Embed Size (px)
DESCRIPTION
Review of periodontal - endodontic combined lesions
Citation preview

The Perio – EndoRelationship
, DDSUTHSC Periodontology
Topical Literature ReviewOctober 7, 2013

Introduction
Primary pulpal infection leading to periradicular periodontitis
Both infections occur simultaneously as independent perio and endo lesions
Primary periodontal infection causing breakdown of alveolar crestal bone, leading all the way to apex
The two infections coalesce to form a combined perio - endo lesion
Carranza’s Clinical Periodontology, 11th ed.Supplement A Figure 51-2
• Persistent infection in the pulp may lead to a secondary infection and breakdown in the periodontium. Likewise, a persistent periodontal infection may lead to inflammatory changes in the pulp tissue. Generally infections of endodontic origin will form retrograde periodontitis, and infections of periodontal origin will form orthograde periodontitis.
• These two types of infection can communicate with each other through physical pathways. The most obvious pathway is the apical foramen, but there may also be communication through lateral and furcal accessory canals, and possibly even dentinal tubules. (Carranza’s Clinical Periodontology 2012)

Classification of perio-endo lesionsPrimary Endodontic (Simon and Glick 1972)• Infection in the pulpal tissues with resulting drainage and/or swelling in the periodontal tissues, or a radiographic
appearance of periodontal disease.• Does not have a secondary periodontal infection, although it may appear that way (example - sinus tract exiting
through sulcus without plaque or calculus)
Primary Endodontic with Secondary Periodontal Involvement• If there is a chronic sinus tract through the sulcus, it may accumulate plaque and calculus resulting in periodontal
breakdown.
Primary Periodontal• Periodontal breakdown progresses along root until it reaches the apex. These teeth are vital.
Primary Periodontic with Secondary Endodontic• Periodontal pathogens may enter the pulp through lateral or accessory canals as well as the apical foramen.
Combined Endodontic and Periodontic• Both infections develop independently and progress until they join together. (Simon et al. 1972)• Usually large attachment loss, and guarded prognosis for tooth. (Sunitha et al. 2008)
Simon JH, Glick DH, Frank AL. The relationship of endodontic-periodontic lesions.
Fig. 1

Communication of Infection
• Apical foramen• The main and obvious route. Exudate leaves the tooth through the apical foramen,
travels through periodontal tissues via sinus tract.• May also have pulpal inflammatory changes secondary to severe periodontitis in cases
where the primary periodontal defect reaches the apical foramina (Carranza’s Clinical Periodontology 2012).
• Accessory canals• 59.6% of maxillary premolars have lateral canals, and of those, 16.2% are in the mid-
root and 4% are in the cervical area (Vertucci et al. 1974).
• 28.4% of permanent molars have patent accessory canals in the furcation area (Gutman 1978).
• Out of 100 teeth extracted due to severe periodontal disease, only 2 had accessory canals within the perio pockets (Kirkham 1975). It is rare that periodontal pathogens would be able to reach the pulp this way.
• Dentinal tubules• Dentinal tubules extend from the pulp to the DEJ with the diameter of 2.5 μm at pulp
and 0.9 μm at the DEJ (Torneck 1998).
• Endodontic pathogens have been shown to populate these tubules adjacent to the pulp (Shovelton 1964).
• Likewise periodontal pathogens have been shown to populate dentinal tubules adjacent to pockets (Guiliana et al. 1997).

Biologic Effects of Pathogens
• It is widely accepted that pulpal disease can cause periodontal pocketing, exacerbate existing periodontal disease and impair healing after periodontal therapy. When the endodontic infection persists, it becomes one of the risk factors for the progression of periodontal disease (Seltzer et al. 1967).
• However the ability of periodontal disease to cause pulpal pathology via dentinal tubules or lateral canals is controversial.
• A number of studies have found pulpal inflammation adjacent to lateral canals exposed by periodontal disease, but a number of other studies have not confirmed any correlation between periodontal disease and changes in the pulp (Carranza’s Clinical Periodontology 2012).

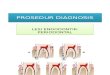
Differential DiagnosisIt is crucial to properly diagnose lesions to be able to provide the appropriate therapy.
This tooth presented with a deep F probing depth and furcation involvement.
The tooth tested non-vital, and root canal therapy was performed. This would be classified as a primary endodontic lesion.
Complete resolution of lesion. No periodontal therapy was indicated.
Carranza’s Clinical Periodontology, 11th ed.Supplement A Figure 51-4

