Embed Size (px)
Citation preview
Progeria syndrome
By : Ahmed Elshahat SaiedSupervisor :DR,AZZA ATIA

Neoplasiafrom Ancient Greek - neo- "new" and plasia"formation, creation"), tumor or tumour
is an abnormal mass of tissue as a result of abnormal growth or division of cells
The term "cancer" implies malignancy, but neoplasms can be subclassified as either benign or malignant.

Nomenclature:
Neoplasms are named based upon two factors
1. on the histologic types :
2. on behavioral patterns : benign and malignant neoplasms
Thus, the suffix -oma denotes a benign neoplasm.
originating from, bone, fat, blood vessel nerve, fibrous tissue and cartilages are
named as, osteoma, lipoma, hemangioma, neuroma, fibroma and
chondroma respectively.

Malignant neoplasia :arising from tissue embryologically derived from ectoderm or endoderm are usually carcinomas. Examples include:
Squamous cell carcinoma of cervix Adenocarcinoma of stomach Hepatocellular carcinoma Renal cell carcinoma
Malignancies arising from mesoderm (connective tissues) are usually sarcomas. Examples include:
Leiomyosarcoma Chondrosarcoma Osteosarcoma
Liposarcoma
Neoplasms with more than one cell type but arising from only one germ layer are called "mixed tumors".
Neoplasms with more than one cell type and arising from more than one germ layer are called teratomas. Such neoplasms are common in the ovary.
Neoplasms ending in "-blastoma" resemble primitive embryonic tissues, which are often pediatric neoplasms. Examples include:
Retinoblastoma NeuroblastomaHepatoblastomaMedulloblastoma
Not all malignant neoplasms have benign counterparts:Hematopoietic and lymphoid cells (as in bone marrow and lymph node) give rise to leukemias and lymphomas. They have no benign counterpart. Gliomas (astrocytomas, oligodengrogliomas, glioblastomamultiforme, etc) arise from glial cells in the CNS. They have no benign counterpart.

Any increase in tissue size is not necessarily neoplasia.
Here is an example of left ventricular cardiac hypertrophy in which there has been an increase in the size of the myocardial fibers in response to an increased pressure load from hypertension. With hypertrophy, the cells increase in size, but the cells do not increase in number. Except for being larger, the cells are normal in appearance.

left ventricular cardiac

Hypertrophy: an increase in cell size. Increase in skeletal muscle fiber size is a physiologic response to exercise, but the cardiac hypertrophy shown above is a pathologic response to abnormally elevated blood pressure.
Hyperplasia: an increase in the number of cells. Postpartum breast lobules undergo hyperplasia for lactation, but endometrial hyperplasia in a postmenopausal woman is abnormal.

Tissue evidence of carcinogenic factors at work
Metaplasia: an initial change from normal cells to a different cell type (such as chronic irritation of cigarette smoke causing ciliated pseudostratifiedepithelium to be replaced by squamous epithelium more able to withstand the insult).

The first step toward neoplasia is cellular transformation. The chronic irritation from cigarette smoke has led to an exchanging of one type of epithelium (the normal respiratory epithelium at the right) for another (the more resilient squamous epithelium at the left). Thus, there is metaplasia of normal respiratory laryngeal epithelium to squamous epithelium in response to chronic irritation of smoking.

The two forms of cellular transformation that are potentially reversible, but may be steps toward a neoplasm, are:
Metaplasia: the exchange of normal epithelium for another type of epithelium. Metaplasia is reversible when the stimulus for it is taken away.

