Embed Size (px)
Citation preview
Brightwater Oats St An Innovative approach to Brain Injury Rehabilitation
Overview of Presentation
1. Oats St in the WA Brain Injury Rehab pathway
2. The Oats St difference
3. Outcome Measures – using the MPAI-4
4. The Story of Cheryl – a case history
5. The Story of Fred – a case history
6. So What – why is Oats St important
7. What are the key features of the Oats St model
8. A graduated progression through rehab
9. The importance of the built environment
10. Key messages from this presentation
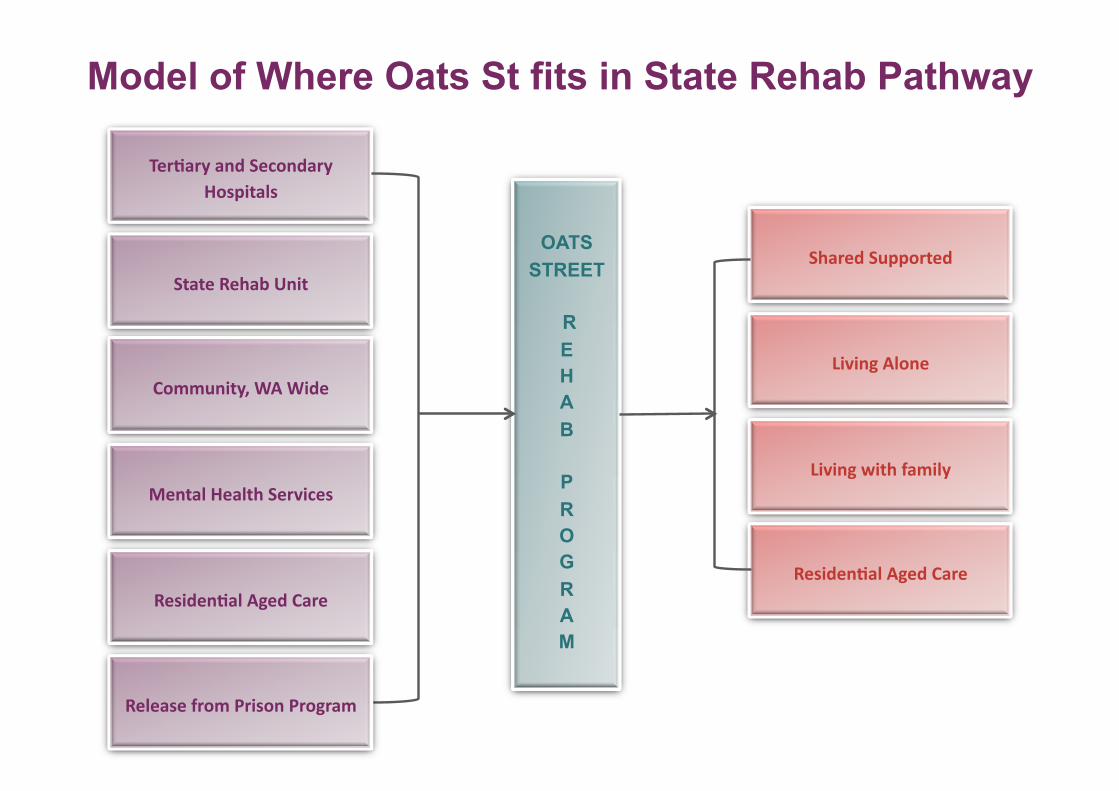
Model of Where Oats St fits in State Rehab Pathway
Mental Health Services
Ter1ary and Secondary Hospitals
State Rehab Unit
Community, WA Wide
OATS
STREET
R
E
H
A
B
P
R
O
G
R
A
M
Shared Supported
Living Alone
Living with family
Residen1al Aged Care
Release from Prison Program
Residen1al Aged Care
Why is Oats St Different ? Translating Neuroplasticity into Functional Rehabilitation
Key Features To Make Gains Utilising Brain Plasticity:
• Context – it must be important and real to the person
• Consistency – doing things in the same way
• Repetition – doing the same thing regularly
• Time – giving time to embed skills
• Persistence – don’t give up
• Approach – positive, all working together and celebrating success
Why Is Oats St Different? – Translating Neuroplasticity Into Functional Rehabilitation
How Is This Reflected In the Oats St Program?
