Embed Size (px)
Citation preview
5th Annual EMM Conference
Clinical Decision Support
Development, Maintenance & Evaluation:
A 10 year review
Anmol Sandhu
Pharmacist – eMedicines Management
St Vincent’s Hospital, Sydney
Agenda
1. Clinical Decision Support (CDS) at SVHS
I. On or off?
II. Development & maintenance
2. CDS for Drug-drug interactions – a tough nut to crack
I. Context matters – who, what, where, when and how
II. Research & evaluation to inform implementation
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 2
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 3
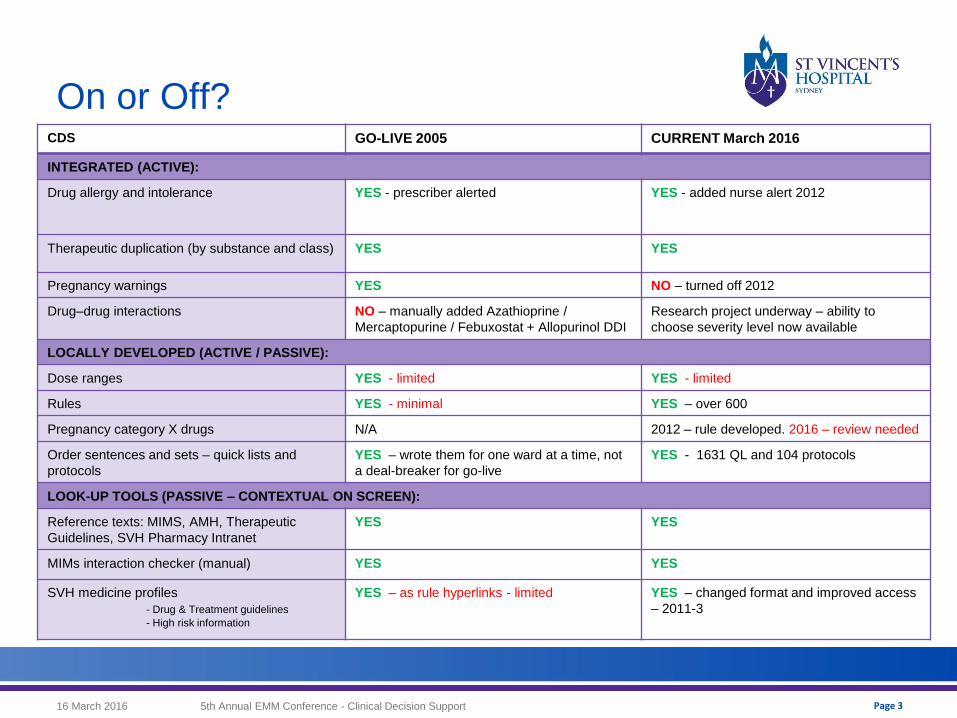
On or Off? CDS GO-LIVE 2005 CURRENT March 2016
INTEGRATED (ACTIVE):
Drug allergy and intolerance YES - prescriber alerted YES - added nurse alert 2012
Therapeutic duplication (by substance and class) YES YES
Pregnancy warnings YES NO – turned off 2012
Drug–drug interactions NO – manually added Azathioprine /
Mercaptopurine / Febuxostat + Allopurinol DDI
Research project underway – ability to
