Embed Size (px)
Citation preview

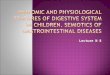
AGE RELATED CHANGES IN THE EYE?
“ARE WE AWARE ABOUT IT”
Hira Nath Dahal
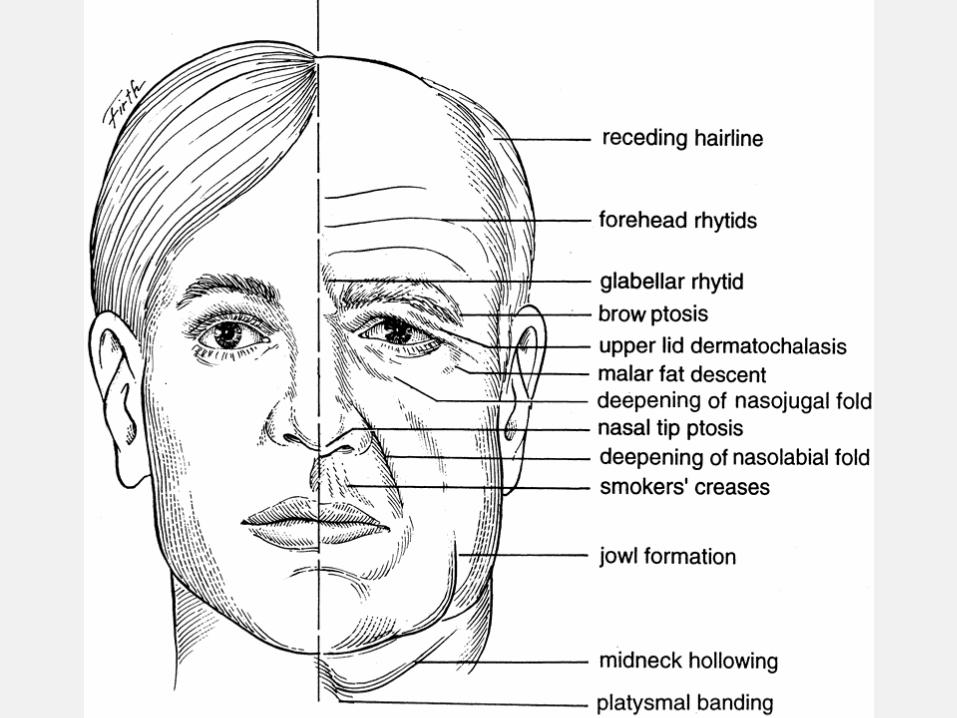
• Decreased visual field• corneal hypoxia
dermatochalasisptosis
Periorbit and eyelid
skin & soft tissue atrophy
glabellar rhytids
poliosis
orbital septal dehiscene ⇒ herniation of orbital fat
lacrimal gland dysfunction, ↓ed tear production,
