5 8)
Low-dose 1400W (5 mg/min) No
Non I Control(n 5 9)
Saline vehicle No
HD 5 high dose; LD 5 low dose; L-NAME 5 Nv-nitro-l-argininemethyl ester; Non I 5 Nonischemic; 1400W 5 N-[3-(aminomethyl)benzyl] acetamidine.
Table 2. Coronary Flow Before Intervention (Ischemia 1 Drug or Drug Alone), After 20 Minutes of PostinterventionPerfusion, and Percent Recoverya
GroupPreintervention CF
(mL/min)Postintervention CF
(mL/min)% CF
Recovery
Control (n 5 7) 6.70 6 0.56 7.69 6 1.13b 113.46 6 12.81L-NAME (n 5 8) 7.50 6 0.75 7.41 6 0.63c 104.12 6 10.63LD 1400W (n 5 7) 7.28 6 1.06 11.10 6 1.28d 167.73 6 30.24f
HD 1400W (n 5 7) 7.16 6 0.86 11.64 6 1.58e 175.47 6 34.38g
Non I 1400W (n 5 8) 7.69 6 0.65 4.99 6 0.20 66.65 6 3.49Non I Control (n 5 9) 6.40 6 0.29 5.25 6 0.37 82.10 6 4.22
a Analysis of variance results: for preintervention CF: p 5 not significant; for postintervention CF: b p , 0.001 vs. HD 1400W, c p , 0.001 vs. HD1400W, LD 1400W, d p , 0.001 vs. Non I 1400W, Non I Control, e p , 0.001 vs. Non I 1400W, Non I Control; for % CF recovery: f p , 0.001 vs.Non I 1400W, Non I Control, g p , 0.001 vs. Non I 1400W, Non I Control.
CF 5 coronary flow; see Table 1 for definitions of groups.
735Ann Thorac Surg PARRINO ET AL1998;66:733–9 ROLE OF iNOS IN POSTISCHEMIC CORONARY FLOW
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from
munoassay [17]. The results of all assays are reported aspicomoles per gram of tissue (wet weight).
Statistical AnalysisAll results are expressed as the mean 6 standard error ofthe mean. All functional, metabolic, and molecular datawere analyzed for between-group differences using anal-ysis of variance (ANOVA) and Tukey’s HSD test. Signif-icance was defined as a p value less than 0.05. Allanalyses were performed using SPSS software (SPSS Inc,Chicago, IL).
Results
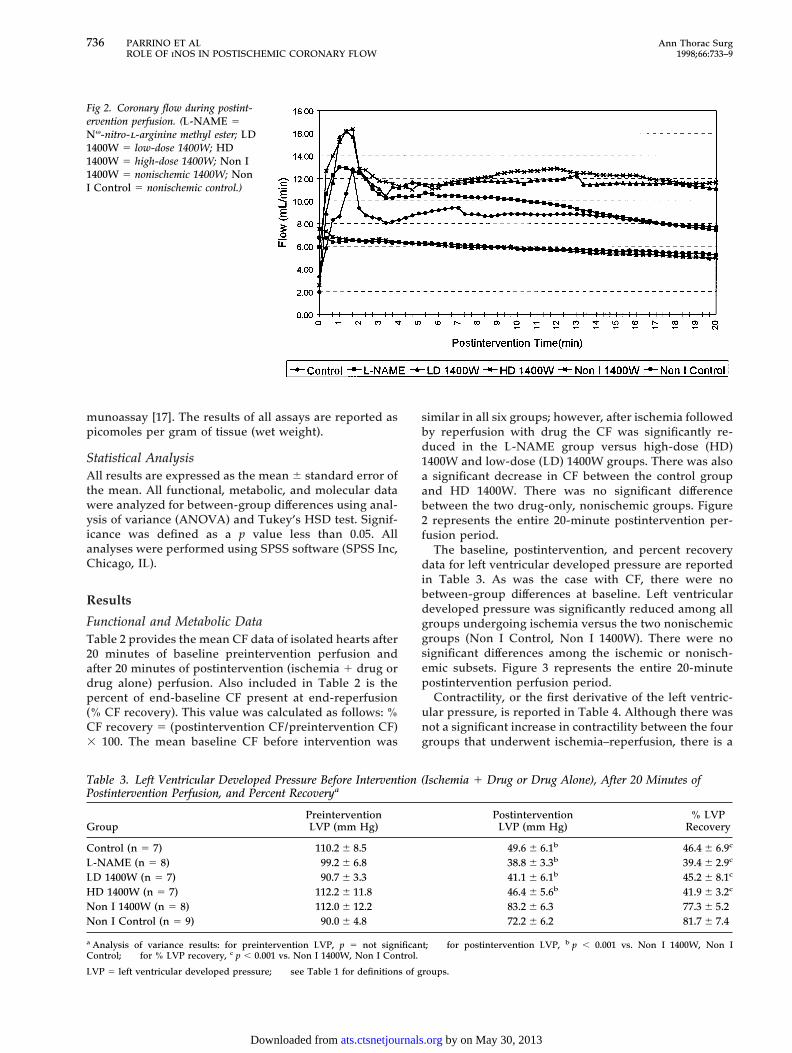
Functional and Metabolic DataTable 2 provides the mean CF data of isolated hearts after20 minutes of baseline preintervention perfusion andafter 20 minutes of postintervention (ischemia 1 drug ordrug alone) perfusion. Also included in Table 2 is thepercent of end-baseline CF present at end-reperfusion(% CF recovery). This value was calculated as follows: %CF recovery 5 (postintervention CF/preintervention CF)3 100. The mean baseline CF before intervention was
