Embed Size (px)
Citation preview

International Ophthalmology 8:159-166 (1985) �9 Dr W. Junk Publishers, Dordrecht. Printed in the Netherlands
Alteration of the blood-retina barriers in cases of viral retinitis
Bfilint Kovfics POcs, Hungary
Keywords: viral retinitis, blood-retina barrier, fluorescein angiography
Summary
This paper presents three cases of serologically documented viral retinitis, and the great value of fluorescein angiography in outlining the structural abnormalities and the site of the lesions.
Of our series in the case of influenza retinitis, the fluoroangiographic findings showed dye leakage from retinal vessels in the posterior pole. The dye leakage did not appear completely in the sites of macular edema. This edema was similar to the clinical appearance of cotton-wool spots and was arranged in a star-like pattern.
One of the cases of cytomegalovirus retinitis (Case 3), a previously healthy adult with dysfunction of the cellular immune system, seems to be a further example of an inflammation in the inner retina presenting cotton-wool spots at the early stage.
Case 2, a previously healthy adult, fulfilled the criteria for Vogt-Koyanagi-Harada syndrome. The patient had serologically documented cytomegalovirus infection with dysfunction of the cellular immune system. The fluorescein angiographic examination showed alteration both in the inner and the outer blood-retina barriers as it is characteristic in cases of Harada syndrome. The cytomegalovirus infection might be assumed to play a role in the clinical picture as well as in the etiology of this disease.
Introduction
A number of publications (1, 2, 4, 6, 8-14, 16, 19, 21) on viral retinitis can be found in the recent ophthal- mic literature, however, no agreement has yet been reached concerning the location of the primary lesion within the retina. There is evidence of a close relationship between the alteration of the blood- retina barriers (BRB) and almost every retinal dis- ease, particularly, such as vascular retinopathies and pigment epitheliopathies.
We examined the barrier function, using a stan- dard method of fluorescein angiography.
The purpose of this paper is to describe the
fluoroangiographic characteristics of serologically documented viral retinitis which have been ob- served in one case of influenza retinitis, and in two cases of cytomegalovirus retinitis. All the three patients were healthy previously.
Report of cases
Case 1
A 23-year-old previously healthy man was first seen in December 1977 with a two-week history of generalized malaise, fatique and fever. He had

160 B. Kov~cs
observed decrease in his left vision for two days. The right eye was known to have been amblyopic since childhood. On the basis of influenza epidemic at that time a viral infection had been diagnosed by the G.P. and tetracycline therapy had been admin- istered.
He was admitted to the University Eye Clinic of P6cs because of left visual disturbance. On examin- ation he had fever (37.5 ~ C), otherwise he had no other complaints except ocular ones. The findings of the physical examinations were unremarkable except for prostatic enlargement and tenderness. The WBC was 6200 with 56 percent neutrophils, 2 percent eosinophils and 42 percent typical lympho- cytes. The other haematological values and liver enzyme values were all normal. An extensive workup failed to reveal evidence of syphilis; toxo- plasmosis; fungal infection; bacterial infections; autoimmune disease; liver disease or diabetes mellitus.
On initial examination the best corrected visual acuity was 0.3 on both sides, with slight meta- morphopsy, central scotoma and distorsion on the Amsler's chart. The visual field examination was normal on the right, and there was a small relative
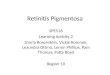
central scotoma on the left. The ERG and EOG were normal. The slit-lamp examination showed no abnormalities. Ophthalmoscopically normal disc and slightly dilated veins were found in both eyes. In the macular areas there were quite regular star-like figures originating from superficial retinal edema resembling the picture seen in cases of obstructed axoplasmic transport (Figs. la, b). No haemorrhages or other abnormalities were present in the fundi.
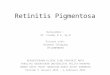
Fluoroangiographic examination was per- formed. During the early phases only a very slight masking of the perifoveal vasculature was ob- served. On the late-phase angiogram an increased affinity to fluorescein of the walls of the larger veins, hyperpermeability at the temporal disc border, and dye leakage from the retinal capillaries in the posterior pole were seen. These leaking areas appeared in different sites as compared to the sites of star-like edemas (Figs. 2a, b).
A diagnosis of acute influenza A virus infection was established by serial complement fixing anti- body tests. The titer, two weeks after the onset of the illness (on admission), was 1:128 and falling to 1:32, six weeks later. Gentamycine, vitamines B
Fig. 1-ab. Case 1: Fundus photograph of the right- and left fundus with perifoveal edema arranged in a star-like pattern.

