Embed Size (px)
Citation preview

COMMON HAND DISSORDERCOMMON HAND DISSORDER
DR JOSE A. RICO-PECERODR JOSE A. RICO-PECEROEAST SURREY HOSPITALEAST SURREY HOSPITAL
JUNE 15JUNE 15THTH 2006 2006

COMMON HAND DISSORDERCOMMON HAND DISSORDER
• CARPAL TUNNEL SYNDROME.CARPAL TUNNEL SYNDROME.
• TRIGGER FINGERS.TRIGGER FINGERS.
• DUPUYTREN DISSEASE.DUPUYTREN DISSEASE.
• GANGLIONSGANGLIONS

CARPAL TUNNEL SYNDROMECARPAL TUNNEL SYNDROME
1. DEFINITION.
Carpal tunnel syndrome (CTS) is the most commonly diagnosed and treated entrapment neuropathy. The syndrome is characterized by pain, paresthesias, and weakness in the median nerve distribution of the hand. Surgical and nonsurgical treatments exist that can produce excellent outcomes for patients.
2. FREQUENCY
- Industrial workers, whose hands and wrists are subjected to repetitive motion and trauma.
- prevalence: 1% for men and 7% for women in Netherlands
3 % in Sweden
- Women > men

3. ETIOLOGY: MULTIFACTORIAL3. ETIOLOGY: MULTIFACTORIAL
- Local: - Local: Fracture callus, osteophytes, anomalous muscle bodies, tumors, Fracture callus, osteophytes, anomalous muscle bodies, tumors, hypertrophic synovium, gout and other inflammatory conditions, and hypertrophic synovium, gout and other inflammatory conditions, and infection.infection.
- Sistemic: - Sistemic: # # Endocrine system: Endocrine system: diabetes, hypothyroidism and pregnancydiabetes, hypothyroidism and pregnancy # Metabolic: # Metabolic: alcoholism, renal failure with hemodialysis, alcoholism, renal failure with hemodialysis,
mucopolysaccharidosesmucopolysaccharidoses
CARPAL TUNNEL SYNDROMECARPAL TUNNEL SYNDROME
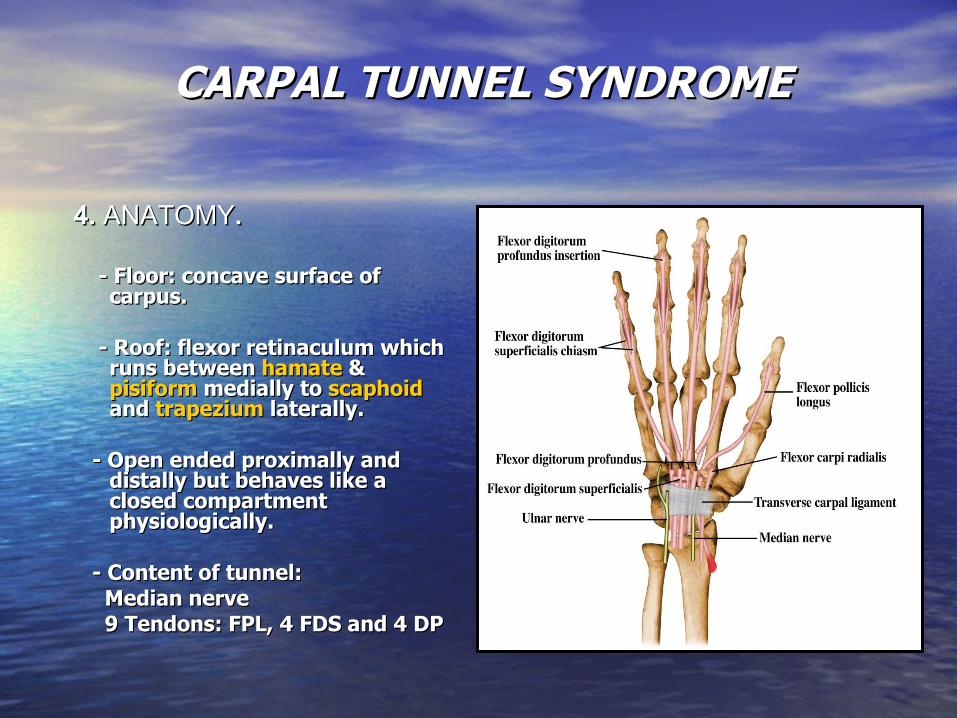
4. 4. ANATOMYANATOMY. .
- - Floor: concave surface of Floor: concave surface of carpus.carpus.
- - Roof: flexor retinaculum which Roof: flexor retinaculum which runs between runs between hamatehamate & & pisiformpisiform medially to medially to scaphoidscaphoid and and trapeziumtrapezium laterally. laterally.
- - Open ended proximally and Open ended proximally and
distally but behaves like a distally but behaves like a closed compartment closed compartment physiologically.physiologically.
- Content of tunnel:- Content of tunnel: Median nerveMedian nerve 9 Tendons: FPL, 4 FDS and 4 DP9 Tendons: FPL, 4 FDS and 4 DP
CARPAL TUNNEL SYNDROMECARPAL TUNNEL SYNDROME

