Embed Size (px)
Citation preview

Akut amp Kronisk Kompartment
Akut amp Kronisk Kompartment
bull Anatomi (Kort gennemgang)
bull Akut Kompartment
bull Kronisk Kompartment (gennemgang)
bull PAES (meget KORT gennemgang)
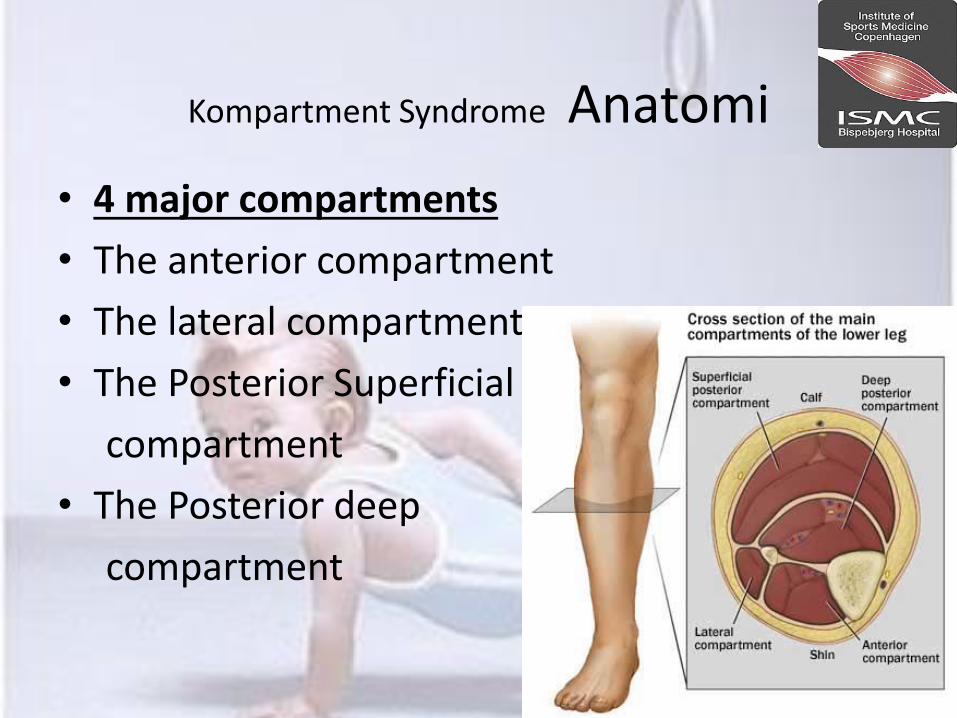
Kompartment Syndrome Anatomi bull 4 major compartments
bull The anterior compartment
bull The lateral compartment
bull The Posterior Superficial
compartment
bull The Posterior deep
compartment
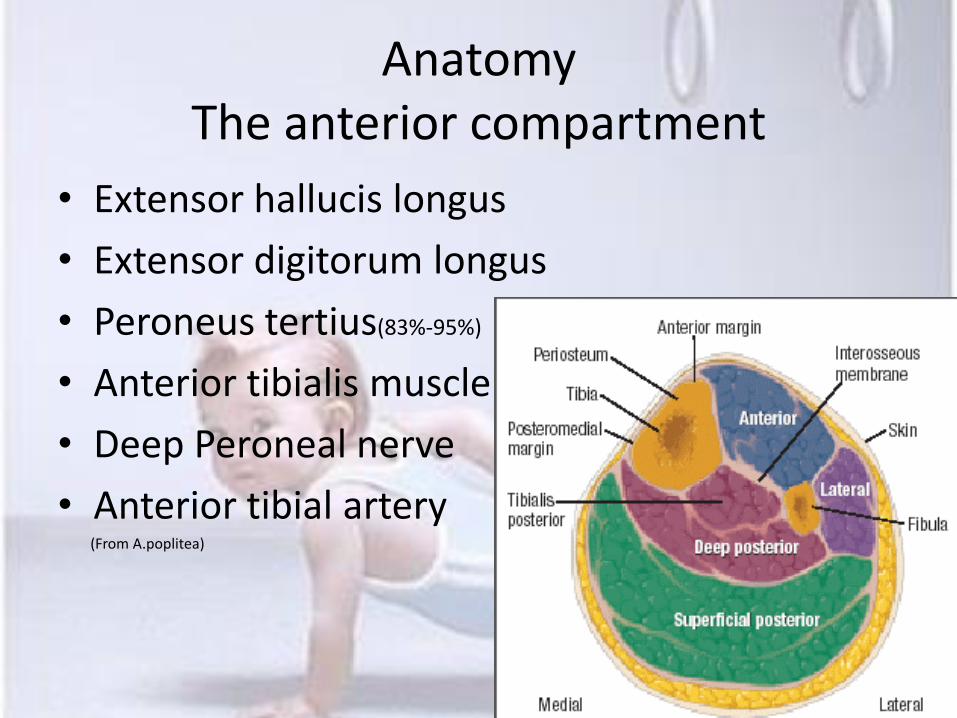
Anatomy The anterior compartment
bull Extensor hallucis longus
bull Extensor digitorum longus
bull Peroneus tertius(83-95)
bull Anterior tibialis muscle
bull Deep Peroneal nerve
bull Anterior tibial artery (From Apoplitea)
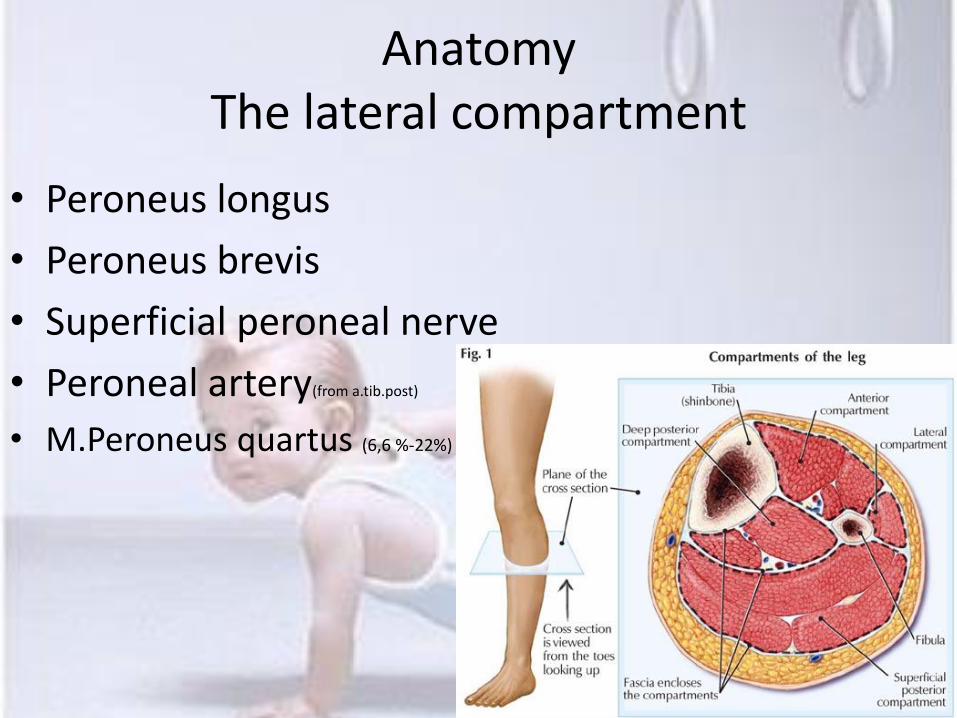
Anatomy The lateral compartment
bull Peroneus longus
bull Peroneus brevis
bull Superficial peroneal nerve
bull Peroneal artery(from atibpost)
bull MPeroneus quartus (66 -22)
Anatomy The Posterior Superficial compartment
bull Gastrocnemicus
bull Soleus
bull rdquoplantaris musclerdquo (90-93)
bull rdquoAccesory soleus musclerdquo(07-56)
bull rdquoThird head of gastrocnemicusrdquo bull (29-55)
bull Sural nerve
Anatomy The Posterior deep compartment
bull Flexor hallucis longus bull Flexor digitorum longus bull Flexor digitorum acces- bull sorius longus (2-8)
bull Posterior tibialis muscle bull Popliteus muscle (other post superf)
bull Popliteus accessorius muscle (rare)
bull Tibial nerve bull posteriorTibial artery and vein (from apoplitea)
bull Posterior tibial muscle bull (own compartment Wilder RP(2004) + Albertson K (2001))
Akut Kompartment
bull Akut behandlingskraeligvende tilstand
bull Opstaringr ofte efter stoslashrre traumer og frakturer men kan forekomme ved mindre traumer
bull Feks Slag mod laeliggmuskel (kontaktsport)
Akut Komptartment
bull Symptomer
bull Smerter
bull Smerter relateret til bevaeliggelse (flex eversion osv)
bull Sensibilitetsforstyrrelser
bull Kraft nedsaeligttelse
bull Forvaeligrres (akut) over tid trods aflastning (tiltagende)
Akut Kompartment
Sneppen 6udg
Anterioere kompartment Deep Peroneal nerve
Laterale kompartment Superficial peroneal nerve
Dybe bagerste kompartment Tibial nerve
Akut Kompartment
bull Diagnose
bull Klinik
bull Trykmaringling (30 mm Hg)
bull Der forsoslashges med
UL MR Skintigrafi blod-
Proslashver Infraroslashd mfl bull (Can J Surg 2010 October 53(5) 329ndash334)
Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut

Akut amp Kronisk Kompartment
bull Anatomi (Kort gennemgang)
bull Akut Kompartment
bull Kronisk Kompartment (gennemgang)
bull PAES (meget KORT gennemgang)
Kompartment Syndrome Anatomi bull 4 major compartments
bull The anterior compartment
bull The lateral compartment
bull The Posterior Superficial
compartment
bull The Posterior deep
compartment
Anatomy The anterior compartment
bull Extensor hallucis longus
bull Extensor digitorum longus
bull Peroneus tertius(83-95)
bull Anterior tibialis muscle
bull Deep Peroneal nerve
bull Anterior tibial artery (From Apoplitea)
Anatomy The lateral compartment
bull Peroneus longus
bull Peroneus brevis
bull Superficial peroneal nerve
bull Peroneal artery(from atibpost)
bull MPeroneus quartus (66 -22)
Anatomy The Posterior Superficial compartment
bull Gastrocnemicus
bull Soleus
bull rdquoplantaris musclerdquo (90-93)
bull rdquoAccesory soleus musclerdquo(07-56)
bull rdquoThird head of gastrocnemicusrdquo bull (29-55)
bull Sural nerve
Anatomy The Posterior deep compartment
bull Flexor hallucis longus bull Flexor digitorum longus bull Flexor digitorum acces- bull sorius longus (2-8)
bull Posterior tibialis muscle bull Popliteus muscle (other post superf)
bull Popliteus accessorius muscle (rare)
bull Tibial nerve bull posteriorTibial artery and vein (from apoplitea)
