Embed Size (px)
Citation preview

Secular Learning in Anglo-Saxon England, ed. Chardonnens and Carella Amsterdamer Beiträge zur älteren Germanistik 69 (2012), 145–74
‘FOR A BROKEN LIMB’: FRACTURE TREATMENT IN ANGLO-SAXON ENGLAND
Anne Russcher and Rolf H. Bremmer Jr Mention of the Middle Ages often conjures up a picture of dark and crowded places, inhabited by limping, smelly people covered in ulcers for which there was no cure and where a simple infection usually re-sulted in a miserable death. Application of herbal salves or squashed frogs for infected wounds worsened the inflammation sooner than healed it.1 Earlier studies of medieval health care have consequently concluded that ‘medieval people lived in a medically dangerous and helpless world’.2 Is such a conclusion wholly justified? Medically dangerous their world surely was, but perhaps they were not com-pletely helpless, at least not in the case of fractures. Anglo-Saxons had plenty of opportunities to acquire some skill and achieve a moderate success in fracture treatment, which is what this paper seeks to demonstrate. The greater part of the population in Anglo-Saxon England spent their working lives tilling the soil and tending livestock. Nowadays, agriculture ranks among the top three most dangerous occupations in industrialized countries.3 The advent of industrialization has certainly increased the hazards of farm life, but today non-mechanized causes of injury still contribute to approximately forty per cent of all farm-related injuries, consisting of, amongst other mishaps, falls from lofts and ladders, bovine assaults, or accidents with horses on the road.4 These causes of injury are unlikely to have differed significantly in
1 For a reappraisal of Anglo-Saxon pharmacy, see A. Van Arsdall, ‘Challenging the
“Eye of Newt” Image of Medieval Medicine’, The Medieval Hospital and Medical Practice, ed. B. S. Bowers (Aldershot, 2007), 195–205.
2 M. L. Cameron, Anglo-Saxon Medicine, CSASE 7 (Cambridge, 1993), 40. 3 M. Judd and C. Roberts, ‘Fracture Trauma in a Medieval British Farming Village’,
American Jnl of Physical Anthropology 109 (1999), 229–43, at 229. 4 Ibid. 239.

146 Anne Russcher and Rolf H. Bremmer Jr
early medieval England. Reports of incidents resulting in broken bones can be found, for example, in saints’ lives, followed inevitably by their miraculous healing. The Natale Sancti Oswaldi, for example, narrates that ‘[s]um man feoll on ise þæt his earm tobærst and læg þa on bedde gebrocod forðearle’.5 Or, from the Natale Sancti Swyðuni: ‘Sumes þegnes cniht feoll færlice of his horse þæt him tobærst se earm and se oðer sceanca and swiðe wearð gecwysed þæt hi sona wendon þæt he þærrihte sceolde sweltan heom ætforan’.6 In the latter instance, fractures of arm and leg threaten to become lethal injuries. Unreliable timber constructions, too, would lead to serious injury:
Her on þissum geare ealle þa yldestan Angelcynnes witan gefeollan æt Cal-ne of anre upfloran, butan se halgan Dunstan arcebiscop ana ætstod uppon anum beame, 7 sume þær swiðe gebrocode wæron, 7 sume hit ne gedygdan mid þam life.7
Next to domestic and farming accidents, violent assault – whether inflicted in a drunken brawl or on the battlefield – was another im-portant cause of skeletal injury. Blows to arms and legs would often have resulted in fractures. The people who received such blows were not always simple farm hands but frequently the elite, whether drawn from the secular or religious classes. For example, when Guthlac, a noble warrior turned miles Christi, was assaulted by devils, an angel
5 Aelfric’s Lives of Saints, Being a Set of Sermons on Saints’ Days Formerly Ob-
served by the English Church, ed. W. W. Skeat, EETS os 76, 82, 94 and 114, 2 vols (London, 1881–1900) II, 126–8/34–5. ‘A certain man fell on the ice, so that he broke his arm, and he lay in bed severely afflicted’. All translations are ours unless noted otherwise.
6 Ibid. I, 460/323–6. ‘A certain thane’s servant suddenly fell from his horse so that he broke his arm and one of his legs, and was so seriously bruised that they thought at once that he would die on the spot before their eyes’. For more reports of horse-riding accidents, see, e.g., Das altenglische Martyrologium, ed. G. Kotzor, ABAW, philosophisch-historische Klasse, ns 88.1–2, 2 vols (Munich, 1981) II, 200–1; Bischof Wærferths von Worcester Übersetzung der Dialoge Gregors des Grossen über das Leben und die Wundertaten italienischer Väter und über die Unsterblichkeit der Seelen, ed. H. Hecht, Bibliothek des angelsächsischen Prosa 5, 2 vols (Hamburg, 1900–7) I, 81–2.
7 The Anglo-Saxon Chronicle MS E, ed. S. Irvine, The AS Chronicle: a Collabora-tive Edition 7 (Cambridge, 2004), 59. ‘In this year [978] all the chief councillors of the English people fell from an upper storey at Calne, but Archbishop Dunstan re-mained standing upon a beam; and some were severely injured there, and some did not survive it’.

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 147
warned them: Ne sy him banes bryce ne blodig wund, lices læla ne laþes wiht þæs þe ge him to dare gedon motan.8
The warning succinctly sums up the two most frequent kinds of injury in battle: fractures and open wounds. Elsewhere, Andreas, the Old English verse Life of St Andrew, also mentions these two kinds of injuries (1441–1443a):
Geseoh nu seolfes swæðe, swa þin swat aget þurh bangebrec blodige stige, lices lælan;9
Inflicting fractures was a serious crime for which compensation was relatively high. For example, an arm broken above the elbow (humer-us) incurred a penalty of fifteen shillings (and the amount was doubled if both arms were broken); a broken thigh (femur) was double the compensation of a humerus, as was the lower leg: thirty shillings. Ap-parently, an injury that afterwards required crutches was apparently considered to be a greater handicap, and hence a more shameful dis-grace, than were malfunctioning arms.10 Above all other activities in the Anglo-Saxon lifestyle, farming and fighting must have occasioned the most fractures and, consequently, the need for treatment. Fractures that today might cause nothing more than inconvenience and discomfort would often have proved fatal in Anglo-Saxon England.11 We may presume, however, that many people survived their injuries, which encouraged the development of some kind of medical therapy.
8 Guthlac A 698–700 (The Guthlac Poems of the Exeter Book, ed. J. Roberts (Ox-
ford, 1979), 104). ‘Let him not incur the breaking of a bone, or a bloody wound, inju-ry of the body, or any harm from that which you may do to his hurt’.
9 Andreas and the Fates of the Apostles, ed. K. R. Brooks (Oxford, 1961), 46. ‘Now see your track, where your blood has shed a bloody path through the breaking of your bones, the injury of your body’.
10 Æthelberht 53.1 (arm), 65 (leg); Alfred 54–5 (arm), 62–3 (leg) (Die Gesetze der Angelsachsen, ed. and trans. F. Liebermann, 3 vols (Halle, 1903–16) I, 6, 7, 82–5). See also L. Oliver, The Beginnings of English Law (Toronto, 2002), 99–100.
11 L. I. Conrad et al., The Western Medical Tradition: 800 BC to AD 1800 (Cam-bridge, 1996), 126.

148 Anne Russcher and Rolf H. Bremmer Jr
The treatment of fractures is a relatively simple and logical proce-dure mastered by many cultures worldwide, so it seems likely prima facie that the Anglo-Saxons would have had some means for treating such injuries as well. To investigate this matter, we shall first describe the modern standards of fracture treatment. Fractures can occur in any type or size of bone, but this paper will focus on long bone fractures, i.e., fractures of the arms and legs, since these were the most likely to be diagnosed correctly by Anglo-Saxon physicians, and hence most likely to received successful treatment. Then, after we describe com-mon methods for treating these injuries in modern medicine, we will next turn to Anglo-Saxon medical literature and its classical sources. Finally, we shall analyse archaeological evidence of fractures in order to gauge the practice of treatment. Modern Standards for Fracture Treatment The term ‘fracture’ indicates a complete or partial break in the conti-nuity of a bone.12 When a fracture occurs, blood seeps out through torn vessels and collects around the injured bone, forming a haematoma, which is partly responsible for the swelling around the fracture site. Bone-forming cells, known as osteoblasts, deposit new bone from both the outer layer of the fractured bone (periosteum) and the inner layer (endosteum) and quickly begin to bridge the gap. This new layer of bone, called callus, becomes quite thick and forms a bridging collar around the fracture site that acts as a natural splint. The primary callus is subsequently transformed into more mature bone, which in the course of months and years is remoulded and strengthened into fully mature bone. The thick collar of callus gradually dissipates until the fracture resolves completely and the bone is firm again and straight. Each type of fracture has its own optimal treatment. Remarkably, modern fracture treatment still revolves around three fundamental principles, the basics of which were formulated long ago by Hippocra-tes. The first of these three is reduction, i.e., the manipulation of the fractured bone ends into their original anatomical alignment. Reduc-tion is not always necessary; for example, if the bone is fractured in such a way that the ends remain in perfect (or acceptable) apposition where manipulation would cause more harm than good. When the
12 What follows in this section is based mainly on J. Crawford Adams and D. L. Hamblen, Outline of Fractures, including Joint Injuries, 11th ed. (Edinburgh, 1999), 7–10.