choose severity level now available
LOCALLY DEVELOPED (ACTIVE / PASSIVE):
Dose ranges YES - limited YES - limited
Rules YES - minimal YES – over 600
Pregnancy category X drugs N/A 2012 – rule developed. 2016 – review needed
Order sentences and sets – quick lists and
protocols
YES – wrote them for one ward at a time, not
a deal-breaker for go-live
YES - 1631 QL and 104 protocols
LOOK-UP TOOLS (PASSIVE – CONTEXTUAL ON SCREEN):
Reference texts: MIMS, AMH, Therapeutic
Guidelines, SVH Pharmacy Intranet
YES YES
MIMs interaction checker (manual) YES YES
SVH medicine profiles
- Drug & Treatment guidelines
- High risk information
YES – as rule hyperlinks - limited YES – changed format and improved access
– 2011-3
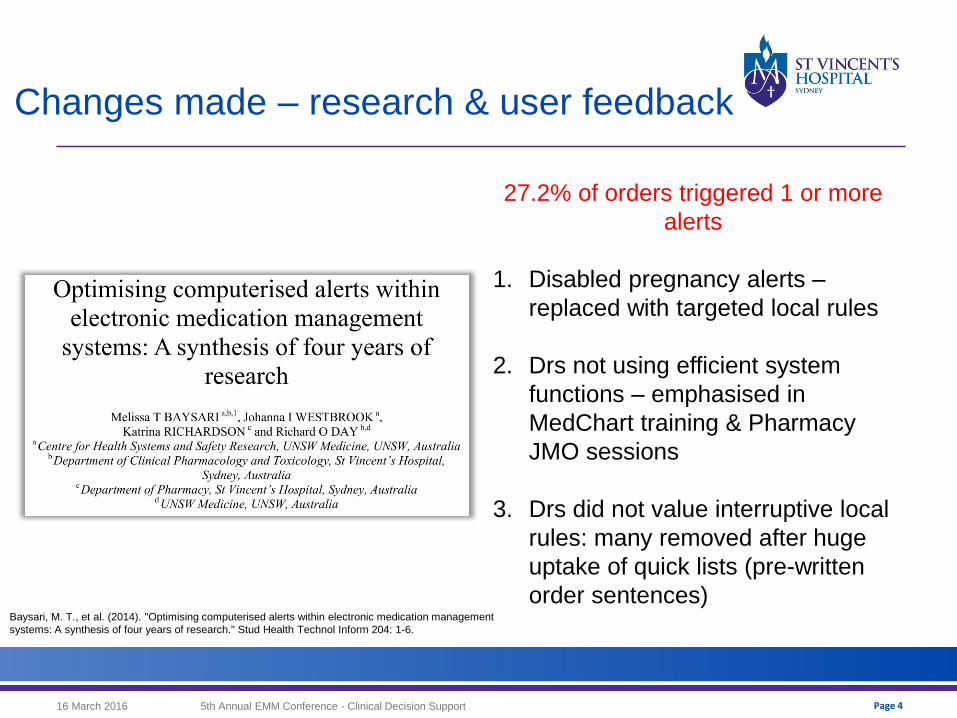
Changes made – research & user feedback
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 4
27.2% of orders triggered 1 or more
alerts
1. Disabled pregnancy alerts –
replaced with targeted local rules
2. Drs not using efficient system
functions – emphasised in
MedChart training & Pharmacy