5. DIAGNOSTIC.5. DIAGNOSTIC.
- Hx of symtoms- Hx of symtoms Gradual in onset, pain and paresthesias in the median nerve Gradual in onset, pain and paresthesias in the median nerve
distribution, often worsening at night. With long standing thenar distribution, often worsening at night. With long standing thenar atrophy frequently is observed.atrophy frequently is observed.
- Presence of risks factors.- Presence of risks factors.
- Physical and neurological examination.- Physical and neurological examination.
- Imaging test: X-rays.- Imaging test: X-rays. Only 0.4% of routine wrist radiographs for CTS were Only 0.4% of routine wrist radiographs for CTS were
demonstrated to have findings of therapeutic significance.demonstrated to have findings of therapeutic significance.
CARPAL TUNNEL SYNDROMECARPAL TUNNEL SYNDROME

5. DIAGNOSTIC.5. DIAGNOSTIC.
- - Provocative tests:Provocative tests:
# Phalen wrist flexion test# Phalen wrist flexion test
# # Tinel test Tinel test
# # Carpal compression test: 30’’ Carpal compression test: 30’’
CARPAL TUNNEL SYNDROMECARPAL TUNNEL SYNDROME
5. DIAGNOSTIC.5. DIAGNOSTIC.
- - Nerve conduction studiesNerve conduction studies
- - Electromyography Electromyography
- - Diagnostic Procedures: Direct pressure measurementDiagnostic Procedures: Direct pressure measurement
CARPAL TUNNEL SYNDROMECARPAL TUNNEL SYNDROME

