Embed Size (px)
Citation preview

Introduction
Sonography is the technique of choice for routineevaluation of the brain in premature infants and forthe study of a broad range of pathological condi-tions in full-term neonates. Improvements in imageresolution and the use of additional acoustic win-dows, such as the posterior and mastoid fontanelles,now allow proper visualization of the brain stemand posterior fossa. Familiarity with the sono-graphic brain anatomy and artifacts related to thetechnique is essential for proper interpretation ofthe studies.
This pictorial essay illustrates several normal struc-tures, anatomic variants and scanning artifacts relatedto the ventricular system, choroid plexus and brainparenchyma, which can mimic pathology on neonatalcranial sonography. The work is based on cranial USstudies that were performed on a routine basis on 176premature neonates and on 26 full-term newborns toinvestigate brain pathology. We used the anterior,posterior and mastoid fontanelles as acoustic windows.All the images referred to as pitfalls belonged to infantswho were followed up using US and found to beneurologically and developmentally normal on clini-cal assessment. Images of several brain disorders areincluded for comparison purposes.
ORIGINAL ARTICLEPediatr Radiol (2003) 33: 110–117DOI 10.1007/s00247-002-0836-y
Goya Enrıquez
Flavia Correa
Javier Lucaya
Joaquim Piqueras
Celestino Aso
Aranzazu Ortega
Potential pitfalls in cranial sonography
Received: 8 February 2002Accepted: 29 August 2002Published online: 22 November 2002� Springer-Verlag 2002
G. Enrıquez (&) Æ F. Correa Æ J. LucayaJ. Piqueras Æ C. AsoDepartment of Pediatric Radiology,Hospital Vall d’Hebron, Ps. Vall d’Hebron119-129, 08035 Barcelona, SpainE-mail: [email protected].: +34-93-2746793Fax: +34-93-2746775
A. OrtegaDepartment of Pathology,Hospital Vall d’Hebron, Ps. Vall d’Hebron119-129, 08035 Barcelona, Spain
Abstract Background: We presentseveral anatomic variants of thebrain and artifacts related to scan-ning techniques which could bemisinterpreted as lesions on neonatalcranial sonography. Materials andmethods: The findings were derivedfrom US studies performed on 176premature infants and 26 full-termnewborns, using the anterior,posterior and mastoid fontanellesas acoustic windows. Results: Thepseudolesions are divided into threegroups: ventricular system(asymmetric lateral ventricle sizeand coarctation of the lateralventricles); choroid plexus (‘‘split’’choroid, ‘‘truncated’’ choroid andchoroid cyst); and brain paren-chyma (peritrigonal blush, thalamicpseudolesion, pseudo-absence of theinferior vermis, occipital
pseudomass and calcar avis simu-lating intraventricular clot). Weprovide images of these pseudole-sions and clues to their differentia-tion from true brain pathology.Images of several brain disordersare included for comparison.Knowledge of these potentialpitfalls is essential for proper inter-pretation of US brain studies andwill help to avoid the use of othermore invasive diagnostic tests.Conclusions: Misleading imagesseen on US examination of theneonatal brain that could bemisinterpreted as pathology arepresented, with clues to theirdifferentiation from true lesions.
Keywords Ultrasound Æ Brain ÆVariants Æ Pitfalls
Ventricular system
The most common anatomic variants related to theventricular system are asymmetric lateral ventricle sizeand lateral ventricle coarctation.
Asymmetric lateral ventricle size
Sonographic recognition of lateral ventricular asymme-try in neonates was first reported in the 1980s (andbefore that at autopsy and by ventriculography). It wasassessed subjectively by inspection of the images [1] orwas defined by a difference in ventricular width of morethan 2 mm [2]. We subjectively observed some degree oflateral ventricle asymmetry in 77% of 84 normalneonates, the left ventricle being wider than the right in90%. Our experience has shown that the enlarged ven-tricle is often associated with a larger ipsilateral choroidplexus (Fig. 1a, b). The ventricular asymmetry is usuallymore pronounced in the most posterior portion of theoccipital horn, a fact that should be taken into account,particularly when using the posterior fontanelle asacoustic window (Fig. 1c). This posterior approach canbe used to evaluate intraventricular hemorrhage in themost dependent portion of the lateral ventricle.
Reference tables that attempt to establish normalventricular measurements are available [3, 4] but we donot rely on single measurements alone to establish nor-mality in all cases of asymmetry. Preservation of the
lateral ventricle triangular configuration in coronalviews, thin ventricular walls showing only faint echo-genicity and no increase in size on follow up scans are,in our experience, the clues suggesting normality.