JMO sessions
3. Drs did not value interruptive local
rules: many removed after huge
uptake of quick lists (pre-written
order sentences) Baysari, M. T., et al. (2014). "Optimising computerised alerts within electronic medication management
systems: A synthesis of four years of research." Stud Health Technol Inform 204: 1-6.
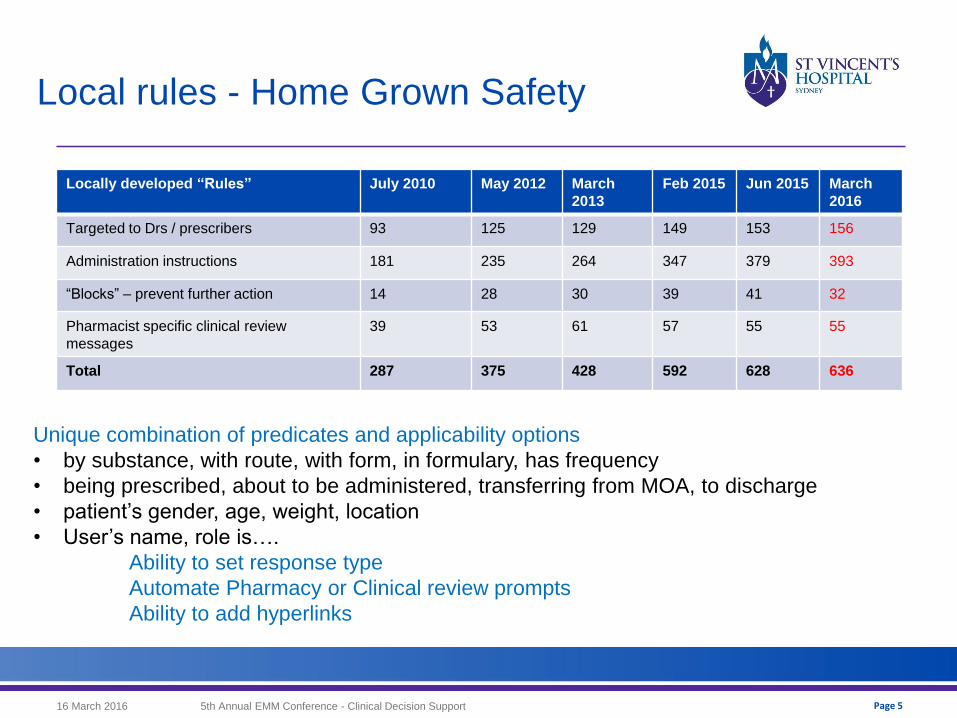
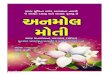
Local rules - Home Grown Safety
16 March 2016 5th Annual EMM Conference - Clinical Decision Support
Locally developed “Rules” July 2010 May 2012 March
2013
Feb 2015 Jun 2015 March
2016
Targeted to Drs / prescribers 93 125 129 149 153 156
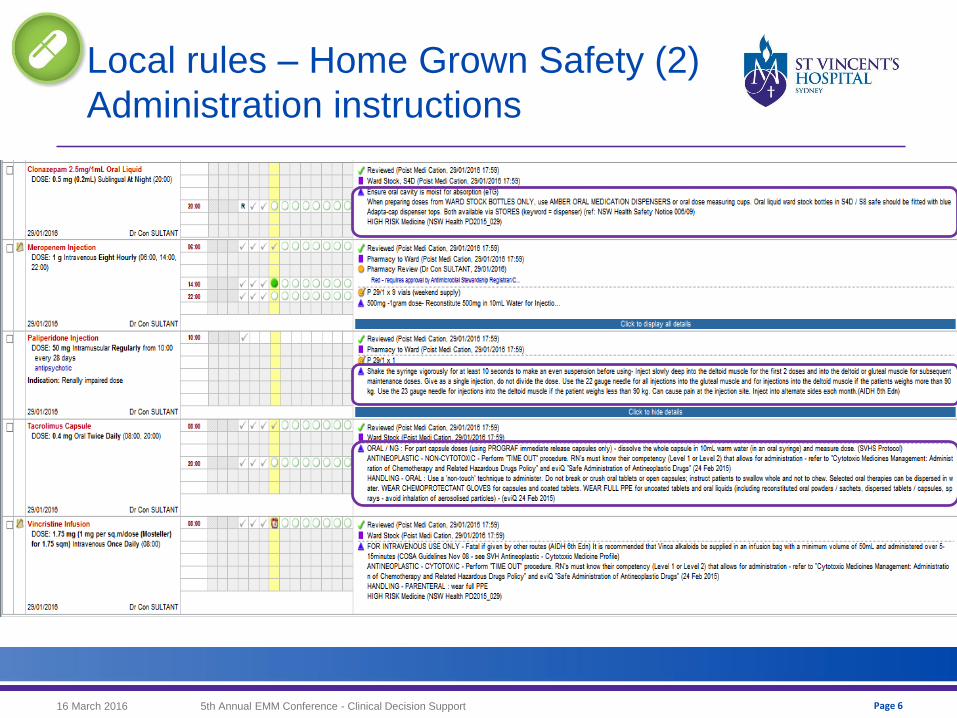
Administration instructions 181 235 264 347 379 393
“Blocks” – prevent further action 14 28 30 39 41 32
Pharmacist specific clinical review
messages
39 53 61 57 55 55
Total 287 375 428 592 628 636
Unique combination of predicates and applicability options
• by substance, with route, with form, in formulary, has frequency