6. DIFFERENTIAL DIAGNOSIS6. DIFFERENTIAL DIAGNOSIS
- Radiculophaty C6-C7.- Radiculophaty C6-C7.
- Compresion of the median nerve outside of the carpal tunnel.- Compresion of the median nerve outside of the carpal tunnel.
CARPAL TUNNEL SYNDROMECARPAL TUNNEL SYNDROME
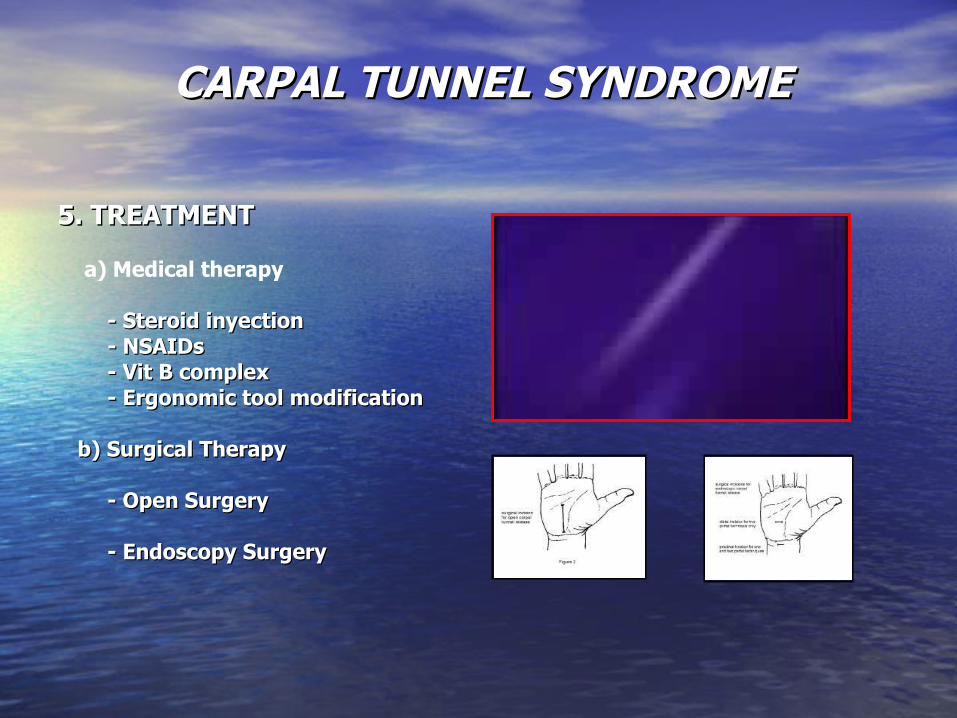
5. TREATMENT5. TREATMENT
a) Medical therapy
- Steroid inyection- Steroid inyection - NSAIDs- NSAIDs - Vit B complex- Vit B complex - Ergonomic tool modification- Ergonomic tool modification
b) Surgical Therapyb) Surgical Therapy - Open Surgery- Open Surgery
- Endoscopy Surgery- Endoscopy Surgery
CARPAL TUNNEL SYNDROMECARPAL TUNNEL SYNDROME
TRIGGER FINGERTRIGGER FINGER
Stenosing tendovaginitis, or trigger finger (TF), is Stenosing tendovaginitis, or trigger finger (TF), is one of the most common causes of hand pain and disability. one of the most common causes of hand pain and disability. The condition begins as discomfort in the palm during The condition begins as discomfort in the palm during movements of the involved digit(s). Gradually, or, in some movements of the involved digit(s). Gradually, or, in some cases, acutely, the flexor tendon causes painful popping or cases, acutely, the flexor tendon causes painful popping or snapping as the patient flexes and extends the digit. The snapping as the patient flexes and extends the digit. The patient may present with a digit locked in a particular patient may present with a digit locked in a particular position, more often flexion, which may require gentle position, more often flexion, which may require gentle passive manipulation into full extension. passive manipulation into full extension.

The phenomenon is due to a The phenomenon is due to a mismatch between the size of mismatch between the size of the flexor tendon and the the flexor tendon and the retinacular pulley. Most often, retinacular pulley. Most often, this is due to formation of a this is due to formation of a nodule in the flexor digitorum nodule in the flexor digitorum superficialis (FDS) tendon, superficialis (FDS) tendon, where it glides under the A1 where it glides under the A1 pulley in the region of the pulley in the region of the metacarpal head, and, in rare metacarpal head, and, in rare instances, a nodule distal to it instances, a nodule distal to it in the tendon of the flexor in the tendon of the flexor digitorum profundus could be digitorum profundus could be the culprit. the culprit.
TRIGGER FINGERTRIGGER FINGER

TRIGGER FINGERTRIGGER FINGER
FREQUENCY
• Women>men.
• Peak incidence: 55 – 60 years.
• Dominant hand.
• Thumb>ring>middle>little>index.
TRIGGER FINGERTRIGGER FINGER
SYMPTOMS.• Locking or catching during active flexion-extension activity; may need passive manipulation to extend the digit in later stages • Stiff digit, especially in long-standing or neglected cases • Pain over the distal palm • Pain radiating along the digit
SINGS.• Triggering on active or passive extension by the patient • Palpable snapping sensation or crepitus over the A1 pulley • Tenderness over the A1 pulley • Palpable nodule in the line of the FDS, just distal to the MCP joint in the palm • Fixed-flexion deformity in late presentations, especially the PIP joint • Evidence of associated conditions (eg, RA, gout) • Early signs of triggering in other digits (may be bilateral)