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 149
Fig. 1. A: Simple fracture B: compound fracture (Craw-ford Adams and Hamblen, Outline of Fractures, 4)
bone ends are in correct position, it is important to immobilize them (the second principle), so that the bone fragments have time to grow back together. Immobilization is necessary only in unstable fractures. Fractures that need to be reduced often prove to be unstable. When no displacement has occurred, however, immobilization is not always required, but is nonetheless often used anyway, as a measure to relieve pain. Note that fractures of the ulna and femur always require immobi-lization. The third principle of fracture treatment is rehabilitation, aimed at restoring proper function to the body part.13 Today, rehabili-tation usually takes place under the guidance of a physiotherapist; in the past, patients would probably have been guided by pain on the one hand, and the need to survive on the other. Nowadays, the success of fracture treatment is estimated by assessing four criteria: (1) by ob-serving whether union has actually occurred, (2) by measuring degrees of deformity after union for which estimation standards are sometimes formulated, (3) by assessing complications of fractures such as gross vascular or nerve injury, and (4) by assessing functionality of the limb after healing. In order to understand the nature of fractures and their treatment, some further background information on fractures is essential. All fractures are either closed (simple) or open (compound). Closed frac-tures show no contact between the bone and the open air. We speak of open fractures, on the other hand, when there is contact between the fractured bone and the surface, resulting in an accompanying wound (fig. 1). The wound might only be a small puncture, but the distinction is important none-theless, since open fractures carry with them a greater risk of infection, which complicates healing and can result in sepsis (blood poi-soning) and death.
13 Ibid. 28–48.

150 Anne Russcher and Rolf H. Bremmer Jr
Fig. 2. Frequent fracture patterns: 1. transverse (caused by direct trauma: fracture occurs on point of impact), 2. oblique (indirect trauma), 3. spiral (indi-rect trauma), 4. comminuted (direct trauma) (Roberts and Manchester, Archaeology of Disease, 89)
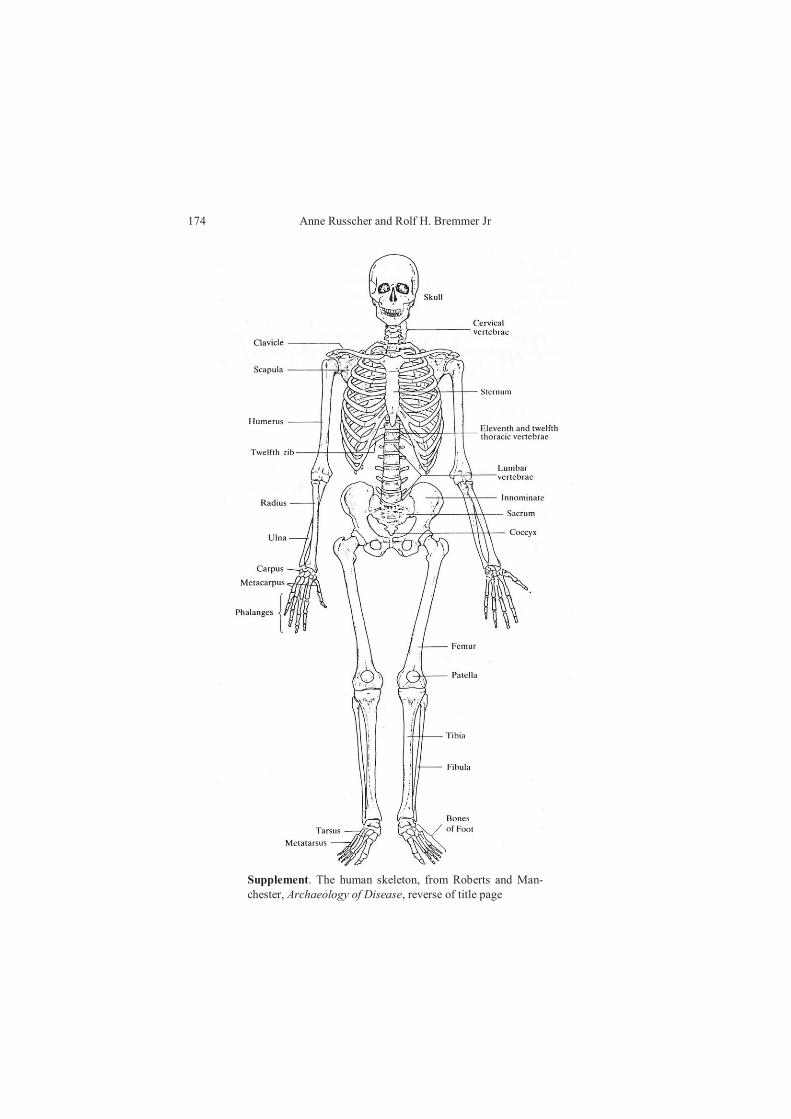
Fractures can occur in many different patterns depending on the force and circumstances which caused the injury (fig. 2).14 It is im-portant to be aware of these different fracture patterns and their natural healing patterns, be-cause if such patterns are left unobserved, erroneous conclusions about whether treat-ment was practised could easily be drawn from archaeological re-mains. The simplest of these patterns is a transverse fracture, in which the bone breaks in two in an angle per-pendicular to the shaft. An oblique fracture runs diagonally across the shaft, and a spiral fracture follows the pattern of a spiral staircase, winding down the shaft of the bone. A transverse fracture is an exam-ple of the sort for which reduction is not always required; sometimes the bone ends are still in perfect apposition and alignment despite the fracture. Immobilization in the form of ‘anatomical splinting’ sometimes oc-curs naturally.15 Anatomical splinting refers to splinting by an accom-panying bone, as in the case of the forearm and the lower leg. These limbs contain two parallel bones, unlike the upper arm and the thigh, which both contain only one bone (see supplement, p. 174). For ex-ample, a transverse, anatomically splinted fracture might heal perfect-ly without any treatment besides rest. The situation is different, however, for oblique and spiral fractures, especially for those occur-ring in the upper arm and the thigh. In such fractures, the broken bone ends slide away from each other, making such injuries extremely dif-
14 C. Roberts and K. Manchester, The Archaeology of Disease, 3rd ed. (Ithaca, 2005), 89; S. Mays, The Archaeology of Human Bones (London, 1998), 162–5; N. C. Lovell, ‘Trauma Analysis in Paleopathology’, Yearbook of Physical Anthropology 40 (1997), 139–70, at 141–4.
15 A. L. Grauer and C. A. Roberts, ‘Paleoepidemiology, Healing, and Possible Treatment of Trauma in the Medieval Cemetery Population of St. Helen-on-the-Walls, York, England’, American Jnl of Physical Anthropology 100 (1996), 531–44, at 541.

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 151
Fig. 3. Stable, transverse fracture versus unstable, oblique fracture (Crawford Adams and Hamblen, Outline of Frac-tures, 6)
ficult to stabilize (fig. 3). Oblique and spiral fractures are also accom-panied by severe muscle strain that pulls the bone fragments into an overlap. In this position, the bone ends will then unite. E-ventually, this unification will result in a short-ening of the in-jured limb and, consequently, in an impairment of function (fig. 4). In order to heal such fractures satisfactorily, reduction must over-come the heavy muscle pull and immobilization is required.
An issue that should not be overlooked in the his-torical evolution of fracture treatment is the availa-bility of radiography which, since c. 1900, has been an indispensable tool in the diagnosis and follow-up treatment of fractures. Today, a diagnosis is always made with the help of a radiographic image.16 In case of a visible deformity, a diagnosis is easy to deter-mine. In many cases, however, the outward appear-ance alone is not sufficient to distinguish between a fracture or a simple strain or contusion. This lack of certainty would have posed an additional difficulty to the Anglo-Saxon physician or bonesetter, and would necessarily have resulted in many misdiag-noses of fractures that would consequently have been left untreated. Archaeologists, thus, may wrongly conclude from such untreated fractures that treatment of fractures was lacking among the Anglo-Saxons generally. In modern practice, radiographs are used to evaluate the success of reduction. After reduction, a standard radiograph is performed to see
16 Crawford Adams and Hamblen, Outline of Fractures, 22.
Fig. 4. limb shortening due to overlap in the lower leg (Craw-ford Adams and Hamblen, Out-line of Frac-tures, 62)