• being prescribed, about to be administered, transferring from MOA, to discharge
• patient’s gender, age, weight, location
• User’s name, role is….
Ability to set response type
Automate Pharmacy or Clinical review prompts
Ability to add hyperlinks
Page 5
16 March 2016 5th Annual EMM Conference - Clinical Decision Support
Local rules – Home Grown Safety (2)
Administration instructions
Page 6
16 March 2016 5th Annual EMM Conference - Clinical Decision Support
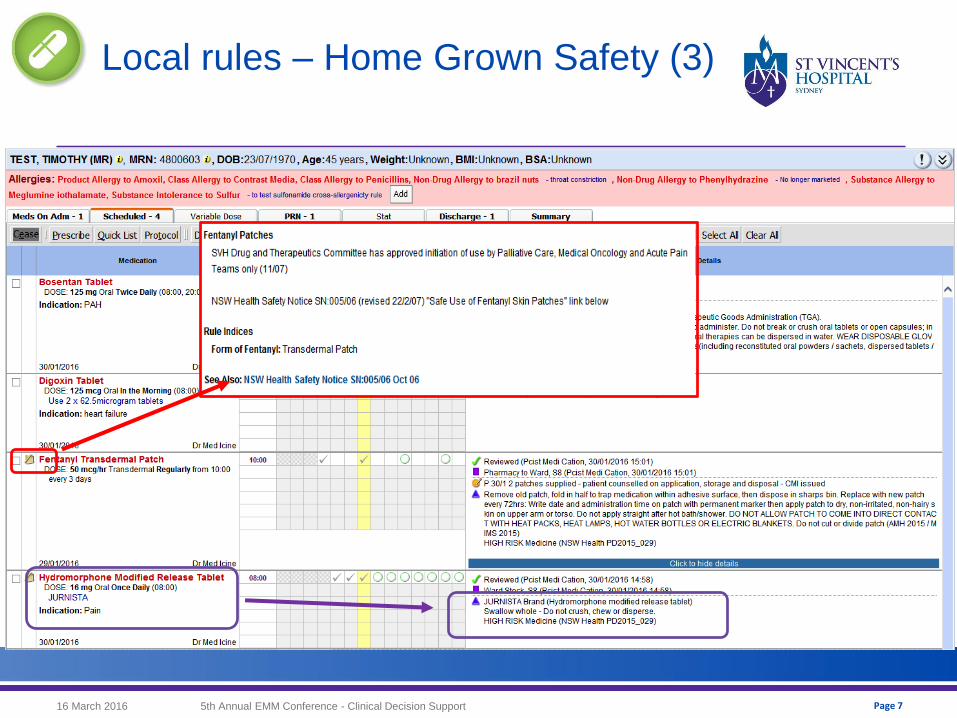
Local rules – Home Grown Safety (3)
Page 7
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 8
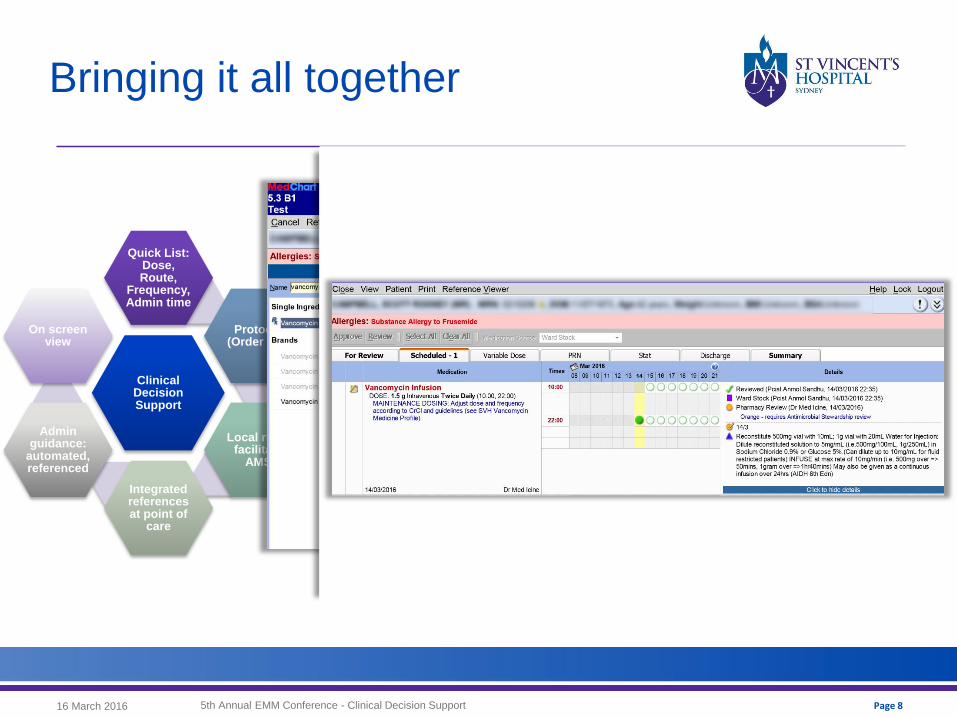
Bringing it all together
Clinical Decision Support
Quick List: Dose, Route,
Frequency, Admin time
Protocol (Order Set)
Local rules facilitate
AMS
Integrated references at point of
care
Admin guidance:
automated, referenced
On screen view
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 9
CDS for drug-drug interactions:
A tough nut to crack
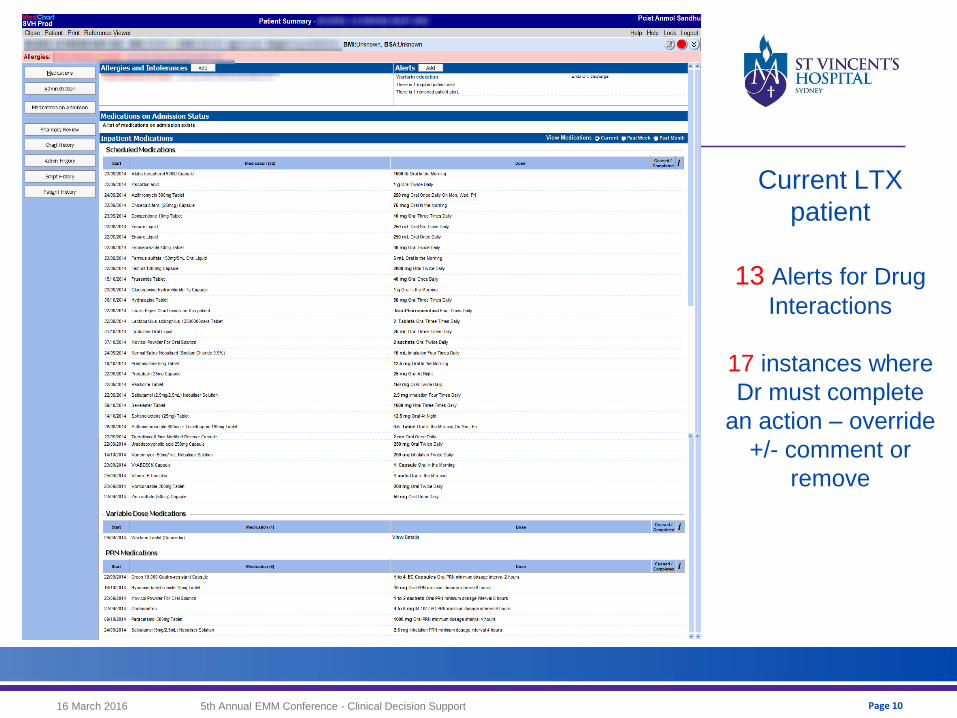
Page 10