similar in all six groups; however, after ischemia followedby reperfusion with drug the CF was significantly re-duced in the L-NAME group versus high-dose (HD)1400W and low-dose (LD) 1400W groups. There was alsoa significant decrease in CF between the control groupand HD 1400W. There was no significant differencebetween the two drug-only, nonischemic groups. Figure2 represents the entire 20-minute postintervention per-fusion period.
The baseline, postintervention, and percent recoverydata for left ventricular developed pressure are reportedin Table 3. As was the case with CF, there were nobetween-group differences at baseline. Left ventriculardeveloped pressure was significantly reduced among allgroups undergoing ischemia versus the two nonischemicgroups (Non I Control, Non I 1400W). There were nosignificant differences among the ischemic or nonisch-emic subsets. Figure 3 represents the entire 20-minutepostintervention perfusion period.
Contractility, or the first derivative of the left ventric-ular pressure, is reported in Table 4. Although there wasnot a significant increase in contractility between the fourgroups that underwent ischemia–reperfusion, there is a
Fig 2. Coronary flow during postint-ervention perfusion. (L-NAME 5Nv-nitro-l-arginine methyl ester; LD1400W 5 low-dose 1400W; HD1400W 5 high-dose 1400W; Non I1400W 5 nonischemic 1400W; NonI Control 5 nonischemic control.)
Table 3. Left Ventricular Developed Pressure Before Intervention (Ischemia 1 Drug or Drug Alone), After 20 Minutes ofPostintervention Perfusion, and Percent Recoverya
GroupPreinterventionLVP (mm Hg)
PostinterventionLVP (mm Hg)
% LVPRecovery
Control (n 5 7) 110.2 6 8.5 49.6 6 6.1b 46.4 6 6.9c
L-NAME (n 5 8) 99.2 6 6.8 38.8 6 3.3b 39.4 6 2.9c
LD 1400W (n 5 7) 90.7 6 3.3 41.1 6 6.1b 45.2 6 8.1c
HD 1400W (n 5 7) 112.2 6 11.8 46.4 6 5.6b 41.9 6 3.2c
Non I 1400W (n 5 8) 112.0 6 12.2 83.2 6 6.3 77.3 6 5.2Non I Control (n 5 9) 90.0 6 4.8 72.2 6 6.2 81.7 6 7.4
a Analysis of variance results: for preintervention LVP, p 5 not significant; for postintervention LVP, b p , 0.001 vs. Non I 1400W, Non IControl; for % LVP recovery, c p , 0.001 vs. Non I 1400W, Non I Control.
LVP 5 left ventricular developed pressure; see Table 1 for definitions of groups.