152 Anne Russcher and Rolf H. Bremmer Jr
whether the bones are in acceptable apposition and alignment again or if they still need some adjustment. This kind of fine-tuning in the re-duction process was not available to the Anglo-Saxons. Fractures in the Medical Literature of the Anglo-Saxons The treatment of fractures does not make up a considerable part of the relatively large collection of Anglo-Saxon medical literature.17 All in all, six specific remedies for long bone fractures are mentioned, com-pared to a total number of over a thousand remedies for various ail-ments found in the Anglo-Saxon medical books (‘leechbooks’). This seems strange, since fractures must have occurred frequently in vio-lence-prone, agriculturally-centred Anglo-Saxon society, a claim that is confirmed by analysis of skeletal remains found in gravesites.18 In many cases, the diagnosis and treatment of these fractures would have been rather straightforward. What explains this incongruity between the small number of written remedies for fractures in Anglo-Saxon England in contrast with the much larger number of such injuries found in the archaeological record? A possible explanation may lie in the fact that monasteries, as centres of learning, occupied themselves primarily with theoretical medicine (describing, for example, many kinds of vegetal remedies for internal or external application), while the more practical skill of bone-setting was a matter for secular physi-cians, a craft that – presumably – remained unwritten but instead was passed on by first-hand instruction from master to apprentice.19 In all likelihood, however, such a dichotomy between theorizing monks and practising seculars might very well be too rigid. After all, practical treatments must have been applied in monastic infirmaries. Medical theory, in any case, seems to have been the kind of medicine that was set to vellum, while pragmatic medicine, on the other hand, appears to have remained a lay craft, passed on from master to student directly. Anglo-Saxon medicine was a mixture of native healing techniques and borrowed classical learning. The medicine found in the leech-
17 For good summaries of medical writings in Anglo-Saxon England, see Hollis, ‘Scientific and Medical Writings’, 194–208; Cameron, Anglo-Saxon Medicine, 30–4.
18 C. Wells, Bones, Bodies and Disease: Evidence of Disease and Abnormality in Early Man (London, 1964), 50, and Roberts and Manchester, Archaeology of Disease, 98–100.
19 On tacit or skill-based knowledge in medicine, see A. Van Arsdall, ‘Medical Training in Anglo-Saxon England’, Form and Content of Instruction, ed. Lendinara, Lazzari and D’Aronco, 415–34, at 424–6.

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 153
books centred on the principle of the four humours ultimately derived from Greco-Roman thought, but it also showed a great interest in herbal medicine. At the same time, superstitious, magical and reli-gious medicine were ubiquitous. The leechbooks are characterized by an interest that is confined to specific remedies for specific ailments. Instructions on how to diagnose a disease or how to develop a patho-physiology remained outside the realm of Anglo-Saxon medical cul-ture; nor were these concerns, for that matter, points of concern on the continent. In fact, early medieval medicine was mostly remedy-oriented until about the eleventh century, when the medical schools of Salerno and Montpellier began to spread their influence.20 For that reason, early medieval western medicine was very sparing with de-scriptions of symptoms. What Anglo-Saxon leechbooks we have can be divided into original vernacular texts, translations of Latin treatises and leechbooks in Latin copied in England.21 The existing translations are by no means pedes-trian versions of their originals. While translating, compilers rear-ranged the material for greater ease of use, and sometimes presented English alternatives for exotic Mediterranean herbs, a clear indication that these medicine books were actually consulted and intended for practical use. Translating, however, inevitably introduced errors. Some errors would have been inconsequential, but some changed the meaning of the remedy entirely. An example is the case of the remedy Ad caput deplendum (‘for clearing the head’) which, in the Herbarium of Pseudo-Apuleius,22 became ‘in case one’s hair is falling out’, by reading L deplendum (‘emptying’) as depilendum (‘epilating’). Some-times, Anglo-Saxon translators were apparently so confused by their exemplars that they left out what they were unable to understand. The reasons for such omissions are not always entirely clear, however. When analysing these texts, it is necessary to be aware of the fact that errors may have been introduced by the translator, and – likewise –
20 M. A. D’Aronco, ‘How “English” is Anglo-Saxon Medicine? The Latin Sources for Anglo-Saxon Medical Texts’, Britannia Latina: Latin in the Culture of Great Brit-ain from the Middle Ages to the Twentieth Century, ed. C. Burnett and N. Mann, Warburg Institute Colloquia 8 (London, Turin, 2005), 27–41. See also L. C. MacKin-ney, ‘“Dynamidia” in Medieval Medical Literature’, Isis 24 (1935–6), 400–14.
21 On the influence of Latin learning on vernacular medical texts, see M. A. D’Aronco, ‘Il bilinguismo del medico anglosassone’, Il plurilinguismo in area germa-nica nel medioevo, ed. L. Sinisi, Palomar Athenaeum 49 (Bari, 2005), 39–55.
22 Cameron, Anglo-Saxon Medicine, 62.

154 Anne Russcher and Rolf H. Bremmer Jr
some relevant information may have been omitted, especially in ver-nacular translations from Latin originals. Texts produced by modern editors have many problems as well.23 Therefore, in order to gain a clear picture of the Anglo-Saxon remedies for fractures, we thought it best to discuss the sources briefly. A. Leechbooks The oldest surviving medical text in Old English is London, Brit. Lib., Royal 12. D. xvii, a manuscript that was written c. 950, probably at Winchester.24 It appears to be a copy of a lost exemplar that may have been composed some fifty years earlier, in the last year of Alfred’s reign. The manuscript is divided into three parts: the two-part Bald’s Leechbook (the colophon on folio 109r naming Bald as the owner of the book), followed by Leechbook III, a shorter and less well-organized compilation. Bald’s Leechbook gives a sum total of about 150 læcedomas (‘remedies’) for a wide variety of afflictions, includ-ing remedies against toothaches, baldness and snakebites. It is orga-nized a capite ad calcem (‘from head to foot’), a system that was usual for both antique and contemporaneous medical books. In these works, native Anglo-Saxon remedies are combined with borrowed Mediterranean remedies.25 Bald’s Leechbook I, on the whole, deals more or less with the external manifestations of disease, while Bald’s Leechbook II covers internal diseases. This division, together with the seamless integration of native and borrowed remedies, turns Bald’s Leechbook into a unique scholarly achievement. Leechbook III repre-sents the only surviving Old English example of a standard medical recipe book. Much like its contemporary continental counterparts, it
23 See M. A. D’Aronco, ‘The Transmission of Medical Knowledge in Anglo-Saxon
England: the Voices of Manuscripts’, Form and Content of Instruction, ed. Lendinara, Lazzari and D’Aronco, 35–58; idem, ‘The Edition of the Old English Herbal and Me-dicina de quadrupedibus: Two Case-Studies’, Old Names – New Growth: Proceed-ings of the 2nd ASPNS Conference, University of Graz, Austria, 6-10 June 2007, and Related Essays, ed. P. Bierbaumer and H. W. Klug (Frankfurt a.M., 2009), 35–56; W. Hofstetter, ‘Zur lateinischen Quelle des altenglischen Pseudo-Dioskurides’, Anglia 101 (1983), 315–60.
24 Ker, Catalogue, no. 264; Gneuss, Handlist, no. 479; Doane, Books, no. 10; Bald’s Leechbook: British Museum Royal Manuscript 12 D. XVII, ed. C. E. Wright, EEMF 5 (Copenhagen, 1955). For the milieu and provenance of the manuscript, see Stephanie Hollis’s contribution in the present volume, 11–9, 17–9.
25 Cameron, Anglo-Saxon Medicine, 42.

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 155
pays little attention to symptoms or prognosis but includes remedies only. All in all, it contains about seventy-five such remedies. In Bald’s Leechbook I, extended remedies for fractures are found, for example:
Gif scancan synd forode, nim banwyrt, gecnuwa, geot æges þæt hwite, meng tosomne scanc foredum men. Wið foredum lime lege þas sealfe on þæt forode lim 7 forlege mid elmrinde, do spilc to eft simle niwa oþþæt ge-halod sie gerendra elmrinde 7 awyl swiðe, do þonne of þa rinde genim lin-sæd, gegrind briwe wið þam elmes drænce, þæt bið god sealf foredum lime.26
This remedy takes a sensible approach to the treatment of fractures. Reduction is not mentioned, but the application of splints, providing immobilization of the limb, is discussed. That the application of splints was considered an important part of the treatment is apparent from its explicit mention in the table of contents, which includes ‘Læcedomas wið scancena sare, 7 gif scancan forade synd, oþþe oþer lim; feower cræftas 7 hu mon spelcean scyle’.27 Egg whites, in combi-nation with lime or flour, were used for plaster casts in the Arabic world from at least the ninth century.28 However, no evidence has been found that Anglo-Saxons were familiar with the application of this means of immobilizing broken limbs. Familiarity with the application of splints to fractures may well have to do with the fact that many Anglo-Saxons were raised on or near a farm, where livestock (especially sheep) with broken bones were treated in this way. The evidence for this claim, however, is circum-
26 Bald’s Leechbook I.xxv (Kleinere angelsächsische Denkmäler ed. G. Leonhardi,
Bibliothek der angelsächsischen Prosa 6 (Hamburg, 1905), 21). ‘If legs are broken, take bonewort, pound it, pour the white of an egg, mix together for a man with broken legs. For a broken limb: lay this salve on the broken limb, and overlay it with elm rind; apply a splint; again, always renew [the salve] until [the limb] is healed; strip off some elm bark, and boil it thoroughly; then remove the bark; take linseed, grind it, brew it with the elm drink; that shall be a good salve for a broken limb’.
27 Kleinere angelsächsische Denkmäler ed. Leonhardi, 2. ‘Leechdoms for pain in the legs, and if legs are broken, or another limb, four recipes, and how splints shall be applied’.
28 Immobilization in the form of plaster-of-Paris casts, much practised today, would not be developed until centuries later in the Arabic world, see C. L. Colton, ‘The His-tory of Fracture Treatment’, Skeletal Trauma: Fractures, Dislocations, Ligamentous Injuries, ed. B. D. Browner et al., 2 vols, 2nd ed. (Philadelphia, 1998) I, 3–31, at 5–6.

