Embed Size (px)
Citation preview

EVIDENCE-BASED MANAGEMENT OF PCOS
BUDI SANTOSO
HALAL BI HALAL- 17 JULI 2016

References


Evidence-based guideline for the
assessment and management of
polycystic ovary syndrome
Developed 2011
Updated August 2015 - Section 7.4 Aromatase
inhibitors
Further update scheduled 2016/2017

An Overview of the Magnitude of The Problem of PCOS
Prevalence~ 20%
ComplexPathophy-
siology
Diagnosis2003
Women’s HealthAspects
2011
Treatment & Outcome
2007
Three ESHRE/ASRM PCOS Consensus Workshops
Approximately 75% of PCOS women suffer from infertility due to anovulation.

EVIDENCE-BASED MANAGEMENT OF PCOS
Surgical• Laparoscopic Ovarian Drilling• Bariatric Surgery
Pharmacological• Clomiphene Citrate• Metformin• Aromatase inhibitors• Gonadotropins
Non PharmacologicalLife style modification

Lifestyle intervention (to optimise preconception health, fertility and long-term complications)
Lifestyle interventions include diet, exercise, behavioralmanagement techniques for modifying diet or exercise,or a combination of these.
1st Line Non Pharmacological management for Infertility

Lifestyle change
4 RCTs, (20, 21, 46 and 343 PCOS Obese/over weight
womens) intervension groups VS lifestyle
Metformin only, CC only, Metformin + CC ( 24 – 28 weeks) VS
( diet only, diet + exercise, and diet + exercise + behavioral).
No significant different between Lifestyle VS pharmaceutical
in term of menstrual fuction, pregnancy rate
Pasquali , 143 obese PCOS women, RCTs metformin + diet VS placebo + diet
Menstrual improvement : 4.3 vs 3.2 ( p= 0,017)No diff. in pregnancy rate

Secara singkat, bukti2 RCT tidak mendukung pengobatan
dengan induksi ovulasi seperti CC/metformin yang
mendahului treatment gaya hidup atau memulai
treatment gaya hidup yang dikombinasi dengan
pengobatan induksi ovulasi dibandingkan dengan tretmen
gaya hidup saja pada wanita obes infertil anovulatoar
dengan PCOS

Balen Adam H. et.al. 2005 Polycystic ovary syndrome a guide to clinical management.
Lifestyle change is the first line treatment for womenwith PCOS who are over weight or obese, with as littleas 5-10 % weight loss improving psycological outcome,reproductive features and metabolic features.
Amplification of sign and symtoms of PCOS with
Increasing obesity and insulin resistance

Clomiphene Citrate• 1967
• as anti estrogenic and estrogenic
• competitive binding ER
• Studies with clomiphene citrate show
ovulation rates of 60%–85% and
pregnancy rates of 30%–50% after six
ovulatory cycles.
• The rates of twin 5%-7% and triplet
pregnancy 0.3%, respectively.
• The incidence of OHSS less than 1%
- Usadi, R, Fritz, M, Glob. libr. women's med., (ISSN: 1756-2228) 2008; DOI 10.3843/GLOWM.10337
- Teede et al, Med J Australia 2011

Clomifene citrate
If ovulation cannot be achieved with clomifene citrate,
then the patient is said to have clomifene citrate
resistance. If pregnancy cannot be achieved after six
ovulatory cycles with clomifene citrate, then the patient is
described as having clomifene citrate failure.
Systematic review and meta-analysis 3 RCTs comparing
CC VS placebo, 3 trials 133 patients CC improves ovulation
rate and pregnancy rate, but no publish CC VS placebo/ no
treatment examining live- birth as outcome.

1st line Pharmacological management for Infertility
Teede et al, Med J Australia 2011
Evidence based recommendation:
CC should be fisrt line pharmacological therapy to improve
fertility No other infertility factor. CC is selective estrogen
receptor modulator with both estrogenic and anti estrogenic
properties.
Clinical practice point:
The risk of multiple pregnancy is increased with CC use and
therefore monitoring is recommended.

METFORMIN
Biguanide
Rationale as ISA to retore ovulation
1994 as tretment for PCOS
Adnistration metformin for PCOS many protocol : 1500 –
2550 mg.
The most adverse reaction gastrointestinal symtoms

Metformin
o Metformin alone has been shown to improve ovulation and
clinical pregnancy rate but not live- birth rate.
o Metformin combined with clomifene citrate has a higher
ovulation, pregnancy and live-birth rate compared with
clomifene citrate alone only in clomifene citrate-resistant
(CCR) PCOS.