TRIGGER FINGERTRIGGER FINGER
STAGING: Green's classification
• Grade I (pretriggering) - Pain; history of catching that is not demonstrable on clinical examination; tenderness over the A1 pulley
• Grade II (active) - Demonstrable catching, but the patient can actively extend the digit
• Grade III (passive) - Demonstrable locking, requiring passive extension (grade III A) or inability to actively flex (grade III B)
• Grade IV (contracture) - Demonstrable catching, with a fixed flexion contracture of the PIP joint
TRIGGER FINGERTRIGGER FINGER
TREATMENT
• Steroid injection into the tendon sheath.
A highly satisfactory rate of success can be predicted in female patients and in patients with single digit involvement, a discrete palpable nodule, short duration of symptoms (ie, <4 mo), or no associated conditions (eg, RA, DM).
2. Splinting.
For those patients who decline injection, consider splinting the involved digit. The MCP joint is splinted in approximately 15° of flexion. Very few series use splinting in isolation. Although results are claimed to be efficacious, splinting clearly is inferior to injection treatment or surgery

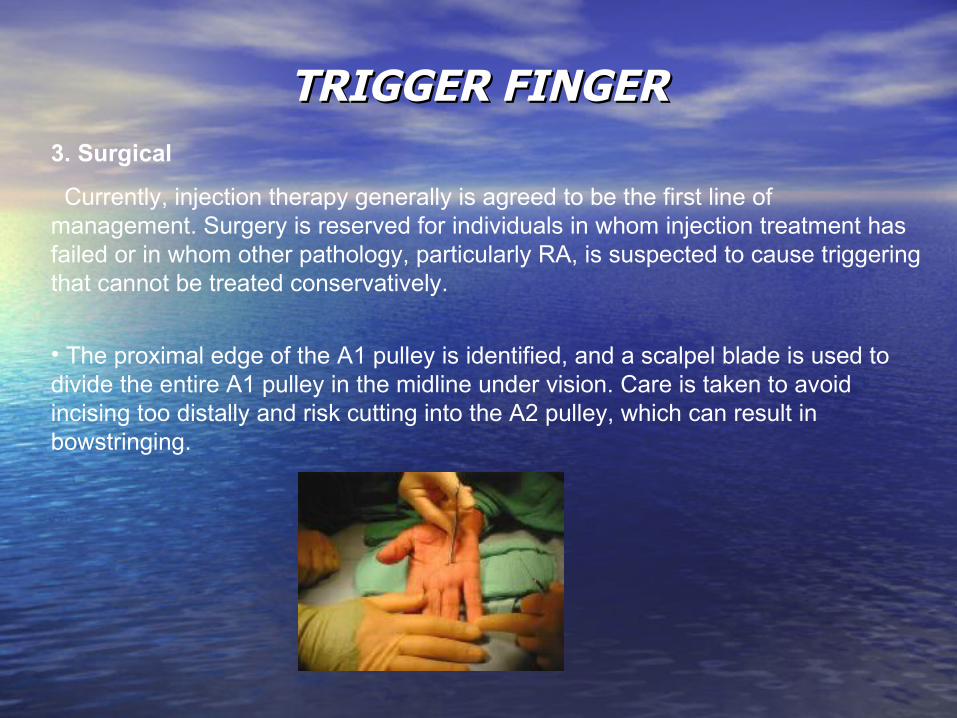
TRIGGER FINGERTRIGGER FINGER3. Surgical
Currently, injection therapy generally is agreed to be the first line of management. Surgery is reserved for individuals in whom injection treatment has failed or in whom other pathology, particularly RA, is suspected to cause triggering that cannot be treated conservatively.
• The MP joint is hyperextended to displace the neurovascular structures dorsally.