156 Anne Russcher and Rolf H. Bremmer Jr
stantial. It is found in Pope Gregory the Great’s interpretation of a passage from Ezekiel, wherein the prophet inveighs against the leaders of Israel, calling them bad shepherds (Ezek. 34:3–5):
3 lac comedebatis et lanis operiebamini et quod crassum erat occidebatis gregem autem meum non pascebatis 4 quod infirmum fuit non consolidas-tis et quod aegrotum non sanastis quod fractum est non alligastis et quod abiectum est non reduxistis quod perierat non quaesistis sed cum austeritate imperabatis eis et cum potentia 5 et dispersae sunt oves meae eo quod non esset pastor et factae sunt in devorationem omnium bestiarum agri et dis-persae sunt.29
Gregory, perhaps influenced by the pastoral imagery, quoted this pas-sage in his Regula pastoralis, and interpreted it by using imagery drawn from the world of a medical practitioner:
Hinc pastores increpat per prophetam dicens: ‘Quod fractum est non alli-gastis, et quod abiectum non reduxistis’ [Ezek. 34:4]. Abiectus enim reducitur cum quisque in culpa lapsus, ad statum iustitiae ex pastoralis sol-licitudinis uigore reuocatur. Fracturam uero ligamen astringit, cum culpam disciplina deprimit, ne plaga usque ad interitum diffluat, si hanc districtio-nis seueritas non coartat.30
29 Biblia Sacra iuxta Vulgatam versionem, ed. R. Gryson and R. Weber, 4th ed.
(Stuttgart, 1994), 1315. ‘3 You ate the milk, and you clothed yourselves with the wool, and you killed that which was fat: but my flock you did not feed. 4 The weak you have not strengthened, and that which was sick you have not healed, that which was broken you have not bound up, and that which was driven away you have not brought again, neither have you sought that which was lost: but you ruled over them with rigour, and with a high hand. 5 And my sheep were scattered, because there was no shepherd: and they became the prey of all the beasts of the field, and were scat-tered’: trans. Douay-Rheims.
30 Gregory, Regula pastoralis II.6 (Grégoire le Grand, Règle pastorale, ed. and trans. B. Judic, F. Rommel and C. Morel, Sources Chrétiennes 381–2, 2 vols (Paris, 1992) I, 214/169–75). ‘So, too, he chides the shepherds by the Prophet, saying: That which was broken you have not bound up, and that which was driven away you have not brought back. One who has been cast away is brought back when, after having fallen into sin, he is recalled to the state of righteousness by the influence of pastoral care; and the ligature binds a fracture when discipline subdues sin, lest the wound’s continued flow lead to death if a tight compress does not bind it up. Often, however, the fracture is made worse by an unskilful ligature, so that the lesion causes even greater pain from being bound up too tightly’: Gregory the Great, Pastoral Care, trans. H. Davis, Ancient Christian Writers 11 (Westminster, MD, London, 1950), 66.

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 157
In Old English, this passage from Gregory is translated as: And eft ðurh ðone witgan wæs gecidd ðæm hierdum, ða he cwæð: Đæt sceap ðæt ðær scancforad wæs ne spilcte ge ðæt, & ðæt ðær forloren wæs ne sohte ge ðæt, ne ham ne brohton. Se bringð ham ðone forlorenan se þe mid geornfulnesse ðære hierdelican giemenne ðone þe afielð on synne eft gehwierfð & arærð ðæt he stent on ryhtwisnesse. Hwæt se foroda sceonca bið gewriðen mid ðæm bende, swæ bioð ða synna mid ðæm lareowdome gebundne. Swæ swæ sio wund wile toberan, gif hio ne bið gewriðen mid wræðe, swæ willað ða synna weaxende toflowan, gif hie ne beoð gebundne hwilum mid stræclice lareowdome. & swæðeah oft sio wund bið ðæs þe wierse & ðy mare, gif hio bið unwærlice gewriðen, & him bið ðæt sar þe gefredre, gif sio wund bið to ungemetlice fæste gewriðen.31
The crucial term in this passage is OE spilcte, which Sweet translated as ‘bound up’. This translation, however, is not adequate, since spil-can (spelcean, spylcan) has a wider range of meanings than simply ‘to bind up’. In fact, the verb is derived from the noun spelc (‘splint’),32 itself related to ON spelkur (plurale tantum; ‘a splint for binding up broken bones’),33 and MDu spalke (‘chip, strip of wood; also: for keeping together and supporting a broken bodily part, a splint’).34 To the present day, spelk (‘strip of wood’) is used in England, although its specialized use with the meaning of ‘surgical splint’ seems to have survived only in northern dialects.35 Apparently, when the Anglo-Saxon translator encountered L alligastis in Gregory’s quotation from the Vulgate, he could not help but think of the application of a splint
31 King Alfred’s West-Saxon Version of Gregory’s Pastoral Care, ed. and trans. H.
Sweet, EETS os 45, 50 (London, 1871–2) 122/9–20. ‘And, again, shepherds were blamed through the prophet, when he said: “Ye did not bind up the broken leg of the sheep, nor did ye seek that which was lost, and bring it home.” He brings home the lost one who, with the zeal of pastoral care, brings back and raises up him who falls into sin, so that he stands in righteousness. The broken leg is bound with a bandage; in the same way sins are bound with instruction. As the wound is sure to swell unless bound with a bandage, so will sins increase and spread unless sometimes bound with rigorous discipline. And yet the wound is often aggravated and increased if carelessly bound, and the wound is more painful if bound too tightly’: ibid. 122–3.
32 An Anglo-Saxon Dictionary, ed. J. Bosworth and T. N. Toller (Oxford, 1898). 33 R. Cleasby and G. Vigfusson, An Icelandic-English Dictionary, 2nd ed. revised
W. A. Craigie (London, 1957). 34 J. Verdam, Middelnederlandsch handwoordenboek, revised C. H. Ebbinge Wub-
ben (The Hague, 1932). 35 Oxford English Dictionary Online, accessed 1 July 2011 <http://www.oed. com>.

158 Anne Russcher and Rolf H. Bremmer Jr
to a sheep’s broken leg. The same association was made by Ælfric a century later:
Þæt ðæt losode ic sece 7 þæt aworpen wæs ic ongean læde. þæt þæt to-brocen wæs ic spylce. 7 ðæt untrume ic getrymme.36
In this addition to the homily Dominica secunda post Pasca, Ælfric used forms of the verb spylcan (‘to fasten with a splint’) three times.37 Both the translator of Gregory’s Regula pastoralis and Ælfric – nei-ther of them practising shepherds so far as we know – were apparently led to think of this particular kind of treatment for broken bones with splints. Thus, they translated forms of L alligare to reflect this mean-ing, rather than rendering it with the more general meaning of ‘to bind’.38 Their translations – made independently – strongly suggest that splints were commonly used in Anglo-Saxon England for animals with broken legs. Reduction and immobilization of broken bones, then, whether for animals or humans, appear not to have been unknown techniques in Anglo-Saxon England. The following excerpt from Bald’s Leechbook I describes the kind of injury described in the previous section, namely when a fracture caused the surrounding muscles to pull the fractured pieces into an overlap, resulting in a shortening of the limb. This kind of injury is most often seen in the thigh, as it is described in remedy XXVI:
Monegum men gescrincað his fet to his homme, wyrc baþo, do earban to 7 cersan 7 smale netelan 7 beowyrt, do on troh hate stanas wel gehætte, ge-beþe þa hamma mid þam stan, baðe þonne hie sien geswate þonne recce he þa ban, swa he swiþost mæge, do spelc to 7 betere swa mon oftor mid þy beþige.39
36 Ælfric’s Catholic Homilies: the First Series, Text, ed. P. Clemoes, EETS ss 17
(Oxford, 1997), 536/28–30. ‘That which was lost I will find, and that which was re-jected I shall bring back; that which was broken I shall splint and what is weak I shall strengthen’. For further instances, see ibid. 537/57–61 and 541/209–11.
37 Ibid. 536/25, 28 and 31. Apparently, Ælfric’s use of the verb was overlooked by J. R. Clark Hall, A Concise Anglo-Saxon Dictionary, 4th ed. (Cambridge, 1960), s.v. spelcan, according to whom the verb is found in the Leechdoms only.
38 Oxford Latin Dictionary (Oxford, 1982), s.v. alligo, which gives no instances of a meaning such as ‘to bind with a splint’.
39 Kleinere angelsächsische Denkmäler ed. Leonhardi, 21. ‘In the case of many a man [with a broken leg], his feet shrink up to his buttocks; make baths, add tares and