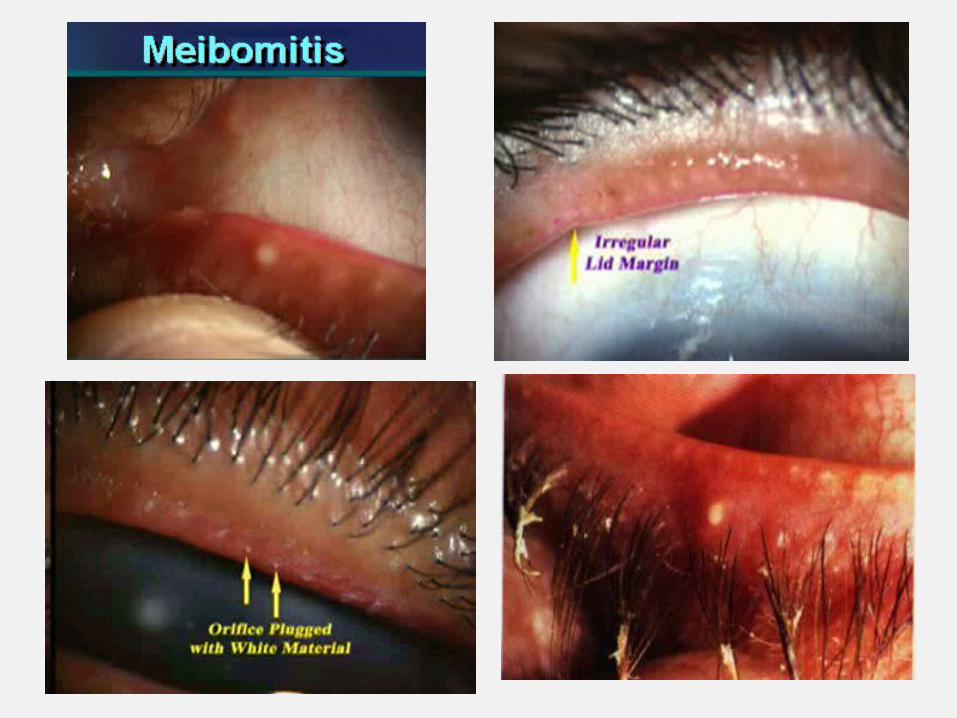
meibomian gland disease & goblet cell dysfunction ⇒
dry eye
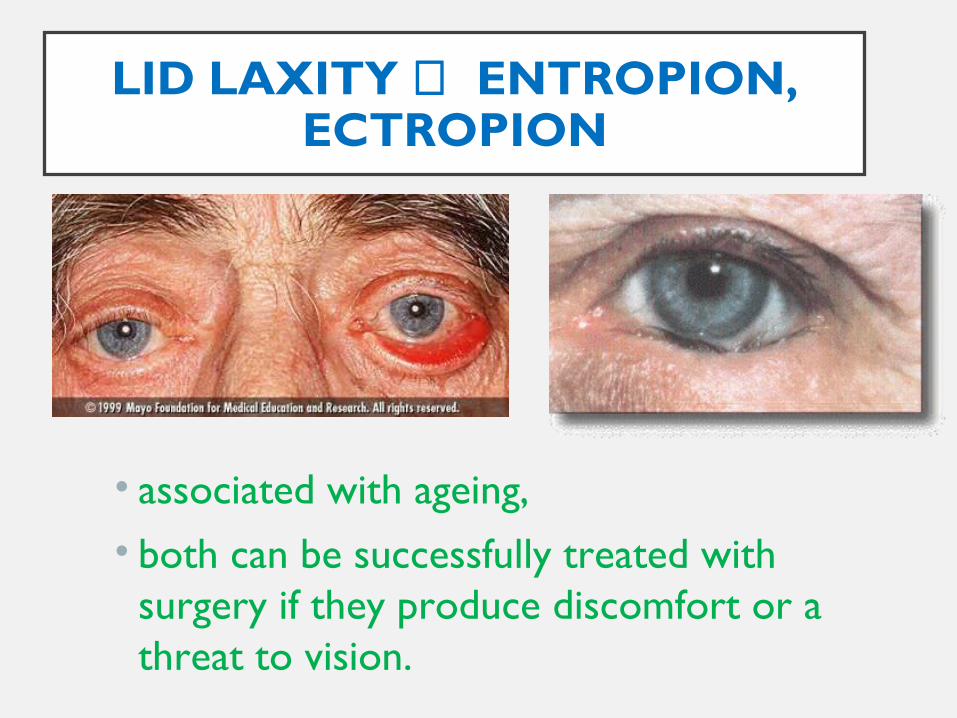
LID LAXITY ⇒ ENTROPION, ECTROPION
• associated with ageing, • both can be successfully treated with
surgery if they produce discomfort or a threat to vision.
CONJUNCTIVA:
• atrophy & degeneration
• ↓ in no. & height of epithelial cells
• shortening of inferior fornix
• the number of mucous cells decreases leading to
dry eye.