Coarctation of the lateral ventricles
This unusual uni- or bilateral variant consists in a focalapproximation of the ventricle walls at any point medialto their external angle [5]. When the approximation iscomplete or nearly complete, the external part of theventricle acquires a rounded configuration, simulating acyst (Fig. 2). Coarctation should not be confused withgerminal matrix cyst or cystic periventricular leuko-malacia (PVL) (Fig. 3). To differentiate these entitiesfrom coarctation, it is essential to carefully note theposition of the cystic image in relation to the externalventricle angle. A diagnosis of germinolytic cyst should
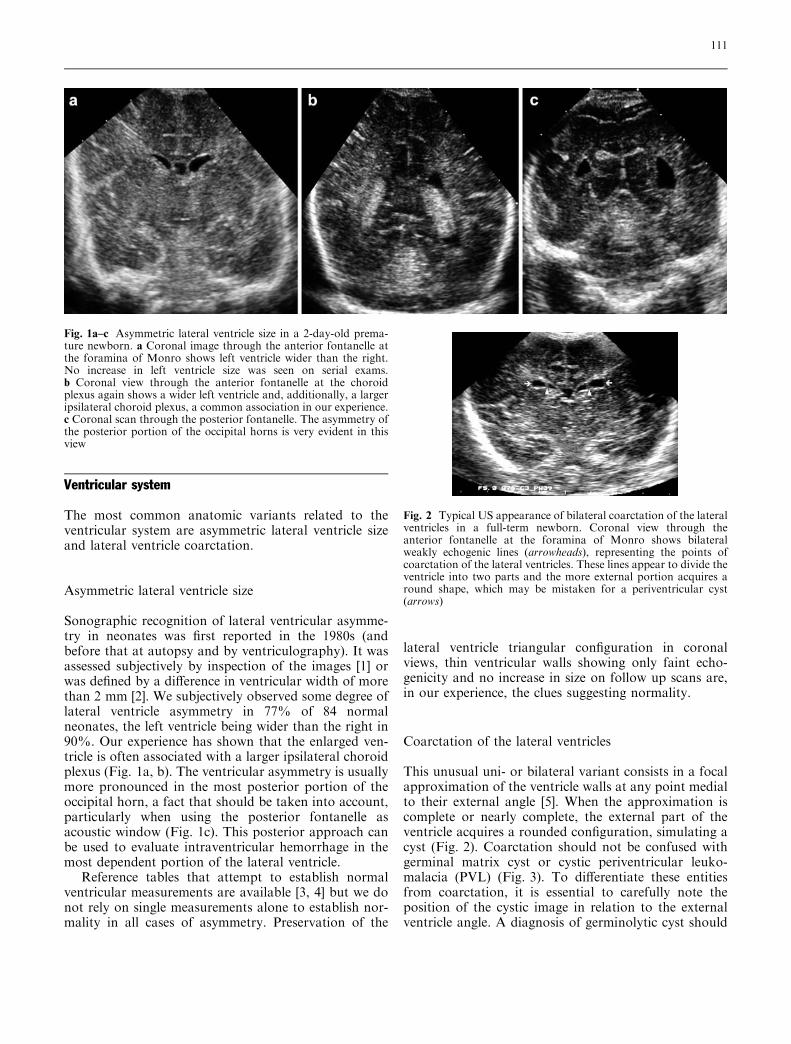
Fig. 2 Typical US appearance of bilateral coarctation of the lateralventricles in a full-term newborn. Coronal view through theanterior fontanelle at the foramina of Monro shows bilateralweakly echogenic lines (arrowheads), representing the points ofcoarctation of the lateral ventricles. These lines appear to divide theventricle into two parts and the more external portion acquires around shape, which may be mistaken for a periventricular cyst(arrows)
Fig. 1a–c Asymmetric lateral ventricle size in a 2-day-old prema-ture newborn. a Coronal image through the anterior fontanelle atthe foramina of Monro shows left ventricle wider than the right.No increase in left ventricle size was seen on serial exams.b Coronal view through the anterior fontanelle at the choroidplexus again shows a wider left ventricle and, additionally, a largeripsilateral choroid plexus, a common association in our experience.c Coronal scan through the posterior fontanelle. The asymmetry ofthe posterior portion of the occipital horns is very evident in thisview
111
be considered when the lesion is located below theexternal ventricle angle and PVL should be consideredwhen it is above [6]. In lateral ventricle coarctation, thefalse cystic image is seen at the external angle.