bull Posterior tibial muscle bull (own compartment Wilder RP(2004) + Albertson K (2001))
Akut Kompartment
bull Akut behandlingskraeligvende tilstand
bull Opstaringr ofte efter stoslashrre traumer og frakturer men kan forekomme ved mindre traumer
bull Feks Slag mod laeliggmuskel (kontaktsport)
Akut Komptartment
bull Symptomer
bull Smerter
bull Smerter relateret til bevaeliggelse (flex eversion osv)
bull Sensibilitetsforstyrrelser
bull Kraft nedsaeligttelse
bull Forvaeligrres (akut) over tid trods aflastning (tiltagende)
Akut Kompartment
Sneppen 6udg
Anterioere kompartment Deep Peroneal nerve
Laterale kompartment Superficial peroneal nerve
Dybe bagerste kompartment Tibial nerve
Akut Kompartment
bull Diagnose
bull Klinik
bull Trykmaringling (30 mm Hg)
bull Der forsoslashges med
UL MR Skintigrafi blod-
Proslashver Infraroslashd mfl bull (Can J Surg 2010 October 53(5) 329ndash334)
Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Kompartment Syndrome Anatomi bull 4 major compartments
bull The anterior compartment
bull The lateral compartment
bull The Posterior Superficial
compartment
bull The Posterior deep
compartment
Anatomy The anterior compartment
bull Extensor hallucis longus
bull Extensor digitorum longus
bull Peroneus tertius(83-95)
bull Anterior tibialis muscle
bull Deep Peroneal nerve
bull Anterior tibial artery (From Apoplitea)
Anatomy The lateral compartment
bull Peroneus longus
bull Peroneus brevis
bull Superficial peroneal nerve
bull Peroneal artery(from atibpost)
bull MPeroneus quartus (66 -22)
Anatomy The Posterior Superficial compartment
bull Gastrocnemicus
bull Soleus
bull rdquoplantaris musclerdquo (90-93)
bull rdquoAccesory soleus musclerdquo(07-56)
bull rdquoThird head of gastrocnemicusrdquo bull (29-55)
bull Sural nerve
Anatomy The Posterior deep compartment
bull Flexor hallucis longus bull Flexor digitorum longus bull Flexor digitorum acces- bull sorius longus (2-8)
bull Posterior tibialis muscle bull Popliteus muscle (other post superf)
bull Popliteus accessorius muscle (rare)
bull Tibial nerve bull posteriorTibial artery and vein (from apoplitea)
bull Posterior tibial muscle bull (own compartment Wilder RP(2004) + Albertson K (2001))
Akut Kompartment
bull Akut behandlingskraeligvende tilstand
bull Opstaringr ofte efter stoslashrre traumer og frakturer men kan forekomme ved mindre traumer
bull Feks Slag mod laeliggmuskel (kontaktsport)
Akut Komptartment
bull Symptomer
bull Smerter
bull Smerter relateret til bevaeliggelse (flex eversion osv)
bull Sensibilitetsforstyrrelser
bull Kraft nedsaeligttelse
bull Forvaeligrres (akut) over tid trods aflastning (tiltagende)
Akut Kompartment
Sneppen 6udg
Anterioere kompartment Deep Peroneal nerve
Laterale kompartment Superficial peroneal nerve
Dybe bagerste kompartment Tibial nerve
Akut Kompartment
bull Diagnose
bull Klinik
bull Trykmaringling (30 mm Hg)
bull Der forsoslashges med
UL MR Skintigrafi blod-
Proslashver Infraroslashd mfl bull (Can J Surg 2010 October 53(5) 329ndash334)
Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Anatomy The anterior compartment
bull Extensor hallucis longus
bull Extensor digitorum longus
bull Peroneus tertius(83-95)
bull Anterior tibialis muscle
bull Deep Peroneal nerve
bull Anterior tibial artery (From Apoplitea)
Anatomy The lateral compartment
bull Peroneus longus
bull Peroneus brevis
bull Superficial peroneal nerve
bull Peroneal artery(from atibpost)
bull MPeroneus quartus (66 -22)
Anatomy The Posterior Superficial compartment
bull Gastrocnemicus
bull Soleus
bull rdquoplantaris musclerdquo (90-93)
bull rdquoAccesory soleus musclerdquo(07-56)
bull rdquoThird head of gastrocnemicusrdquo bull (29-55)
bull Sural nerve
Anatomy The Posterior deep compartment
bull Flexor hallucis longus bull Flexor digitorum longus bull Flexor digitorum acces- bull sorius longus (2-8)