Alteration of the blood-retina barriers in cases of viral retinitis 161
Fig. 2-ab. Case 1: Fluorescein angiogram of the right and left posterior pole showing blurred hyperfluorescent, temporal disc border, dilated veins and spotty hyperfluorescence from leaking capillaries. There are also two dot-like spots above the left fovca, likely representing capillary microaneurysms.
and C, and dexamethasone (subconjunctivally) were administered. The patient rapidly became afebrile.
On re-examination, six weeks later, he was com- pletely asymptomatic. The corrected visual acuity was 0.6 on both sides. The fundus lesions disap- peared without any remnants. Three years later the visual acuity was the same and only subtle pigmen- tary changes were seen in the maculas.
Case 2
A 23-year-old man with sudden loss of vision on the right, and four days later, in the left eye was admit- ted to our clinic in December 1978. He complained of having had fever (max. 38.5~ for 7 days, throatache, splitting headache and retrobulbar pain which had been more severe at the time of visual loss. At the first examination his visual acuity was counting fingers from 2 m on both sides. The visual field examination revealed big central abso- lute scotomata. The external eye examination showed no abnormalities. The lenses were clear,
the vitreous body was clear on the left, and moder- ately hazy on the right.
The fundus examination showed moderate hy- peraemy of the optic disc, peripapillary edema and swollen nerve-fibre bundles. In the posterior pole there were exudative retinal detachments with macular involvement almost the same in shape and size on both sides.
The WBC was 9800 with 4% eosinophils and 14% lymphocytes. The other haematological val- ues were normal. The physical examinations were unremarkable. The neurological examination re- vealed lymphocytic meningitis with 3000/3 lympho- cytes in CSF. The protein concentration of the CSF was elevated to 156mg%. The EEG showed no pathological changes. The patient was transferred to the neurological department where penicillin, streptomycin, gentamycin and dexamethasonc were administered. An extensive workup failed to reveal evidence of tuberculosis, leptospirosis, toxoplasmosis or bacterial infections. The findings of repeated virus cultures from urine, blood and liquor were negative. The influenza A, B, HSV,

162 B. Kov6cs
measles, coxackie, echo and mumps virus comple- ment fixing antibody titers were all normal.
But, the titers of complement fixing antibodies to cytomegalovirus were 1:152 at the first examin- ation and 1:32 six weeks later.
While he was hospitalized in the neurological department, the fundus picture changed rapidly. One week after the first examination the ophthal- moscopy revealed pronounced disc edema in both eyes and dilated veins. The arteries were attenu- ated and sheathed close to the optic disc. The retina was edematous and there were some superficial flame shaped haemorrhages. The exudative retinal detachment in the posterior pole flattened com- pletely. Some days later severe anterior uveitis and vitritis developed on both sides. The initial therapy of subconjunctivally administered dexamethasone and topical mydriatics was continued.
The patient was readmitted to our clinic. He was afebrile, the headache disappeared but the vision still persisted to be blurred. The visual acuity was 0.1 on both sides. The ERG was subnormal, the EOG examination showed the L/D ratio 1.65 in each eye. Because of hazy media fluorescein an- giography was performed only in the left eye (the fundus pictures changed simultaneously and
showed almost the same features). Thefluorescein angiography (Fig. 3) revealed an
edematous disc, dilated veins with increased stain- ing of their walls and a prominent widespread dye leakage from the retinal capillaries in the entire fundus. There were some bright dotlike fluorescent spots and subretinal leakage areas.
The immunological examination revealed that 'The percentage of the T cells was reduced in the blood, but the response of T cells to phytohaemag- glutinin was found to be normal. The percentage of circulating B cells was slightly reduced. The lower C3, C4 concentrations are indicators of an in vivo complement activation'. (Report issued by the Im- munological Department.)
Four months after the onset of his illnes, the eyes became quiet, the inflammatory signs disappeared, the vitreous cleared up, and the visual acuity im- proved to 1.0 on both sides. The fundus examin- ation revealed widespread atrophic changes of the retina and of the pigmentary epithelium. The con- trol fluorescein angiography (Fig. 4) showed
Fig. 3. Case 2: Left eye, late phase fluorescein angiogram taken 7 weeks after the onset of the disease. Note the profuse leakage of fluorescein both from the capillaries of the optic disc and from the retinal vessels. There are some bright dot-like fluorescent
spots.
Fig. 4. Case 2: Left eye, late phase fluorescein angiogram taken 3 months later, as seen on Fig. 3. The angiogram shows a mott led pat tern of hyperfluorescence in the posterior pole and the irregular disc border. There is no leakage of fluorescein from retinal vessels or from the choroid.