• It is a 24/7 program operating within a domestic environment that is part of the local community
• Each person’s program is based around own goals – things that are important to them
• These goals are underpinned by life skills – things that enable independence
• Adding purpose to skills encouraging each person to practice them as part of everyday life
• All staff work in the same way with each person reinforcing their learning
• Feedback happens regularly through reviews, outcome measures, graduation – people knowing they are hitting the target!
• We celebrate achievement!
Measuring Change – Using the MPAI-4
• The Mayo-Portland Adaptability Inventory (MPAI-4) : − evaluates the progress of people with brain injury who are no longer in
acute hospital care − evaluates the effectiveness of post hospital rehabilitation programs
• MPAI-4 items represent the range of physical, cognitive, emotional,
behavioural, and social problems that people may encounter after ABI
• MPAI-4 items provide an assessment of major obstacles to community
integration which may result directly from ABI
• MPAI-4 has three subscales: − Ability Index - productive activities − Adjustment Index - emotional and interpersonal factors − Participation Index - involvement in social & community activity
Measuring Change – Using the MPAI-4
• We can demonstrate to each individual the gains they are making and help them plan future goals
• We can measure how well the program is doing and understand its overall impact in providing rehabilitation to people with brain injury
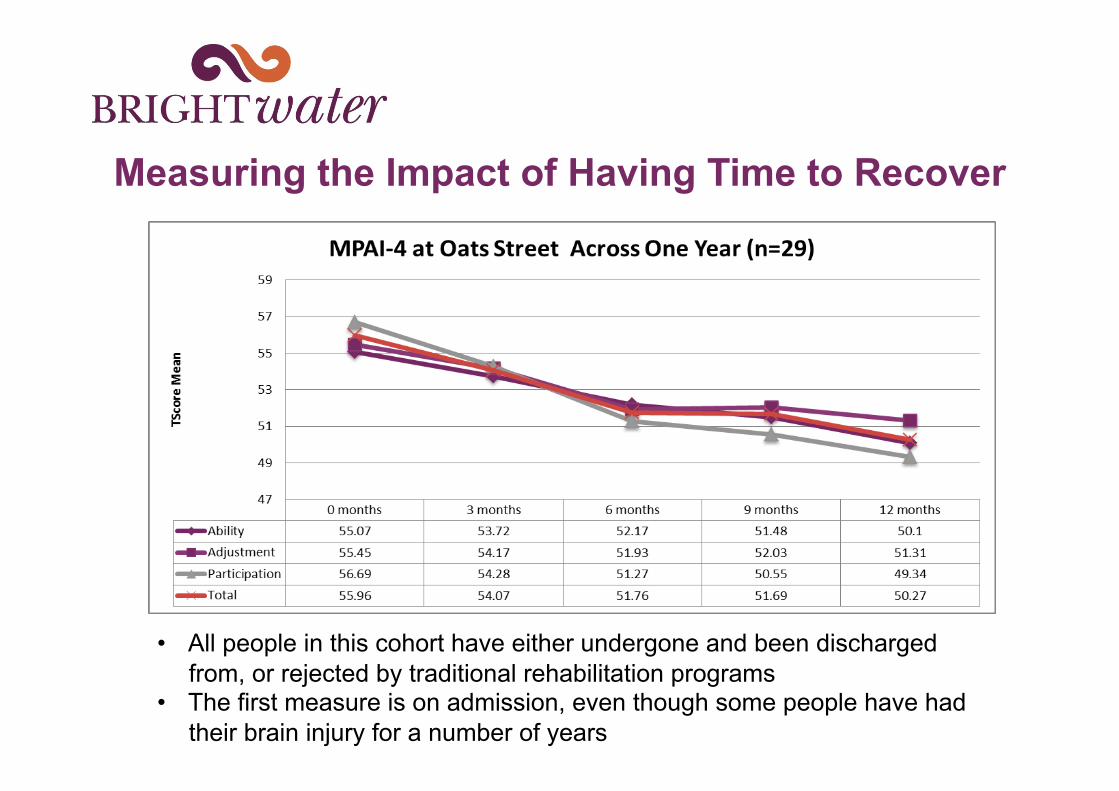
Measuring the Impact of Having Time to Recover
