Embed Size (px)
Citation preview
an educational program of:
Allergic ConjunctivitisRevised guidelines June 2003
Slide 2
GLORIA resource documents
Allergic Conjunctivitis: Assessment and Therapy
• World Allergy Organization-IAACI 2003
Contemporary Approaches to Ocular Allergy Management
• American College of Allergy, Asthma and Immunology 1998
World Allergy Forum Program Series
• World Allergy Organization 2000-2003

Slide 3
Revised Nomenclature of Allergic Disease
Intermittent – occasional symptoms lasting < 4 days per week on ≤ 4 weeks
Persistent – symptoms lasting > 4 days per week or > 4 weeks
Slide 4
Allergic Conjunctivitis
A broad group of allergic conditions involving inflammation of the conjunctiva• Acute Allergic Conjunctivitis (AAC)• Intermittent/Seasonal Allergic Conjunctivitis
(IAC/SAC)• Persistent/Perennial Allergic Conjunctivitis (PAC)• Giant Papillary Conjunctivitis (GPC)• Vernal Keratoconjunctivitis (VKC)• Atopic Keratoconjunctivitis (AKC)
Slide 5
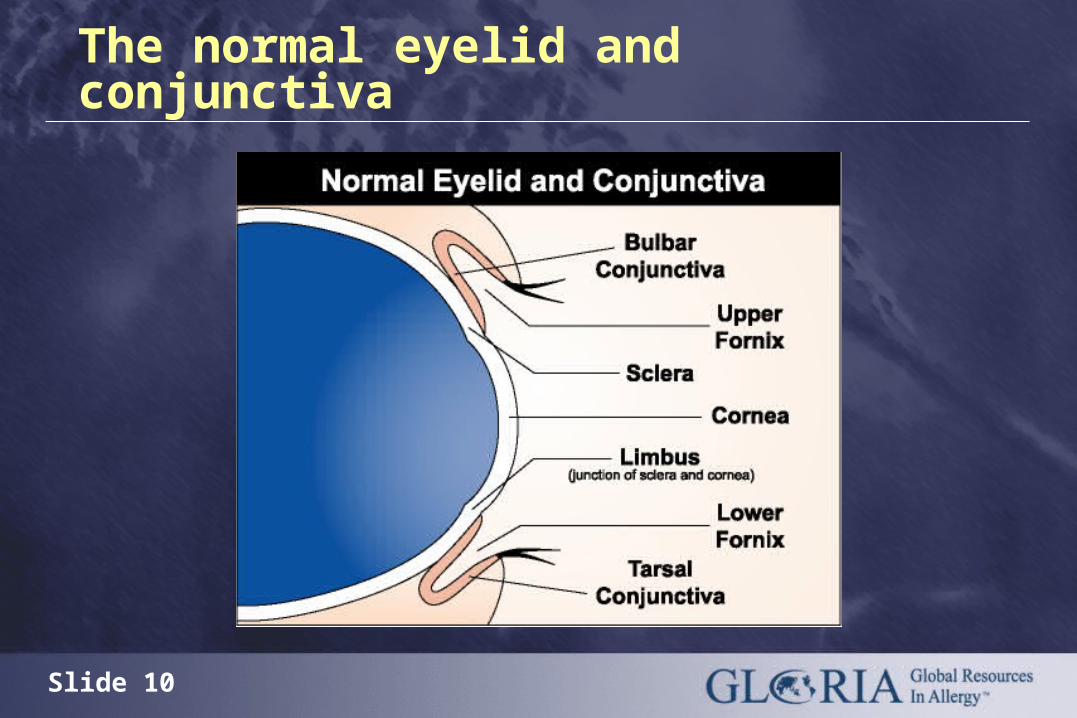
The Conjunctiva
The surface of the eye is the most obviously exposed mucous membrane of the body
The conjunctival surface is accessible to allergens and is the site of allergic reactions
Slide 6
Allergic conjunctivitis: Epidemiology
Acute Allergic Conjunctivitis (AAC)
• Occurs at any age, especially childhood
Intermittent/Seasonal Allergic Conjunctivitis (IAC/SAC)
• Affects 5% to 22% of the general population
Slide 7
Allergic conjunctivitis: Epidemiology
Persistent/Perennial Allergic Conjunctivitis (PAC)
• Found in 4% of patients attending an inner city health center during summer months, USA Dart et al, 1986
Giant Papillary Conjunctivitis (GPC)
• 1 - 5% of rigid gas permeable contact lens wearers; 10-15% of hydrogel (soft) contact lens wearers, USA Abelson, 2000
Slide 8
Allergic conjunctivitis: Epidemiology
Vernal Keratoconjunctivitis (VKC)
• Pre-pubescent boys in warm, dry climate
• 10% of all eye patients in East Jerusalem, O’Shea, 2000
• 0.5-1.0% of all patients in eye clinics worldwide, Beigelman, 1950