bull Posterior tibialis muscle bull Popliteus muscle (other post superf)
bull Popliteus accessorius muscle (rare)
bull Tibial nerve bull posteriorTibial artery and vein (from apoplitea)
bull Posterior tibial muscle bull (own compartment Wilder RP(2004) + Albertson K (2001))
Akut Kompartment
bull Akut behandlingskraeligvende tilstand
bull Opstaringr ofte efter stoslashrre traumer og frakturer men kan forekomme ved mindre traumer
bull Feks Slag mod laeliggmuskel (kontaktsport)
Akut Komptartment
bull Symptomer
bull Smerter
bull Smerter relateret til bevaeliggelse (flex eversion osv)
bull Sensibilitetsforstyrrelser
bull Kraft nedsaeligttelse
bull Forvaeligrres (akut) over tid trods aflastning (tiltagende)
Akut Kompartment
Sneppen 6udg
Anterioere kompartment Deep Peroneal nerve
Laterale kompartment Superficial peroneal nerve
Dybe bagerste kompartment Tibial nerve
Akut Kompartment
bull Diagnose
bull Klinik
bull Trykmaringling (30 mm Hg)
bull Der forsoslashges med
UL MR Skintigrafi blod-
Proslashver Infraroslashd mfl bull (Can J Surg 2010 October 53(5) 329ndash334)
Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Anatomy The lateral compartment
bull Peroneus longus
bull Peroneus brevis
bull Superficial peroneal nerve
bull Peroneal artery(from atibpost)
bull MPeroneus quartus (66 -22)
Anatomy The Posterior Superficial compartment
bull Gastrocnemicus
bull Soleus
bull rdquoplantaris musclerdquo (90-93)
bull rdquoAccesory soleus musclerdquo(07-56)
bull rdquoThird head of gastrocnemicusrdquo bull (29-55)
bull Sural nerve
Anatomy The Posterior deep compartment
bull Flexor hallucis longus bull Flexor digitorum longus bull Flexor digitorum acces- bull sorius longus (2-8)
bull Posterior tibialis muscle bull Popliteus muscle (other post superf)
bull Popliteus accessorius muscle (rare)
bull Tibial nerve bull posteriorTibial artery and vein (from apoplitea)
bull Posterior tibial muscle bull (own compartment Wilder RP(2004) + Albertson K (2001))
Akut Kompartment
bull Akut behandlingskraeligvende tilstand
bull Opstaringr ofte efter stoslashrre traumer og frakturer men kan forekomme ved mindre traumer
bull Feks Slag mod laeliggmuskel (kontaktsport)
Akut Komptartment
bull Symptomer
bull Smerter
bull Smerter relateret til bevaeliggelse (flex eversion osv)
bull Sensibilitetsforstyrrelser
bull Kraft nedsaeligttelse
bull Forvaeligrres (akut) over tid trods aflastning (tiltagende)
Akut Kompartment
Sneppen 6udg
Anterioere kompartment Deep Peroneal nerve
Laterale kompartment Superficial peroneal nerve
Dybe bagerste kompartment Tibial nerve
Akut Kompartment
bull Diagnose
bull Klinik
bull Trykmaringling (30 mm Hg)
bull Der forsoslashges med
UL MR Skintigrafi blod-
Proslashver Infraroslashd mfl bull (Can J Surg 2010 October 53(5) 329ndash334)
Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
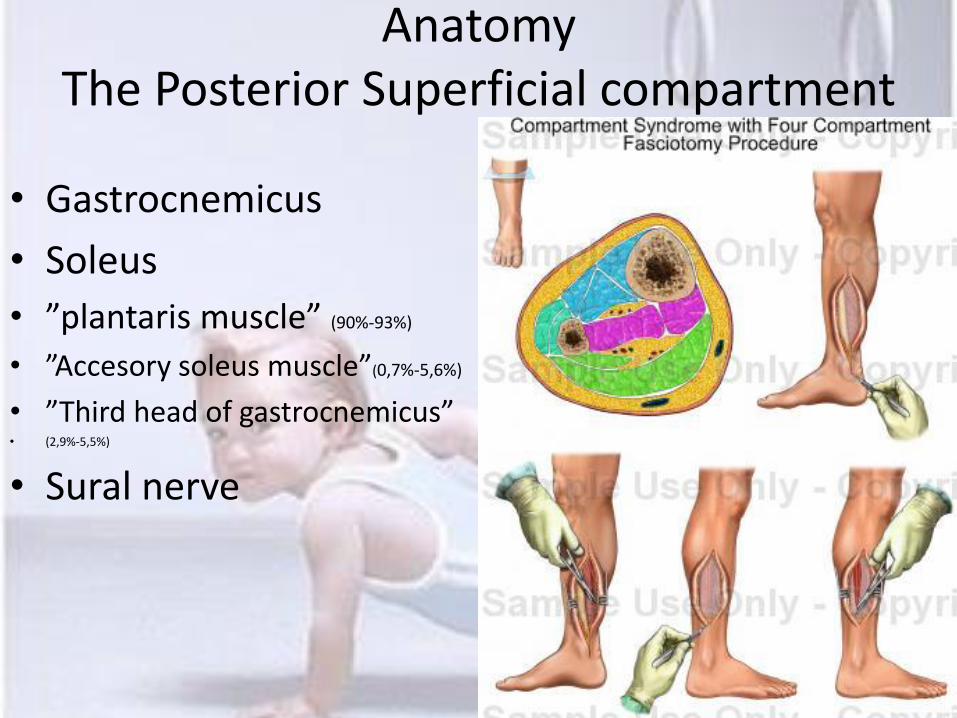
Anatomy The Posterior Superficial compartment
bull Gastrocnemicus
bull Soleus
bull rdquoplantaris musclerdquo (90-93)
bull rdquoAccesory soleus musclerdquo(07-56)
bull rdquoThird head of gastrocnemicusrdquo bull (29-55)
bull Sural nerve
Anatomy The Posterior deep compartment
bull Flexor hallucis longus bull Flexor digitorum longus bull Flexor digitorum acces- bull sorius longus (2-8)
bull Posterior tibialis muscle bull Popliteus muscle (other post superf)
bull Popliteus accessorius muscle (rare)
bull Tibial nerve bull posteriorTibial artery and vein (from apoplitea)
bull Posterior tibial muscle bull (own compartment Wilder RP(2004) + Albertson K (2001))
Akut Kompartment
bull Akut behandlingskraeligvende tilstand
bull Opstaringr ofte efter stoslashrre traumer og frakturer men kan forekomme ved mindre traumer
bull Feks Slag mod laeliggmuskel (kontaktsport)
Akut Komptartment
bull Symptomer
bull Smerter