• All people in this cohort have either undergone and been discharged from, or rejected by traditional rehabilitation programs
• The first measure is on admission, even though some people have had their brain injury for a number of years
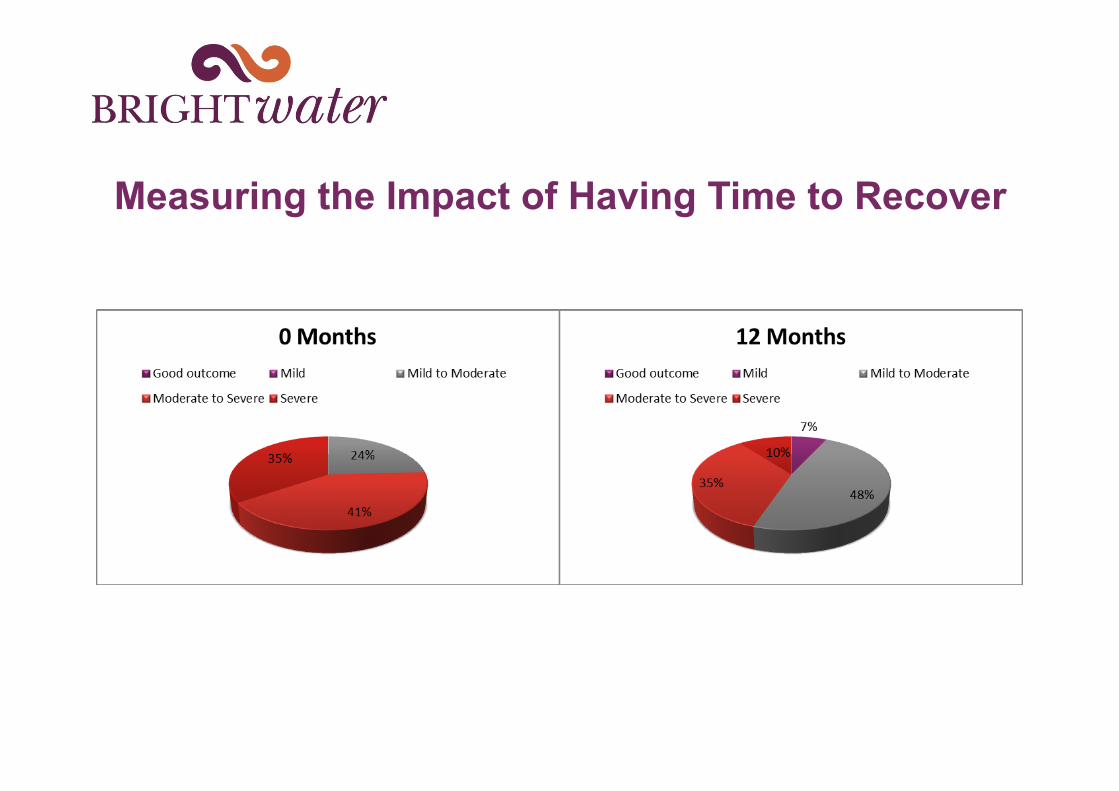
Measuring the Impact of Having Time to Recover
Let’s Meet Cheryl
• 55 year old recently widowed lady with two adult children • Had lived prior to her stroke at home with her husband in an
inner Perth suburb • Was working as a front of house staff member at His Majesty’s
Theatre • Interests included playing keyboard, violin, viola and cello • Cheryl also had a past history of untreated depression and
alcohol abuse
Let’s Meet Cheryl
• August 2010 experienced a Right Middle Cerebral Artery Stroke following a fall
• Cheryl spent over 3 months in a Tertiary Hospital • Assessed as having no rehabilitation potential by State
Rehabilitation Unit • Expected that Cheryl would either not survive, or make little
recovery • Transferred to a Brightwater aged care facility December 2010 • No post hospital neurological follow up but continued to make small
consistent gains • March 2014 Cheryl admitted to Brightwater Oats St into an early
stage house (House 3) • Her husband died from pancreatic cancer May 2014
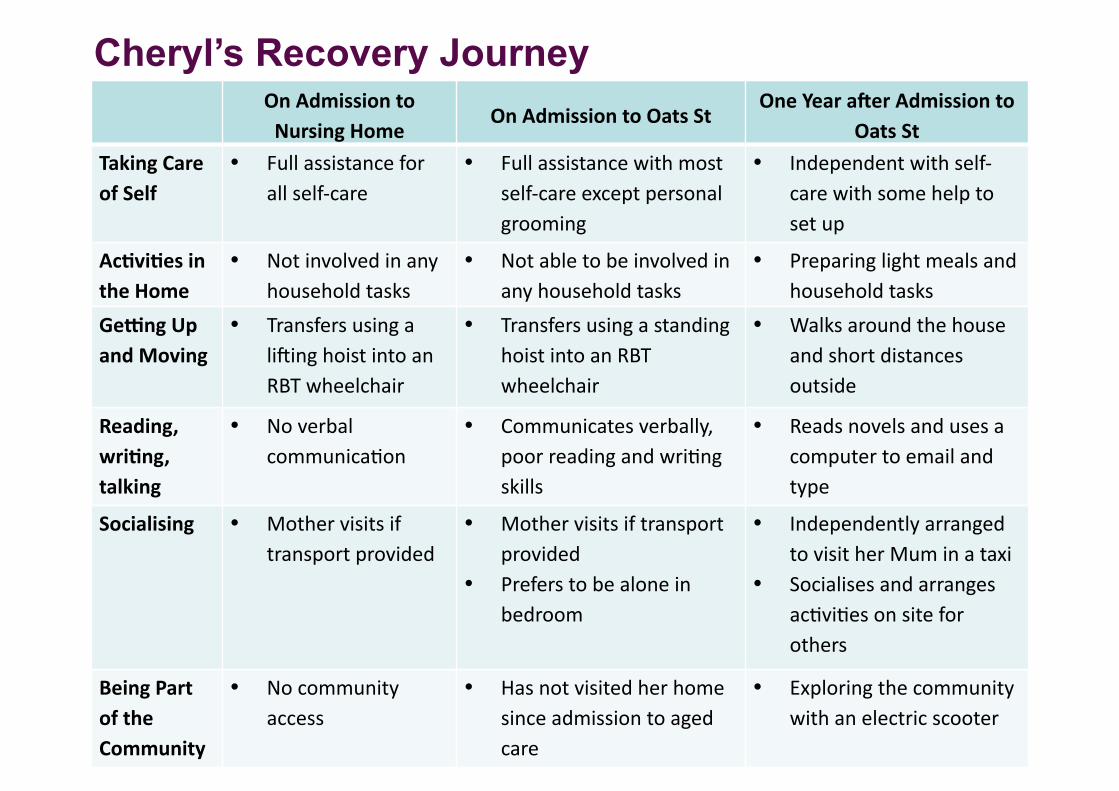
Cheryl’s Recovery Journey On Admission to
Nursing Home On Admission to Oats St
One Year aGer Admission to Oats St
Taking Care of Self
• Full assistance for all self-‐care
• Full assistance with most self-‐care except personal grooming
• Independent with self-‐care with some help to set up