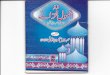
Current LTX
patient
13 Alerts for Drug
Interactions
17 instances where
Dr must complete
an action – override
+/- comment or
remove
16 March 2016 5th Annual EMM Conference - Clinical Decision Support
Page 11
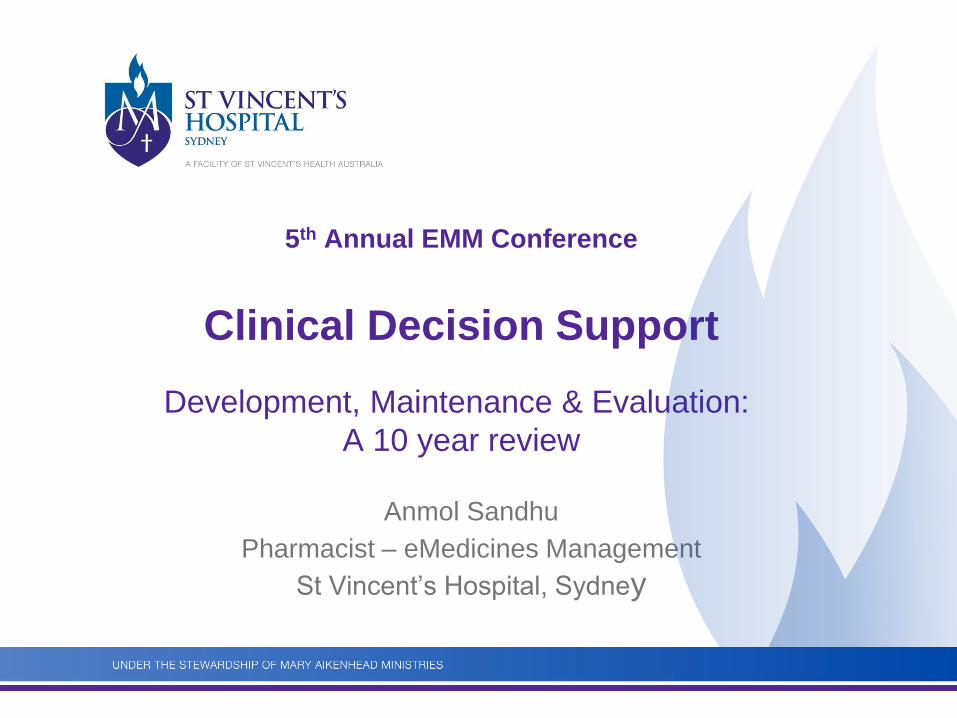
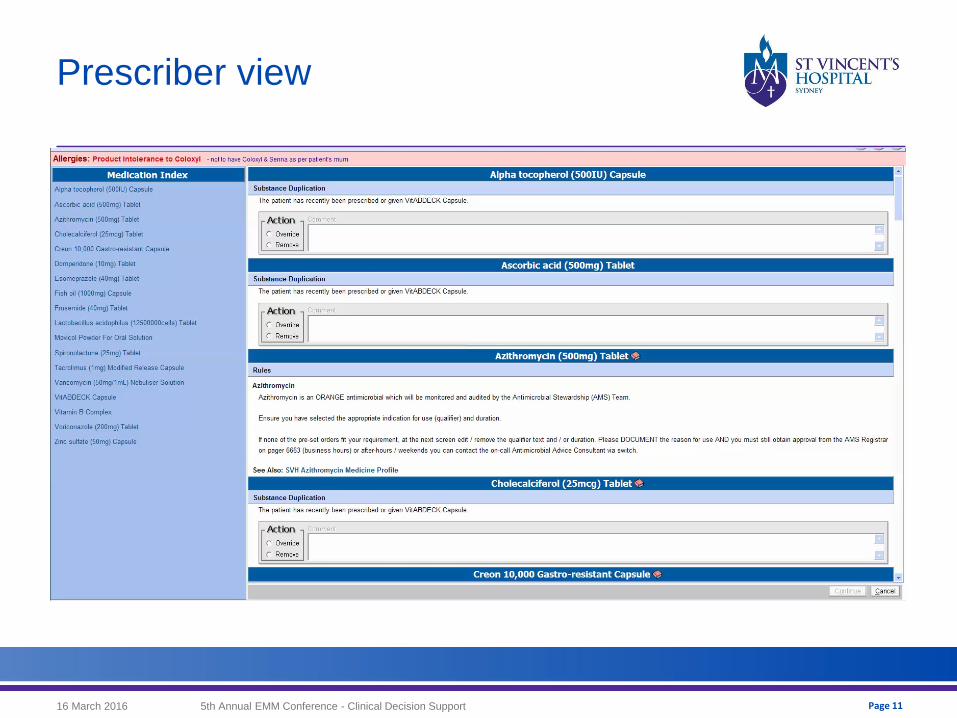
Prescriber view
16 March 2016 5th Annual EMM Conference - Clinical Decision Support
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 12
Drug-Drug Interactions
Not turned on …………. Yet
1/3 orders triggers an alert (!!)
Over 8500 at go-live – all ON or all OFF (could not enable severity levels)
In 2016 there are over 10,000 DDI’s that could be activated
Severe = 2709 pairs
Working towards evidence-based solutions
Oct 2014 – DTC commissioned a multidisciplinary DDI Working
Group
Research projects underway with CHSSR (Dr Melissa Baysari)
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 13
CONTEXT MATTERS:
WHO, WHAT, WHERE, WHEN & HOW
ALERT FATIGUEWhat contextual considerations are
required?