CORNEA:
• ↓ed corneal sensitivity
• ↑ against-the-rule astigmatism
• no. of the people having with-the-rule astigmatism ↓es with
age
• Arcus senilis
• corneal endothelial cell population decreases along with
polymegathism and pleomorphism
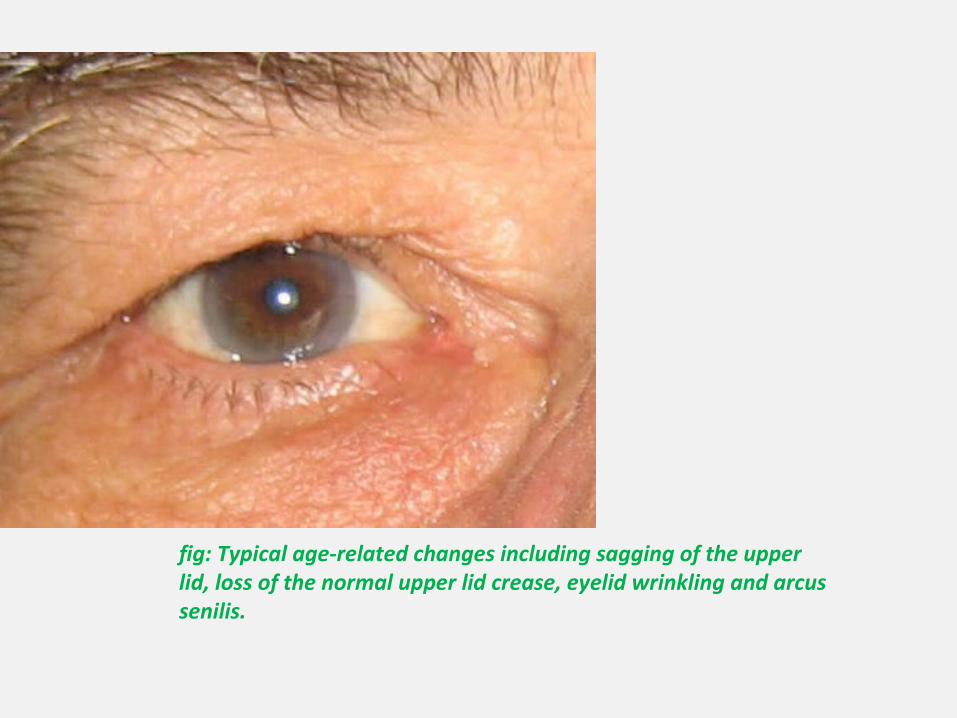
fig: Typical age-related changes including sagging of the upper lid, loss of the normal upper lid crease, eyelid wrinkling and arcus senilis.
ANTERIOR CHAMBER:
• depth ↓es with age, causing
• the increment in the refractive power of the eye
(↑ myopia)
• More interference with aqueous outflow
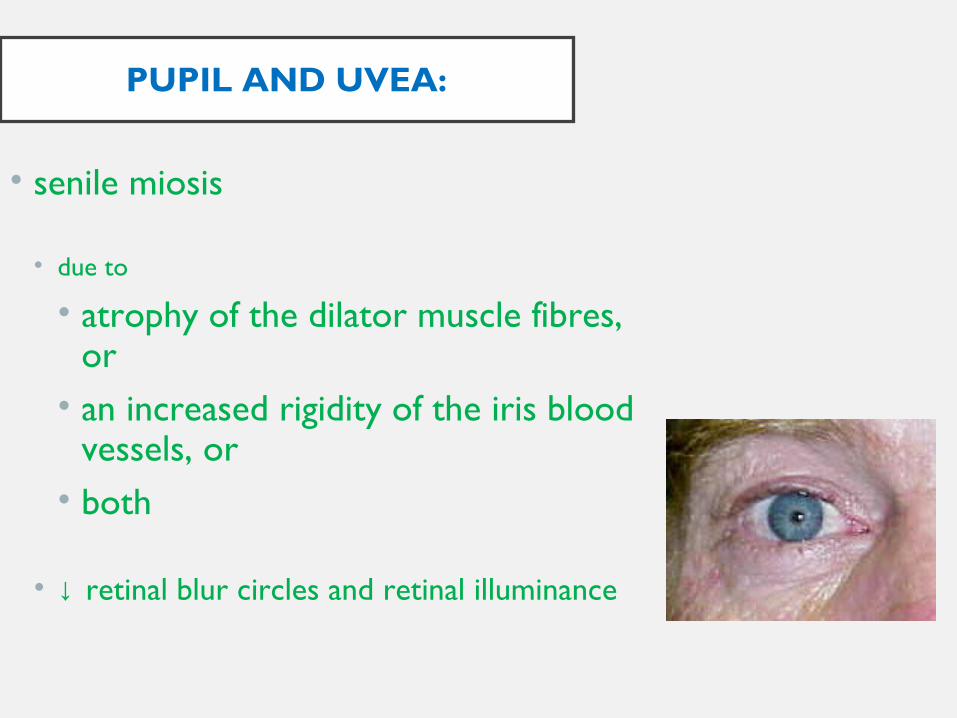
PUPIL AND UVEA:
• senile miosis
• due to
• atrophy of the dilator muscle fibres, or• an increased rigidity of the iris blood
vessels, or• both
• ↓ retinal blur circles and retinal illuminance
less difference in the diameter of the pupil in the light- and
dark-adapted state
less reactive to light
slight ↑ in the latency of pupillary responses
hypertrophy of ciliary muscle

LENS:
• Morphological Changes:
• ↑ in both the mass & dimension of the lens
• axial thickness of the lens ↑es by about 28% by age 70
over that which existed at age 15 to 20 yrs

• the nuclear thickness remains constant while the cortical
thicknesses increase
• the anterior cortex increases by 0.6mm & the posterior,
by 0.4mm