Ac1vi1es in the Home
• Not involved in any household tasks
• Not able to be involved in any household tasks
• Preparing light meals and household tasks
GeJng Up and Moving
• Transfers using a li?ing hoist into an RBT wheelchair
• Transfers using a standing hoist into an RBT wheelchair
• Walks around the house and short distances outside
Reading, wri1ng, talking
• No verbal communicaCon
• Communicates verbally, poor reading and wriCng skills
• Reads novels and uses a computer to email and type
Socialising • Mother visits if transport provided
• Mother visits if transport provided
• Prefers to be alone in bedroom
• Independently arranged to visit her Mum in a taxi
• Socialises and arranges acCviCes on site for others
Being Part of the Community
• No community access
• Has not visited her home since admission to aged care
• Exploring the community with an electric scooter
Cheryl
Oats St staff observations:
• Cheryl’s mood was low. She was not keen to participate in therapy. She was fearful and resigned to her wheelchair. Her husband was unwell, diagnosed with Ca late 2013.
• She became more interested in therapy after her husband died in May 2014 as she felt that she needed to be more independent. Cheryl started engaging in all aspects of therapy.
• By August 2014, whilst she was working with staff on her second goal and rehabilitation plan, it was obvious that she had reached a turning point.
• Cheryl progressed to a mid stage house (House 5). This further encouraged her to be more independent.
Cheryl is now aiming to move into an apartment in the community with regular support for complex tasks.