Choroid plexus
The US configuration of the choroid plexus has beenwell documented as a highly echogenic structure with asmooth, sharply defined outline. In the sagittal view itruns in a semicircular direction around the thalamus,and at the atrium it widens and thickens to form theglomus [7]. Although it has a clear, characteristic form,the choroid plexus can present certain configurationpatterns that may be misinterpreted as choroid pathol-ogy. The most common of these are ‘‘split’’ choroid,‘‘truncated’’ choroid, and choroid cyst.
Split choroid refers to the image of a cleft in theplexus, which can be complete, giving the appearanceof a cut or double choroidal pattern (Fig. 4a), or par-tial in the anteriormost portion, giving a lobular ap-pearance that can mimic choroid hemorrhage (Fig. 4b).Since the choroid plexus is a highly vascularizedstructure, color Doppler can help to differentiate thislatter normal anatomic variant from choroid hemor-rhage [8].
Truncated choroid plexus is the term we apply to aflattening of the usually rounded lower portion of the
plexus, giving the appearance of a solid-fluid level(Fig. 5). Our experience has shown that this finding,particularly common on the left side, is not necessarilyan indirect sign of intraventricular hemorrhage, as hasbeen previously considered. Scans through the posteriorfontanelle can rule out the presence of clots or freshblood within the ventricle.
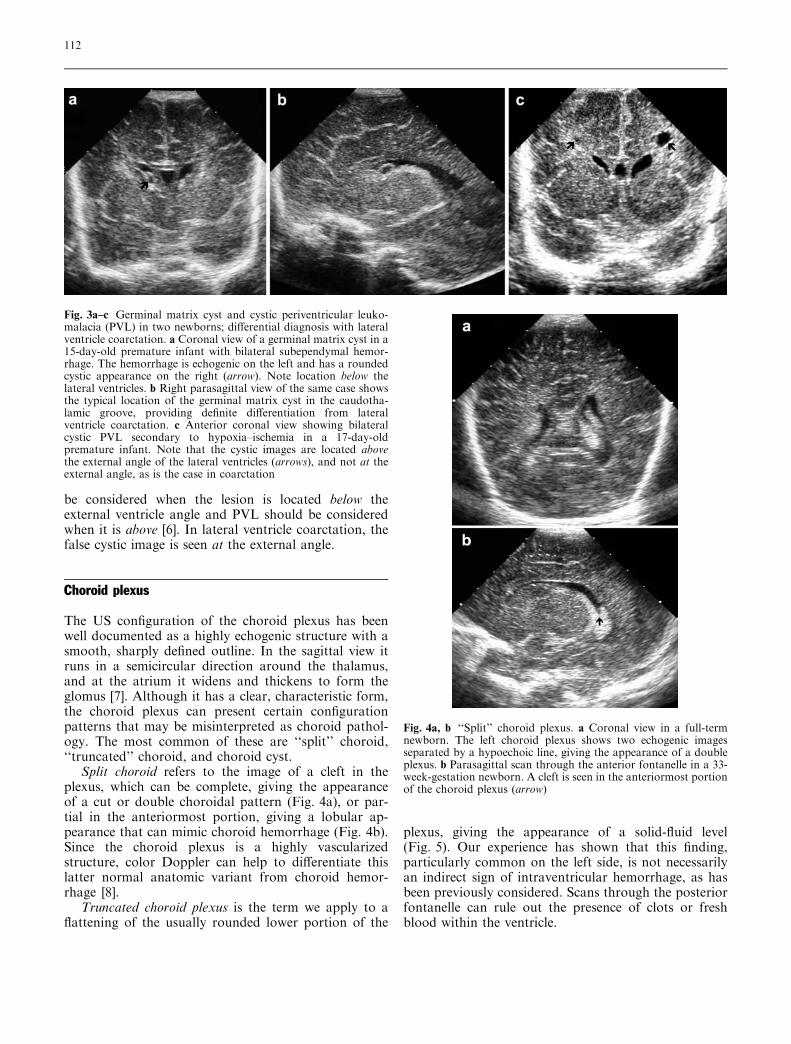
Fig. 3a–c Germinal matrix cyst and cystic periventricular leuko-malacia (PVL) in two newborns; differential diagnosis with lateralventricle coarctation. a Coronal view of a germinal matrix cyst in a15-day-old premature infant with bilateral subependymal hemor-rhage. The hemorrhage is echogenic on the left and has a roundedcystic appearance on the right (arrow). Note location below thelateral ventricles. b Right parasagittal view of the same case showsthe typical location of the germinal matrix cyst in the caudotha-lamic groove, providing definite differentiation from lateralventricle coarctation. c Anterior coronal view showing bilateralcystic PVL secondary to hypoxia–ischemia in a 17-day-oldpremature infant. Note that the cystic images are located abovethe external angle of the lateral ventricles (arrows), and not at theexternal angle, as is the case in coarctation
Fig. 4a, b ‘‘Split’’ choroid plexus. a Coronal view in a full-termnewborn. The left choroid plexus shows two echogenic imagesseparated by a hypoechoic line, giving the appearance of a doubleplexus. b Parasagittal scan through the anterior fontanelle in a 33-week-gestation newborn. A cleft is seen in the anteriormost portionof the choroid plexus (arrow)
112
Choroid cysts are visualized as rounded, well-defined, fluid-filled anechoic structures mainly locatedwithin the choroid plexus (Fig. 6). They may be singleor multiple and vary greatly in size. Choroid cyst, acommon finding in obstetric and postnatal US studies,usually disappears on serial examinations [9]. Thosethat are very large are often associated with chromos-omal abnormalities [10].