bull Smerter relateret til bevaeliggelse (flex eversion osv)
bull Sensibilitetsforstyrrelser
bull Kraft nedsaeligttelse
bull Forvaeligrres (akut) over tid trods aflastning (tiltagende)
Akut Kompartment
Sneppen 6udg
Anterioere kompartment Deep Peroneal nerve
Laterale kompartment Superficial peroneal nerve
Dybe bagerste kompartment Tibial nerve
Akut Kompartment
bull Diagnose
bull Klinik
bull Trykmaringling (30 mm Hg)
bull Der forsoslashges med
UL MR Skintigrafi blod-
Proslashver Infraroslashd mfl bull (Can J Surg 2010 October 53(5) 329ndash334)
Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
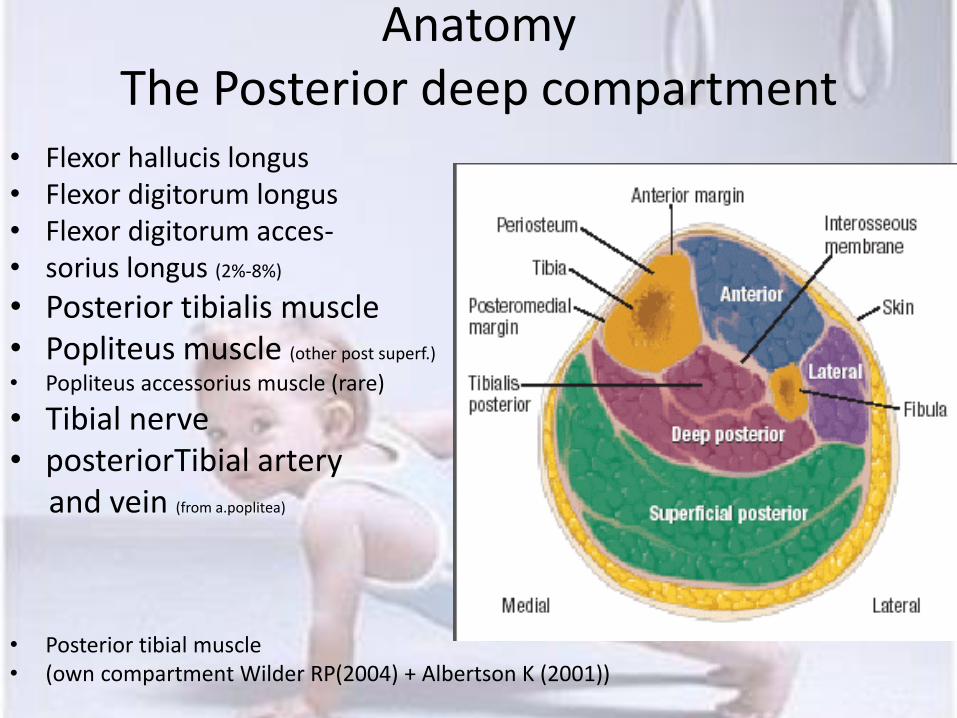
Anatomy The Posterior deep compartment
bull Flexor hallucis longus bull Flexor digitorum longus bull Flexor digitorum acces- bull sorius longus (2-8)
bull Posterior tibialis muscle bull Popliteus muscle (other post superf)
bull Popliteus accessorius muscle (rare)
bull Tibial nerve bull posteriorTibial artery and vein (from apoplitea)
bull Posterior tibial muscle bull (own compartment Wilder RP(2004) + Albertson K (2001))
Akut Kompartment
bull Akut behandlingskraeligvende tilstand
bull Opstaringr ofte efter stoslashrre traumer og frakturer men kan forekomme ved mindre traumer
bull Feks Slag mod laeliggmuskel (kontaktsport)
Akut Komptartment
bull Symptomer
bull Smerter
bull Smerter relateret til bevaeliggelse (flex eversion osv)
bull Sensibilitetsforstyrrelser
bull Kraft nedsaeligttelse
bull Forvaeligrres (akut) over tid trods aflastning (tiltagende)
Akut Kompartment
Sneppen 6udg
Anterioere kompartment Deep Peroneal nerve
Laterale kompartment Superficial peroneal nerve
Dybe bagerste kompartment Tibial nerve
Akut Kompartment
bull Diagnose
bull Klinik
bull Trykmaringling (30 mm Hg)
bull Der forsoslashges med
UL MR Skintigrafi blod-
Proslashver Infraroslashd mfl bull (Can J Surg 2010 October 53(5) 329ndash334)
Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut

Akut Kompartment
bull Akut behandlingskraeligvende tilstand
bull Opstaringr ofte efter stoslashrre traumer og frakturer men kan forekomme ved mindre traumer
bull Feks Slag mod laeliggmuskel (kontaktsport)
Akut Komptartment
bull Symptomer
bull Smerter
bull Smerter relateret til bevaeliggelse (flex eversion osv)
bull Sensibilitetsforstyrrelser
bull Kraft nedsaeligttelse
bull Forvaeligrres (akut) over tid trods aflastning (tiltagende)
Akut Kompartment
Sneppen 6udg
Anterioere kompartment Deep Peroneal nerve
Laterale kompartment Superficial peroneal nerve
Dybe bagerste kompartment Tibial nerve
Akut Kompartment
bull Diagnose
bull Klinik
bull Trykmaringling (30 mm Hg)
bull Der forsoslashges med
UL MR Skintigrafi blod-
Proslashver Infraroslashd mfl bull (Can J Surg 2010 October 53(5) 329ndash334)
Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut

Akut Komptartment
bull Symptomer
bull Smerter
bull Smerter relateret til bevaeliggelse (flex eversion osv)
bull Sensibilitetsforstyrrelser
bull Kraft nedsaeligttelse
bull Forvaeligrres (akut) over tid trods aflastning (tiltagende)
Akut Kompartment
Sneppen 6udg
Anterioere kompartment Deep Peroneal nerve
Laterale kompartment Superficial peroneal nerve
Dybe bagerste kompartment Tibial nerve
Akut Kompartment
bull Diagnose
bull Klinik
bull Trykmaringling (30 mm Hg)
bull Der forsoslashges med
UL MR Skintigrafi blod-
Proslashver Infraroslashd mfl bull (Can J Surg 2010 October 53(5) 329ndash334)
Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
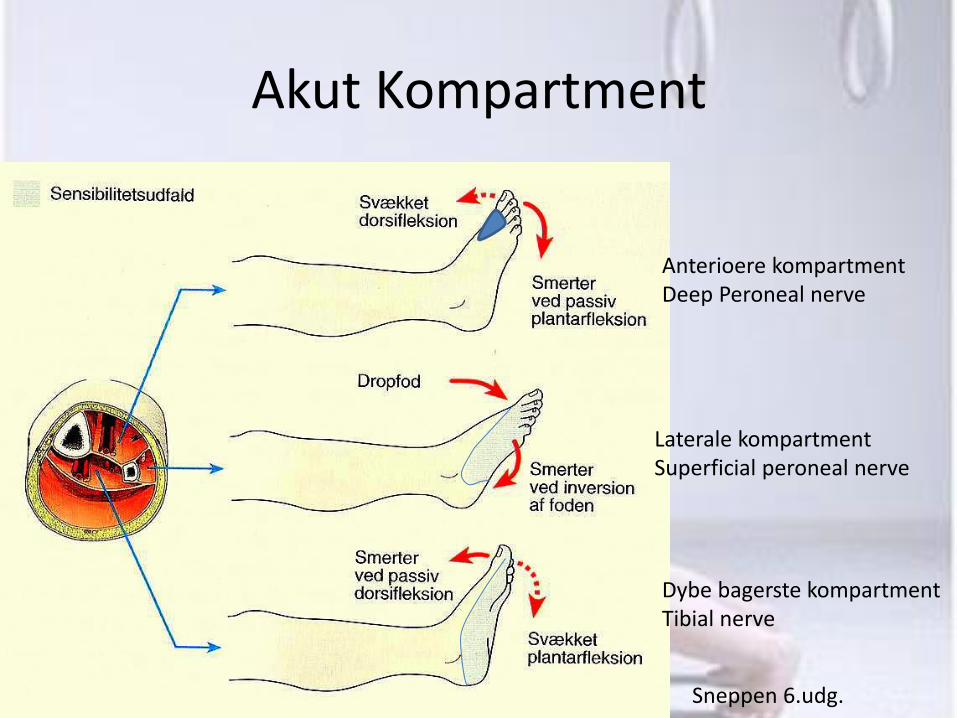
Akut Kompartment
Sneppen 6udg
Anterioere kompartment Deep Peroneal nerve
Laterale kompartment Superficial peroneal nerve
Dybe bagerste kompartment Tibial nerve
Akut Kompartment
bull Diagnose
bull Klinik
bull Trykmaringling (30 mm Hg)
bull Der forsoslashges med
UL MR Skintigrafi blod-