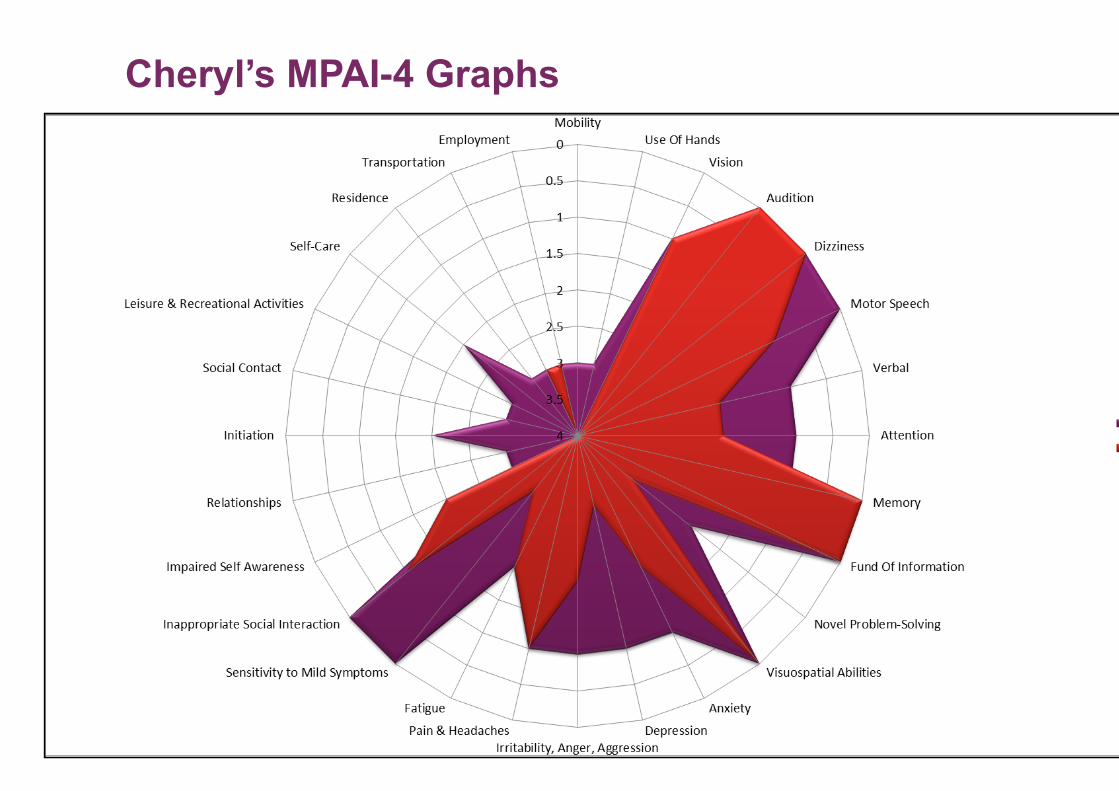
Cheryl’s MPAI-4 Graphs
Introduction to Fred
• 50 year old man –Traumatic Brain Injury sustained in a motorbike accident in September 2011
• Discharged home to his partner and two young daughters after six weeks in hospital
• Admitted as a “social” admission to a secondary hospital when relationship with partner broke down
• History of poor relationship with parents • He was admitted to Brightwater Oats St in July 2012 • Independent with self care but required full support for all other
tasks requiring planning and organising • Fred demonstrated severely impaired memory, agitation,
aggression and boredom
Fred Four Years Later
• Lives independently • Has worked part-time at a café as a dishwasher for over a year,
earning a small income • Improved self esteem and socialisation • Able to cook easy meals, do basic housework and other simple tasks • Manages his weekly budget - assistance from the Public Trustee for
complex money management • Travels independently on public transport, including going to work • Significantly less agitated with no episodes of aggression for some
time • Has made new friends in the community where he has regular contact • Now has a good relationship with his parents, who visit him regularly
Some Quotes About Life For Fred Now
“He is so proud of himself and his job at Dome. He even wears his apron on the
train when he goes to work”
“Fred is extremely calm and very (very!) happy – so house proud and very insightful into the benefits from working and living with
support in the areas that he needs most.”