Brain parenchyma
In the brain parenchyma group we describe severalscanning artifacts (peritrigonal echogenicity, thalamicpseudolesion and pseudo-absence of the inferior vermis)
and normal parenchymal structures (occipital pseudo-mass and calcar avis) that can mimic brain pathology.
Peritrigonal echogenicity
Bilateral peritrigonal hyperechogenicity (‘‘blush’’ or‘‘halo’’) is a well-known sonographic finding in pretermand some full-term neonates caused by an anisotropiceffect of scanning [11]. In views through the anteriorfontanelle, the US beam strikes the nerve fibers andblood vessels of the superior and posterior trigonal re-gions almost perpendicularly, producing multiple sono-graphic interfaces seen as a relatively homogeneous,flame-shaped hyperechogenicity with poorly definedmargins in the peritrigonal area (Fig. 7a). In scansthrough the posterior fontanelle, the US beam is ori-ented more parallel to the fibers and the hyperechoge-nicity in this region is not so evident (Fig. 7b). Thisnormal US finding must be differentiated from abnor-mal peritrigonal hyperechogenicity caused by PVL. Inpatients with PVL, the hyperechogenicity is more bub-ble-like or heterogeneous, it persists in scans through theposterior fontanelle, and on follow-up studies cavitarycysts can often be seen (Fig. 8).
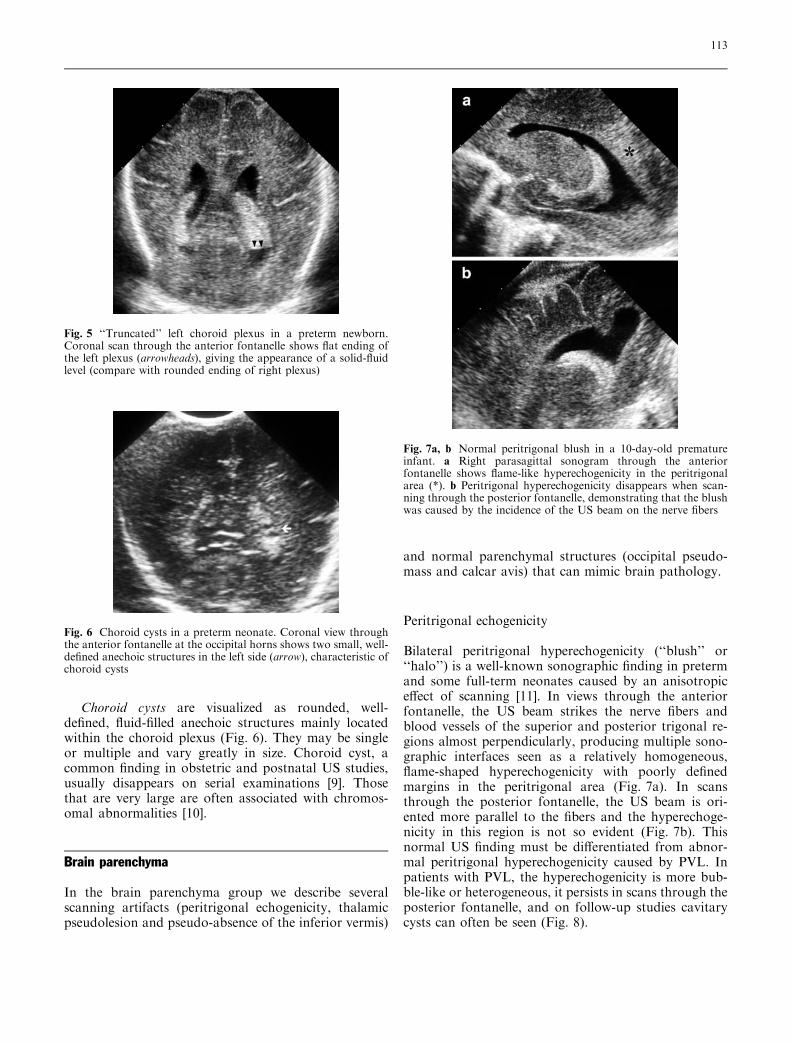
Fig. 5 ‘‘Truncated’’ left choroid plexus in a preterm newborn.Coronal scan through the anterior fontanelle shows flat ending ofthe left plexus (arrowheads), giving the appearance of a solid-fluidlevel (compare with rounded ending of right plexus)