Proslashver Infraroslashd mfl bull (Can J Surg 2010 October 53(5) 329ndash334)
Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut

Akut Kompartment
bull Diagnose
bull Klinik
bull Trykmaringling (30 mm Hg)
bull Der forsoslashges med
UL MR Skintigrafi blod-
Proslashver Infraroslashd mfl bull (Can J Surg 2010 October 53(5) 329ndash334)
Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut

Akut Kompartment
bull Differential diagnoser
bull DVT
bull Muskelforstraeligkningbloslashdning
bull Arteriel okklusion (husk at akut kompartment hyppigst har bevaret pulse)
bull Nekrotiserende Fasciitis (Mortalitet paring 73)
(feber)(nekrotisk vaeligv)(feks GrA strep) (streptokokbetinget toksisk shock syndromSTSS)(80 ekstremiteter)
Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut

Akut Kompartment
bull Behandling
bull Diuretika steroid NSAID
bull Fasciotomi (dekompression)
NB HUSK information omkring kronisk kompartment og billeder paring nettet
Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut

Kronisk Kompartment Syndrom
bull = Chronic Exertional Compartment Syndrome (CECS)
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Historical
bull 1912 Edward Wilson described as the first the sympotoms of Compartment (acute) during an antarctic expedition
bull 1956 Mavor first cases of CECS (Mavor GE J Bone Joint
surg Br 1956 38B513-17)
bull 1962 French and Price first to correlate history and symptomps with raised intracompartmental pressure (French EB Price WH
Anterior tibial pain BMJ 1962ii1290-96) (Needle manometer technique)
aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut

aetiology
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Aetiology
bull Leading theorys bull Muscle hypertrophy bull Metabolic derangement bull Decreased fascial compliance
bull Muscle hypertrophy (Detmer DE) bull increased osmotic pressure under activity (Edwards P)(more theory than proven)
bull Ingen forskel paring tykkelse eller stivhed (CECS DM kontrol) bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub
2011 Sep 24
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Aetiology
bull Pain Pressure Ischaemia
bull Muscle volume can increase up to 20 during exercise and increased muscle volume causes an increase in the internal pressure (Shah S 2004)
bull No studies has shown that increased pressure leads to ischaemia
bull Using SPECT scanning it has been shown that increased intracompartmental pressure didnacutet lead to decreased perfusion in the muscle (Trease L 2001)
bull To low oxygen Stretch of the fascia Pressure on nervefibers
Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut

Symptoms
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Symptoms CECS
bull Prevalence of CECS
bull Anterior compartment 45
bull Deep posterior compartment 40
bull Lateral compartment 10
bull Superficial posterior compartment 5 bull Edwards P
CECS account for 27-33 of athletes with chronic leg pain (Clanton TO amp Styf J) MTSS number one
MTSS CECS and Stress fractures are the most common causes of exertional leg pain
(Edwards PH 2005)
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Symptoms CECS
bull Anterior Compartment (45 )
bull Cramping Burning Pain with exercise(all comparments) bull Examination at rest is normal (all compartments)
bull Paresthesias at the dorsum of the foot bull Weakness of dorsiflexion bull Weakness of toe extension bull Foot drop
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Symptoms
bull Deep posterior compartment (40 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Parasthesias in the plantar aspect of the foot bull Weakness of toe flexion bull Weakness of foot inversion
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Symptoms
bull Lateral compartment (10 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Sensory changes anterolateral aspect of the foot