Alteration of the blood-retina barriers in cases of viral retinitis 163
hyper-, and hypofluorescent areas in the entire fundus, but no leakage from the vessels was detec- table.
During the first two years after the onset there had been many recurrences of the anterior uveitis with secondary glaucoma on both sides.
Meanwhile some aequatorial lens opacities de- veloped which had been proved stationary for four years. A year after the onset poliosis of the upper lashes and, half a year later, vitiligo on the lower eyelids, appeared.
During the last check-up examination, about 6 years following the onset, there were no signs of inflammation and the asymptomatic patient had normal vision, and only slightly restricted visual field, with enlarged blind spots, and the diminished dark adaptation remained unnoticed for the pa- tient.
Case 3
A 25-year-old midwife with viral infection ac- companied by 'mononucleosis' and swelling of the submandibular lymph nodes had been observed in a hospital. At that time she had complained of blurred vision in the right eye, and the ophthal- mologist had reported fundus lesions as 'perimacu- lar cotton-wool exudates'. She had been referred to our clinic 2 months after the beginning of her com- plaints.
The eye examination revealed the visual acuity 0.2 in the right, and 1.0 in the left eye. There was a central scotoma in the visual field. The ERG and EOG were normal. The external status of the eyes was unremarkable. The fundus examination showed (Fig. 5a) a well outlined, relatively large depigmented area at the posterior pole of the right eye. In the fovea there was a glial scarring and some deep and superficial haemorrhages around it. The central retina was edematous in a moderate degree. The disc and vessels were normal. The left fundus was entirely normal.
Fluorescein angiography on the right side was performed. The angiograms showed (Fig. 5b) a large hyperfluorescent area indicating the depig- mentation in the pigmentary epithelium. In the fovea the glial scarring showed only a moderate
Fig. 5a. Case 3: Fundus photograph of right eye with pigmentary changes in the posterior pole, glial scarring and haemorrhages in the macular area.
Fig. 5b. Case 3: Right eye, late venous phase fluorescein angio- gram. The mottled hyperfluorescence indicates the pigmentary disturbance. The glial scar in the fovea shows only a moderate degree of fluorescence. Small haemorrhages blocking fluores- cence are also visible. There is no leakage of fluorescein.

164 B. Kovdcs
affinity to fluorescein. The angiography failed to show evidences of dye leakage either from the retinal vessels or from the choriocapillaries. There were no signs of new vessel formations beneath the retina.
The control fluorescein angiogram (Fig. 6) showed the same extent of pigmentary changes, but the foveal scarring became flattened. Later on all of the haemorrhages had disappeared and the visual acuity improved to 0.4.
An extensive workup failed to reveal evidence of syphilis, toxoplasmosis, fungal infections, autoim- mune disease, liver disease or diabetes mellitus. Viral cultures from urine and tear were negative. The initial WBC was 6000 with 54 percent neu- trophils and 46 percent lymphocytes.
No antibodies were detected to HSV, varicella- zoster virus, EBV, and measles virus. The fluores- cent antibody titer for CMV was 1:160 at the first examination and 1:32 two months later.
The immunological examination revealed that the percentage of the T cells was normal and of the B cells was reduced in the blood. Although the complement breakdown products did not exceed
Fig. 6. Case 3: Right eye, late phase control fluorescein angio- gram. Almost identical findings as seen in Fig. 5b except for the flattened central glious scar.
the normal level, the decreases C3 and C4 concen- trations indicated an increased in vivo complement consumption.
On the last control examination, 8 months after the beginning, the patient had no complaints and her visual acuity was reduced to 0.4.
Discussion
The first of our cases, reported above, had star-like figures at the maculas, which proved to be a com- plication of influenza infection. In a review of Duke-Elder (7) stellate retinopathy was foun~t as a frequent fundus lesion in such cases. Mathur (14) reporting one case of macular lesion after influenza drew the conclusion (from the etiology) that the macular lesion seemed to be of vascular origin, due to involvement of the retinal and choroidal vessels. In our case the fluoroangiographic findings showed dye leakage from the retinal vessels in the posterior pole. It appeared, at least partially, in different sites as compared to the sites of macular edema. These lesions were white opacities, similar to the clinical appearance of cotton-wool spots with indis- tinct borders in the nerve fiber layer of the retina arranged in star-like pattern. McLeod et al. (15) have shown that cotton-wool spots represent the accumulation of cytoplasmic organelles in axons of the nerve fiber layer caused by ischaemia-induced obstruction of axoplasmic transport. Holland et al.