Fig. 6 Choroid cysts in a preterm neonate. Coronal view throughthe anterior fontanelle at the occipital horns shows two small, well-defined anechoic structures in the left side (arrow), characteristic ofchoroid cysts
Fig. 7a, b Normal peritrigonal blush in a 10-day-old prematureinfant. a Right parasagittal sonogram through the anteriorfontanelle shows flame-like hyperechogenicity in the peritrigonalarea (*). b Peritrigonal hyperechogenicity disappears when scan-ning through the posterior fontanelle, demonstrating that the blushwas caused by the incidence of the US beam on the nerve fibers
113
Thalamic pseudolesion
The normal thalamus is composed of multiple parallelfibers (Fig. 9a) and on US study through the anteriorfontanelle it is seen as an almost uniform echogenicstructure (Fig. 4b). However, in parasagittal viewsthrough the posterior fontanelle, the US beam strikesthe thalamic fibers perpendicularly, sometimes produc-ing a rounded focal hyperechogenicity within the thal-amus (Fig. 9b). This anisotropic scanning artifact,known as thalamic pseudolesion, may be misinterpretedas a hemorrhagic or ischemic lesion [12]. The imagesproduced by true lesions persist in scans performedthrough the anterior fontanelle, whereas pseudolesionsdisappear.
Pseudo-absence of the inferior vermis
In some normal newborns, the vermis tilts slightly for-ward from its usual position, and on angled axial imagesthrough the mastoid fontanelle a wide communicationmay be visualized between the fourth ventricle and thecisterna magna, simulating inferior vermian agenesis[13]. This scanning artifact mainly depends on trans-