736 PARRINO ET AL Ann Thorac SurgROLE OF iNOS IN POSTISCHEMIC CORONARY FLOW 1998;66:733–9
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from

clear trend toward improved function in the LD 1400Wand HD 1400W groups that approaches that of thenonischemic groups.
Biochemical DataTable 5 lists the results of the biochemical assays thatwere performed. There was a statistically significantdifference in MPO levels between the L-NAME groupand the HD 1400W, Non I 1400W, and Non I Controlgroups. The Non I Control group had cGMP levelssignificantly higher than all other groups except Non I1400W.
Comment
Knowledge of the physical locations and functions of thevarious isoforms of NOS within the heart is necessarywhen considering manipulations of the l-arginine–NOSpathway. Virtually ubiquitous throughout the heart,eNOS is found in the endothelium of both the endocar-dium and the coronary vasculature, in myocytes, and inspecialized cardiac conduction tissue [10]. Although itsrole is multifaceted, its primary function is the regulationof coronary blood flow [10]. Although iNOS is not signif-
icantly expressed by any tissues within the heart in thenormal state, with appropriate stimulation (as discussedsubsequently), iNOS may be manifested by a variety oftissues and cells within the heart. Endocardial endothe-lium, infiltrating inflammatory cells, vascular smoothmuscle, fibroblasts, cardiac myocytes, and microvascularendothelium have all been shown in vitro and in vivo toproduce iNOS after appropriate stimuli [10]. Amongthese cell types, cardiac myocytes and the microvascularendothelium probably account for the majority of NOproduction after induction of iNOS [10]. The role of iNOSis a topic of considerable and persistent debate. Theproduction of large amounts of NO after induction ofiNOS has been shown to be detrimental in a variety ofways, including decreased contractile function, a de-creased rate of spontaneous contraction, and even apo-ptosis in cardiac myocytes [10].
Determining the relative contributions of eNOS andiNOS to the pathogenesis of ischemia–reperfusion injuryhas been made more difficult by the lack of truly specificinhibitors of the various isoforms. 1400W is a highlyspecific inhibitor of iNOS. Aminoguanidine, frequentlyused as a specific inhibitor of iNOS is, at best, 30 timesmore selective for iNOS versus constitutive, or eNOS,
Fig 3. Left ventricular developedpressure during postintervention per-fusion. (L-NAME 5 Nv-nitro-l-argi-nine methyl ester; LD 1400W 5 low-dose 1400W; HD 1400W 5 high-dose 1400W; Non I 1400W 5nonischemic 1400W; Non I Control5 nonischemic control.)
Table 4. Left Ventricular Contractility Before Intervention (Ischemia 1 Drug or Drug Alone), After 20 Minutes ofPostintervention Perfusion, and Percent Recoverya
Group
PreinterventionContractility(mm Hg/s)
PostinterventionContractility(mm Hg/s)
% Recovery ofContractility
Control (n 5 7) 1,524.5 6 118.7 810.2 6 96.3 53.8 6 6.7L-NAME (n 5 8) 1,347.5 6 168.2 687.9 6 85.1 52.7 6 5.7LD 1400W (n 5 7) 1,150.4 6 77.6 758.7 6 128.6 73.5 6 14.5HD 1400W (n 5 7) 1,326.0 6 157.5 893.3 6 107.9 73.3 6 11.2Non I 1400W (n 5 8) 1,734.2 6 240.5 1,077.2 6 120.3 66.5 6 6.1Non I Control (n 5 9) 1,125.5 6 125.9 820.5 6 89.2 78.5 6 10.5
a Analysis of variance results: for all p 5 not significant. See Table 1 for definitions of groups.
737Ann Thorac Surg PARRINO ET AL1998;66:733–9 ROLE OF iNOS IN POSTISCHEMIC CORONARY FLOW
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from

whereas 1400W is more than 5,000 times more selectivefor iNOS [14].