Slide 9
Allergic conjunctivitis: Epidemiology
Atopic Keratoconjunctivitis (AKC)
• Atopic Eczema/Dermatitis Syndrome affects 3% of US population; 15-40% of AEDS patients develop AKC.
• Occurs 2nd through 5th decade, males more often affected than females
Slide 10
The normal eyelid and conjunctiva
Slide 11
Allergic conjunctivitis: Major symptoms
Pronounced itching
Watery, stringy or ropy discharge
Redness
Slide 12
Diagnosis of allergic conjunctivitis
Detailed personal and family allergic history and physical examination
History of typical eye symptoms
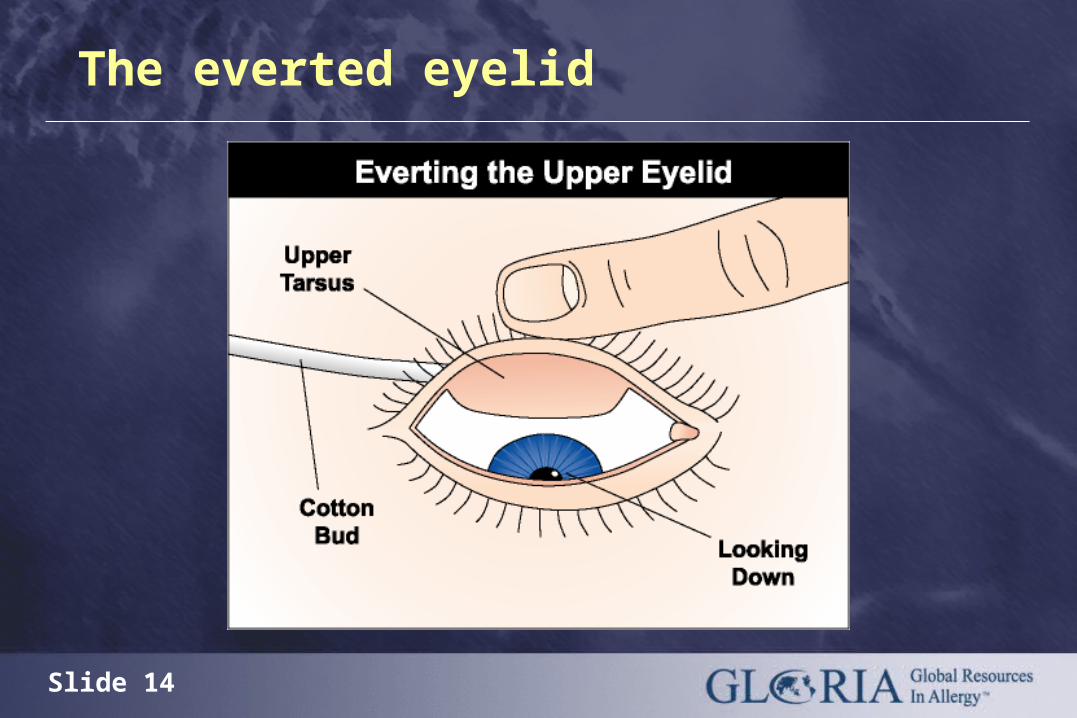
Appearance of everted (flipped) eyelid

