Embed Size (px)
DESCRIPTION
RADIATION THERAPY FOR EARLY STAGE HODGKIN’S LYMPHOMA CURRENT CONSENSUS
Citation preview

RADIATION THERAPY FOR EARLY STAGE HODGKIN’S LYMPHOMA
CURRENT CONSENSUS
DR. SANDIP SARKAR FELLOW, TMC

Vera Peters (1950): The first physician to present definitive
evidence of curability of Hodgkin’s disease.
Reviewed the records 113 patients treated at the Ontario
Institute of Radiotherapy from 1924 – 1942 and reported 10
year survival rates of 79% for stage I Hodgkin’s disease using
high dose fractionated extended field radiation therapy
Am J Roentgenol 1950; 63: 299-311.

1960’sDevelopment of the MOPP regimenAppreciation of adverse effects of “High Dose Radiation”Investigation of “Combined Modality Therapy”
1970’s & 80’sDevelopment of better imaging facilities (CT scan)Diminished importance of staging laparotomy
GHSG HD 78 – all pts lap stagedGHSG HD 82 – all lap staged, splenectomy only if visible
abnormalities at lapGHSG HD 85 – lap staging only if abnormal USG/ CT scanGHSG HD 90 – laparotomy abandoned
Risks of Infertility / Leukemogenesis – Alkylating agentsDevelopment of ABVD regimenDevelopment of MOPP/ ABVD hybrid regimenReduction in doses of radiotherapy when used with chemo

IMROVEMENT IN SURVIVAL

COTSWALDS MODIFICATION OF ANN ARBOR STAGING

The 90’s
Recognition of the need to optimize therapy (Chemo & RT)
Recognition of prognostic groupsEarly Stage FavourableEarly Stage Unfavourable
Development of risk adapted therapy

RISK FACTORS & TREATMENT GROUPS
Early Stage Risk Factor Treatment Group
EORTC Bulky Mediast. MassAge ≥ 50 yrsElevated ESRB Symptoms≥ 4 nodal regions
Fav: St. I-II without risk factorsUnfav: St. I-II with risk factors
GHSG Bulky Medist. MassElevated ESRB Symptoms≥ 3 nodal regions
Fav: St. I-II without risk factorsIntermed: St. I-IIA with risk factorsUnfav: St. IIB with Elevated ESR
ECOG & NCI-C Histology (MC, LD)Age ≥ 40 yrsElevated ESRB Symptoms≥ 4 nodal regions
Fav: St. I-II without risk factorsUnfav: St. I-II with risk factors

LYMPH NODAL REGIONS

CAN WE AVOID CHEMOTHERAPY FOR EARLY STAGE
FAVOURABLE DISEASE ?

JCO August 2007
RT Alone: 67%CTh + RT: 88%

RT vs. CT + RT FOR EARLY STAGE FAVOURABLE HD
Trial Treatment Outcome OS
EORTC H7STNI (36-40Gy)6 EBVP+IFRT (36-40Gy)
10 yr EFS78%88%
10 yr92%92%
SWOG 9133STNI (36-40Gy)3 x Dox + Vinblast + STNI
3 yr EFS8194
3 yr9698
EORTC/ GELA H8 STNI 36Gy (IF 40Gy)
3 x MOPP/ ABV + IFRT (36Gy)
4 yr FFTF7799
4 yr9599

COMBINED MODALITY
13 randomized clinical trialsMultiagent CT+RT VsRadiation alone
At 10 years RFSR 85% and 67% p=0.00001 10-year OAS 79% and 76%
(p=0.07).
Diehl V.. J Cancer Res Clin Oncol 1990.
Metaanalysis

3 Year EFS CTh Alone: 85%3 Year EFS CTh + RT: 93%, p=0.0024


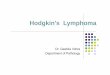
WHAT IS THE OPTIMAL RADIATION VOLUME ?