In this investigation 1400W was used to demonstratethat a highly specific inhibitor of iNOS improves CFwhen given during reperfusion, but has no effect whengiven to hearts that have undergone continuous perfu-sion. From an examination of the CF data (Fig 2), it wouldappear that the effects of 1400W are not caused by someunsuspected, intrinsic vasodilating property unrelated toiNOS inhibition, as the two nonischemic groups demon-strated virtually identical CFs throughout the 20-minuteperiod. Furthermore, it is unlikely that 1400W was actingas a substrate for eNOS or iNOS. Detailed studies con-ducted by the group that synthesized 1400W could notdemonstrate any activity for 1400W as a substrate ofiNOS [14]. It is also unlikely that 1400W inhibited eNOS.Inhibition of eNOS has been shown in several studies tobe associated with a decrease in CF and an increase inneutrophil accumulation, contrary to what was seen inthis experiment [3, 4, 13]. And, as was shown previously,eNOS has a low, rapidly reversible affinity for 1400W [14].
The net effects of administration of 1400W, increasedCF and decreased neutrophil accumulation, were similarto observed effects of administration of exogenous NO orof l-arginine, the substrate for NOS (all isoforms) [2–5,13]. It is possible, therefore, that by inhibiting iNOS wehave provided, in effect, additional substrate for theresident eNOS. Increased eNOS production of NO wouldbe expected to promote coronary vasodilation and todecrease neutrophil accumulation. Several studies havedemonstrated the presence of iNOS in myocardium[18–20]. In our experimental protocol, the isolated heartswere exposed to 30 minutes of ischemia followed by 20minutes of perfusion. This 50 minutes is adequate for theearly demonstration of iNOS activity, which would thenbe inhibited by the administration of 1400W [20].
Myeloperoxidase levels were lower in hearts treatedwith HD 1400W during reperfusion compared with theother ischemic groups (Table 5). This difference wassignificant when compared with the L-NAME group.Inhibition of iNOS may account for this effect. Selective
inhibition of iNOS could, as theorized previously, ineffect provide additional substrate for eNOS. Nitric ox-ide, produced by the vascular endothelium, exerts aninhibitory effect on neutrophils that compromises theirability to attach to the endothelium [21]. Interestingly,aminoguanidine has been shown to promote neutrophiladhesion to venules in the rat mesentery, an effect thatcorrelated with the effect of L-NAME and was reversedby the addition of l-arginine [22]. This further illustratesthe need for specific inhibitors to dissect the varying rolesof iNOS and eNOS.
Left ventricular developed pressure was essentially thesame within the ischemic groups and within the twononischemic groups (Table 3). Contractility, thoughfound to be statistically nonsignificant, demonstrated aclear trend toward improvement in the groups treatedwith 1400W, based on the percent recovery of baselinevalues (Table 4). Previous reports have demonstratedreduced contractility in both isolated cardiac myocytesand in whole-organ models in response to iNOS stimu-lation [7, 9, 23]. In some studies, this has been found to belinked to increased cGMP levels thought to be mediatedby NO [24, 25]. In an effort to explore this further, allhearts were assayed for cGMP content using a radioim-munoassay [17]. All the ischemic groups demonstrateddecreased tissue levels of cGMP relative to the nonisch-emic controls, with a significant difference between theNon I Control group and all four ischemic groups. Thus,no conclusions could be drawn from this data.
We have shown that iNOS inhibition increased CFsignificantly. It also reduced MPO significantly, suggest-ing an effect on neutrophils. It may be that iNOS inhibi-tion increases the available substrate for eNOS, thusincreasing the amount of NO produced by this isoformand accounting for the findings we have demonstrated.Clearly both eNOS and iNOS have a major role in thecoronary circulation. Augmentation of eNOS while in-hibiting iNOS could ultimately be used clinically afterischemia–reperfusion.
We express our grateful appreciation to Mr. Anthony J. Herringfor his invaluable technical assistance. We also thank Mr. JefferyOplinger for synthesizing the 1400W.
This research was supported by a National Research ServiceAward (Fellowship No. 1 F32 HL09558-01A1) granted by theNational Heart, Lung, and Blood Institute of the NationalInstitutes of Health.
References
1. Williams MW, Taft CS, Ramnauth S, et al. Endogenous nitricoxide (NO) protects against ischemia–reperfusion injury inthe rabbit. Cardiovasc Res 1995;30:79–86.