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 159
The author must have been aware of the severe muscle strain that caused the overlap of the bone fragments, and so he prescribed hot baths to overcome this strain. In sound limbs, hot baths will definitely cause a reduction of muscle tone. Whether this treatment would also work for strains caused by fractures will most likely remain unknown, since fractures are no longer treated this way. However, if hot baths did in fact succeed succeeded in relaxing the muscles, then reduction could certainly have been carried out.40 A note on Cockayne’s translation provides a good example of this procedure. Cockayne renders ‘recce he þa ban, swa he swiþost mæge’ as follows: ‘let him, the patient, duly arrange the bones as well as he can’, which is suggestive of reduction.41 Not only does our translation ‘let him [the patient] stretch his legs as well as he can’ seem to capture the meaning of the passage better, it also makes more sense if the pur-pose of the act is taken into account. Why the patient himself, as in Cockayne’s translation, should carry out reduction is a mystery: pain or the sedating effect of analgesics and anaesthetics – if any were used – would have made reduction by the patient himself impossible. On the other hand, stretching the legs, which the patient himself can do (albeit with significant pain in most cases), and the subsequent appli-cation of a splint by a bonesetter, would still improve the position of the fractured ends and help to keep them straight. Stretching the legs, however, is not equivalent to appropriate reduction. Precise apposition can be achieved only by a strong and knowledgeable person, i.e., an unlikely characterization for someone who has just broken their leg. The splint is intended to provide stabilization and immobilization. Once the patient is removed from the hot stone baths, however, recur-rence of the muscle strain is likely, and with it recurrence of the de-formity. For this reason, apparently, the advice is given to repeat the hot baths. In view of the place and time in which these leechbooks were written, these procedures are reasonable. Whether the treatment would be successful remains doubtful, because general anaesthesia is
cress and small nettle and beewort, put hot stones well heated in a trough, warm the buttocks with the stone bath, when they are in a sweat, then let him [the patient] stretch his legs as well as he can, apply a splint, and it is so much the better the more often one warms [the buttocks] with it [i.e., the preparation]’.
40 See also I. Metzler, Disability in Medieval Europe: Thinking about Physical Im-pairment during the High Middle Ages, c. 1100–1400 (London, 2006), 105.
41 Leechdoms, ed. and trans. Cockayne, II, 69.

160 Anne Russcher and Rolf H. Bremmer Jr
often required to effectively reduce muscle tone so that reduction is possible. External splints are generally not effective enough to keep the fractured bone in the right position. Today, such complicated frac-tures are always managed by operative, internal fixation with plates and screws designed to keep the limb straight. Bald’s Leechbook is generally thought to represent the culmination of medical knowledge in the Anglo-Saxon period.42 It remains uncer-tain whether the principle of reduction was fully understood. That said, fracture treatment by immobilization is demonstrably in evidence in this leechbook. Cameron states that ‘splints are mentioned only twice’ in the medical literature, but fails to mention that these two at-testations are in fact in the only two remedies prescribed for fractures in Bald’s Leechbook I.43 In other words, fractures were invariably treated with splints in Bald’s Leechbook I, putting Cameron’s sugges-tive ‘only twice’ into perspective, because the other remedies in the book had no need for splints.44 B. The Herbarium of Pseudo-Apuleius and its Associated Old Eng-lish Works The work known as the enlarged Old English Herbarium is an English translation of the Herbarium of Pseudo-Apuleius, a text that may have been known to the Anglo-Saxons already in the eighth century, to-gether with two pseudo-Dioscoridean tracts on herbs.45 The Old Eng-lish Herbarium survives in four copies, the oldest of which was produced c. 1000.46 For the most part, the Old English Herbarium lists
42 Cameron, Anglo-Saxon Medicine, 42. 43 Ibid. 12. 44 Cameron’s remark ‘splints are only mentioned twice’ is repeated (without source)
by T. Anderson, ‘The Treatment of the Feet in Anglo-Saxon England’, The Foot 14 (2004), 38–41, at 40.
45 For a full discussion of the Latin sources, see M. A. D’Aronco, ‘Introduction’, The Old English Illustrated Pharmacopoeia. British Library Cotton Vitellius C III, ed. M. A. D’Aronco and M. L. Cameron, EEMF 27 (Copenhagen, 1998), 13–60. See also M. A. D’Aronco, ‘Anglo-Saxon Plant Pharmacy and the Latin Medical Tradition’, From Earth to Art: the Many Aspects of the Plant-World in Anglo-Saxon England, ed. C. P. Biggam, Costerus ns 148 (Amsterdam, New York, 2003), 133–51.
46 London, Brit. Lib., Cotton Vitellius C. iii, fols 11–85 (s. x1 or ximed, Canterbury, Christ Church?; Ker, Catalogue, no. 219; Gneuss, Handlist, no. 402; Doane, Books, no. 4); London, Brit. Lib., Harley 585 (s. x/xi and xi1; Ker, Catalogue, no. 231; Gneuss, Handlist, no. 421; Doane, Books, no. 5); London, Brit. Lib., Harley 6258B (s. xiiex; Ker, Catalogue, xix; Ker, ‘Supplement’, 126, n. 1; Doane, Books, no. 7); Ox-

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 161
medicines compounded from plants; but shorter, related works also list medicines derived from animals, an example of what was former-ly, and sometimes still is, denigratingly called a ‘Dreckapotheke’.47 In the Old English Herbarium, medicines for fractures, excluding those for skull fractures, are mentioned twice. The first states:
Wið banbryce genim þysse ylcan wyrte wyrtruman 7 cnuca mið smerwe þam gelice þe ðu clyþan wyrce, ðonne atyhð hyt of þam lichoman þa to-brocenan ban; ðas wyrte þu scealt niman on þam monðe þe man Iulium nemneð.48
This recipe seems to be designated for treatment of an open fracture, i.e., a fracture in which a there is contact between the bone and the surface, in particular for effectuating the discharge of bone fragments from the wound. Given the nature of this injury, it is not surprising that there is no hint of the aforementioned principles of fracture treat-ment by immobilization, splinting and reduction. In an Anglo-Saxon context, bone setting would be quite impossible for fractures in which the bone was shattered into multiple pieces. Nowadays, surgery is al-ways required for this kind of fracture, so that a surgeon can remove the fragments and then line up the remaining ends. Open fractures in general must have been difficult for Anglo-Saxon physicians to cure, since the danger of a lethal infection would have been a gruesome re-ality in an age still far removed from the invention of antibiotics. Let us consider another remedy from the Old English Herbarium:
Wið banece 7 wið banbryce genim þas ylcan wyrte, cnuca hy, lege to þam bane, þy þriddan dæge him bið sel swylce þær clyþa to gelæd wære.49
ford, Bod. Lib., Hatton 76, fols 68–130a (s. ximed, Worcester?; Ker, Catalogue, no. 328; Gneuss, Handlist, no. 633; C. Franzen, Worcester Manuscripts, ASMMF 6 (Tempe, 1998), no. 5).
47 On ‘Dreckapotheke’, see, e.g., P. Prioreschi, Greek Medicine, A Hist. of Medicine II (Omaha, 1994), 298.
48 Old English Herbarium XV.2 (The Old English Herbarium and Medicina de quadrupedibus, ed. H. J. de Vriend, EETS os 286 (London, 1984), 60/13–6). ‘For broken bone, take the roots of this same plant (dragon), and mix them with grease, just like you make a poultice; the broken bones will appear out of the body. You should gather the plant in the month called July’: A. Van Arsdall, Medieval Herbal Remedies: The Old English Herbarium and Anglo-Saxon Medicine (London, New York, 2002), 155.
49 Old English Herbarium LI.1 (The Old English Herbarium and Medicina de quad-