Slide 13
Examination of surface of the eye
The surface markings of the conjunctiva extend beyond the visible limits of the eye
Slide 14
The everted eyelid
Slide 15
Diagnosis of allergic conjunctivitis: Clinical investigations
Allergy skin tests performed by an allergist
and/or
Measurement of allergen specific IgE antibody (Radioallergosorbent tests)
Conjunctival scrapings for eosinophils – particularly elevated in VKC, AKC and GPC
Conjunctival challenge
Slide 16
Differential diagnosis of allergic conjunctivitis
Acute Allergic Conjunctivitis (AAC) occurs at any age, especially childhood
Large quantity of allergen (eg, plant pollen) inoculated into eye causes:
• Intense itching
• Immediate swelling of conjunctiva and lids (eye may close)
Self-limiting

Slide 17
Acute allergic conjunctivitis
Slide 18
Differential diagnosis of allergic conjunctivitis
Intermittent/Seasonal Allergic Conjunctivitis (IAC/SAC)
Persistent/Perennial Allergic Conjunctivitis (PAC)
• Related to seasonal or perennial allergens, association with genetic predisposition to allergic rhinitis

Slide 19
Everted eyelid in intermittent/seasonal allergic conjunctivitis

Slide 20
Persistent/perennial allergic conjunctivitis
Slide 21
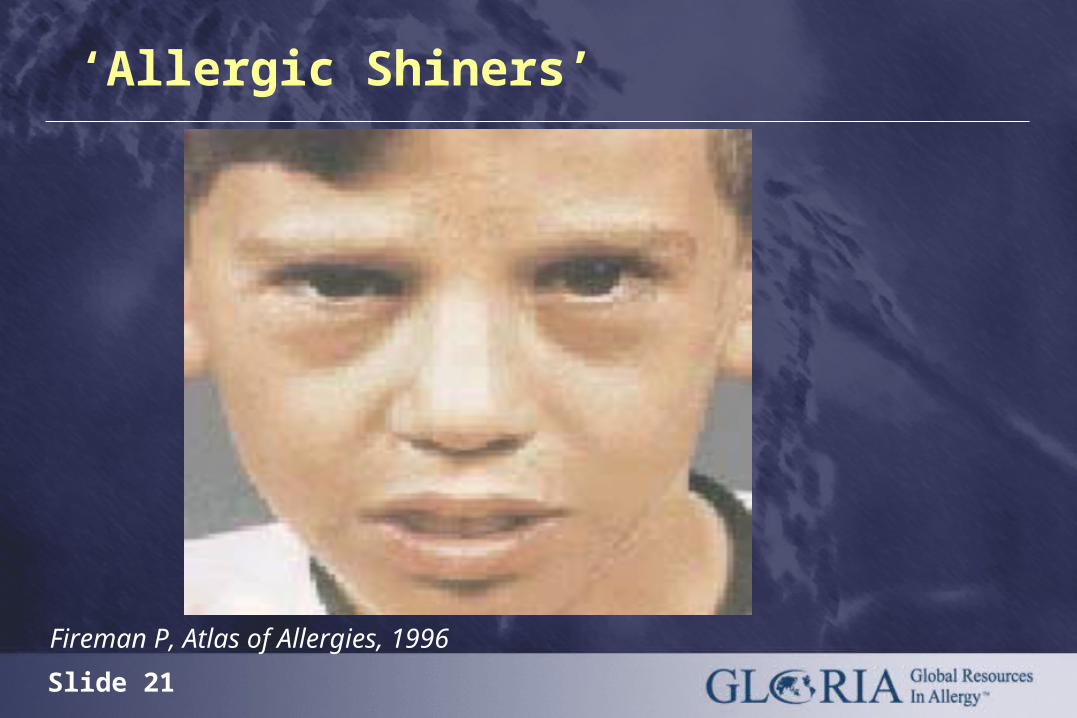
‘Allergic Shiners’
Fireman P, Atlas of Allergies, 1996
Slide 22
Giant Papillary Conjunctivitis (GPC)
• Trauma due to contact lens, ocular prosthesis, aggravated by concomitant allergy
Differential diagnosis of allergic conjunctivitis