ducer angulation. By changing the tilt of the transducer,the normal inferior vermis can be properly identified(Fig. 10). This false image is also a common source ofdiagnostic error in fetal scanning performed after18 weeks of gestation, the time at which the vermis iscompletely closed.
Occipital pseudomass
The occipital lobe in patients under 34 weeks of ges-tation has a hypoechoic aspect due to poor gyraldevelopment that contrasts strongly with the encirclingwell-developed hyperechoic parieto-occipital fissureand tentorium, producing a mass-like effect (Fig. 11).
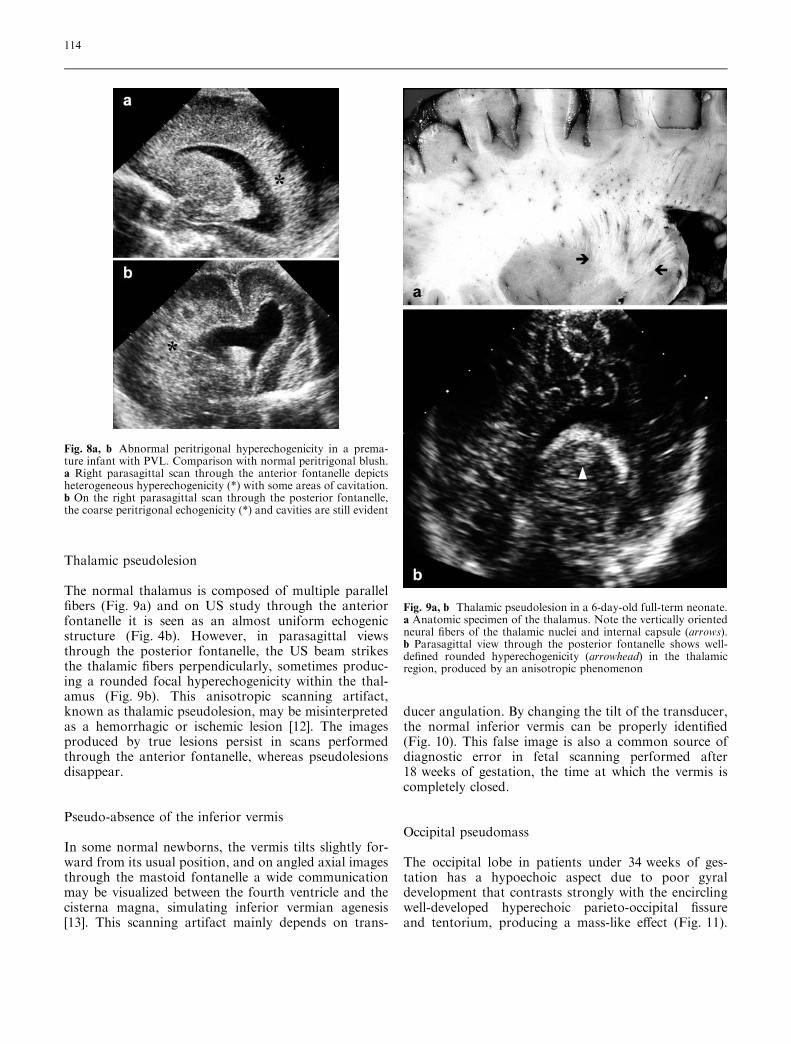
Fig. 8a, b Abnormal peritrigonal hyperechogenicity in a prema-ture infant with PVL. Comparison with normal peritrigonal blush.a Right parasagittal scan through the anterior fontanelle depictsheterogeneous hyperechogenicity (*) with some areas of cavitation.b On the right parasagittal scan through the posterior fontanelle,the coarse peritrigonal echogenicity (*) and cavities are still evident
Fig. 9a, b Thalamic pseudolesion in a 6-day-old full-term neonate.a Anatomic specimen of the thalamus. Note the vertically orientedneural fibers of the thalamic nuclei and internal capsule (arrows).b Parasagittal view through the posterior fontanelle shows well-defined rounded hyperechogenicity (arrowhead) in the thalamicregion, produced by an anisotropic phenomenon
114
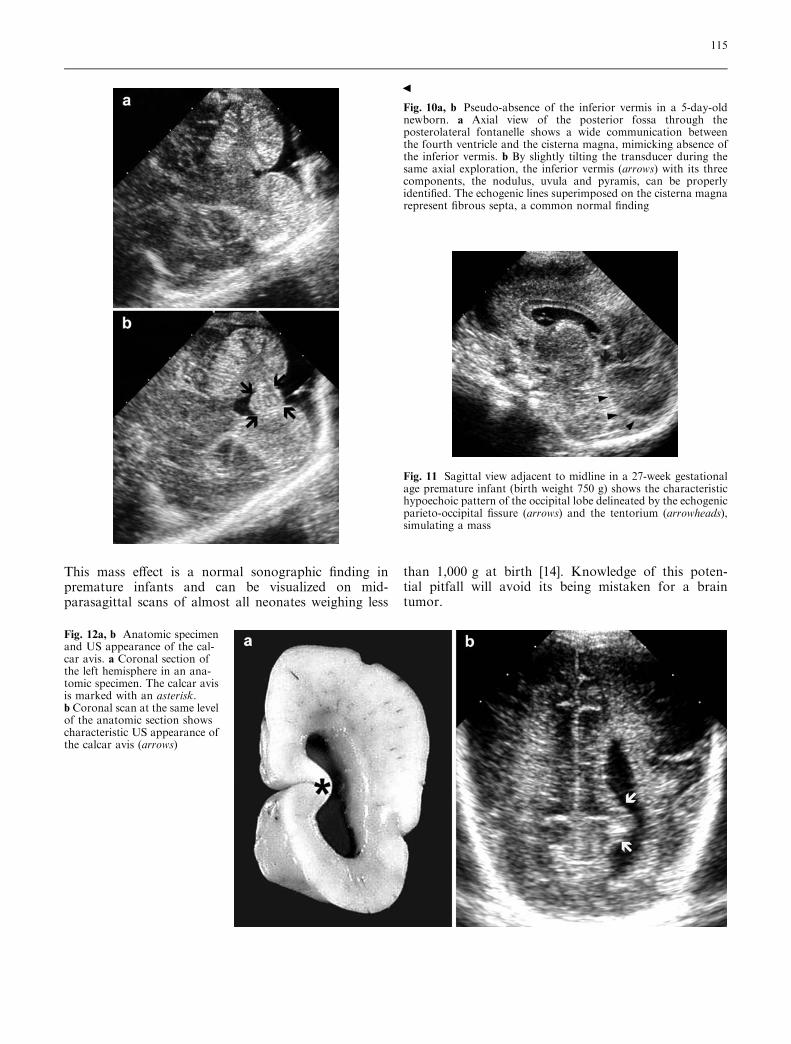
This mass effect is a normal sonographic finding inpremature infants and can be visualized on mid-parasagittal scans of almost all neonates weighing less
than 1,000 g at birth [14]. Knowledge of this poten-tial pitfall will avoid its being mistaken for a braintumor.