162 Anne Russcher and Rolf H. Bremmer Jr
Leg ache and leg breach are taken together here, perhaps indicating that the recipe is not so much intended as a treatment for a broken bone, but rather as a remedy for delivering patients from the pain as-sociated with such a fracture. A general question that should be borne in mind while analyzing the Old English Herbarium is whether this text can actually be considered a suitable source to look for fracture treatment. The Old English Her-barium, as its title reveals, concerns itself with herbal remedies, which do not play a great part in the treatment of fractures. As it stands, nu-merous remedies for various ailments are listed per herb. We might deduce, therefore, that it was never the intention of the compiler or translator to present a complete treatment protocol. Where the text addresses fractures, it would appear – at most – to aim only at com-plementing a more thoroughgoing treatment (presumably conducted by a bonesetter) with herbal remedies. In contrast to Bald’s Leechbook which takes diseases as its ordering principle, the Old English Herbar-ium may be classified as a pharmacopoeia, i.e., a list of medicinal drugs together with information on their preparation and use. One of the works associated with the Old English Herbarium is the Medicina de quadrupedibus, a vernacular compilation consisting of three parts, the third of which is a translation/adaptation of the Liber medicinae ex animalibus, attributed to Sextus Placitus. As indicated by its title, this treatise lists medicines derived from animals or animal products. It includes two remedies for the treatment of fractures, the first of which is short and reassuringly optimistic: ‘Wiþ bryce fearres gor wearm lege on þone bryce, syþþan him bið sel’,50 while the second one entails more extensive treatment: ‘To gehwylcum bryce hundes brægen aled on wulle 7 on þæt tobrocene to gewriþen feowertyne dagas, þonne byþ hyt fæste gebatod, 7 þær byð þearf to fæstere gewriðennysse’.51 Neither of these two prescriptions seems likely to produce a sound limb. However, the same that holds true for the Old rupedibus, ed. de Vriend, 96/16–8). ‘For aching or broken legs, take the same plant [madder], pound it, and lay it on the leg. In three days, the place on which the poultice was laid will be much better’: Van Arsdall, Medieval Herbal Remedies, 173.
50 Medicina de quadrupedibus XII.11 (The Old English Herbarium and Medicina de quadrupedibus, ed. de Vriend, 268/20– 1). ‘For a fracture: lay a bull’s dung warm on the fracture; afterwards it will be well with him’.
51 Medicina de quadrupedibus XIV.9 (Ibid. 270/25–7). ‘For any fracture: a dog’s brain laid upon wool and bound upon the broken place for fourteen days; then it will be firmly healed, and there will be a need for a firmer binding up’.

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 163
English Herbarium also applies to the Medicina de quadrupedibus, in that it is organized by medicinal ingredients, not by illness or injury. These two remedies for fractures are grouped in the manuscripts near or under the drawing of a bull and a dog, respectively,52 included in lists that discuss multiple applications of bull dung and dog products for various ailments. Like those in the Old English Herbarium dis-cussed above, these remedies might have been intended only as com-plementary measures. In any case, these were certainly not sound complementary measures: when dealing with an open fracture, bull dung would have been catastrophic for the patient in that it would cer-tainly cause infection. The remedy with dog brain, on the other hand, might have some utility. According to the text’s author, a firmer binding is required af-ter fourteen days, a treatment which implies an attempt at stabilizing and immobilizing the fracture. It is a testimony to the author’s good sense to advise the leech to wait a few days before firmly binding up the wound, since by then the initial swelling will have subsided. If binding is carried out too soon after the fracture has occurred, before the swelling has reached its peak, arteries and nerves might be com-pressed, leading to necrosis (death of tissue) and functional impair-ment. Hippocrates was aware of these potential complications, which he describes in his treatise On Fractures.53 Their prevention might have found its way into certain Latin works as well, and via this route into Old English translations. Fracture Treatment according to Classical Sources It is unlikely that all the Anglo-Saxon knowledge concerning fractures has been preserved. For that reason, it may be instructive to look at the sources available to Anglo-Saxons physicians in order to make up for what we lack in direct evidence. Anglo-Saxon medical literature con-sists predominantly of reworkings or translations of Latin works. Greek was not routinely studied, except perhaps by those under the direct influence of Theodore and Hadrian at Canterbury,54 but many of
52 The Old English Illustrated Pharmacopoeia, ed. D’Aronco and Cameron, 81vb
(bull), 82rb (dog). 53 Hippocrates III, ed. and trans. E. T. Withington, Loeb Classical Lib. 149 (Lon-
don, 1944), 107–11 and 123. 54 M. C. Bodden, ‘Evidence for the Knowledge of Greek in Anglo-Saxon England’,
ASE 17 (1988), 217–46; idem, ‘The Preservation and Transmission of Greek in Early

164 Anne Russcher and Rolf H. Bremmer Jr
the principal post-Hippocratic medical texts in Greek had already been either translated into Latin or summarized and digested in Latin by the sixth and seventh centuries.55 One of the first classical authors to write extensively on the treat-ment of fractures is Hippocrates of Cos (460–370 BC). In his treatise On Fractures, he conscientiously describes the treatment of bone frac-tures. Hippocrates distinguishes between closed and open fractures and their differing prognoses; open fractures, he notes, are much more serious because of the risk of infection. He gives precise and detailed directions on how to reduce various kinds of fractures and subsequent-ly on how to splint them. His instructions range from information on the required length of the splint to a schedule prescribing when the splints should be renewed. Hippocrates recognized that the joints above and below the fracture should be immobilized, as is common practice today. Furthermore, he points out certain possible complica-tions, such as pressure sores that may develop if a patient is bedridden for a substantial length of time. In general, despite his limited means, Hippocrates’ anatomical information concerning bones and their sur-rounding structures is usually correct (by modern standards) and his proposed treatment for fractures is detailed and sensible. Hippocrates’ writings were available in the early medieval west, as is clear, for ex-ample, from the works of Cassiodorus. On the other hand, Isidore of Seville, in De medicina, refers to him only as one of the founders of the study of medicine, without giving any further evidence of having knowledge of the contents of his works.56 Parts of Hippocrates’ works were transferred in Latin summaries, e.g., dietary books, compilations, herbals and so on, although the process of summarization reduced the quality of his ideas. In the centuries after Cassiodorus, however, de-monstrable familiarity with Hippocrates in the west, and hence also in Anglo-Saxon England, is negligible.57
England’, Sources of Anglo-Saxon Culture, ed. P. E. Szarmach (Kalamazoo, 1986), 53–63.
55 Cameron, Anglo-Saxon Medicine, 65. 56 Isidore, Etymologiae IV.iii (Isidori Hispalensis episcopi Etymologiarum sive
Originum libri XX, ed. W. M. Lindsay, 2 vols (Oxford, 1911) I). 57 M. Lapidge, The Anglo-Saxon Library (Oxford, 2006), 18 and 22; Gneuss, Hand-
list, does not mention a single manuscript with any of Hippocrates’ works; see also J. D. A. Ogilvy, Books Known to the English, 597–1066 (Cambridge, MA, 1967), 159. On Hippocrates in the early medieval west, see S. Ihm, Clavis commentariorum der antiken medizinischen Texte, Clavis Commentariorum Antiquitatis et Medii Aevi 1

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 165
Galen (129–199/217 AD) discussed fractures and their treatment in both his Ars medica and Therapeutica (or De methodo medendi).58 He served as a physician to the gladiator school in his native Pergamum in what is now Turkey, where he gained extensive experience with treating traumas. In the Ars medica, Galen developed a plan for the treatment of open wounds which he then adapted for the treatment of fractures. Both procedures involved bringing the separated parts to-gether and keeping them in this state to allow nature to work its cure. For wounds, Galen used stitches; for fractures, he availed himself of chalkstone to make a binding around the break to form a circle, there-by providing a rigid splint. He chose chalkstone because of its similar-ity to bone in form. Like Hippocrates, he also recommended a diet to enhance the healing of the fracture. Of the classical physicians, Galen was also the first to describe the apparatus known as a glossoconium, i.e., a device designed to reduce a fracture by means of traction (fig. 5). The glossoconium proved particularly useful for stabilizing femoral fractures: it allowed them to heal in the right position. However, Galen be-lieved that traction should be discontin-ued once splints had been applied, thereby not utilizing the ap-paratus to its maximum effect. Unfortunately, only descriptions of Ga-len’s glossoconium remain, none of which include graphic representa-tions; so we cannot know for certain what this apparatus looked like and whether it was indeed useful for treating fractures. Traction as a part of fracture treatment does not reappear on the medical scene until (Leiden, Boston, Cologne, 2002), 19–20.
58 De methodo medendi, along with some of Galen’s other treatises, survives in one Anglo-Saxon manuscript, viz. Cambridge, Peterhouse 251, fols 106–191 (s. xiex or xi/xii, Canterbury, St Augustine’s; Gneuss, Handlist, no. 145; Gameson, Manuscripts, no. 117). However, this late manuscript gives evidence not to a long tradition of fa-miliarity but to recent developments in the schools of medicine, inspired by especially the Schola medica Saliternitana (personal communication, Maria D’Aronco). See also Hollis’s contribution in the present volume, 36–9.
Fig. 5. The elastic pull of the muscles that causes over-lap of bone fragments can be balanced by sustained weight traction (Crawford Adams and Hamblen, Out-line of Fractures, 42)