bull Weakness of ankle eversion
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Symptoms
bull Superficial posterior compartment (5 )
bull Cramping Burning Pain with exercise (all comparments)
bull Examination at rest is normal (all compartments)
bull Dorsolateral hypoesthesia of the foot
bull Plantar flexion weakness
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Symptomer
bull Det altafgoslashrende for at man faringr mistanken til CECS er tidsforloslashbet
bull Der er en graelignse hvor spaeligndingensmerten kommer og hvis patienten holder pause svinderfalder symptomerne heltvaeligsentsligt Hvis de starter igen gentager moslashnstret sig
bull IKKE mange sygdomme udviser dette bratte fald i smerte score (VAS 8-10 til 0-3)
bull PAES Claudication (vaskulaeligr) Claudication (neurogen)
bull Stoslashttes yderligere af en NORMAL objektiv undersoslashgelse (i hvile)
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Diagnosis
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Diagnosis
bull Manually detection of compartment (manual palpation)
bull Sensitivity 24
bull Specificity 55 bull (Franklin D 2010)
bull Sensitivity of clinical findings (pain pain with passive stretch paresthesia and paresis) is
bull 13-19 (Ulmer T 2002)
bull rdquoPassive stretching of the calf musculature increases the pain when pressurees are elevated and is a key diagnostic findingrdquo(Pedowitz RA 2001)
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Diagnosis
bull Invasive
bull Needle manometer
bull Wick catheter
bull Slit catheter continous infusion
bull Solid-state transducer intracompartmental catheter
bull Non-invasive
bull MRi (more sensitive post exercise) increased T2-weighted signal But not specific (Brown R 2001) (edema presumed shift in extra and intracellular water)
bull thallium-201 single-photon emission tomography (SPECT) imaging= 201Tl SPET
bull radiopharmaceutical known as methoxy isobutyl isonitrile (combined with MRI) (muscle ischemia leads to less uptake of Technetium-99M)
bull Triple-phase bone scan (less uptake in area with high pressure)
bull Near-infrared spectrometroscopy (measure tissue deoxygenation)(sens 90 spec63)(van der brand 2005)
bull Laser Doppler flowmetry
bull Infrared imaging (measure the temperature differences) (Katz LM 2008) (acute)
bull Thallous Chloride Scintigraphy + PET (shows ischemia)
bull Ultrasound (compression of deep veins increased movement of the arterial wall end diastolic closure)
bull No sure clinical test (Robert P)
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Diagnosis bull One or more of
bull 1) Preexercise pressure 15 mm Hg Or greater
bull 2) 1 minute postexercise pressure 30 mm Hg Or greater
bull 3) 5 minutes postexercise pressure 20 mm Hg Or greater
bull In addition with history and physical examination consistent with CECS
bull (Pedowitz RA)
bull Threshold 35 mm Hg specificity 73 Sensitivity 93 (van der brand JG 2005)
bull Diagnosis may require the sport-specific activity to induce symptoms (Padhiar N 1996)
Sep 2011 review af 38 artikler vedr graelignsevaeligrdier der saringr tvivl om anvendeligheden
(Scand J Med Sci Sports 2011 Sep 13)
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Diagnosis
bull Difinitive testing for CECS is invasive Therefore if diagnosis is uncertain consider differential diagnosis and examination
bull Bone scan (DEXA) stress fracture
bull EMG Nerveentrapment
bull Doppler Ultrasound Poplitea entrapment (PAES)
Muscle hernia muscle lesion tendinopathy myositis ossificans aneurism tumor and more
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Diagnosis
bull Diabetes type 1 and 2 42 cases with intermittens claudication (but no vascular signs) 38 had CECS (Edmundsson D 2010)