• flattening of the anterior lens surface & conical bulging of
the posterior lens surface
LENS:…
Morphological Changes:
epithelial cells- becomes flatter & density ↓es
lens fibers- total loss or partial degradation of a no. of plasma
membrane & cytoskeletal proteins
cholesterol:phospholipid ratio ↑es
lens capsule- thickens throughout life (collagen type IV vs. I, III,
IV)
LENS:…
Physiological Changes:
Changes to the cellular junctions and alteration on cation
permeability
membrane potential- from –50mV (at age of 20 yrs) to –20mV (at
the age of 80 yrs)
• sodium concentration - ↑es
• Na+:K+ permeability ratio ↑es by six fold
• free calcium level ↑es Ca ATPase inhibited
LENS:…
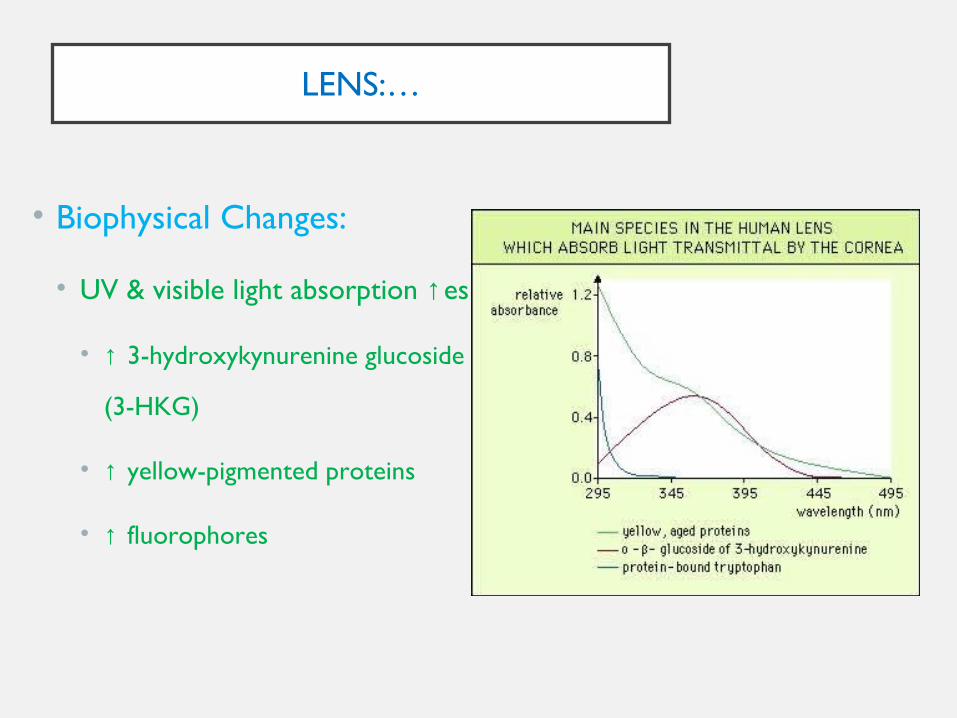
• Biophysical Changes:
• UV & visible light absorption ↑es
• ↑ 3-hydroxykynurenine glucoside
(3-HKG)
• ↑ yellow-pigmented proteins
• ↑ fluorophores

• thus transmission of visible light & lens transparency ↓es
• the amount of light reaching the retina in a normal 60-
year-old is only about 1/3rd that reaching the retina of a 20-
year old
• amplitude of accommodation ↓es
LENS:…
• Biochemical Changes:
• overall metabolic activity of the lens ↓es
• ↓ glycolytic activity
• ↓ level / activity of antioxidants
• Changes in Crystallins:
• accumulation of high molecular weight aggregates
• some act as scatter points for light