166 Anne Russcher and Rolf H. Bremmer Jr
the fourteenth century.59 After Galen the next most influential Greek medical writer was Di-oscorides (c. 40–90 AD), who was born Asia Minor but practised medicine in Rome. His De materia medica is a pharmacological work containing over two thousand recipes and formulas, grouped into five books and arranged according to the pharmaceutical properties of the various materials. Dioscorides gave medical recipes derived from plants, animals and minerals. The sheer size of De materia medica probably restricted its practical usefulness, but his pharmacopeia was translated, edited and abridged and, as a result, survived in many dif-ferent forms. It was considered an authoritative work until well into the seventeenth century, when its popularity began to wane due to the development of modern botanical classifications.60 De materia medica contains four references to fractures, none of which mention or even hint at reduction, immobilization or splinting.61 However, this silence need not surprise us since, like the Herbarium of Pseudo-Apuleius, De materia medica is primarily a pharmacologi-cal work, identifying natural materials and explaining their medicinal uses; it is not an orthopaedic manual. Medicines that are mentioned in relation to treatment of fractures show similarities between Hippocra-tes’ instructions for fractures and Anglo-Saxon measures. For in-stance, Dioscorides mentions greasy wool as a bandage and recommends the application of cerate to fractures; the latter had also been advocated by Hippocrates. He furthermore recommends that a decoction of elm roots or elm leaves should be poured over fractured bones to ‘knit them quickly’.62 As we have seen, elm appears in Bald’s Leechbook I as ‘a good salve for a broken limb’.63 As far as we know, however, Dioscorides’ massive work remained unknown to Anglo-Saxons,64 but pseudo-Dioscoridean texts, notably Liber medicinae ex
59 Colton, ‘The History of Fracture Treatment’, I, 9. 60 V. Nutton, Ancient Medicine (Abingdon, 2005), 174–5. 61 De materia medica by Pedanius Dioscorides, trans. L. Y. Beck (Hildesheim,
2005), I.55.3, I.84.1, II.73.1, IV.22.1. 62 Ibid. 63. 63 The curative effects of elm for fractures were widely recognized in the Middle
Ages, see, e.g., E. G. Sánchez, ‘Utility and Aesthetics in the Gardens of al-Andalus: Species with Multiple Uses’, Health and Healing from the Medieval Garden, ed. P. Dendle and A. Touwaide (Woodbridge, 2008), 205–27, at 220.
64 Cameron, Anglo-Saxon Medicine, 76; see also J. M. Riddle, ‘Dioscorides’, Cata-logus translationum et commentariorum: Mediaeval and Renaissance Latin Transla-

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 167
herbis femininis and Curae herbarum, circulated widely as part of the Old English Herbarium.65 Fractures do not seem to have interested the remainder of classical, late antique and early medieval authors whose works were known by the Anglo-Saxons. These include Oribasius of Pergamum (c. 320–400), Alexander of Tralles, a sixth-century physician, and Caelius Au-relianus, a fifth-century physician.66 All of their medical works are silent on the treatment of fractures. Classical authors seem, on the whole, to have been concerned much more with internal diseases than with injuries. This observation might support the hypothesis that car-ing for injuries was not primarily the domain of literate physicians, but rather of a separate class of bonesetters or surgeons. Perhaps boneset-ters never recorded their expertise in writing, as was the case with many practical professions in the past that have left no traces of the tricks of their trade. This is the situation, for example, with black-smiths and carpenters. In the words of J. M. Riddle: ‘Medical educa-tion was conducted by the physician father teaching his son or apprentice’.67 Archaeological Assessment of Fractures It is striking how sparse references to fracture treatment are in Anglo-Saxon medicine, especially given how plentiful they must have been in Anglo-Saxon society. Textual evidence alone cannot tell us every-thing we want to know. Because of their theoretical nature and their focus on internal diseases, it is difficult to assess on the basis of the leechbooks alone how sophisticated Anglo-Saxon treatment for bro- tions and Commentaries, Annotated Lists and Guides IV, ed. F. E. Cranz and P. O. Kristeller (Washington, DC, 1980), 1–143.
65 Vitellius C. iii; Harley 585; Oxford, Bod. Lib., Ashmole 1431 (s. xi/xii, Canter-bury, St Augustine’s; Ker, Catalogue, no. 289; Gneuss, Handlist, no. 527; Gameson, Manuscripts, no. 622; Doane and Grade, Deluxe and Illustrated Manuscripts, no. 8); Oxford, Bod. Lib., Bodley 130 (s. xiex, prob. Bury St Edmunds; Ker, Catalogue, no. 302; Gneuss, Handlist, no. 549; Gameson, Manuscripts, no. 636; Franzen, Worcester Manuscripts, no. 2); Hatton 76.
66 For these and other authors known in Anglo-Saxon England, see M. L. Cameron, ‘The Sources of Medical Knowledge in Anglo-Saxon England’, ASE 11 (1982), 135–55. For indications that the compilers of Bald’s Leechbook were familiar with some of these, see idem, ‘Bald’s Leechbook: its Sources and their Use in its Compilation’, ASE 12 (1983), 153–82.
67 J. M. Riddle, ‘Theory and Practice in Medieval Medicine’, Viator 5 (1974), 157–84, at 159. See also Van Arsdall, ‘Medical Training’.

168 Anne Russcher and Rolf H. Bremmer Jr
ken limbs were, whether these treatments were applied inside or out-side a literate, monastic setting. For this reason, any investigation into the capacity of the Anglo-Saxons to treat fractures would not be com-plete, without considering relevant archaeological evidence that may afford a glimpse into who tended to suffer from fractures and how they coped with their injuries. Searching for this kind of evidence in the archaeological record, however, necessarily brings with it a number of pitfalls. The fact that Anglo-Saxon physicians – who were in many ways no different from any other doctor before the twentieth century – had to diagnose frac-tures without recourse to radiography will of course have led to erro-neous diagnoses. Failing to diagnose a fracture properly most likely meant that no treatment was given, or, at best, an inappropriate one. The visible remains of these untreated fractures might very well lead archaeologists to conclude that proper treatment for fractures was un-known at the time. Such evidence, however, should not be interpreted as lack of treatment, but perhaps instead of an erroneous diagnosis or of unsuccessful or inappropriate treatment (as still happens today). Another pitfall involves the transverse, non-displaced fracture that not infrequently healed without having had reduction applied to it. From such cases, archaeologists might mistakenly conclude that treatment was applied successfully since, by all appearances, the fracture had healed. Similarly, some fractures, especially those that occur in chil-dren, heal so well that they cannot be seen in the bone later in life, at least not macroscopically. In theory, such a case might have resulted from successful treatment, but it would never be acknowledged as such. There are other problems with interpreting the archaeological record as well. According to Wells, for example, the Anglo-Saxons suffered fractures of the legs more frequently than of the arms,68 whereas Rob-erts concluded in her survey of analyses of late medieval cemeteries that arms were broken more often than legs.69 This incongruity of con-clusions can plausibly be explained by the fact that Anglo-Saxon soci-ety was predominantly rural, while life in late medieval England had become much more urban in nature. The general trend seems to be that rural populations break their lower limbs more often, whereas
68 Wells, Bones, 50. 69 Roberts and Manchester, Archaeology of Disease, 99.

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 169
Fig. 6. Left: fractured tibia and fibula sur-rounded by callus, right: healed, angulated end-result (Crawford Adams, 61)
urban populations more often break their forearms. Fractures of the thigh and upper arm are altogether rare. On the whole, rural popula-tions were much more prone to fractures than urban populations, a distinction that is also observed by Judd and Roberts.70 Calvin Wells, an archaeologist who specifically studied fractures and their treatment in the Anglo-Saxon period, arrived at the conclu-sion that anatomically splinted bones healed well, but ascribes these results to the fact that the initial displacement in these fractures proba-bly was negligible, not because skilful reduction was applied. Oblique fractures of the femur, humerus or tibia healed solidly, but almost in-variably with overlap of the bone ends and hence with consequent shortening of the limb.71 Why such oblique fractures are difficult to re-duce and immobilize has been explained above. Wells remarks that angulation of the fragments (angular distortion of a broken bone both before and after healing) is not found as often as might be expected in the presence of such oblique fractures (fig. 6). There might be overlap, but the fragments often lie reasonably parallel. This re-sult can be explained only by assuming that active man-agement of the bone frag-ments has taken place. The overlap as such might have been too difficult to overcome, but angula-tion can quite easily be corrected. Wells’ overall conclusion is that Anglo-Saxon treatment of fractures made virtually no difference to what ‘the natural healing powers of the body would have achieved unaided’, granting an exception to the improvement of angulation.
70 Judd and Roberts, ‘Fracture Trauma’, 242. 71 C. Wells, ‘The Results of Bone Setting in Anglo-Saxon Times’, Medical and Bio-
logical Illustration 24 (1974), 215–20.