Fig. 11 Sagittal view adjacent to midline in a 27-week gestationalage premature infant (birth weight 750 g) shows the characteristichypoechoic pattern of the occipital lobe delineated by the echogenicparieto-occipital fissure (arrows) and the tentorium (arrowheads),simulating a mass
Fig. 12a, b Anatomic specimenand US appearance of the cal-car avis. a Coronal section ofthe left hemisphere in an ana-tomic specimen. The calcar avisis marked with an asterisk.b Coronal scan at the same levelof the anatomic section showscharacteristic US appearance ofthe calcar avis (arrows)
Fig. 10a, b Pseudo-absence of the inferior vermis in a 5-day-oldnewborn. a Axial view of the posterior fossa through theposterolateral fontanelle shows a wide communication betweenthe fourth ventricle and the cisterna magna, mimicking absence ofthe inferior vermis. b By slightly tilting the transducer during thesame axial exploration, the inferior vermis (arrows) with its threecomponents, the nodulus, uvula and pyramis, can be properlyidentified. The echogenic lines superimposed on the cisterna magnarepresent fibrous septa, a common normal finding
b
115
Calcar avis
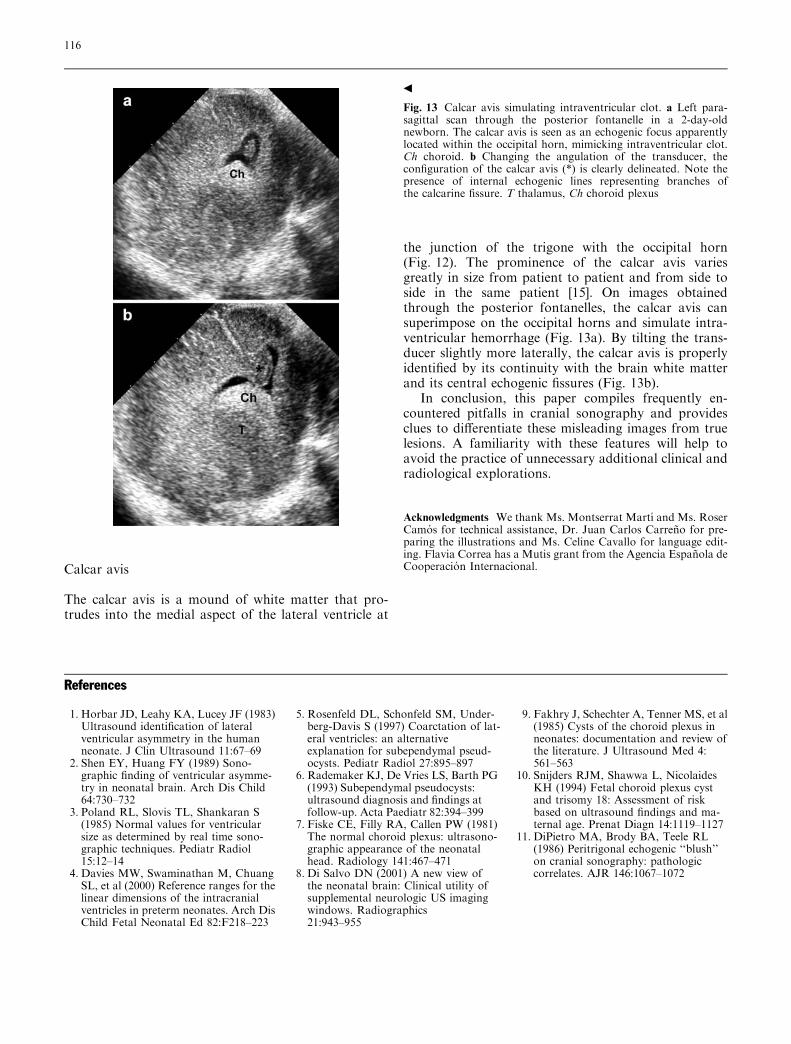
The calcar avis is a mound of white matter that pro-trudes into the medial aspect of the lateral ventricle at
the junction of the trigone with the occipital horn(Fig. 12). The prominence of the calcar avis variesgreatly in size from patient to patient and from side toside in the same patient [15]. On images obtainedthrough the posterior fontanelles, the calcar avis cansuperimpose on the occipital horns and simulate intra-ventricular hemorrhage (Fig. 13a). By tilting the trans-ducer slightly more laterally, the calcar avis is properlyidentified by its continuity with the brain white matterand its central echogenic fissures (Fig. 13b).
