Embed Size (px)
Citation preview
Evidence Based Practical Tips
For
Luteal Phase Support
Dr. Shashwat Jani.M. S. ( Obs – Gyn )
Diploma in Advance Laparoscopy.
Consultant Assistant Professor,
Smt. N.H.L. Municipal Medical College.
Sheth V. S. General Hospital , Ahmedabad.
Mobile : 99099 44160.
E-mail : [email protected]
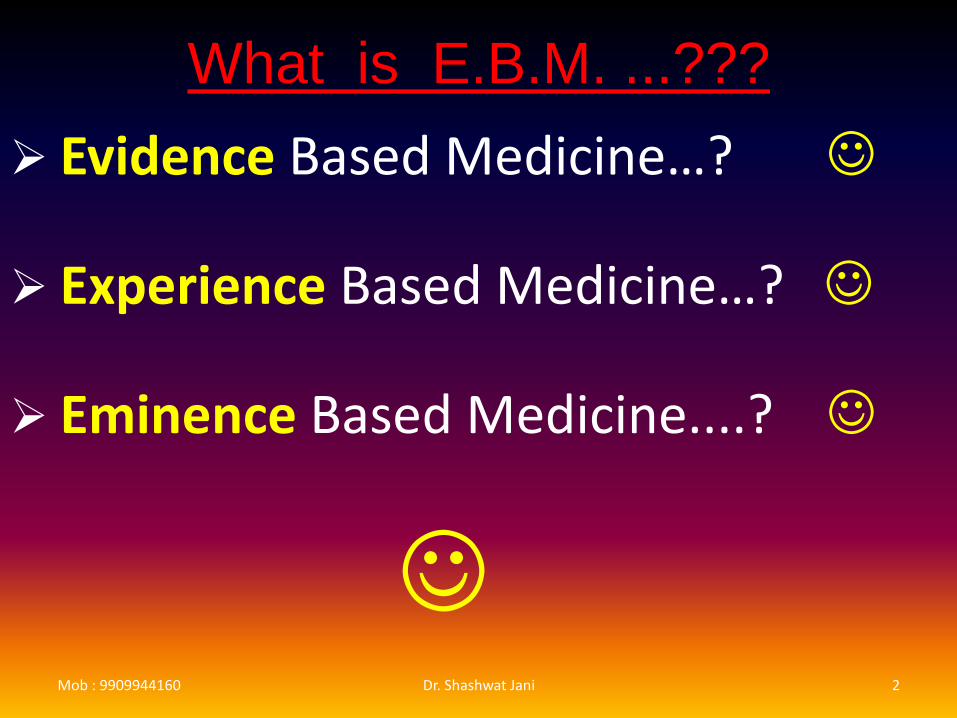
What is E.B.M. ...???
Evidence Based Medicine…?
Experience Based Medicine…?
Eminence Based Medicine....?
Mob : 9909944160 Dr. Shashwat Jani 2
Mob : 9909944160 Dr. Shashwat Jani 3
Sources
Cochrane library .
Royal College of Obstetricians &Gynecologists (RCOG) Guidelines.
American Society of Reproductive Medicine (ASRM)
( April, 2015 )
European Society of Human Reproduction & Endocrinology
( ESHRE )
National Institute of Health & Care Excellence. ( NICE )
Journal of Evidence Based Obstetrics & Gynecology.
National Guideline Clearinghouse . ( U.S. Govt. ).
Royal Austr. & NZ College of Obst. & Gynec .( RANZCOG )
PubMed.Mob : 9909944160 4Dr. Shashwat Jani
Once Upon a Time….
ƒ In 1949, the premature onset of menses was recognized as indicative of a luteal phase deficiency of progesterone production, which was shown to be correctable by exogenous progesterone administration (Jones, 1979). ƒ
The prevalence of a luteal phase defect in natural cycles in normo-ovulatory patients with primary or secondary infertility was demonstrated to be about 8.1%
(Rosenberg et al., 1980)
Mob : 9909944160 5Dr. Shashwat Jani
Maintenance of
pregnancy Corpus luteum Progesterone
– After ovulation ~ during the early first trimester ~ until placental function established
– Removal of the corpus luteum spontaneous pregnancy loss
Ovarian progesterone production implantation & early pregnancy support.
