Embed Size (px)
Citation preview

CLASSICAL HODGKIN’S LYMPHOMA:
TREATMENT STRATEGIESDR ANKIT RAIYANI
Dept. of haematologySSH, Pune.

OVERVIEW OF PRESENTATION• Staging & risk stratification• Role of PET scan• Treatment protocols (First line and second line)• ABVD protocol and its modifications• BEACOPP and its modifications• Newer agents
• Treatment of newly diagnosed HL• Early stage (Stage I/II) favourable risk• Early stage unfavourable risk• Advanced stage disease• Elderly (> 60 yr) newly diagnosed HL
• Treatment of refractory/relapseed HL

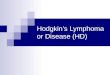
ANN ARBOR CLINICAL STAGING

RISK STRATIFICATION
Hasenclever D, et al. NEJM, 1998

ROLE OF PET SCAN• 97- 100 % HL are FDG avid• Preferable to CT for initial staging • will upstage a minority of patients and aid the interpretation of subsequent PET scan
• PET response should be reported according to Deauville criteria• 1, 2 should be considered ‘negative’ • 4, 5 considered ‘positive’• Deauville score 3 should be interpreted according to the clinical context but in many HL patients indicates
a good prognosis with standard treatment.• Interim PET scan at end of 2 cycles of chemotherapy has greatest prognostic value• Even overrules the initial IPS risk stratification• Can guide in escalation or de-escalation of further treatment
• End-of-treatment PET scan positivity: • Biopsy is advised prior to second-line therapy to confirm residual disease with score 4,5 to exclude false
positive uptake with FDG.


TREATMENT PROTOCOLS

First line protocols
• ABVD (Adriamycin, Bleomycin, Vinblastin, Dacarbazine) ± ISRT• Stanford 5 (Adriamycin, Bleomycin, Vinblastin, Vincristine, Meclorethamine, Etoposide,
Prednisone)• BEACOPP (Bleomycin, Etoposide, Adriamycin, Cyclophosphamide, Vincristine,
Procarbazine, Prednisone)•
Second line protocols ± HDT/ASCR

NEWER AGENTS• Brentuximab vedotin• Antibody-drug conjugate (ADC) directed to the protein CD30• Approved for relapsed HL• Potential uses: B-AVD, post ASCT single drug maintenance, single agent
palliation in elderly frail patients• Adverse effects: peripheral neuropathy, neutropenia• Nivolumab• Humanized IgG4 anti-PD-1 monoclonal antibody used to treat cancer.• Works as a checkpoint inhibitor, blocking a signal that would have
prevented activated T cells from attacking the cancer, thus allowing the immune system to clear the cancer

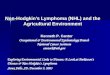
ABVD PROTOCOL

MODIFICATION OF ABVD PROTOCOL

STUDY OUTCOMEABVD AVD ABV AV
Number of
patients566 571 198 167
FFTF @ 5 years 93% 89% 81% 77%
Gr III/IV toxicity 33% 26% 28% 26%
Upfront dose reduction not recommended for treatment of cHL with ABVD


OUTCOME

ADVERSE EVENTS

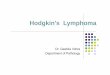
BEACOPP & ESCALATED BEACOPP (NEJM 2003)

DISADVANTAGES OF BEACOPP VS ABVD• Very high rates of severe adverse events• Very high cost of treatment• No benefit in 5 yr OS as compared to ABVD• Reported PFS, OS rates may be difficult to replicate in India• Benefit in FFTF is balanced by acceptable RR of 2nd line
protocol + HDT/ASCR

TREATMENT STRATEGIES

TREATMENT OF NEWLY DIAGNOSED HL• Early stage (Stage I/II) favourable risk• Early stage unfavourable risk• Advanced stage disease

EARLY STAGE (STAGE I/II) FAVOURABLE RISK
ABVD X 2 cycles
Interim PET scan
Deauville 1-4 ISRT: 20 Gy
Deauville 5 Biopsy
Negative: ISRT 20 GyPositive: treat as
refractory disease

EARLY STAGE (I/II) UNFAVOURABLE RISK
ABVD X 4 cycles
Restage with PET scan
Deauville 1-3
ABVD X 2 cycles
AVD X 2 cycles
ISRT: 30 Gy
Deauville 4 ABVD X 2 cycles
Restage with PET scan
Deauville 5 Biopsy
Negative: ABVD X 2
cycles AND ISRT 30 - 45
GyPositive: treat as
refractory disease

ADVANCED STAGE (III/IV) DISEASE
ABVD X 2 cycles
Restage with PET
scan
Deauville 1-3
AVD X 4 cycles
Deauville 4, 5
ABVD X 4 cycles
Restage with PET
scan
Deauville 1-3
Observe or ISRT
Deauville 4ISRT to PET
positive sites
Deauville 5 Biopsy
Negative: Observe or
ISRT (30 - 45 Gy)
Positive: treat as
refractory disease

ELDERLY (> 60 YR) NEWLY DIAGNOSED HL
Non-Frail (No comorbiditie
s)
A(B)VD X 2 cycles Interim PET
Negative (1-3)
AVD X 4 cycles
Positive (4-5)Change
protocol (2nd line/
palliative)VEPEMB X 6 cycles ± ISRT
PVAG X 6 cycles ± ISRT
Frail ( Co morbiditi
es)
ChlVPPVEPEMB
Brentuximab
ISRTPalliation

TREATMENT OF REFRACTORY/RELAPSE (<1 YR) HL
Biopsy proven disease
2nd line therapy PET scan
Deauville 1-4
HDT/ASCR if eligible
Brentuximab maintenanc
e X 1 yr
ISRT/ Observe
Allogeneic SCT
Deauville 5ISRT/
Additional systemic therapy*
Allogeneic SCT
* Brentuximab, Bendamustine

CHEMOTHERAPY REGIMENS IN RELAPSED CLASSICAL HL

THANK YOU!!