MANTLE FIELD FOR TREATMENT OFSUPRADIAPHRAGMATIC NODAL REGIONS
RT DOSE: 15-30Gy

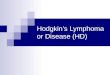
INVERTED “Y” FIELDFOR TREATMENT OF
INFRADIPHRAGMATICNODAL REGIONS

INRT (Involved Nodal RT)
IFRT
Mini Mantle
Mantle
Modified Mantle
Inverted “Y”
Subtotal Nodal Irradiation
Total Nodal Irradiation


CT + RT FOR EARLY STAGE FAV. HD
Trial Treatment Outcome OS
Milan Group4 ABVD + STNI 30Gy (36-40Gy)4 ABVD + IFRT (36-40Gy)
12 yr EFS87%91%
12 yr96%94%
GHSG HD 102 ABVD + IFRT 30Gy 2 ABVD + IFRT 20Gy 2 ABVD + IFRT 30Gy 2 ABVD + IFRT 20Gy
2 yr EFS 96.6% 2 yr 98.5%
EORTC/ GELA H9F 6 EBVP + IFRT 36Gy
6 EBVP + IFRT 20Gy6 EBVP
4 yr FFTF87%84%70%
4 yr98%98%98%

Trial Treatment Outcome OS
EORTC-GELA H8-U 6 MOPP/ABV + IFRT (36-40Gy)
4 MOPP/ABV + IFRT (36-40Gy)4 MOPP/ABV + STNI (36-40Gy)
4 yr TFFS89%92%92%
4 yr90%94% 92%
GHSG HD 82 COPP/ABVD + EFRT 30Gy2 COPP/ABVD + IFRT 30Gy
% yr FFTF86%84%
5 yr 9192
EORTC-GELA H9U 6 EBVP + IFRT 36Gy
6 MOPP/ABV + IFRT 36Gy
10yr EFS68%88%
10 yr79%87%
GHSG HD-114 ABVD + IFRT 30Gy4 ABVD + IFRT 20Gy4BEACOPP + IFRT 30Gy4 BEACOPP + IFRT 20Gy
FFTF 89.9% OS 97.4%
CT + RT FOR EARLY STAGE UNFAV. HD

Reduction in field sizes
8 randomized controlled trialsExtensive portals (e.g. subtotal
mantle, total nodal irradiation etc)
Vs less extensive portals (e.g.
mantle, mini mantle, involved field radiation etc).
Results –• At 10 years, the risk of recurrence
was 31% vs. 43% ( p=0.00001).• Subgroup analysis showed similar
results. • 10-year actuarial OAS- 77% in both
groups (p=0.1)
Metaanalysis BY Specht 1998

WHAT IS THE OPTIMAL RADIATION DOSE ?

RADIATION DOSE
HD-10 trial
1131 patients (1998-2002)
Randomized into 4 arms: a) ABVD x 2 + (30Gy) b) ABVD x 2 + IFRT (20Gy) c) ABVD x 4 + IFRT (30Gy) d) ABVD x 4 + IFRT (30Gy).
• Results: interim analysis conducted in August 2003 of 847 pts (75%)
• Complete remission rates-98.4%
• FFTF after two years – 96.6% with no statistical differences between arms
• Overall survival- 98.5% without any statistical differences in CT and RT comparisons.

JCO July 2007

IJROBP 2003

IJROBP 2001

HODGKIN’S DISEASE CURRENT GUIDELINES
Early Stage Favourable (Low Risk)Multiagent CTh x 2 - 4 cycles + IFRT
Early Stage Unfavourable (Intermediate Risk)Multiagent CTh x 4 cycles + IFRT
Advanced Stage (High Risk)Multiagent CTh x 6-8 cycles ± IFRT

INDICATIONS FOR ADJUVANT RADIATION THERAPY
Bulky Disease at Presentation (Irrespective of Response to CT)
Residual Disease/ Partial Response after Chemotherapy

WITHIN CLINICAL TRIAL
Adults: Microscopic: 19.8Gy/11#/3wks @ 1.8Gy / fr.Gross: 30.6Gy/17#/3wks @ 1.8Gy / fr
Paediatric: Microscopic: 14.4Gy/8#/2wks @ 1.8Gy / fr.Gross: 25.2Gy/14#/3wks @ 1.8Gy / f
RADIATION DOSE GUIDELINES IN TMC
OUTSIDE CLINICAL TRIAL
Adults: Microscopic: 25.2Gy/14#/3wks @ 1.8Gy/fr.Gross: 34.2Gy/19#/4wks @ 1.8Gy/fr. Paediatric: Microscopic: 19.80Gy/11#/3wks @ 1.8Gy/fr.Gross: 30.60Gy/17#/3wks @ 1.8Gy/fr.

Definition of IFRT (ASTRO 2002)
• IFRT encompasses a region, not an individual LN
• Initially involved pre-chemo sites and volume are treated except transverse diameter of mediastinum and paraaortic LN for which reduced post chemo vol is treated
Major involved field region are: • Neck: Ipsilateral cervical and SCV

Cont…
• Mediastinum: Include B/L hilar region , if SCV involved then B/L SCV and cervical region
• Axilla: Include ipsilateral SCV and infraclavicular region
• Inguinal: Include ext iliac and femoral regions.