TRIGGER FINGERTRIGGER FINGER3. Surgical
Currently, injection therapy generally is agreed to be the first line of management. Surgery is reserved for individuals in whom injection treatment has failed or in whom other pathology, particularly RA, is suspected to cause triggering that cannot be treated conservatively.
• A transverse incision measuring 1-1.5 cm is made over the involved metacarpal head.
TRIGGER FINGERTRIGGER FINGER3. Surgical
Currently, injection therapy generally is agreed to be the first line of management. Surgery is reserved for individuals in whom injection treatment has failed or in whom other pathology, particularly RA, is suspected to cause triggering that cannot be treated conservatively.
• The proximal edge of the A1 pulley is identified, and a scalpel blade is used to divide the entire A1 pulley in the midline under vision. Care is taken to avoid incising too distally and risk cutting into the A2 pulley, which can result in bowstringing.

TRIGGER FINGERTRIGGER FINGER3. Surgical
Currently, injection therapy generally is agreed to be the first line of management. Surgery is reserved for individuals in whom injection treatment has failed or in whom other pathology, particularly RA, is suspected to cause triggering that cannot be treated conservatively.
•The patient is asked to actively move the digit to confirm full release.
•The hand is left free, and motion is encouraged immediately following the procedure.
DEFINITIONDEFINITION..
A localized formation of scar tissue in the palm of the hand. A localized formation of scar tissue in the palm of the hand. The scarring accumulates in a tissue called the fascia beneath The scarring accumulates in a tissue called the fascia beneath the skin of the palm that normally covers the tendons that pull the skin of the palm that normally covers the tendons that pull the fingers grip. As Dupuytren contracture progresses, more of the fingers grip. As Dupuytren contracture progresses, more of the fascia becomes thickened and shortened. Dimpling and the fascia becomes thickened and shortened. Dimpling and puckering of the skin over the area eventually occur.puckering of the skin over the area eventually occur.
DUPUYTREN’S DISSEASEDUPUYTREN’S DISSEASE
AETIOLOGY.AETIOLOGY. Unknown but Unknown but Oxygen free radicals stimulate myofibroblast proliferation Oxygen free radicals stimulate myofibroblast proliferation
& increases in & increases in type III collagen type III collagen and platelet derived growth factor B: and platelet derived growth factor B: Associated with:Associated with:
• Anglo-Saxons • Family history:autosomal dominant; 68% prevelance in first-degree
relatives
• - Epileptics (42%) • - Alcohol-induced liver disease • - Diabetes mellitus • - COAD • - hypertension • - IHD
DUPUYTREN’S DISSEASEDUPUYTREN’S DISSEASE