What are the current challenges and
are there any proposed strategies?

16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 14
Context matters – WHO
Considerations Challenges / Strategies
1. Feldstein, A., et al. (2004). "How to design computerized alerts to safe prescribing practices." Jt Comm J Qual Saf 30(11): 602-613.
2. Payne, T. H., et al. (2015). "Recommendations to Improve the Usability of Drug-Drug Interaction Clinical Decision Support Alerts.
WH
O
Who should see the DDI alert?
(Dr, Pcist, Nurse, Patient?)
• Who is responsible for acting on the alert?
• Divert or “forward” alerts to the relevant clinician:
e.g. diversion of time-dependent DDI alerts to nurse or alerts about INR monitoring to anticoagulation service
Are the decision makers targeted?
• Retrospective DDI alert monitoring report sent to AMOs
• Ability to “snooze” alerts
Disable frequently overridden DDI alerts for specialties
Allow Drs to self-define alert content / severity thresholds?
• Unable to agree to turn off any alerts hospital-wide: - variable levels of clinician DDI knowledge- differing specialties.
• >50% disagreed with option to disable or self-define alert content.1
• Nil evidence currently. Error-management strategy & legal implication require consideration.2
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 15
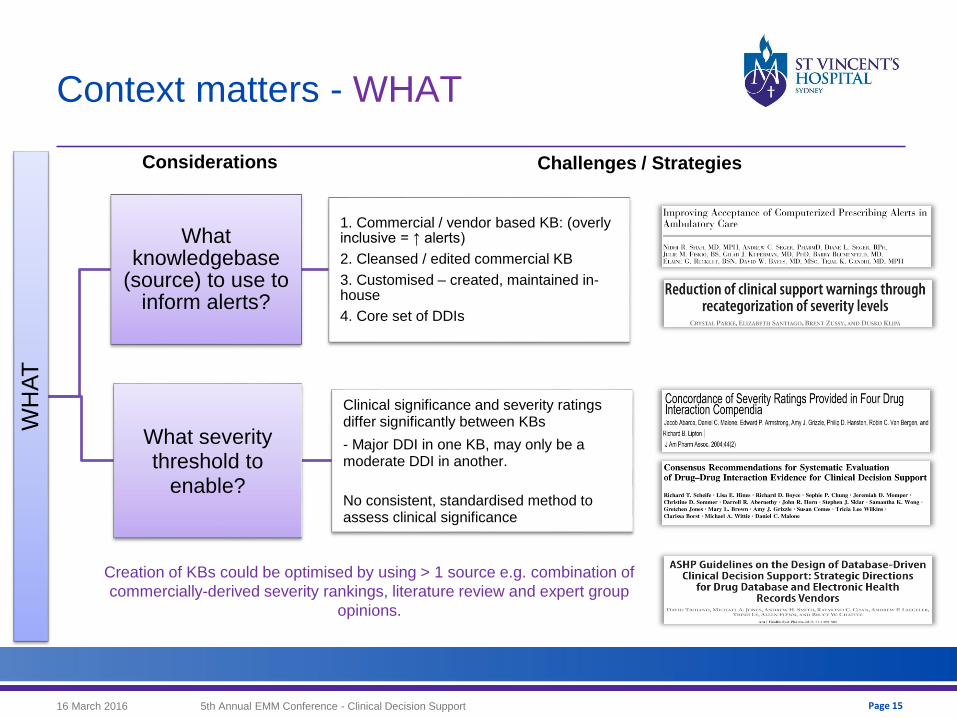
Context matters - WHAT
WH
AT
What knowledgebase
(source) to use to inform alerts?
1. Commercial / vendor based KB: (overly inclusive = ↑ alerts)
2. Cleansed / edited commercial KB
3. Customised – created, maintained in-house
4. Core set of DDIs
What severity threshold to
enable?
Clinical significance and severity ratings differ significantly between KBs
- Major DDI in one KB, may only be a moderate DDI in another.
No consistent, standardised method to assess clinical significance
Creation of KBs could be optimised by using > 1 source e.g. combination of
commercially-derived severity rankings, literature review and expert group
opinions.