• ↑ed insolubility
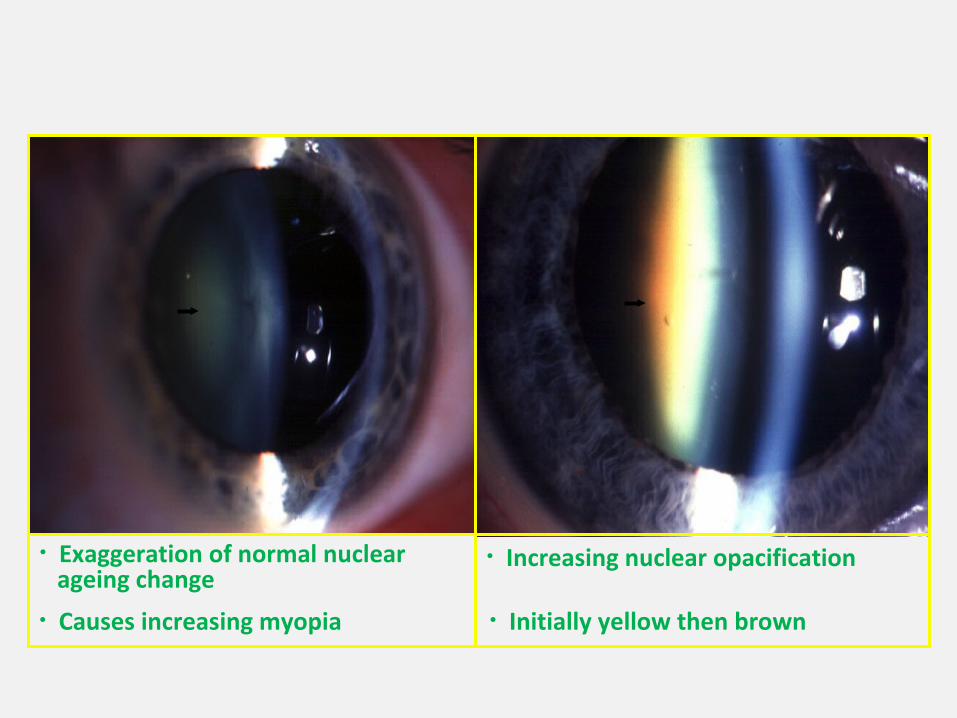
• Exaggeration of normal nuclear ageing change• Causes increasing myopia
• Increasing nuclear opacification
• Initially yellow then brown
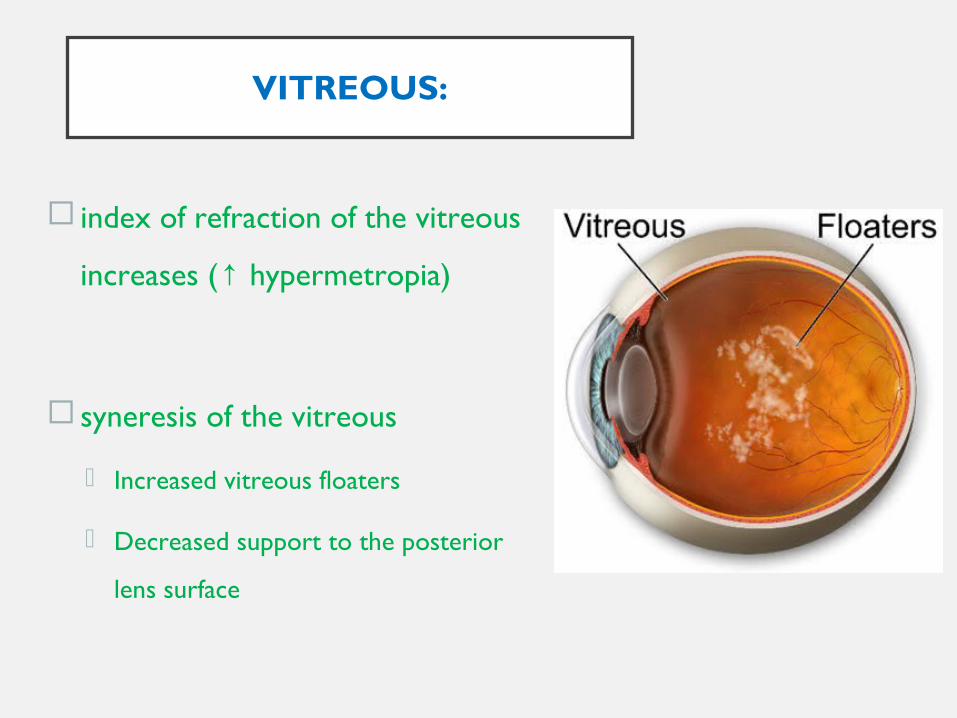
VITREOUS:
index of refraction of the vitreous
increases ( hypermetropia)↑
syneresis of the vitreous
Increased vitreous floaters
Decreased support to the posterior
lens surface

RETINA AND NEURAL CONNECTIONS:
in the absence of pathology, only little decline in static
visual acuity with age that can not be accounted for by
miosis and increased density of the lens
pathologies that are the major cause of decline in static
visual acuity are cataract, macular degeneration and
glaucoma

• mesopia occurs at higher levels of ambient illuminace in older people
• The arteries and veins of the retina become narrower with age, reducing the flow of blood.
The ageing retina is duller and exhibits a less
responsive light reflex.
The optic disk may be paler also.
This creates a need for more light in order to read or
accomplish other tasks.

SENILE MACULAR DEGERATION
• Warning signs may include:• gradual, spotty loss of detail vision
(dry macular degeneration);
• sudden and severe loss of central vision (wet macular degeneration);
• a need for more light.