BASIC RULES
• Examination of patient by Radiation Oncologist.
• Pre and Post chemotherapy CT and FDG-PET scan performed in the treatment position.
• Scans should encompass cervical, axillary, and mediastinal areas.
• Remission status – For each initially involved lymph node should be determined exclusively on CT scans.
• Modern Radiation techniques
- Immobilization. - CT simulation. - Fusion techniques. - 3D-CRT. - Intensity modulated Radiotherapy. - Respiratory Gated Radiotherapy.







Initially involved lymph nodes in PR (Partial Remission)

CERVICAL AND AXILLARY LYMPH NODES
• GTV - The lymph node remnant(s).
• CTV - The initial volume of the lymph node(s) before chemotherapy.
• PTV1 - The CTV including the GTV [i.e. initial tumor mass and lymph node remnant(s)] with a
margin.
• PTV2 - The GTV alone with a margin.



MEDIASTINAL AREA
• GTV - Lymph node remnant(s) or the remaining mass alone.
• CTV - The initial volume of the mediastinal mass.
• PTV1 - The CTV including the GTV (i.e. the initial tumor mass and the lymph node remnant(s) with a margin.
• PTV2 - The GTV alone with a margin.




TREATMENT AND DOSE PRESCRIPTION
PTV1 – 30 GY
PTV2 – 6 GY

HODGKIN’S DISEASEABVD X 6 Cycles ------- Relapsed Salvage MINE X 2 cycles
Progressive Disease + Chest Wall Nodule




TOMOTHERAPY DVH

PTV Dose
Tomotherapy Con. IMRT
V95 % 99.44% 69%
V99% 98.44% 53%
V107% 0.1% 15%

LATE CAUSES OF DEATHIN HODGKIN’S DISEASE
STANFORD
JCRT
IDHD

LATE EFFECTS OF HODGKIN’S DISEASE TREATMENT
Musculoskeletal abnormalities
Pulmonary Sequelae
Cardiovascular Sequelae
Thyroid dysfunction
Second MalignanciesLeukemogenesisNHLSolid Tumors

GROWTH, HEIGHT, MUSCULOSKELETAL EFFECTS
Factors Influencing Growth
• Chronological age at treatment• RT volume• Total RT dose• RT dose per fraction• Site of treatment• Homogeneity of growth plate irradiated• Surgery• Chemotherapy
S Donaldson , 1992

RELATIVE LOSS OF ADULT HEIGHT
• 7.7% (13cm) with RT dose > 33Gy, Entire spine (pre-pubertal age)• No clinically significant loss of height with low dose RT • IFRT associated with clinically insignificant height loss• No disproportion between sitting & standing height
William KY, IJROBP 1993;28:85Stanford

CARDIOVASCULAR LATE EFFECTS
STANFORD(1960-1995)
2498 Pts. 754 Deaths 16% CV disease
JCRT(1969-1996)
794 Pts. 124 Deaths 14%CV disease
EORTC(1963-1986)
1449 Pts. 240 Deaths 7%CV disease
BNLI 1043 Pts. 43 Deaths 14%CV disease
Decreasing CV deaths with improving therapy (CT & RT)
Stage I & II at Stanford (CV deaths after 15yrs of treatment)1962 - 1980: 812 pts. ------ 5.4%1980 – 1996: 628 pts. ------ 0.8%

TYPE/ SITE RELATIVE RISK ABSOLUTE RISK /10,000 pts,Per Yr.
RELATIVE RISKIn 10yr survivor
ABSOLUTE RISK In 10yr survivor Per 10,000 pts,Per Yr.
All cancers 3.5 (3.1 – 3.8) 56.2 4.7 (3.8 – 5.7) 111.7
Leukemia 32.4 (25.5 – 40.6)
16.8 16.2 (6.5 – 33.3)
9.9
NHL 18.6 (13.8 – 24.6)
10.7 32.7 (19.7 – 51.1)
27.8
Solid tumors Female breast Lung
2.4 (2.1 – 2.7)2.5 (1.8 – 3.4)4.2 (3.3 – 5.2)
29.3 11.3 13.5
3.6 (2.8 – 4.6)4.6 (3.0 – 6.6)7.3 (4.7 – 10.6)
74.439.533.8
RISK OF SECOND CANCERS
Van Leeuwen FE, J Clin Oncol 1994;12:312Swerdlow AJ, Br Med J 1992;304:1137Tucker MA, NEJM 1988;318:76

THANK YOU