Considerations Challenges / Strategies
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 16
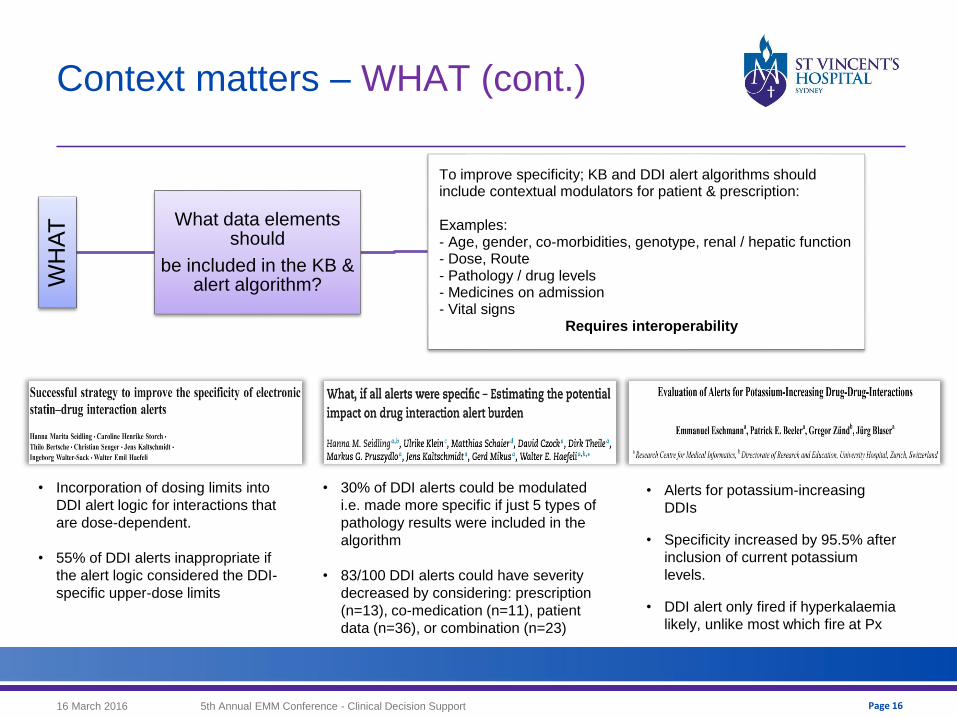
WH
AT What data elements
should
be included in the KB & alert algorithm?
To improve specificity; KB and DDI alert algorithms should include contextual modulators for patient & prescription:
Examples:- Age, gender, co-morbidities, genotype, renal / hepatic function- Dose, Route- Pathology / drug levels - Medicines on admission- Vital signs
Requires interoperability
Context matters – WHAT (cont.)
• Incorporation of dosing limits into
DDI alert logic for interactions that
are dose-dependent.
• 55% of DDI alerts inappropriate if
the alert logic considered the DDI-
specific upper-dose limits
• 30% of DDI alerts could be modulated
i.e. made more specific if just 5 types of
pathology results were included in the
algorithm
• 83/100 DDI alerts could have severity
decreased by considering: prescription
(n=13), co-medication (n=11), patient
data (n=36), or combination (n=23)
• Alerts for potassium-increasing
DDIs
• Specificity increased by 95.5% after
inclusion of current potassium
levels.
• DDI alert only fired if hyperkalaemia
likely, unlike most which fire at Px
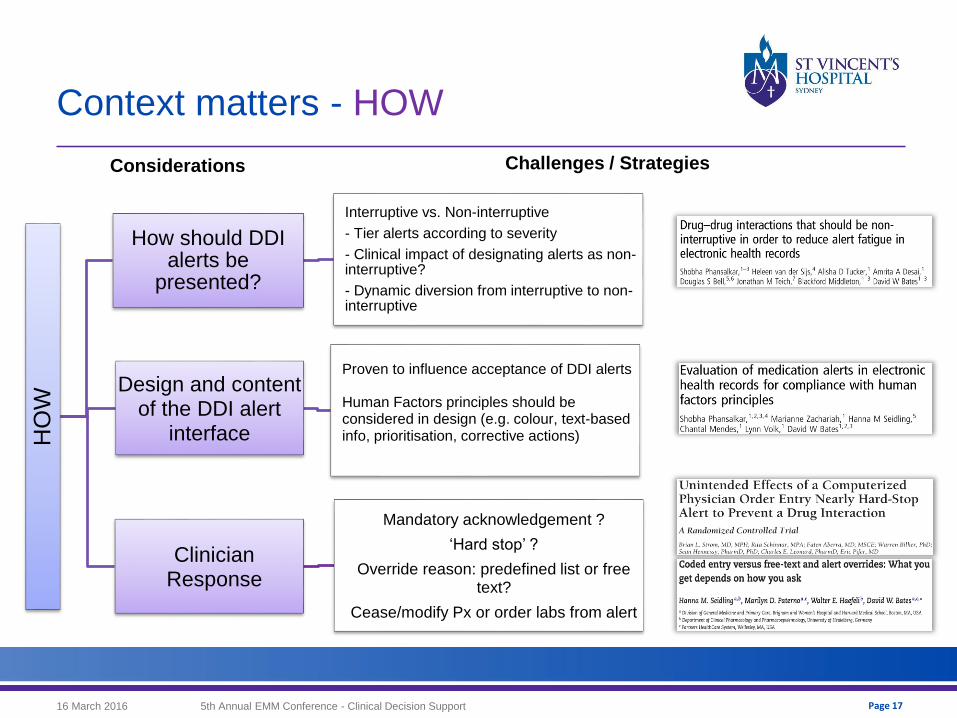
Context matters - HOW
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 17
HO
W
How should DDI alerts be
presented?
Interruptive vs. Non-interruptive
- Tier alerts according to severity
- Clinical impact of designating alerts as non-interruptive?
- Dynamic diversion from interruptive to non-interruptive
Design and content of the DDI alert
interface
Proven to influence acceptance of DDI alerts
Human Factors principles should be considered in design (e.g. colour, text-based info, prioritisation, corrective actions)
Clinician Response
Mandatory acknowledgement ?