Differential DiagnosisIt is crucial to properly diagnose lesions to be able to provide the appropriate therapy.• If the lesion originates from a pulpal infection, periodontal therapy will not resolve it.• Likewise if the lesion originates from a periodontal infection, endodontic therapy will not completely resolve it.• A diagnosis should be based on multiple findings. The practitioner must perform vitality, percussion, palpation, periodontal probing, and
radiographic examination (Carranza’s Clinical Periodontology 2012)
Subjective Symptoms (Carranza’s Clinical Periodontology 2012)
• Pulpitis (reversible or irreversible) is USUALLY painful, while periodontal infection is USUALLY not.• Pulpitis generally starts with hot/cold sensitivity and progresses to a more severe spontaneous throbbing and/or pain when
chewing. Often the pain will subside with pulpal necrosis, then return as an abscess forms and the tooth is elevated in the socket.
• Generally, an acute periradicular abscess causes extreme pain to pressure, bite, percussion, and, at times, to palpation if the infection has penetrated the cortical bony plate. However abscesses that are able to drain through a sinus tract will often not be painful.
• The degree of pain varies widely with endodontic infections, but in general they are more painful than periodontal infections.• An acute periodontal abscess is thought to be less painful because there is no associated elevation of the periosteum. The
swelling with a periodontal abscess is usually confined to the cervical area.
Carranza’s Clinical Periodontology, 11th ed.Supplement A Table 51-3

Coronal Integrity• Teeth with primary periodontal involvement may have fully or mostly intact crowns.• Primary endodontically involved teeth usually have extensive coronal breakdown, or deep, or large restorations.• A true combined lesion would have primary periodontal infection, but also extensive coronal breakdown and primary endodontic
infection.
Radiographic Apperance• A lesion that appears wider apically than coronally indicates a primary endodontic infection.• Primary periodontal lesions appear wider cervically than apically.
Vitality• Thermal testing is the most reliable way to assess vitality• Teeth that are periodontally involved only will test vital• Endodontally involved teeth will either test non-vital, or will have a delayed response or lingering pain in the case of irreversible
pulpitis.• There are always exceptions such as calcified canals, teeth with only some non-vital roots, or extensively restored teeth.
(Carranza’s Clinical Periodontology 2012)
Differential Diagnosis
Primary periodontal involvement. Lesion is wider in the cervical portion.(Simon & Glick Fig 7B)
Primary endodontic involvement. Lesion is wider in the apical portion.(Carranza’s Clinical Periodontology, 11th ed.Supplement A Fig 51-3)

Treatment of Perio – Endo Lesions
If endodontic involvement is diagnosed, RCT should be performed first.
• Primary endodontic lesions – RCT will resolve the endodontic infection, and its effects on periodontal tissues (for example sinus tracts).
• Primary endodontic with secondary perio – RCT will resolve the endodontic and possibly some, but not all, of the periodontal infection. Periodontal therapy will be needed.
• Primary Periodontal with secondary endo – completing RCT will resolve the endo – it will probably not resolve any of the periodontal disease since this was there prior to the endodontic disease.
• single rooted teeth have poor prognosis. Multi rooted teeth with only 1 root is involved have better prognosis since the root can be amputated.
• True combined lesions – same treatment as with Periodontal with secondary endo. (Sunitha et al. 2008)
o Allow 3 months for healing of tissue and resolution of infectionfollowing RCT before beginning periodontal treatment.
If endodontic involvement is not diagnosed, proceed with periodontal treatment.
Case 1 – Independant endo and perio lesions. Completion of RCT resolved endo lesion, but perio bone loss remains on M & D.Case 2 – Combined endo – perio lesion. Completion of RCT resolved endo lesion, but perio bone loss remains in furcation and on M.
Carranza’s Clinical Periodontology, 11th ed.Supplement A Figure 51-7

Treatment of Perio – Endo Lesions
Guided tissue regeneration following root canal therapy• Guided tissue regeneration 77.5% five year success rate following root canal therapy in perio-endo
combined lesions. (Oh et al. 2009)
• Allow 3 months for healing of tissue following RCT before beginning periodontal treatment.
Oh et al. Figs 1 and 2
Perio-endo combined lesion tooth #3. GTR procedure with e-PTFE membrane only 1 month following RCT. Membrane exposure seen at 2 week post op. Membrane removed at 7 weeks.
Incomplete bone fill of defect possibly due to membrane exposure, or insufficient healing time after RCT. 2nd GTR done 10 months later with resorbable collagen membrane.

References
• Newman, M. G., Takei, H. H., & Carranza, F. A. (2012). Carranza's clinical periodontology. St. Louis, Mo: Elsevier/Saunders.• Simon JH, Glick DH, Frank AL. The relationship of endodontic-periodontic lesions. Journal of periodontology 1972;43:202-208.• Singh P. Endo-perio dilemma: a brief review. Dental research journal 2011;8:39-47.• Sunitha VR, Emmadi P, Namasivayam A, Thyegarajan R, Rajaraman V. The periodontal - endodontic continuum: A review.
Journal of conservative dentistry : JCD 2008;11:54-62.• Oh SL, Fouad AF, Park SH. Treatment strategy for guided tissue regeneration in combined endodontic-periodontal lesions:
case report and review. Journal of endodontics 2009;35:1331-1336.