DYSPLASIAvariation in somatotype (as in degree of ectomorphy, endomorphy, or mesomorphy) from one part of a human body to another
: abnormal growth or development (as of organs or cells); broadly: abnormal anatomic structure due to such growth
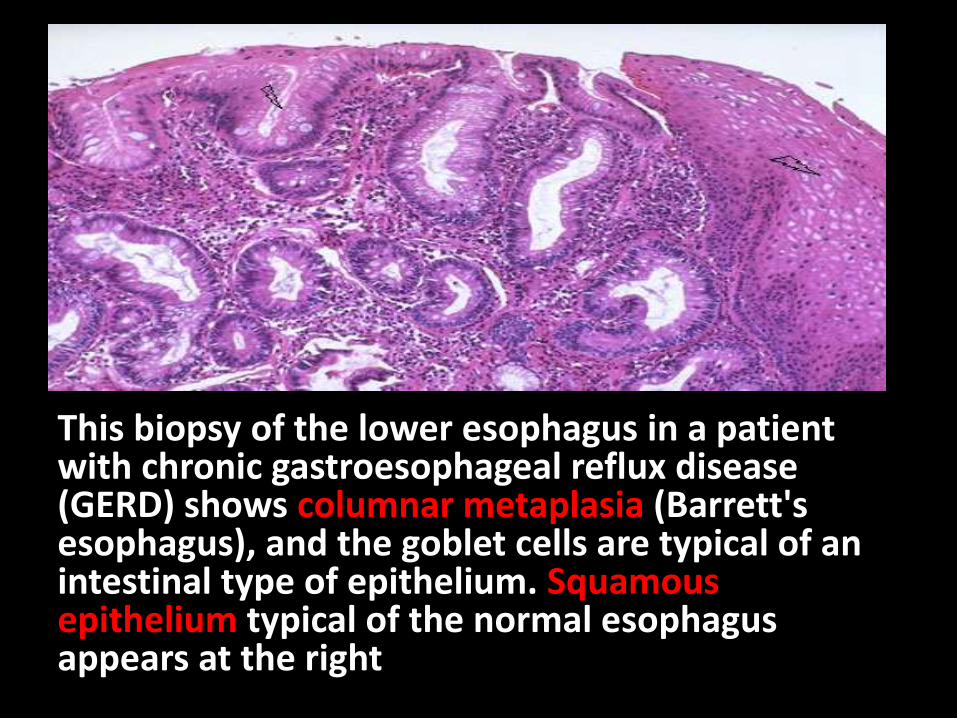
This biopsy of the lower esophagus in a patient with chronic gastroesophageal reflux disease (GERD) shows columnar metaplasia (Barrett's esophagus), and the goblet cells are typical of an intestinal type of epithelium. Squamousepithelium typical of the normal esophagus appears at the right
Characteristics of Benign Neoplasms
A benign neoplasm looks a lot like the tissue with normal cells from which it originated, and has a slow growth rate. Benign neoplasms do not invade surrounding tissues and they do not metastasize. Thus, characteristics include:
Slow growth
Resemblance to tissue of origin (well differentiated)
Circumscription
Lack of invasion
Absence of metastases
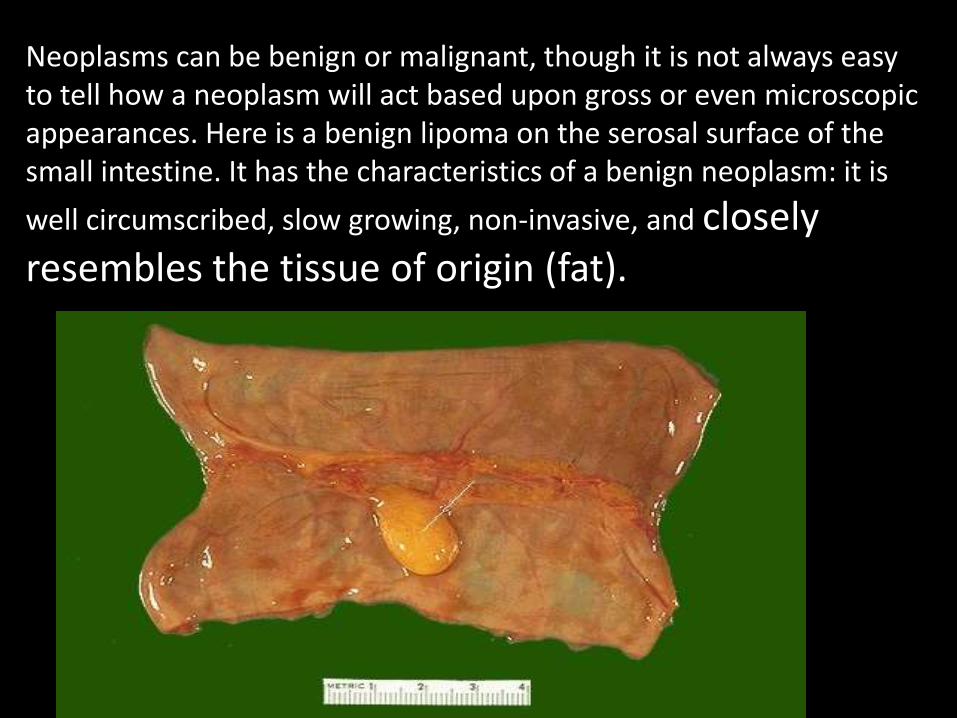
Neoplasms can be benign or malignant, though it is not always easy to tell how a neoplasm will act based upon gross or even microscopic appearances. Here is a benign lipoma on the serosal surface of the small intestine. It has the characteristics of a benign neoplasm: it is
well circumscribed, slow growing, non-invasive, and closely resembles the tissue of origin (fat).
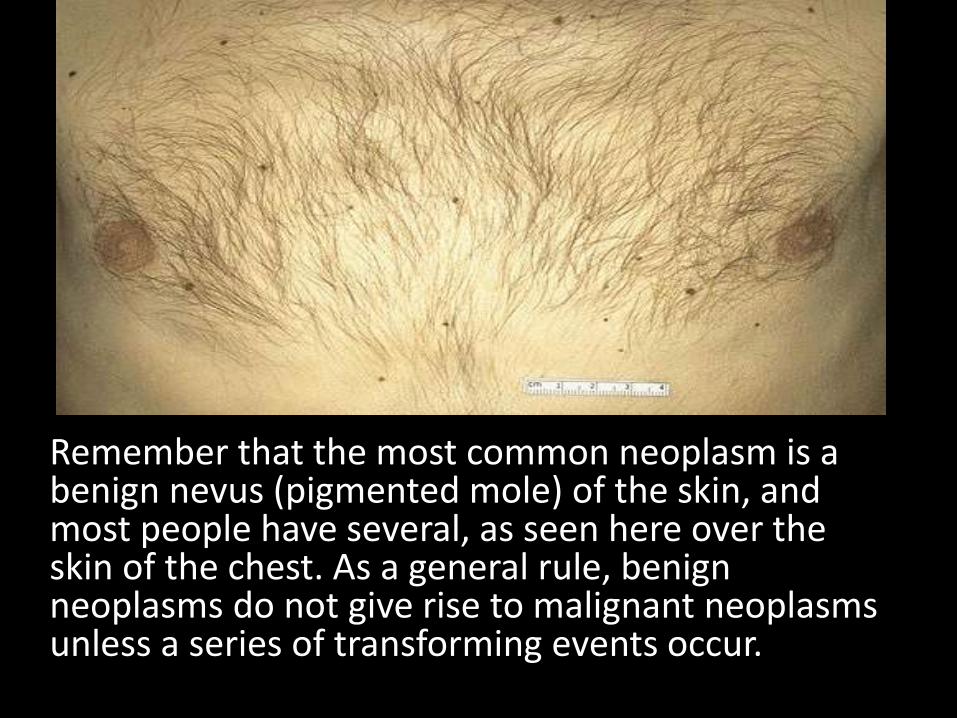
Remember that the most common neoplasm is a benign nevus (pigmented mole) of the skin, and most people have several, as seen here over the skin of the chest. As a general rule, benign neoplasms do not give rise to malignant neoplasmsunless a series of transforming events occur.