2. Wang QD, Morcos E, Wiklund P, et al. l-Arginine enhancesfunctional recovery and Ca11 dependent nitric oxide syn-thase activity after ischemia and reperfusion in the rat heart.J Cardiovasc Pharmacol 1997;29:291–6.
3. Engelman DT, Watanabe M, Engelman RM, et al. Constitu-tive nitric oxide release is impared after ischemia andreperfusion. J Thorac Cardiovasc Surg 1995;110:1047–53.
4. Vinten-Johansen J, Sato H, Zhao ZQ. The role of nitric oxide
Table 5. Results of Biochemical Assaysa
Group
MPO(change in
absorbance/g tissue(wetweight)/min)
cGMP(pmol/g
tissue(wetweight))
Control (n 5 7) 0.37 6 0.02 143.14 6 5.25L-NAME (n 5 8) 0.71 6 0.22a 137.60 6 12.52LD 1400W (n 5 7) 0.40 6 0.05 128.27 6 16.58HD 1400W (n 5 7) 0.28 6 0.03 144.75 6 8.57Non I 1400W (n 5 8) 0.25 6 0.02 168.35 6 8.28Non I Control (n 5 9) 0.24 6 0.04 220.12 6 26.16b
a Analysis of variance results: for MPO, a p 5 0.014 vs HD 1400W, Non I1400W, and Non I Control; for cGMP, b p 5 0.001 vs Control, L-NAME, LD 1400W, and HD 1400W.
cGMP 5 cyclic guanosine monophosphate; MPO 5 myeloperoxidase;see Table 1 for definitions of groups.
738 PARRINO ET AL Ann Thorac SurgROLE OF iNOS IN POSTISCHEMIC CORONARY FLOW 1998;66:733–9
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from

and NO-donor agents in myocardial protection from surgi-cal ischemic–reperfusion injury. Int J Cardiol 1995;50:273–81.
5. Carrier M, Khalil A, Tourigny A, et al. Effect of l-arginine onmetabolic recovery of the ischemic myocardium. Ann Tho-rac Surg 1996;61:1651–7.
6. Wang P, Zweier JL. Measurement of nitric oxide and per-oxynitrite generation in the postischemic heart. J Biol Chem1996;27:29223–30.
7. Matheis G, Sherman MP, Buckberg GD, et al. Role ofl-arginine–nitric oxide pathway in myocardial reoxygen-ation injury. Am J Physiol 1992;262:H616–20.
8. Lefer DJ, Scalia R, Campbell B, et al. Peroxynitrite inhibitsleukocyte–endothelial cell interactions and protects againstischemia–reperfusion in rats. J Clin Invest 1997;99:684–91.
9. Schulz R, Wambolt R. Inhibition of nitric oxide synthesisprotects the isolated working rabbit heart from ischemia–reperfusion injury. Cardiovasc Res 1995;30:432–39.
10. Kelly RA, Balligand JL, Smith TW. Nitric oxide and cardiacfunction. Circ Res 1996;79:363–80.
11. Akiyama K, Suzuki H, Grant P, et al. Oxidation products ofnitric oxide, NO2 and NO3, in plasma after experimentalmyocyte infarction. J Mol Cell Cardiol 1997;29:1–9.
12. Mauney MC, Cope JT, Binns OAR, et al. Non-heart-beatingdonors: a model of thoracic allograft injury. Ann Thorac Surg1996;62:54–62.
13. Hoshida S, Yamashita N, Igarashi J, et al. Nitric oxidesynthase protects the heart against ischemia–reperfusioninjury in rabbits. J Pharmacol Exp Ther 1995;274:413–8.
14. Garvey EP, Oplinger JA, Furfine ES, et al. 1400W is a slow,tight binding, and highly selective inhibitor of induciblenitric-oxide synthase in vitro and in vivo. J Biol Chem 1997;272:4959–63.
15. Loscalzo J, Welch G. Nitric oxide and its role in the cardio-vascular system. Prog Cardiovasc Dis 1995;38:87–104.
16. Lohmann SM, Fischmeister R, Walter U. Signal transductionby cGMP in heart. Basic Res Cardiol 1991;86:503–14.
17. Brooker G, Terasaki WL, Price MG. Gammaflow: a com-pletely automated radioimmunoassay system. Science 1976;194:270–6.