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Risk Factors bull Trauma (Tubb amp Vermillion 2001) bull Shoe Jerosch J Influence of the running shoe sole on
the pressure in the anterior tibial compartment (says something about shoe and pressure but not directly about CECS)
bull Anabolic steroid (Brennan F 2003)
bull Supplement of creatine (Glorioso J 2001) bull (Due to fluid retention and muscular hypertrophy)
bull Simvastatin induced myositis (Walker JL 2010)
bull Eccentric muscle contraction increased intracompartmental pressure DOMS reduction in compliance of the fascia (review Tweed J2008) (but not CECS)
bull Koslashn(hun) alder(stigende) race(hvid) og militaeligr rang (lav) bull (Am J Sports Med 2013 Aug 2)
bull 832 millioner militaeligrfolk fulgt i 5 aringr (4100 tilfaeliglde) NB Ingen anatomi deficit
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Deficits (factors which are present during CESC)
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Deficits bull 30 stress fracture of the tibia or fibula(Robert
PWilder 2010) (unpublished) bull Clinics in Sports Medicine - Volume 29 Issue 3 (July 2010)
bull 60 have fascial defects (Touliopolus S) (increased
intracompartmental pressure results in herniation og an attenuated fascial defect)
bull 25 of 26 had thickened and noncompliant fascia (biopsy) (Hurschler CR et al 1994)
bull Morten Dahl Peter Magnusson Clin Orthop Relat Res 2011 Dec469(12)3495-500 Epub 2011 Sep 24
bull MTSS (own experience)
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Deficits
bull Parestesias
bull Muscular weakness
bull Foot drop
bull Median age of occurence is 20 years old (Shah S 2004)
bull Men = women (incidenceprevalence)
bull Women gt men (Micheli LJ 1999)
bull 70-95 bilaterally (measure both sides) bull Hislop M Br J Sports Med 2011 Sep45(12)954-5
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Physical rehabilitation
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Physical rehabilitation
bull 2 years delay in diagnosis=poor outcome and low succes rate
bull NO RCT studies for physical rehabilitation (expert opinionreportscase studies)
bull Activity modification is the only non-surgical treatment to definitively reduce the symptoms (Blackman PG 2000)
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Physical rehabilitation
bull Strengthening exercise bull Stretching exercise bull Changing the biomechanical techniques of running
bull Manual therapy ( may prolong time before onset of symptoms)
bull Soft tissue release bull Stretching ( may prolong time before onset of symptoms)
bull Strengthening of muscles bull Myofascial release (Brennan F 2003)
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Physical rehabilitation
bull Ultrasound ( may prolong time before onset of symptoms)
bull Orthotics to correct pronationpes plano (Englund J
2005)
bull Hyperbaric oxygen
bull Magnetic field therapy
bull Diuretics (acute Jan TChristenson 1985)
bull Forfodsloslashb (Int J Sports Phys Ther 2011 Dec6(4)312-21)
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Physical rehabilitation
Symptoms for more than 3 month despite treatment
Surgery
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
ComplicationsSequelae
bull Calcific myonecrosis (rare outcome of compartment syndrome)
bull (Donacutet do biopsyinfections chronic discharging sinusFistula)(OacuteDwyer HM 2006)
bull Patients can develop acute compartment syndrome on top of CECS (Goldfarb S1997 Thennavan AS 1999 Touliopolous S 1999)
Athlete should be educated on symptoms of acute compartment syndrome (treatment within 12 hours)
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
PAES
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Poplitea Artery Entrapment Syndome PAES