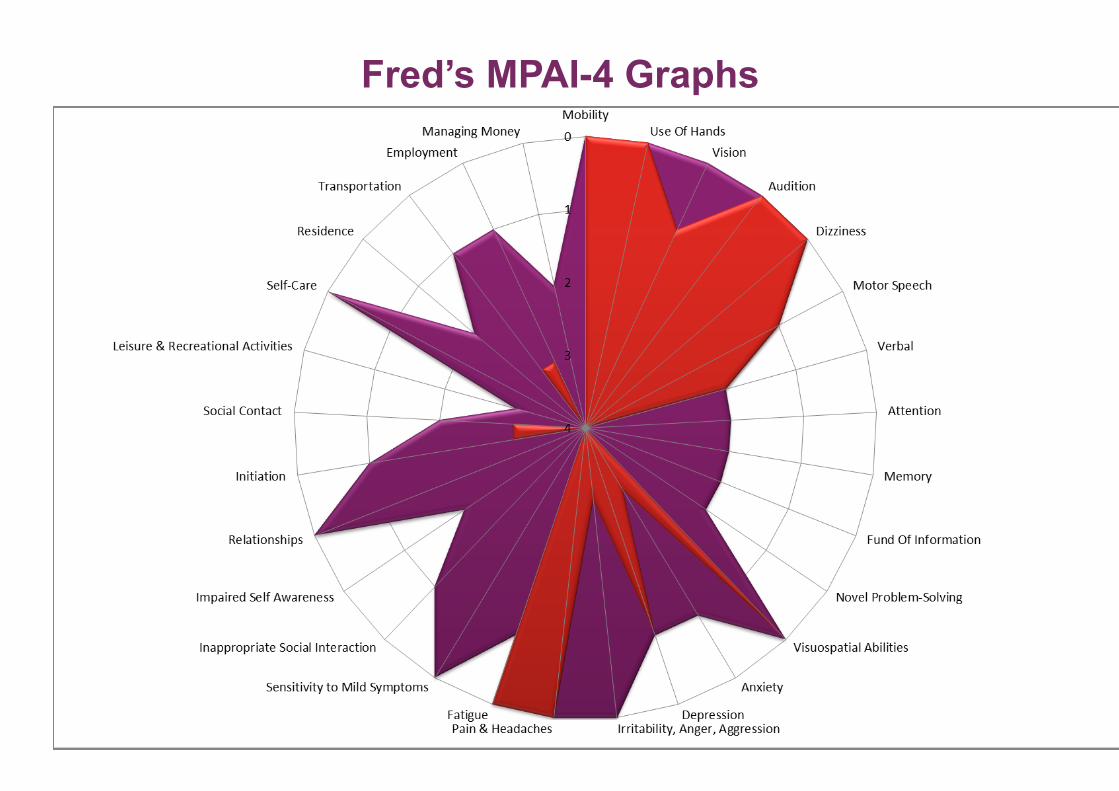
Fred’s MPAI-4 Graphs
So what? Why is Oats St important?
• Importance in the health system − Admits people the hospitals are unable to discharge − Saves the health department money − Reduces readmission to hospital
• Impact on community − Saves long term cost of care provision − Enables increased productivity of individuals and families − Impacts on homelessness and incarceration
• Impact on the individual − Rehabilitation opportunity for people who have been rejected by sub-acute
service − Control over life direction − Increased lifestyle choices − Improved quality of life
Oats St Key Components
• Person-centred, goal directed planning • Recognition of the importance of family and significant
others • Time to explore potential to recover • Graduated stages • Purpose built, domestic style environment • Re-gained skills practiced in surrounding community setting • Case coordination • Interdisciplinary team • Outcome measurements • Celebration
Importance of the Graduated Stages
• Support that matches actual need • Individualised goals overlaid with life skills • Provides incentive, and cause for celebration • Gives the individual the ability to self pace and self direct • Offers clear steps to move forward
We will further research the specific impact of this staging model
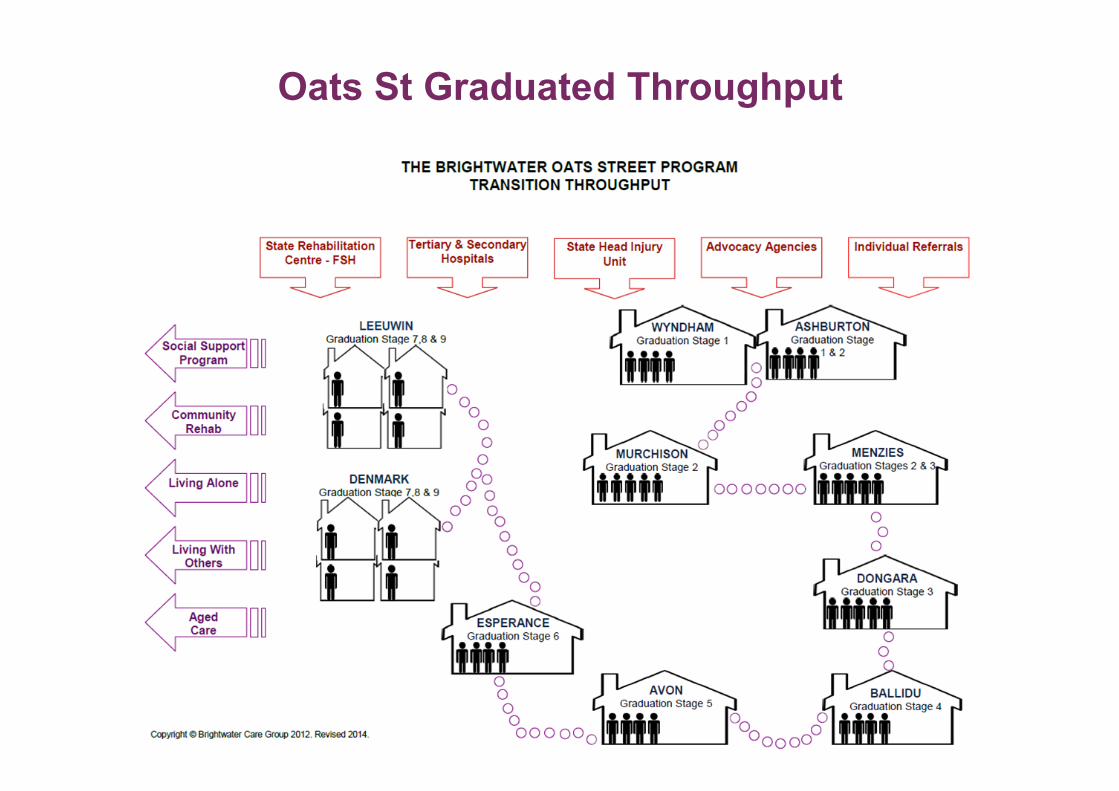
Oats St Graduated Throughput
Features of the Oats St Built Environment
• Internal design changes from house to house - providing opportunity for people to interact with the domestic environment to the level they are able.
• Domestic features such as kitchen and laundry are part of the house not a separate therapy area
• People are cued into engaging in their environment, through line of sight of most of the house and the outdoor areas.
• There is “carry over” from formal therapy sessions into normal day to day living.