18. Bateson AN, Jakiwczyk OM, Schulz R. Rapid increase ininducible nitric oxide synthase gene expression in the heartduring endotoxemia. Eur J Pharmacol 1996;303:141–4.
19. Balligand JL, Ungureanu-Longrois D, Simmons WL, et al.Cytokine-inducible nitric oxide synthase (iNOS) expressionin cardiac myocytes. J Biol Chem 1994;269:27580–8.
20. Schulz R, Nava E, Moncada S. Induction and potentialbiological relevance of a Ca21-independent nitric oxidesynthase in the myocardium. Br J Pharmacol 1992;105:575–80.
21. Ma XL, Weyrich AS, Lefer DJ, et al. Diminished basal nitricoxide release after myocardial ischemia and reperfusionpromotes neutrophil adherence to coronary endothelium.Circ Res 1993;72:403–12.
22. Lopez-Belmonte J, Whittle BJ. Aminoguanidine-provokedleukocyte adherence to rat mesenteric venules: role of con-stitutive nitric oxide synthase inhibition. Br J Pharmacol1995;116:2710–4.
23. Sun X, Wei S, Szabo C, et al. Depression of the ionotropicaction of isoprenaline by nitric oxide synthase induction inrat isolated hearts. Eur J Pharmacol 1997;320:29–35.
24. Kinugawa K, Kohmoto O, Yao A, et al. Cardiac induciblenitric oxide synthase negatively modulates myocardial func-tion in cultured rat myocytes. Am J Physiol 1997;272:H35–47.
25. Balligand JL, Ungureanu D, Kelly RA, et al. Abnormalcontractile function due to induction of nitric oxide synthesisin rat cardiac myocytes follows exposure to activated mac-rophage-conditioned medium. J Clin Invest 1993;91:2314–9.
DISCUSSION
DR JOHN W. HAMMON, JR (Winston-Salem, NC): I think thisis another chapter in the developing story of nitric oxide. I wouldlike to ask Dr Parrino two questions.
In most models of global ischemia and reperfusion like youhave given us, increasing the arginine level up front protectsagainst reperfusion injury. Could you speculate as to why thatis?
And number two, I was intrigued that your model did notshow any definite increase in myocardial function despite thefact that coronary blood flow went up. I am wondering if thatwas a problem related to the way you measured contractility.Contractility is a word that has been thrown around a lot. Iwonder if you, perhaps, used a model in which you couldactually measure chamber size and had a little more accuratedescription of left ventricular function, that you might showincreases in function. It looked like it actually did go up, but itwas not statistically significant.
DR PARRINO: In answer to Dr Hammon’s question regardingwhy early treatment with l-arginine, which is the substrate fornitric oxide synthase, improves myocardial recovery after isch-emia–reperfusion, I think it is related to the duration of theischemic insult that is delivered. If the ischemic insult is rela-tively short and the reperfusion time is also relatively short, thenI think that the l-arginine serves as substrate for the endothelialisoform rather than the inducible isoform as the latter enzymerequires time for expression and activity.
Certainly measures of contractility that use force transducersor other mechanisms of demonstrating segment shortening offermore precise measurements than our saline-filled balloon in theleft ventricle. We try to maintain an end-diastolic pressure ofabout 10 mm Hg by adjusting the volume of our balloon andmeasuring the maximal rate of pressure change over time in thatballoon. But, compared with other techniques, it is a relativelycrude measurement.
739Ann Thorac Surg PARRINO ET AL1998;66:733–9 ROLE OF iNOS IN POSTISCHEMIC CORONARY FLOW
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from

1998;66:733-739 Ann Thorac SurgTerri-Ann Wattsman, Robert C. King, Curtis G. Tribble and Irving L. Kron
Patrick E. Parrino, Victor E. Laubach, John R. Gaughen, Jr, Kimberly S. Shockey, coronary flow
Inhibition of inducible nitric oxide synthase after myocardial ischemia increases
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/66/3/733including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/66/3/733#BIBL
This article cites 25 articles, 9 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/66/3/733#otherarticles
This article has been cited by 5 HighWire-hosted articles:
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from
Recommended

