Mob : 9909944160 6Dr. Shashwat Jani
Luteal phase deficiency (LPD)
Endogenous progesterone is NOT sufficient to
– Maintain a functional secretory endometrium
– Allow normal embryo implantation and growth
– 1st described in 1949.
Mob : 9909944160 7Dr. Shashwat Jani
Who requires
Luteal Phase Support ? Confirmed cases of luteal phase defect Unexplained infertility Advanced reproductive age ART techniques – IUI / IVF / ICSI Hyper- prolactinaemia All down regulated cycles Recurrent pregnancy loss PCOS Women with strenous exercises and
underweight Who require Luteal support .
Mob : 9909944160 8Dr. Shashwat Jani
Luteal Phase Deficiency (LPD)
Purportedly been associated with:
1. Infertility
2. 1st trimester pregnancy loss
3. Short cycles
4. Premenstrual spotting
5. Anorexia
6. Starvation
7. Eating disorders
8. Excessive exercise
9. Stress
10. Obesity & PCOS
11. Endometriosis
12. Aging
13. Inadequately treated 21-hydroxylase deficiency
14. Thyroid dysfunction & hyperprolactinemia
15. Ovulation stimulation alone
16. Ovulation induction with or without GnRH agonists
17. ART
Mob : 9909944160 9Dr. Shashwat Jani
Luteal Phase Deficiency (LPD)
Has been shown to occur:
During the postpartum period
With significant weight loss or exercise
In random cycles of normally menstruating women.
Mob : 9909944160 10Dr. Shashwat Jani
Are There Diagnostic
Criteria For
Inadequate Luteal Function ???
Mob : 9909944160 Dr. Shashwat Jani 11
Diagnostic tests are influenced by and based on the following
Physiologic observations:
1. Normal luteal phase length is relatively fixed at 12 – 14 days.
2. Progesterone levels peak in nonpregnancycycles 6–8 days after ovulation.
3. Progesterone is secreted in pulses.
12
4. The endometrial response is a reflection of the follicular phase estrogen and the luteal-phase estrogen and progesterone.
5. Once implantation occurs, progesterone secretion by the corpus luteum depends on rising hCG levels.
6. Failure of hCG levels to increase directly causes corpus luteum failure and a decline in progesterone levels.
Mob : 9909944160 Dr. Shashwat Jani 13
Methods proposed for diagnosing LPD
Basal body temperature (BBT) charting:
Inaccuracy, inconvenience, should be discouraged
Serum progesterone levels
Endometrial biopsy
TVS
Ovulation & adequate luteal length:
Urinary LH surge detection & Monitoring of luteallength
Mob : 9909944160 14Dr. Shashwat Jani
Sonographic Criteria :
Rupture of follicle < 17 mm
Poorly formed or ill defined dominant follicle
Luteinised unruptured follicle ( LUF )
Lutein cyst formation
Absence of corpus luteum
Lack of endometrial echogenicity on 7th postovulatory day .
Mob : 9909944160 15Dr. Shashwat Jani
Endometrial Biopsy
Abnormalities of endometrial maturation:• Inadequate ovarian hormone secretion
• Intrinsic endometrial abnormality
• ‘‘Gold standard’’ to diagnose luteal inadequacy.
However, prospective, blinded, randomized clinical trials (RCTs) suggest that the endometrial biopsy is an imprecise tool for differentiating fertile women from women with LPD (infertility).
16
April 2015
In summary, currently there is no reproducible, pathophysiologically relevant, and clinically practical standard to diagnose LPD and distinguish fertile from infertile women.
The roles of BBT, urinary LH detection kits, lutealprogesterone levels, endometrial biopsy, and other diagnostic studies have not been established, and performance of these tests cannot be recommended.
Mob : 9909944160 17Dr. Shashwat Jani
If Diagnosis Is Not
Possible,
Is Treatment For
Luteal Inadequacy
Ever Appropriate ???
Mob : 9909944160 18Dr. Shashwat Jani
Treatment Of Potential Luteal
Inadequacy
1st approach: Correction of any underlying
condition …(hypothalamic or thyroid dysfunction, hyperprolactinemia)
2nd approach : Empiric Treatment
(based on limited reliable data)
• Promote endometrial maturation
• Enhance endometrial receptivity
• Support implantation and development of an early pregnancy
Mob : 9909944160 19Dr. Shashwat Jani
What to use for LPS …???