Malignant Neoplasmscharacteristics of malignant neoplasms include:1. More rapid increase in size2. Less differentiation (or lack of differentiation, called anaplasia)3. Tendency to invade surrounding tissues4. Ability to metastasize to distant tissuesCytologic features of malignant neoplasms include: Increased nuclear size Variation in nuclear or cell size (pleomorphism). Lack of differentiation (anaplasia). Increased nuclear DNA content with subsequent dark staining
on H and E slides (hyperchromatism). Prominent nucleoli or irregular chomatin distribution within
nuclei. Mitoses (especially irregular or bizarre mitoses).
Causes of Neoplasia1. The origin for many neoplasms is obscure. However, there are
several theories of origin:2. Environmental causes:3. Chemicals: including those that are man-made (such as aniline dyes
and bladder cancer), drugs (cigarette smoke and lung cancer), and natural compounds (aflatoxins and liver cancer) which are carcinogenic.
4. Oncogenic viruses: such as human papillomavirus (HPV) implicated in most squamous cell carcinomas of cervix and anogenitalsquamous papillomas, Epstein-Barr virus (EBV) implicated in African Burkitt's lymphoma, and hepatitis B virus (HBV) implicated in development of hepatocellular carcinomas.
5. Radiation: including ultraviolet light that induces pyrimidine dimersin DNA and promotes skin cancers. Ionizing radiation (such as gamma radiation) induces mutations in DNA and promotes malignancies such as leukemia, thyroid, lung, colon, and breast cancers.