DUPUYTREN’S DISSEASEDUPUYTREN’S DISSEASE
PATHOANATOMY PATHOANATOMY
Pretendinous cord causes MCPJ contractures
Central & spiral cords cause PIPJ contractures
The spiral cord pushes the NVB towards the skin & midline of the finger.
Involvement of the natatory ligament causes web
space contractures.
The superficial transverse ligament is not involved
Sagittal fibres are not involved in the disease process
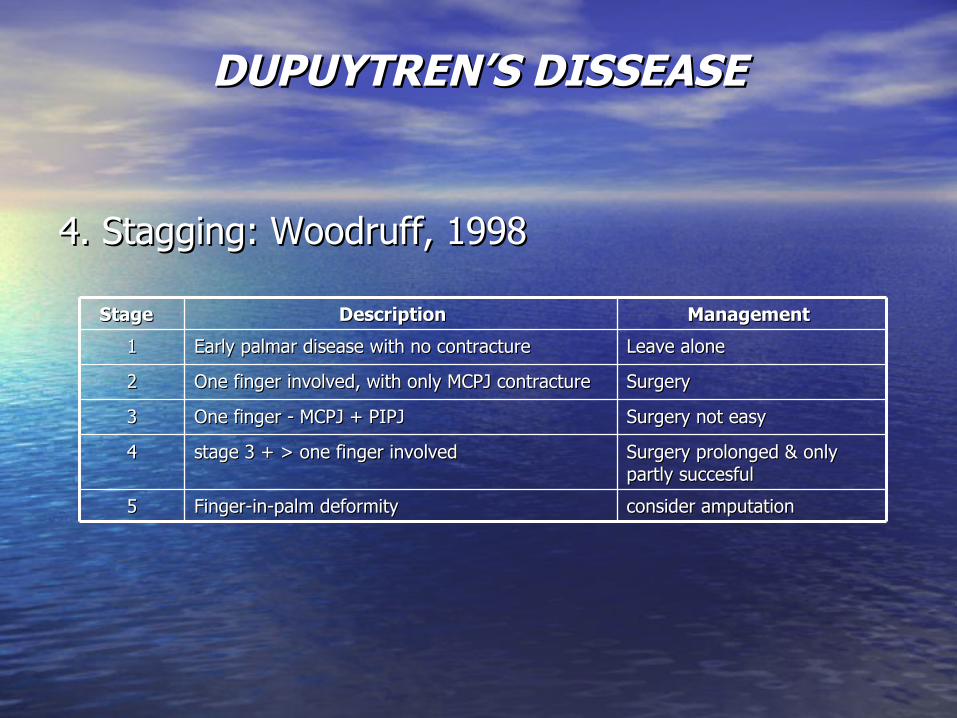
4. Stagging: 4. Stagging: Woodruff, 1998 Woodruff, 1998
DUPUYTREN’S DISSEASEDUPUYTREN’S DISSEASE
Stage Stage Description Description ManagementManagement
11 Early palmar disease with no contracture Early palmar disease with no contracture Leave alone Leave alone
22 One finger involved, with only MCPJ contracture One finger involved, with only MCPJ contracture Surgery Surgery
33 One finger - MCPJ + PIPJ One finger - MCPJ + PIPJ Surgery not easy Surgery not easy
44 stage 3 + > one finger involved stage 3 + > one finger involved Surgery prolonged & only Surgery prolonged & only partly succesful partly succesful
55 Finger-in-palm deformity Finger-in-palm deformity consider amputation consider amputation

5. Indications for surgery5. Indications for surgery
DUPUYTREN’S DISSEASEDUPUYTREN’S DISSEASE
•No absolute indications. •Surgery indicated when patient is inconvenienced or incapacitated by the contracture. •Tabletop test of Hueston = Patient unable to place hand flat on table due to contractures. If negative surgery is not indicated.

6. AIMS OF SURGERY 6. AIMS OF SURGERY
• Excise the diseased fascia. Excise the diseased fascia.
• Release digital contractures. Release digital contractures.
• Retain full flexion of the digits. Retain full flexion of the digits.
• Preserve neurovascular structures.Preserve neurovascular structures.
DUPUYTREN’S DISSEASEDUPUYTREN’S DISSEASE

DUPUYTREN’S DISSEASEDUPUYTREN’S DISSEASE
7. SURGICAL TECHNIQUE
Incision Incision Advantages Advantages Disadvantages Disadvantages
Transverse midpalm Transverse midpalm
for pretendinous band - for pretendinous band - can be left open can be left open (McCash technique) or (McCash technique) or Full thickness graft Full thickness graft (Hueston) (Hueston)
Requires frequent Requires frequent dressings & dressings & cooperation post-op. cooperation post-op.
Bruner's zig-zag Bruner's zig-zag Good exposure Good exposure
Can be difficult to raise Can be difficult to raise flaps if skin is thin, flaps if skin is thin, incr. risk of NVB incr. risk of NVB damage, can cause damage, can cause troublesome scarring troublesome scarring at the sides & base of at the sides & base of finger. finger.
Longit. incision & Longit. incision & Z-plasties Z-plasties
Good exposure, less Good exposure, less chance of damaging chance of damaging NVB NVB
Can be difficult to match Can be difficult to match incisions in 2 finger incisions in 2 finger diseasedisease