Progesterone,
progesterone + estrogen,
hCG
Ovulation induction with clomiphene or gonadotropins
GnRHa
Prednisolone
Aspirin
Heparin
Ascorbic acid
ImmunoglobulinsMob : 9909944160 20Dr. Shashwat Jani
PROGESTERONE
Mob : 9909944160 21Dr. Shashwat Jani
Action
Improves endometrial receptivity
(Kolibianakis & Devroy, 2002)
Promotes local Vasodilatation and uterine musculature quiescence by inducing nitric oxide synthesis in decidua
(Bulletti & de Ziegler, 2005)
Act as immunologic suppressant blocking Th1 and inducing release of Th2 cytokines
Mob : 9909944160 22Dr. Shashwat Jani
I. M. Progesterone
Effective
Physiological serum levels
Painful (long, thick needles)
Occasional sterile abscess
Occasional allergic reaction (oil vehicle)
Needs to be administered by trained person
Acute eosinophilic pneumonia associated with IM administration of progesterone as luteal phase support after IVF: 3 case report
Mob : 9909944160 23Dr. Shashwat Jani
Vaginal Progesterone
Effective
Convenient (self-administration)
First uterine pass effect / targeted delivery
Might require multiple dosing /day (suppositories)
High uterine concentration of progesterone
Minimizes the potential for adverse systemic effects (Bulletti et al., 1997)
Mob : 9909944160 24Dr. Shashwat Jani
Dosage Micronized Progesterone:
No dose finding studies. Most frequently:
300–600 mg daily, spread over 2-3 dosages
(Tavaniotou et al., 2000; ASRM, 2013 ) Vaginal progesterone pessaries:
no dose finding studies. Most frequently used:
400-800 mg daily, spread over 3-4 doses
(NG et al, 2002, Tay et al, 2005)
Mob : 9909944160 25Dr. Shashwat Jani
Vaginal Gel
8% gel in a dose of 90 mg once daily
No differences when administered twice daily
(Tavaniotou et al, 2000)
Low dose or high dose vaginal progesterone gel
Both are equally effective
(van der Linden et al., 2012)
Mob : 9909944160 26Dr. Shashwat Jani
Which Vaginal
Preparation…???
Gel or Capsules ? Both are equally effective (Daya & Grundy, 2004)
Capsule: solid evidence of effectiveness and convenience (Elenany et al, 2011) more cost effective than gel.
Gel is at least 4 times more expensive than Capsules.
No difference exists regarding CPR between vaginal P gel and all other vaginal preparations for LPS
(MA: Polyzoz et al, 2010)
Mob : 9909944160 27Dr. Shashwat Jani
Oral Progesterone
Ineffective ?
Low bioavailability
High rate of metabolites
(scant endometrial effect)
High rate of side effects (somnolence)
Mob : 9909944160 28Dr. Shashwat Jani
Rectal Progesterone
Resulted in serum concentration during the first 8h twice as high as other forms.
No prospective RCT to compare the rectal administration of progesterone with other administration routes for IVF
(Chakmakijan & Zachariah, 2008)
Mob : 9909944160 29Dr. Shashwat Jani
S/C Progesterone
A new water-soluble progesterone
Implantation rate, PR, LBR and early miscarriage rate for Prolutex were similar to those for Crinone.
The adverse event profiles were similar and Prolutex was safe and well tolerated.
Less painful than IM
Mob : 9909944160 30Dr. Shashwat Jani
Which is better…??? Oral or I.M. progesterone ?
Definitely I.M. progesterone
(Daya & Grundy, 2004)
Oral or vaginal progesterone ?
Definitely vaginal progesterone
(Daya & Grundy, 2004)
I.M. or vaginal progesterone ?