RETINA AND NEURAL CONNECTIONS:…
• ↓ contrast sensitivity due to increased lens
fluorescence and light scatter
• with shift of peak sensitivity to lower frequencies
• ↓ in the ability to discriminate colours
• ↓ visual field size and sensitivity
• absolute level of dark adaptation reached by the elderly is
less than that reached by younger individuals
REFRACTIVE STATUS:
• static power of the eye: hypermetropic shift
• cornea: ↑ against-the-rule astigmatism
• anterior chamber: ↑ myopia
• lens: hypermetropia or myopia
• vitreous: ↑ hypermetropia
OCULAR MOTOR SYSTEM:
under scotopic conditions, aging people have difficulty
with fixation
↑ exotropia with age
the range of voluntary eye movements becomes limited
supraduction ↓es with age
↑ tonic vergence with distance heterophoria (esophoria)

↓ positive fusional vergence but same negative
fusional vergence
↓ accommodation with ↑ AC/A ratio & ↓ CA/C
↓ stereopsis
OTHER CHANGES WITH AGING:
• ↓ aqueous secretion
• ↓ resistance to distraction
• ↓ ability to selectively attend to one source of
information in the presence of competing
messages
↓ ability to separate visual events that happen serially declines
with age
↓ dynamic visual acuity (VA for moving targets)
related to ↓ in the rate of smooth following eye movements
↑ variability in visual performance between individuals