‘Hard stop’ ?
Override reason: predefined list or free text?
Cease/modify Px or order labs from alert
Considerations Challenges / Strategies
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 18
Context matters – WHEN / WHERE
When should the DDI alert fire?
At onset of DDI prescription ? Only trigger when parameters are met ?
(e.g. hyperkalaemia)
DDIs with delayed effect?
Fire again when an interacting drug is stopped or dose is changed?
First time only?
Off during business hours / ward round ? On after hours?
Where should DDIs alerts be enabled? How can we target high risk groups? Hospital-wide?
General wards vs. ICU ICU patients: impaired ability to metabolise drugs, larger number of drugs prescribed, particularly high risk, and
frequent dose changes)
One study identified just 20 DDI pairs that accounted for 90% of all interactions in ICU
Inpatients and outpatientsHospitalisation is a known risk factor for DDIs (complex medication regimens, care by multiple clinicians, transfer between
departments).
In a nutshell
More questions than answers….
Evaluations in clinical practice are lacking
No formal guidelines or standards
Vendor support required to improve utility of DDI alerts
Alert design, screening interval is same for all alerts, Duplications – turn on substance,
turn off class.
Interoperability between EMM, EMR, devices etc. required to
improve specificity
16 March 2016 195th Annual EMM Conference - Clinical Decision Support
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 20
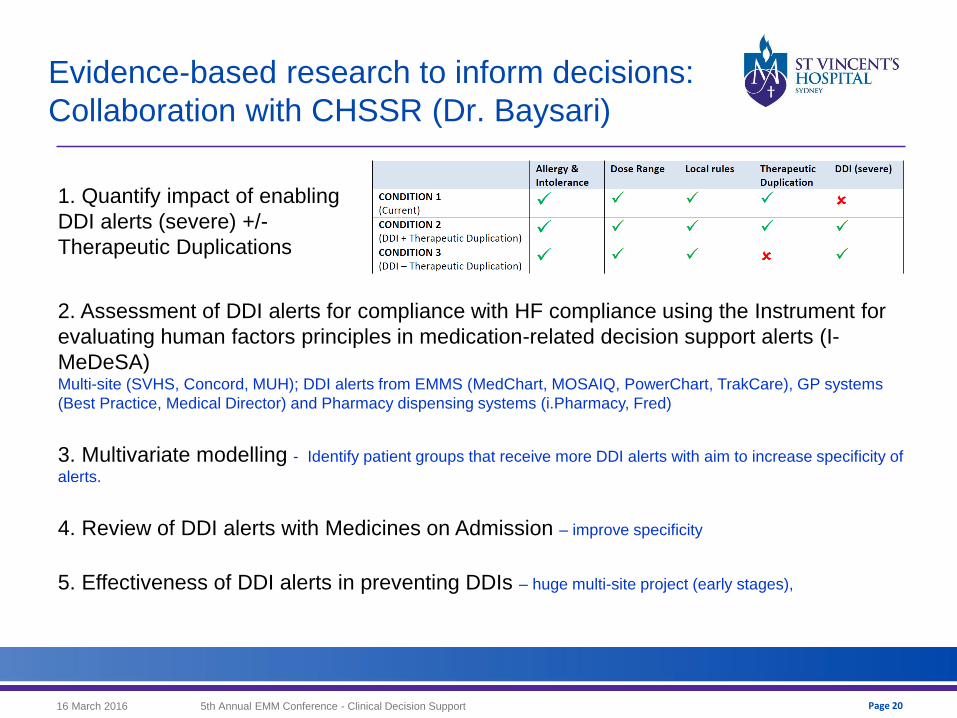
Evidence-based research to inform decisions:
Collaboration with CHSSR (Dr. Baysari)
1. Quantify impact of enabling
DDI alerts (severe) +/-
Therapeutic Duplications
2. Assessment of DDI alerts for compliance with HF compliance using the Instrument for
evaluating human factors principles in medication-related decision support alerts (I-
MeDeSA) Multi-site (SVHS, Concord, MUH); DDI alerts from EMMS (MedChart, MOSAIQ, PowerChart, TrakCare), GP systems
(Best Practice, Medical Director) and Pharmacy dispensing systems (i.Pharmacy, Fred)
3. Multivariate modelling - Identify patient groups that receive more DDI alerts with aim to increase specificity of
alerts.
4. Review of DDI alerts with Medicines on Admission – improve specificity
5. Effectiveness of DDI alerts in preventing DDIs – huge multi-site project (early stages),
Acknowledgments
SVHS DDI Working Group – Prof Ric Day, Prof Jo Brien, Dr P Savage, Dr M Baysari, K Richardson
Dr Melissa Baysari – CHSSR, Macquarie University
Dr Dennis Armstrong – CSC
Participating EMM study sites
Kate Richardson – EMM Pharmacist, SVHS
Maureen Heywood – EMM Pharmacist, SVHS
SVC Clinic Foundation
16 March 2016 5th Annual EMM Conference - Clinical Decision Support Page 21