Both are equally effective No difference in CPR (Daya & Grundy, 2004; MA: Zarutiski & Philips, 2009)
Mob : 9909944160 31Dr. Shashwat Jani
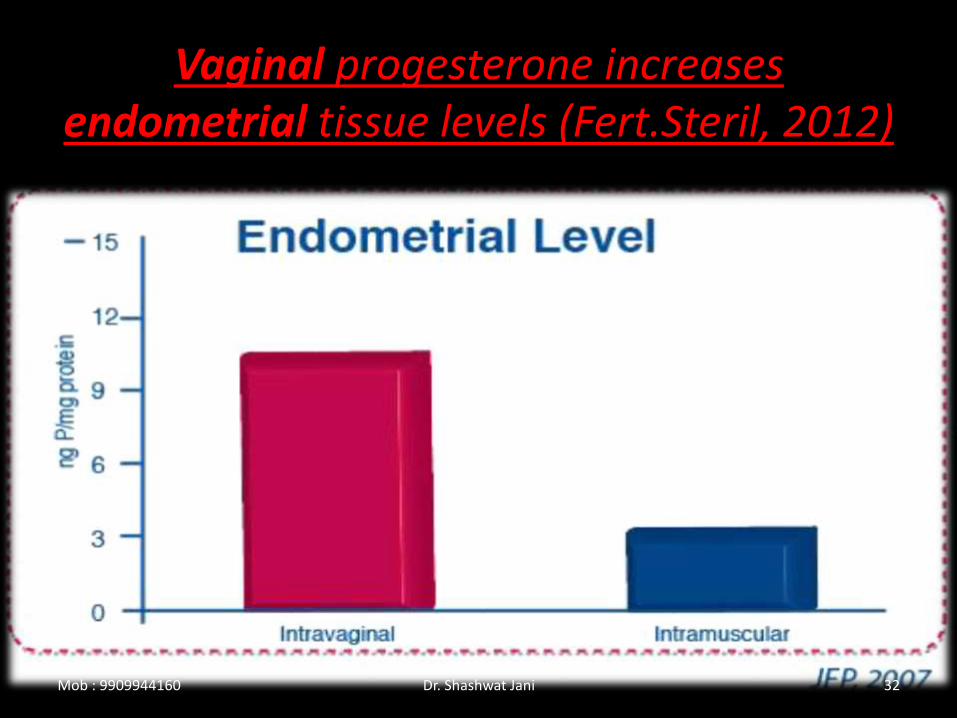
Vaginal progesterone increases endometrial tissue levels (Fert.Steril, 2012)
Mob : 9909944160 32Dr. Shashwat Jani
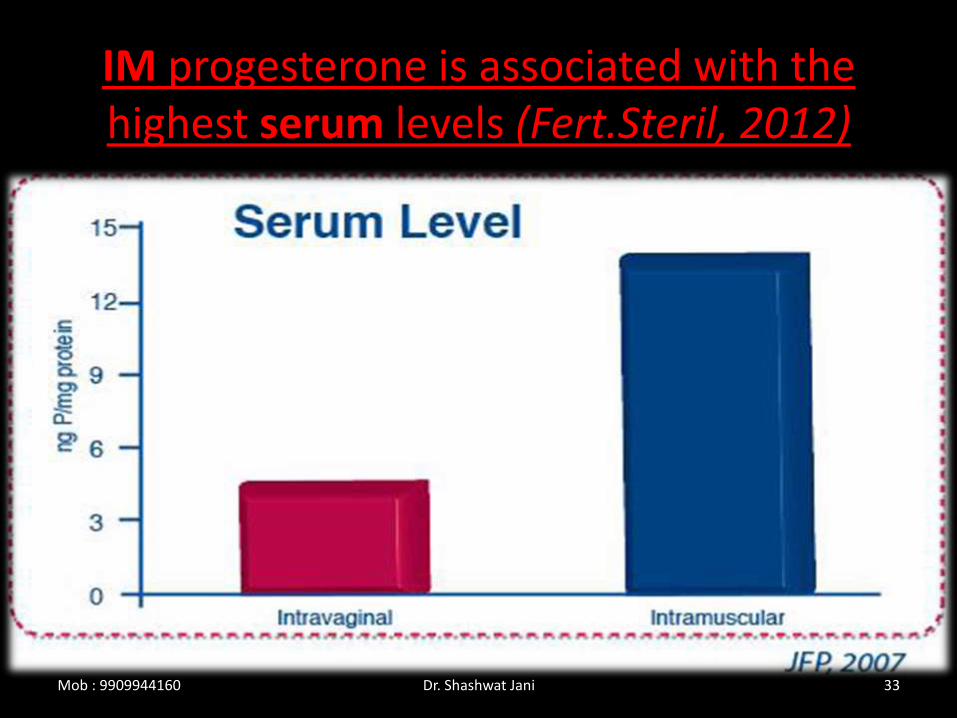
IM progesterone is associated with the highest serum levels (Fert.Steril, 2012)
Mob : 9909944160 33Dr. Shashwat Jani
For Ideal LPS…
IM Progesterone for the Highest Serum levels and Vaginal Progesterone for increasing the Endometrial levels, Until Placental progesterone production adequate, around week 8-10 w of gestation.