170 Anne Russcher and Rolf H. Bremmer Jr
However, Wells does not make clear what data and what statistical analysis of that data he refers to when he states that ‘final repair was often good’ or ‘the final result … was almost invariably bad’.72 He gives selected photographic examples along with the text and claims that they exemplify the Anglo-Saxon repair of fractures, but never gives any statistics, sources or other cumulative data. Another archaeologist who studied fractures to discover whether Anglo-Saxons would have treated them (successfully) is Charlotte Roberts. In her dissertation, she discussed over forty Anglo-Saxon fractures occurring in different bones of skeletons unearthed from var-ious cemetery sites from all over England. Based on a comparison of the results of healing with modern standards of deformity after a breach, she concluded that all fractures had healed successfully, bar-ring only a few exceptions. These exceptions, she explains, include bones healed with deformity of a kind which is often found in modern patients post treatment; moreover, all six samples were fractured fem-ora. All fractured femora had healed with overlap of bone fragments and limb shortening.73 Roberts did not confine her research to the An-glo-Saxon period but also analysed fractures from the preceding Ro-man period and the later medieval period. Interestingly, she concluded that Roman fractures had healed as successfully as the Anglo-Saxon fractures, but all later medieval fractures had healed worse than the fractures of the preceding two periods. Her observations led her to theorize that, within small rural Roman and Anglo-Saxon communi-ties, knowledge of fracture treatment (reduce, splint, rest) probably developed as a result of practical experience, perhaps supplemented by Mediterranean surgical knowledge. Bonesetters made their appearance in Europe at some point in the medieval period,74 but how many there were is unknown, and what remuneration they would have received for their services remains a guess. It is possible that the expense resulting from the need to employ a professional bonesetter to treat a fracture after a sudden, unexpected injury might have led many to rely instead on the cheaper – and less expert – treatment available from relatives. If true, this possibility may
72 Ibid. 220 and 218, respectively. 73 Roberts, ‘Trauma and its Treatment’, 208–9. 74 Grauer and Roberts, ‘Paleoepidemiology’, 539. The word bonesetter itself is re-
corded for the first time c. 1500, see the electronic Middle English Dictionary, ac-cessed 1 July 2011 <http://quod.lib.umich.edu/m/med>, s.v. bon (n.(1)).

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 171
have resulted in a lower number of properly healed fractures. Roberts also draws attention to the unhygienic living conditions in medieval towns that often lead to infections that hampered healing. Anglo-Saxons were not necessarily more hygienic than people in the later Middle Ages, but the increase of people living closely together in in-creasingly urbanized settings may have led to less hygienic conditions. The fact that all fractures investigated by Roberts had healed is also indicative of another important factor: care. In an adult male, a frac-tured femur will take at least four months to heal, both today and in Anglo-Saxon England. During this period, the patient is unable to stand on his leg, a temporary handicap that makes most work impossi-ble. All this time, the injured Anglo-Saxon would have been depend-ent on his relatives and friends for food and care, both of which seem to have been provided, as we may tentatively conclude from the healed specimens. Unlike the written evidence derived from leechbooks, material evi-dence for active treatment in the form of splints has not yet been re-covered from Anglo-Saxon graves or other excavation sites. This is not surprising, perhaps, since there would be no need to keep wearing a splint if a fracture had healed successfully, or to bury the patient with it if it had not. Moreover, splints were most likely made of bio-degradable materials that do not tend to withstand time.75 An example is elm rind, which is mentioned in Bald’s Leechbook I. Would common sense combined with limited means have sufficed to trigger effective treatment of fractures in the Anglo-Saxon period? To answer this question it might be helpful to look into fracture treat-ment as practised by traditional societies today. Although the Anglo-Saxon and modern traditional societies are separated by time and space, the circumstances, viz. non-access to medical sources and mate-rials, are likely to be shared. Oyebola has studied the bone-setting abilities of the Yoruba in Nigeria. The Yoruba were able to diagnose major breaks, but, lacking radiographic facilities, they missed subtler cases, such as hairline or greenstick fractures where the bone is not entirely split in two. They applied and reapplied herbal dressings and splints, but healing was delayed because reduction was not maintained consistently (by rigid immobilization) and patients were mobilized too
75 Grauer and Roberts, ‘Paleoepidemiology’, 532; Roberts and Manchester, Archae-
ology of Disease, 130.

172 Anne Russcher and Rolf H. Bremmer Jr
quickly.76 Nonetheless, it is clear that treatment was practised with moderate success. Other developing societies also treat fractures by reduction and splinting of broken bones with natural products, such as bark or reeds, or even hardened animal skins in Alaska.77 The efficacy of these treatments is not always clear, but it shows that reducing and immobilizing fractures is indeed a fairly simple and straightforward process to learn. Archaeological studies into Anglo-Saxon fractures are few and their conclusions often turn out to be contradictory. However, in the most detailed study of Anglo-Saxon fractures and their treatment based on archaeological remains to date, Roberts concluded that the Anglo-Saxons actively treated of fractures – up to this point Wells agrees78 – and that the outcome was generally good. However, Anglo-Saxons (and later medieval and post-medieval practitioners) by and large lacked the facilities to effectively treat oblique and spiral fractures of the femur and, as a result, patients with such injuries would have had to spend the rest of their lives deformed and limping. Conclusion Hippocrates already knew that ‘he who desires to practice surgery must go to war’.79 Warfaring, physically active Anglo-Saxons would have had ample opportunities to develop skill in fracture treatment, provided the knowledge gained from experience and, to a lesser ex-tent, learning was there. Today we still employ three mainstays in the treatment of long-bone fractures: reduction, immobilization and reha-bilitation, procedures that were already known in antiquity, and which the Anglo-Saxons might have used to their advantage. Anglo-Saxon references to fracture treatment, as we have shown, are sparse. From the leechbooks, it is altogether impossible to conclude without hesita-tion whether reduction was practised or not, but splints seem to have been common treatment. That reduction was practised can, in all like-lihood, be inferred from archaeological remains. Although femoral fractures almost invariably healed badly, Anglo-Saxons seem to have
76 D. D. Oyebola, ‘Yoruba Traditional Bonesetters: the Practice of Orthopaedics in a
Primitive Setting in Nigeria’, Jnl of Trauma 20 (1980), 312–22. 77 Roberts and Manchester, Archaeology of Disease, 129. 78 Wells, ‘Results of Bone-Setting’, 220. 79 A. S. Lyons and R. J. Petrucelli, Medicine: an Illustrated History (New York,
1987), 213.

‘For a Broken Limb’: Fracture Treatment in Anglo-Saxon England 173
made a difference in the outcome of many other fractures, since they did adjust the degree of angulation in many fractures, thereby prevent-ing or diminishing the risk of functional impairment after healing. The number of healed fractures suggests to us the presence of contributing care from the community, a care that kept the patient alive and well-fed during a period of convalescence that could have lasted for a peri-od of months, during which time the patient would have been unable to look after himself. All in all, a picture emerges of a community that took care of itself, was able to recognize fractures and helped them heal through immobilization with the help of splints. It seems justi-fied, therefore, to nuance Cameron’s view, quoted in our introduction, that Anglo-Saxons lived in a ‘medically … helpless world’. Limita-tions are present nonetheless in the ironic fact that those fractures that were most easily diagnosed (without radiography) were also the ones most difficult to treat without impairment after healing. The picture that we have gained is still far from complete, and it seems unlikely to us that full certainty about the results of fracture treatment in Anglo-Saxon England will ever be achieved. Yet, some areas are still open to be explored. An examination of early medieval continental treatment of fractures exceeds the scope of this paper, but it would be extremely helpful to widen our understanding of medieval fracture treatment. We know that bonesetters were active in the late Middle Ages on the continent, but not when and how they developed their craft. Furthermore, we have surveyed classical sources to allow us to make an estimation of the knowledge of fracture treatment avail-able in Anglo-Saxon England, fully aware that not all these sources read by the Anglo-Saxons have actually come down to us. That said, a closer assessment of the classical texts of which we are sure were available to the Anglo-Saxons might fine-tune our knowledge of the possibilities for treatment. Likewise, more skeletal remains are proba-bly available for more systematic and extensive research on fracture treatment than have been analysed so far. Future research should con-centrate on these points and should be multidisciplinary in character, since bridging the gap between disciplines is the only way to bridge the gap in time to learn more about the fascinating world of Anglo-Saxon medicine.80
80 We like to express our deep gratitude to Professor Maria Amalia D’Aronco for
her constructive comments on a draft version of this paper.
174 Anne Russcher and Rolf H. Bremmer Jr
Supplement. The human skeleton, from Roberts and Man-chester, Archaeology of Disease, reverse of title page






![Elfrico grammatico e l'insegnamento linguistico nell'Inghilterra anglosassone ['Ælfric as a Grammarian and Language Teaching in Anglo-Saxon England'] [1991]](https://img.pdfslide.net/doc/110x75/6351db48ba4994660704eb3e/elfrico-grammatico-e-linsegnamento-linguistico-nellinghilterra-anglosassone-alfric.jpg)






