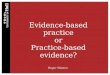
Table 1:RandomizedControlledTrials Comparing ClomipheneCitrate withMetformin inPCOS Women
Source: Costello & Ledger, 2012

Metformin
o Fertility outcomes are improved with the addition of
clomifene citrate to metformin compared with
metformin alone in obese PCOS women (BMI >= 30
kg/m2).
o There is no improvement in fertility outcomes when
metformin is combined with laparoscopic ovarian
drilling, gonadotropin ovulation induction with timed
intercourse, or IVF. However, metformin
coadministration with IVF results in a 70 –80% lower risk
of OHSS

MetforminClinical question. In women with PCOS, is metformin effective for improving fertility outcomes?
Teede et al, Med J Australia 2011
Evidence-based recommendations
Metformin should be combined with clomiphene citrate to improve fertility outcomes
rather than persisting with further treatment with clomiphene citrate alone in women
with PCOS who are clomiphene citrate resistant, anovulatory and infertile with no
other infertility factors.

Gonadotrophins
Gonadotrophins are often used as second-line therapy in
anovulatory PCOS women with CCR (Clomiphene Citrate
Resistance) and CCF (Clomiphene Citrate Failure).
Recent randomized evidence suggests that gonadotropin
therapy may be more effective than clomifene citrate in therapy-
naive PCOS women. Low dose Gonadotropin 70%
monofollicular, PR per ovulatory 15-20%, cumulatif PR 55-70%.
Increased risk of multiple pregnancy and OHSS 1% A low-
dose “step up” protocol
The duration gonadotropin therapy should not exceed 6 ovulatory
cycles
Teede et al, Med J Australia 2011

Gonadotrophins
Cohcrane systemic review rFSH and uFSH no different, in OR, PR, MP and MCR in treatment CCR women with PCOS
2 RCTs FSH induction ovulation VS CC in treatment 76 women with PCOS Improvement in pregnancy rate, no different in live birth, no different in OR, and no Diff in MP.
The second RCT low dose step up of FSH VS CC in 255 women PCOS FSH higher PR and LBR
But > cost and inconvinient
SECOND LINE TREATMENT

Aromatase inhibitors were proposed as ovulation-inducing agents in 2001.
Letrozole and anastrozole are the most commeonly in IO
Aromatase Inhibitors
Aromase Inhibitor === biosyntesa estogen (interfering H/P)
increasing FSH
Growing Follicle
The effectiveness of letrozole is not better than CC
There is conflicting published data on the potential teratogenic
effect of letrozole when used as an ovulation induction agent.
D

LAPAROSCOPI OVARIAN DRILLING
Laparoscopic ovarian “driling” was first
described in
1984
Mechanisms underpinning hormonal
changes
and resumption of ovulation remain
poorly
understood.
Result 6 month : OR 54-76%, PR 28-
76%,
12 month: OR: 33-88%, PR: 54-
70%
Laparoscopic ovarian drilling in PCOS is
thought:

LOD When Recommended?
Second line Tx. CC resistence
in PCOS Patients, alternative
gonadotropin equal in efficacy
but lower of MP and Cost
Hypersecretion LH
Who need laparoscopy?
Who live too far from hospital intensive monitoring during gonadotropin tx

Bariatric Surgery
• Bariatric/ Weight surgery result in aproximally 15-30% weight loss
• A Cohrane review -> conventional Tx in obesity reduce DM, Hypertension based on 3 RCTs, did not assess fertility outcome
• There not any published RCTs assesing the effectiveness of bariatric surgery specifically in PCOS women.
• Another systemic review based in reproductive outcome improve fertility and reduction obstetric complication ( DM in pregnancy, macrosomia, hypertension disorder), but IUGR increase.
• A recent study reported that bariatric surgeryis a potential future tratment option for obese PCOS women, the criteria still large debateble and more scientific research is required

2nd line pharmacological/surgical management
3st line management could be other approriate intervension
1st line Non Pharmacological management for Infertility
Don’t use Aromatesinhibitor as First Tx. (B)
LOD (B)
Under caution
CC+Met (A)
Management of Infertility in women with PCOS
Gonadotropin (B)
Metformin, if BMI <=35 (B)
Bariatric surgery (CR)
Arom Inhibit (D)
Only women CC rest, anovulatoar, infertil with no
other fertility factor
Lifestyle intervension(C)
1st Line Pharmacological managent for Infertility
Clomiphen C (A)
Only for adult who are anovulatory and have a BMI >= 35 kr/m2 and who remain infertile despiter undertaking an intensive structured lifestyle management program
for minimum of 6 months