• The houses offer each person opportunity to personalise their immediate spaces -reconnecting with who they are and what is important to them.

Oats St Built Environment
• There is a connection between the site and the community providing opportunity for key learnings about integration and participation by being part of the community.
• Oats St is a community within the community - a “village” - within the site itself. This offers a safe environment where people come together, support each other through good times and bad, share experiences and create connections with each other.
• The houses are arranged so that people can physically see where they are going on their journey through observing the progression of others through the site and reinforcement of their own progress.

Pictures of Oats St
Key Messages
Most people who attend Oats St have either undergone traditional hospital based
rehabilitation or have been rejected due to lack of potential.
People who have been deemed to have little further potential for change continue to
make remarkable recovery over time
The service operates within a domestic environment that offers opportunity for people
to engage and practice skills 24/7
There is a strong connection with the community
Physically moving through the site enables people to experience success and
rewards improvement. It also ensures that care support is targeted at a level
commensurate with individual need
There is significant longer term cost saving to the government and community with
proven reduced cost of care and increased economic participation.
References and Acknowledgements
Clients and families of Oats St Oats St Staff
Karla Seaman – Oats St Research Program Manager Rachel Singer – Research Assistant Dr Penny Flett – CEO Jennifer Lawrence - GM Disability, Research and Risk
Oats Street Facility Redevelopment – A Social Cost Benefit Analysis. ACIL Tasman 2010






