(Fert.Steril, 2012)
Mob : 9909944160 34Dr. Shashwat Jani
Mob : 9909944160 35Dr. Shashwat Jani

hCG
Mob : 9909944160 36Dr. Shashwat Jani
hCG “Progesterone and estradiol are hormone
supplementations, whereas hCG is used to stimulate these hormones in the corpora lutea. “
Placental protein 14 (Anthony et al., 1993), integrin άν (Honda et al., 1997) and relaxin (lutelpeptide hormone) concentrations, which has been shown to increase at the time of implantation are higher with hCG support ( Ghosh and Sengupta, 1998).
Mob : 9909944160 37Dr. Shashwat Jani
Limitations
OHSS.
Luteal support with hCG should be avoided: ƒ
- If E2 >2700pg/ml (Buvat et al., 1990) ƒ - If Number of follicles is >10 (Araujo et
al., 1994)
Mob : 9909944160 38Dr. Shashwat Jani
Which is better…???
Progesterone is as effective as hCG for luteal phase support but provides a higher safety with regard to ovarian hyper-stimulation syndrome .
(Ludwig and Diedrich, 2001)
( RANZCOG 2014 )
Mob : 9909944160 39Dr. Shashwat Jani
E2
No effect of oral estrogens
(van der Linden et al., 2012)
Transdermal estrogen is beneficial
(van der Linden et al., 2012)
No effect in antagonist protocol
Mob : 9909944160 40Dr. Shashwat Jani
Low dose Aspirin
M.O.A : Vasodilatation and decreased platelet
aggregation, increased ovarian and endometrial blood flow, ovarian responsiveness, endometrial thickness, decrease uterine contraction at the time of ET
Low-dose aspirin (100 mg/d) doesn’t improve ovarian responsiveness, blood flow, and PR
(Dirckx et al., 2009; Lambers et al., 2009).
Mob : 9909944160 41Dr. Shashwat Jani
Piroxicam
An oral dose 10 mg 1-2 h before ET
significantly improves PR (Moon., 2004)
Doesn’t improve PR (Dal and Borini, 2009)
Mob : 9909944160 42Dr. Shashwat Jani
Indomethacin
100 mg q12h rectally for 3 doses from the night before ET does not improve PR in oocyterecipients
(Bernabue, 2006)
43Dr. Shashwat Jani
Low dose Heparin
5000 IU BD and Aspirin 100 mg/day from the day of ET did not improve PR or IR.
(Stern et al., 2003)
Mob : 9909944160 44Dr. Shashwat Jani
Prednisolone
• 10 mg/d before or after ET does not increase PR
(Ubaldi et al., 2002)
Mob : 9909944160 45Dr. Shashwat Jani
Sildenafil
25 mg qid
vaginally from stimulation D1 to hCG day.
(Sher, 2002;
Paulus,2002)
Not Recommended…. ( ESHRE , 2013 )
Mob : 9909944160 46Dr. Shashwat Jani
Ascorbic Acid
Luteal regression is associated with ascorbate depletion and the generation of reactive oxygen species, which inhibit the action of LH and block steroidogenesis
No value
(Griesinger et al.,2002)
Mob : 9909944160 47Dr. Shashwat Jani
GnRHa in Midluteal phase
• GnRH receptor is expressed in the human preimplantation embryos, endometrium, corpus luteum .
• GnRHa has been shown to stimulate trophoblast production of hCG .