Spread of Malignant Neoplasms
By direct extension (invasion) into surrounding tissues.
1. Through lymph channels to lymph nodes (lymphatic spread)--typical of carcinomas.
2. Via the bloodstream (hematogenousspread)--typical of carcinomas or sarcomas.
3. Within body cavities (seeding)--typical of neoplasms impinging upon body cavities, such as the peritoneal cavity.

This renal cell carcinoma demonstrates distortion and displacement of the normal renal parenchyma by the tumor mass in the lower pole of this kidney. This malignant neoplasm has a variegated appearance on its cut surface, with yellow to white to red to brown areas.

Malignant neoplasms are also characterized by their tendency to invade surrounding tissues.
Here, the tan tissue of a lung cancer is seen to be spreading along the bronchi into the surrounding lung. The dark round areas are lymph nodes also involved by the neoplasm.

Bacteria 24
Classification based upon staining
Gram Positive vsGram Negative
Gram positive structure-- thick layer of
peptidoglycan
Gram negative structure-- inner vs outer membranes-- lipopolysaccharides and
endotoxins
Effect of penicillin


The characteristics are present in gram-positive bacteria:
Cytoplasmic lipid membrane
Thick peptidoglycan layer
Teichoic acids and lipoids are present, forming lipoteichoic acids, which serve as chelating agents, and also for certain types of adherence.

Cytoplasmic membraneThin peptidoglycan layer (which is much thicker in gram-positive bacteria)Outer membrane containing lipopolysaccharide (LPS, which consists of lipid A, core polysaccharide, and O antigen) in its outer leaflet and phospholipids in the inner leafletPorins exist in the outer membrane, which act like pores for particular moleculesThere is a space between the peptidoglycan layer and the secondary cell membrane called the periplasmic spaceThe S-layer is directly attached to the outer membrane rather than the peptidoglycanIf present, flagella have four supporting rings instead of twoNo teichoic acids or lipoteichoic acids are presentLipoproteins are attached to the polysaccharide backbone.Some of them contain Braun's lipoprotein, which serves as a link between the outer membrane and the peptidoglycan chain by a covalent bondMost, with very few exceptions, do not form spores.Release some endotoxin

1. Gram Stain Technique
2. Flood the slide with crystal violet solution for up to one minute. Wash off briefly with tap water (not over 5 seconds). Drain.
3. Flood slide with Gram's Iodine solution, and allow to act (as a mordant) for about one minute. Wash off with tap water. Drain.
4. Remove excess water from slide and blot, so that alcohol used for decolorization is not diluted. Flood slide with 95% alcohol for 10 seconds and wash off with tap water. (Smears that are excessively thick may require longer decolorization. This is the most sensitive and variable step of the procedure, and requires experience to know just how much to decolorize). Drain the slide.
5. Flood slide with safranin solution and allow to counterstain for 30 seconds. Wash off with tap water. Drain and blot dry with bibulous paper. Do not rub.
6. All slides of bacteria must be examined under the oil immersion lens.


Staining and IdentificationMicroscopic view of dental plaque, showing Gram-positive (purple) and negative (red) bacteriaIn a Gram stain test, bacteria are washed with a decolorizing solution after being dyed with crystal violet. On adding a counter stain such as safranin or fuchsine after washing, Gram-negative bacteria are stained red or pink while Gram-positive bacteria retain their crystal violet dye. This is due to the difference in the structure of their bacterial cell wall. Gram-positive bacteria do not have an outer cell membrane found in Gram-negative bacteria. The cell wall of Gram-positive bacteria is high in peptidoglycan which is responsible for retaining the crystal violet dye.

Pathogenesis in humans
90-95% of Gram negative bacteria are pathogenic. On the other hand, many Gram-positive bacteria are non-pathogenic.

H. Pylori which infects up to 50% of the human population. Some strains of this bacterium are
pathogenic to humans as it is strongly associated with peptic ulcers, chronic gastritis, duodenitis,
and stomach cancer

Pseudomonas aeruginosa
Pneumonia
Septic shock
Urinary tract infection
Skin and
soft tissue infections