DUPUYTREN’S DISSEASEDUPUYTREN’S DISSEASE
7. Procedures
• Fasciotomy
• Partial Selective Fasciectomy (Skoog)
• Total Fasciectomy (McIndoe)
• Dermofasciectomy (Hueston)
• External Fixator (Messina)
• Amputation for finger-in-palm deformity with macerated skin

9. POST-OPERATIVE CARE 9. POST-OPERATIVE CARE • Splint hand with wrist extended & fingers in a Splint hand with wrist extended & fingers in a
comfortably extended position. comfortably extended position. • Check wounds at 48hrs. & apply Thermoplastic splint. Check wounds at 48hrs. & apply Thermoplastic splint. • Regular dressings for McCash open palm. Regular dressings for McCash open palm. • Hand therapy Hand therapy • active program active program • scar care (massage, silicone pressure pad, compression scar care (massage, silicone pressure pad, compression
wrap) wrap) • determines 50% of the final result determines 50% of the final result • Continue for 3 months Continue for 3 months • Night splint for 6 months. Night splint for 6 months.
DUPUYTREN’S DISSEASEDUPUYTREN’S DISSEASE

DUPUYTREN’S DISSEASEDUPUYTREN’S DISSEASE
8. COMPLICATIONS
• digital nerve division • ischaemic digit - from digital artery spasm or kinking or division • haematoma • skin loss / necrosis • infection (treated with early debridement) (use of K wires is thought to
promote infection) • scar contracture • joint stiffness • CRPS - look for swelling, pain, stiffness, and discoloration; - causes: -
neuroma formation - digital nerve scarring at the incision site; - excessive wound tension;
• secondary carpal tunnel syndrome (from edema) • secondary trigger finger • recurrent disease

GANGLIONSGANGLIONS
Cystic swollen in the neigbourhood of tendon or joint.
Ganglion cysts are generally asymptomatic or minimally symptomatic. Symptoms such as limitation of motion, pain, paresthesias, and weakness are possible.

GANGLIONSGANGLIONS
FRECUENCY• Ganglion cysts are the most common soft tissue tumors of the hand and wrist.
• 15% of ganglion cysts occur in patients younger than 21 years.
• 70 % of ganglion cysts occur in patients between the second and fourth decades of life.
• Women/men 3:1
• Ganglions are usually solitary, and they rarely exceed 2 cm in diameter.
GANGLIONSGANGLIONS
ETIOLOGY
A more recent theory, attributes cyst formation to trauma or tissue irritation. Modified synovial cells lining the synovial-capsular interface are stimulated to produce mucin.
GANGLIONSGANGLIONS
GANGLION SITE
• 60-70 % dorsal wrist ganglion: Scapholunate joint
• 18-20 % volar ganglion.
• 10-20% in the flexor sheath.
• Occult dorsal ganglion: tenderness around the scapholunate fossa region. Pain occurs with extreme wrist motion, especially in extension. Radiographic findings are often normal, and MRI is useful in confirming the diagnosis.

GANGLIONSGANGLIONS
TREATMENT: INDICATIONS
• Limitation of motion
• Pain
• Weakness
• Paresthesias.
• ? Malignancy.
• Cysts that drain externally require attention because of the risk of development of a serious joint or soft tissue infection.
• Stetic

GANGLIONSGANGLIONS
TREATMENT
• Non-surgical:
ASPIRATION +/- STEROID INJECTION
• Surgical:
TOTAL GANGLIONECTOMY WITH REMOVAL OF A MODEST PORTION OF THE ATTACHED CAPSULE

GANGLIONSGANGLIONS
COMPLICATIONS
• Ganglion recurrence.
• Infection, bleeding, nerve and tendon injury, scarring, joint instability, and vascular injury .

THANK YOU





