• Increased LBR
(MA: Kyrou et al., 2008)
Mob : 9909944160 48Dr. Shashwat Jani

GnRHa Vs no treatment : GnRHa is beneficial (Glujovsky et al., 2010)
Effective (van der Linden et al., 2012)
Which GnRHa is more beneficial? No differences (Glujovsky et al., 2010)
Mob : 9909944160 49Dr. Shashwat Jani
Cochrane 2012
Single dose of 0.5 mg S/C on 6 th day after ICSI Increases implantation rate, CPR per transfer, increases live birth rate Single dose GnRH agonist.
Addition of GnRH agonist to progesterone improved outcome of live birth, clinical pregnancy and ongoing pregnancy .
Mob : 9909944160 50Dr. Shashwat Jani
Natural Cycle
No treatment for luteal phase insufficiency has been shown to improve pregnancy outcomes in natural, unstimulated cycles.
( ASRM April 2015 )
Mob : 9909944160 51Dr. Shashwat Jani
Ovulation Induction
Improved pre-ovulatory follicular dynamics Should improve corpus luteum function
Use of agents that induce ovulation Improved corpus luteum function & fertility outcomes.
( ASRM APRIL 2015 )
Mob : 9909944160 52Dr. Shashwat Jani
ART
For luteal support in assisted reproductive technologies (ART), exogenous progesterone supplementation is associated with a significantly higher pregnancy rate.
Strongly Recommended ( ASRM , 2015 )
Mob : 9909944160 53Dr. Shashwat Jani
Why in ART Cycles ?
Abnormal luteal function after COS for IVF
Suppression of LH
Continued down-regulation by GnRHa
Removal of granulosa cells at OR
Supra physiological E2/P4 in early luteal phase
hCG injection before OR
Mob : 9909944160 54Dr. Shashwat Jani
When to start..?
From day of OR or ET
Not be later than day 3 after OR
Mob : 9909944160 55Dr. Shashwat Jani
How long …???
Not established firmly
Often continued Unnecessarily till 12 week
Most evidence based studies suggest to continue till 9 weeks gestation
Mob : 9909944160 56Dr. Shashwat Jani
Pregnancy
First trimester progesterone supplementation in IVF may support early pregnancy through 7 weeks by delaying miscarriage but does not improve live birth rates .
First trimester progesterone supplementation in natural cycle pregnancies also does not prevent a miscarriage. (Wahabi et al., 2007)
Mob : 9909944160 57Dr. Shashwat Jani
Recurrent Miscarriage
There is insufficient evidence to evaluate the effect of progesterone supplementation in pregnancy to prevent a miscarriage .
(RCOG- Green Top Guidelines2011)
Mob : 9909944160 58Dr. Shashwat Jani
It was only in 2011 that Cochrane meta analysis suggested that progesterone supplementation has beneficial effects in patients with Recurrent Pregnancy Loss.
It dose, route, frequency & duration does not affect the outcome.
Cochrane 2011 for Recurrent Miscarriages
Mob : 9909944160 59Dr. Shashwat Jani
“ PRO MIS Trial “
PROgesterone in MIScarriage trial
Newer Evidence is coming up as large multicentre study PROMISE is currently on the Way…
Mob : 9909944160 60Dr. Shashwat Jani
Take Home Message
Abnormal luteal function may occur as the result of a medical condition (e.g., elevated prolactin, abnormal thyroid function), and infertile women suspected of having one of these disorders (e.g., irregular menses, galactorrhea) should be evaluated and appropriately treated for identified conditions.
Mob : 9909944160 61Dr. Shashwat Jani
No diagnostic test for luteal phase insufficiency has been proven to be reliable in a clinical setting.
The roles of BBT, urinary LH detection kits, luteal progesterone levels, endometrial biopsy, and other diagnostic studies have not been established, and performance of these tests cannot be recommended.
Mob : 9909944160 62Dr. Shashwat Jani
There is no proven role in adding progesterone or hCG for luteal support once a pregnancy has been established.
Use of supplemental progesterone in a non-ART cycle beyond the time of expected menses (i.e., 2 weeks after ovulation) is Not proven to be beneficial.
Mob : 9909944160 63Dr. Shashwat Jani
No treatment for luteal phase insufficiency has been shown to improve pregnancy outcomes in natural, unstimulated cycles.
Luteal support after ART procedures with progesterone or hCG improves pregnancy outcomes, but hCG increases the risk of OHSS.
Mob : 9909944160 64Dr. Shashwat Jani