(12), in cases of CMV retinitis, assumed that such spots might have resulted from focal immuno- complex vasculitis. However, Pepose et al. (19) found no data supporting the theory that pro- ductive CMV infection and humoral immunity might play any role in the production of cotton-
wool spots. Our fluoroangiographic findings showed an in-
volvement of the innermost retinal layers only, the pigment epithelium and the choroid remained un- affected. The angiograms revealed no focal retinal ischaemia but the two dot-like bright fluorescent spots on the left fundus likely represent capillary microaneurysms regarded as an indicator of retinal hypoxia.
Case 2 in our studies suggests the necessity of a

Alteration o f the blood-retina barriers' in cases o f viral retinitis 165
new approach since we have found acute CMV infection in a typical Harada case including exuda- tive retinal detachment, which ophthalmo- scopically was the same as found in CMV retinitis by Meredith et al. (16). This case fulfills the criteria for Vogt-Koyanagi-Harada syndrome which had been discussed by Snyder and Tessler (20). The cause of this disease is unknown. Morris and Schlaegel (17) found viruslike inclusion bodies in subretinal fluid in uveo-encephalitis.
A diagnosis of acute cytomegalic virus infection was considered by documenting rise in antibody titers. The viral cultures from urine, blood and CSF were negative. The subretinal fluid was not evalu- ated.
Although CMV antibodies are often acquired during adult life, the generalized form is very sel- dom recognized in adults except as a complication of debilitating diseases, cytotoxic drugs, blood transfusion or acquired cellular immunodeficiency syndrome. The history of our patient was negative according to these factors.
Ocular involvements in CMV infection in other- wise healthy adults have rarely been reported; Chawla et al. (4) found pin-point chorioretinitis and irregular sheathing in one patient, England et
al. (8) found prominent bilateral cotton-wool spots.
In our two CMV cases the evaluation of cellular immunity indicated a dysfunction of the T-cell arm of the immune system for the duration of clinical symptoms. Case 3 has shown almost the same dys- function of the immune system for half a year, therefore, this line of evidence suggests that CMV infection can cause alteration in the cellular im- munity. Holland et al. (12) drew the conclusion that the CMV infection might be the result rather than the cause of the T-cell defect in cases of acquired immunodeficiency syndrome.
Viruses can reach the eyes through the blood stream via the retinal as well as the choroidal ves- sels. The results of animal experiments by Buyuk- mihci et al. (3) suggest that slow virus agents may spread centrifugally in the nerve fibres after intra- cerebral inoculation causing retinopathy.
The histopathoiogical findings of viral retinitis in SSPE by Nelson et al. (18) and in CMV retinitis by
Wyhinny et al. (21) have shown the primary process in the neuronal elements and vessels of the retina.
In most cases, the primary viral disease is a reti- nitis when the involvement of the retinal vessels can be detected by fluorescein angiography show- ing alteration in the inner blood-retina barrier. The limited involvement of the choroid and pigment epithelium could also be demonstrated in the same way.
In a previous report by Kovfics and Vastag (13) the fluoroangiographic examination of the acute stage of retinal lesion of SSPE showed an ex- clusively localized retinal vascular involvement. A similar finding was published by Brudet-Wicket et
al. (2). In a case of acute measles retinopathy Haltia et al. (10) found the fluoroangiographic pic- ture suggestive of early lesion in the pigment epi- thelium. The presence of viral structures verified by ultrastructural and immunofluorescent studies was, however, showed only in the neuroretina. The artificial immunosuppression made in their case might explain the divergent fluoroangiographic features (9). In a rare case of acute rubella retinitis in an adult Hayashi et al. (11) observed the primary lesion in the pigment epithelium angiographically. In a case of Rift Valley fever retinitis (6) the fluo- rescein angiography showed severe bilateral ar- teriolar occlusions and delay in retinal vascular filling. There was leakage of fluorescein in the macular area.
Of our cases the previously published case of acute stage of retinal lesion in SSPE and the case of influenza retinitis clearly demonstrate the primary retinal vascular involvement. These findings refer to a superficial change in retinal vascular and sub- sequently neuronal structures. Case 3 seems to be a further example of lesion in the inner retinal layer, but the late stage fluoroangiographic examination showed only the secondary alterations. The fluor- escein angiographic examination of Case 2 showed alteration both in the inner and the outer blood- retina barriers as it is characteristic in cases of Harada disease.