bull Cases of PAES before 1964 rdquo0rdquo bull Stuart TP J anat physiol 187913162-5 (anatomic variation)
bull 1965 Love and Whelan PAES bull Am J Surg 1965 May109620-4
bull 80acute and 90` cases of PAES rare
bull 00acute cases of PAES rare to frequent
bull You find just what you are looking for bull Pincer impingment Cam impingment (FAI (femoroacetabular impingment))
bull D-vitamin
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
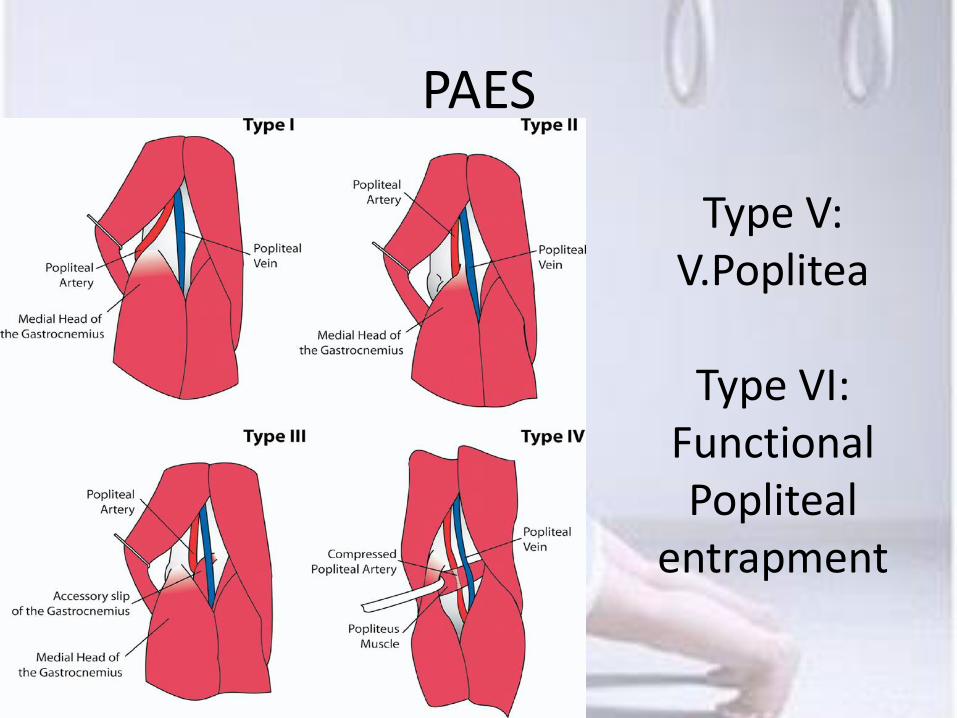
PAES
Type V VPoplitea
Type VI
Functional Popliteal
entrapment
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Poplitea Artery Entrapment Syndome PAES
bullPAES
Anatomic Functional
Popliteal Popliteal
Entrapment Entrapment
Syndrome Syndrome (30 - 50 have compression of the artery with forceful foot movement (functional compression))
(Embryologic explanation)
(Type I-V) (Type VI)
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Poplitea Artery Entrapment Syndome PAES
bull Incidence and frequency
bull Incidence of 0165 in young male entering the military service (Bouhoutsos J 1981)
bull 38 post-mortem limbs have abberant anatomy consistent with PAES (Gibson MHL 1977)
bull Predominant in males (ratio 91) bull Under the age of 30 often athletic bull Football basketball soccer running (Stager A)
bull (excessive dorsiflexion and plantarflexion of foot)
bull Incidence of bilateral (up to) 83 (Levein LJ) (others 22-67 )
bull PAES is responsible for 60 of young patiens with ischaemic pain (Collins PS 1989)
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Poplitea Artery Entrapment Syndome PAES
bull Symptoms
bull Symptoms correlates with the intensity of exercise rather than volume
bull Pain
bull Claudication
bull Deep ache or cramping involving foot and leg
bull Popliteal bruit
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Poplitea Artery Entrapment Syndome PAES
bull Examination
bull Phsical examination at rest ia bull Palpate puls during plantar flexion (knee extended)
bull Ankle-Brachial indices (ABI) bull Duplex sonography bull (30 - 50 have compression of the artery with forceful foot movement (functional compression))
bull Mri or MRA Best arteriography (after exercise or provoation) bull Computed tomographic angiography (CTA) bull Pulse volume recording (high false positive rate in athletes(Ehsan O 2004)
bull Plethysmography (high false positive rate in athletes(Ehsan O 2004)
bull UL brugbar til venoslashse form Eur J Vasc Endovasc Surg 2012 Jan43(1)81-7 Epub 2011 Nov 27
Rest Forceful plantar flexion amp before and after extercise
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Poplitea Artery Entrapment Syndome PAES
bull Treatment
bull Only surgery (Baltopoulos P 2004)
bull (Type l-V)hellipBut Functional entrapment syndrome
bull MHGH myotomi fasciotomy excision og the plantaris muscle release of the soleal sling excision of the popliteal muscle muscle detachment saphenous vein by-pass reverse saphenous vein by-pass
bull gt90 appear to return to activities in sports le 3 month with resolution of all previous symptoms (Levien LJ 2001)
bull Aggresive fascial massagehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Poplitea Artery Entrapment Syndome PAES
bull Complications
bull long term arterial damage (untreated)
bull Fibrosis of thearterial wall bull Thrombosis bull Embolism bull Popliteal aneurysm formation bull Chronic venous hyperteinsion bull DVT bull ill-defined nerve nerve symptoms
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Poplitea Artery Entrapment Syndome PAES
bull Other Compressions diagnosis
bull Thoracic outlet syndrome
bull Superior mesenteric artery syndrome
bull Coeliac artery compresssion
bull Iliac vein comprisseion
bull May Thurneracutes syndrome (left common iliac vein)
bull Nutcracker syndrome (renal vein)
Slut
Slut





