In conclusion, this paper compiles frequently en-countered pitfalls in cranial sonography and providesclues to differentiate these misleading images from truelesions. A familiarity with these features will help toavoid the practice of unnecessary additional clinical andradiological explorations.
Acknowledgments We thank Ms. Montserrat Martı and Ms. RoserCamos for technical assistance, Dr. Juan Carlos Carreno for pre-paring the illustrations and Ms. Celine Cavallo for language edit-ing. Flavia Correa has a Mutis grant from the Agencia Espanola deCooperacion Internacional.
References
1. Horbar JD, Leahy KA, Lucey JF (1983)Ultrasound identification of lateralventricular asymmetry in the humanneonate. J Clin Ultrasound 11:67–69
2. Shen EY, Huang FY (1989) Sono-graphic finding of ventricular asymme-try in neonatal brain. Arch Dis Child64:730–732
3. Poland RL, Slovis TL, Shankaran S(1985) Normal values for ventricularsize as determined by real time sono-graphic techniques. Pediatr Radiol15:12–14
4. Davies MW, Swaminathan M, ChuangSL, et al (2000) Reference ranges for thelinear dimensions of the intracranialventricles in preterm neonates. Arch DisChild Fetal Neonatal Ed 82:F218–223
5. Rosenfeld DL, Schonfeld SM, Under-berg-Davis S (1997) Coarctation of lat-eral ventricles: an alternativeexplanation for subependymal pseud-ocysts. Pediatr Radiol 27:895–897
6. Rademaker KJ, De Vries LS, Barth PG(1993) Subependymal pseudocysts:ultrasound diagnosis and findings atfollow-up. Acta Paediatr 82:394–399
7. Fiske CE, Filly RA, Callen PW (1981)The normal choroid plexus: ultrasono-graphic appearance of the neonatalhead. Radiology 141:467–471
8. Di Salvo DN (2001) A new view ofthe neonatal brain: Clinical utility ofsupplemental neurologic US imagingwindows. Radiographics21:943–955
9. Fakhry J, Schechter A, Tenner MS, et al(1985) Cysts of the choroid plexus inneonates: documentation and review ofthe literature. J Ultrasound Med 4:561–563
10. Snijders RJM, Shawwa L, NicolaidesKH (1994) Fetal choroid plexus cystand trisomy 18: Assessment of riskbased on ultrasound findings and ma-ternal age. Prenat Diagn 14:1119–1127
11. DiPietro MA, Brody BA, Teele RL(1986) Peritrigonal echogenic ‘‘blush’’on cranial sonography: pathologiccorrelates. AJR 146:1067–1072
Fig. 13 Calcar avis simulating intraventricular clot. a Left para-sagittal scan through the posterior fontanelle in a 2-day-oldnewborn. The calcar avis is seen as an echogenic focus apparentlylocated within the occipital horn, mimicking intraventricular clot.Ch choroid. b Changing the angulation of the transducer, theconfiguration of the calcar avis (*) is clearly delineated. Note thepresence of internal echogenic lines representing branches ofthe calcarine fissure. T thalamus, Ch choroid plexus
b
116

12. Schlesinger AE, Munden MM, HaymanLA (1999) Hyperechoic foci in the tha-lamic region imaged via the posteriorfontanelle: a potential mimic of tha-lamic pathology. Pediatr Radiol 29:520–523
13. Luna JA, Goldstein RB (2000) Sono-graphic visualization of neonatal poste-rior fossa abnormalities through theposterolateral fontanelle. AJR 174:561–567
14. Vade A, Otto R (1986) Cranial sonog-raphy of the occipital horns and gyralpatterns in the occipital lobes. AJNR7:873–877
15. DiPietro MA, Brody BA, Teele RL(1985) The calcar avis: demonstrationwith cranial US. Radiology 156:363–364
117
















![[Sonography of synovial and erosive inflammatory changes]](https://img.pdfslide.net/doc/110x75/6356be6d5108319c870372a1/sonography-of-synovial-and-erosive-inflammatory-changes.jpg)
![[Diagnostic pitfalls with Cushing's syndrome]](https://img.pdfslide.net/doc/110x75/634c738d7f5a138881007d0f/diagnostic-pitfalls-with-cushings-syndrome.jpg)