In addition, it is interesting to see that we could demonstrate capillary microaneurysms in Case 1 and 2 similar to the case of Augsburger and Henry (1) with cytomegalovirus infection.

166 B. Kov6cs
References
1. Augsburger, J.J. & R.Y. Henry. Retinal aneurysms in adult cytomegalovirus retinitis. Am. J. Ophthal. 86: 794- 797 (1978).
2. Brudet-Wickel, C.L.M., M. Hogeweg & D. de Wolff- Rouendaal. Subacute sclerosing panencephalitis (SSPE) A case report. Documenta Ophthalmologica 52:241-249 (1982).
3. Buyukmihci, N., M. Rorvik & R.F. Marsh. Replication of the scrapie agent in ocular neural tissues (hamster) slow virus infection (retinopathy). Proc. Natl. Acad. Sci. U.S.A. 77/211:1169-1171 (1980).
4. Chawla, H.B., M.J. Ford, J.F. Munro, R.E. Scorgie & A.R. Watson. Ocular involvement in cytomegalovirus in- fection in a previously healthy adult. Brit. Med. J. 2: 281- 282 (1976).
5. Cunha-Vaz, J.G. The blood-retinal barriers. Doeumenta Ophthalmologica 41, 2:287-327 (1976).
6. Deutman, A.F. & H.J. Klomp. Rift Valley fever retinitis. Am. J. Ophthal. 92:38~2 (1981).
7. Duke-Elder, S. System of Ophthalmology, Vol. X, p. 271. London, Henry Kimpton (1967).
8. England, A.C., S.A. Miller & D.G. Maki. Ocular findings of acute cytomegalovirus infection in an immunologically competent adult. New Engl. J. Med. 307/2:94-95 (1982).
9. Erkkilfi, H. & A. Tarkannen. Fluoroangiographic picture of the acute stage in measles retinopathy. Ophthalmologica (Basel) 178:70 (1979).
10. Haltia, M., A. Tarkannen, A. Vaheri, A. Paetau, K. Kaakinen & H. Erkkil~i. Measles retinopathy during immunosuppression. Brit. J. Ophthal. 62:356-360 (1978).
11. Hayashi, M., N. Yoshimura & T. Kondo. Acute rubella retinal pigment epitheliitis in an adult. Am. J. Ophthal. 93: 285-288 (1982).
12. Holland, G.N., M.S. Gottlieb, R.D. Yee, H.M. Schanker
& T.H. Pettit. Ocular disorders associated with a new se- vere acquired cellular immunodeficiency syndrome. Am. J. Ophthal 93:393-402 (1982).
13. Kov~cs, B. & O. Vastag. Fluoroangiographic picture of the acute stage of the retinal lesion in subacute sclerosing pan- encephalitis. Ophthalmologica (Basel) 177:264-269 (1978).
14. Mathur, S.P. Macular lesion after influenza. Brit. J. Oph- thal. 42:702 (1958).
15. McLeod, D., J. Marshall, E. Kohner & A. Bird. The role of axoplasmic transport in the pathogenesis of retinal cotton- wool spots. Brit. J. Ophthal. 61:177-191 (1977).
16. Meredith, T.A., T.M. Aaaberg & F.H. Reeser. Rheg- matogenous retinal detachment complicating cytomegalo- virus retinitis. Am. J. Ophthal. 87:793-796 (1979).
17. Morris, W.R. & T.F. Schlaegel. Viruslike inclusion bodies in subretinal fluid in uveo-encephalitis. Am. J. Ophthal. 58: 940-944 (1964).
18. Nelson, D.A., A. Weiner, M. Yanoff & J. de Peralta. Retinal lesions in subacute sclerosing panencephalitis. Arch. Ophthal. 84:613-621 (1970).
19. Pepose, J.S., M.S. Nestor, G.N. Holland, A.J. Cochran & R.Y. Foos. An analysis of retinal cotton-wool spots and cytomegalovirus retinitis in the acquired immunodeficiency syndrome. Am. J. Ophthal. 95:118--120 (1983).
20. Snyder, D.A. & H.H. Tessler. Vogt-Koyanagi-Harada syn- drome. Am. J. Ophthal. 90:69-75 (1980).
21. Wyhinny, G.J., D.J. Apple, F.R. Guastella & Ch.M. Vygantas. Adult cytomegalic inclusion retinitis. Am. J. Ophthal. 76:773-781 (1973).
Authors' address: B. Kov~cs M.D. Department of Ophthalmology University of P6cs H-7643 P6cs, Ifjtls~ig u. 31. Hungary