Slide 23
The upper tarsal conjunctiva in giant papillary conjunctivitis
Slide 24
Differential diagnosis of allergic conjunctivitis
Vernal Keratoconjunctivitis
• A disease of childhood sometimes associated with atopic constitution.
Severe T-cell mediated disease involving the cornea: may be sight-threatening

Slide 25
Conjunctival appearance in vernal keratoconjunctivitis
Slide 26
Atopic Keratoconjunctivitis• A persistent disease of the eyelids usually
beginning in young adulthood. Associated with the atopic eczema/dermatitis syndrome (AEDS) infection, corneal thinning, cataracts and environmental allergens.
Differential diagnosis of allergic conjunctivitis
Severe T-cell mediated disease involving the cornea: may be sight-threatening

Slide 27
The eye and periorbital region in atopic keratoconjunctivitis
Slide 28
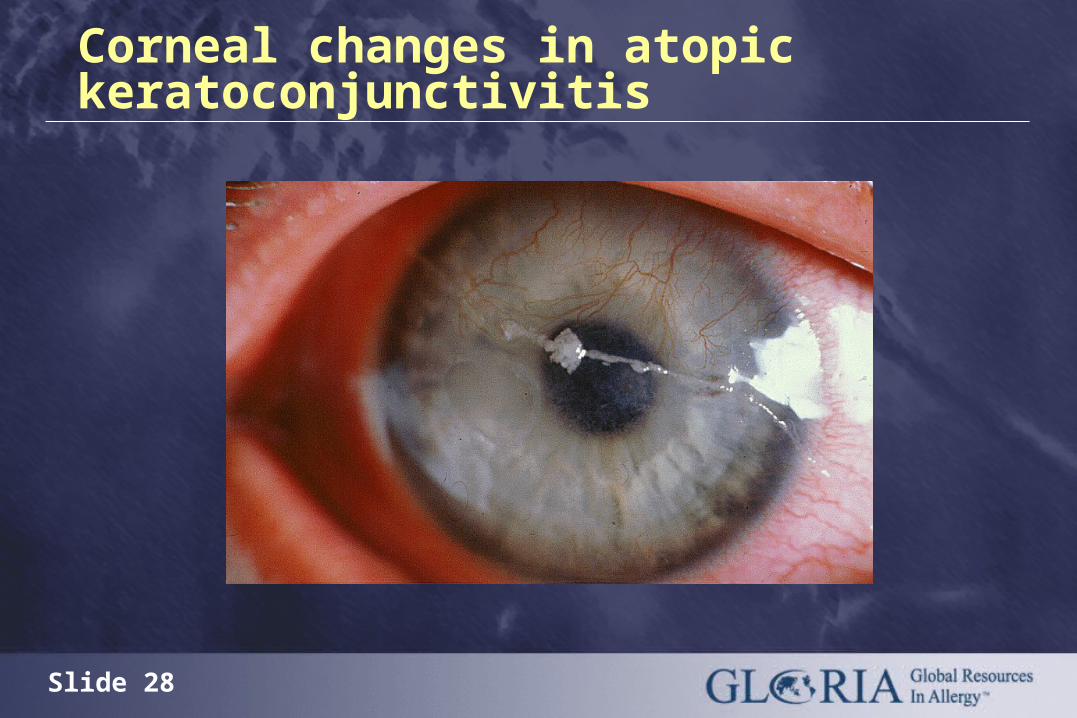
Corneal changes in atopic keratoconjunctivitis
Slide 29
Simple differential diagnosis of allergic conjunctivitis and other conditions
If it itches, it is allergy;
if it burns, it is probably dry eye;
if the eyelids are stuck together in the
morning, it is a bacterial infection.

Slide 30
Globally important allergens
House dust mites
Grass, tree and weed pollen
Pets
Cockroaches
Molds

Slide 31
Clinical investigations: Allergy skin prick testing
Skin prick test / positive result
Slide 32
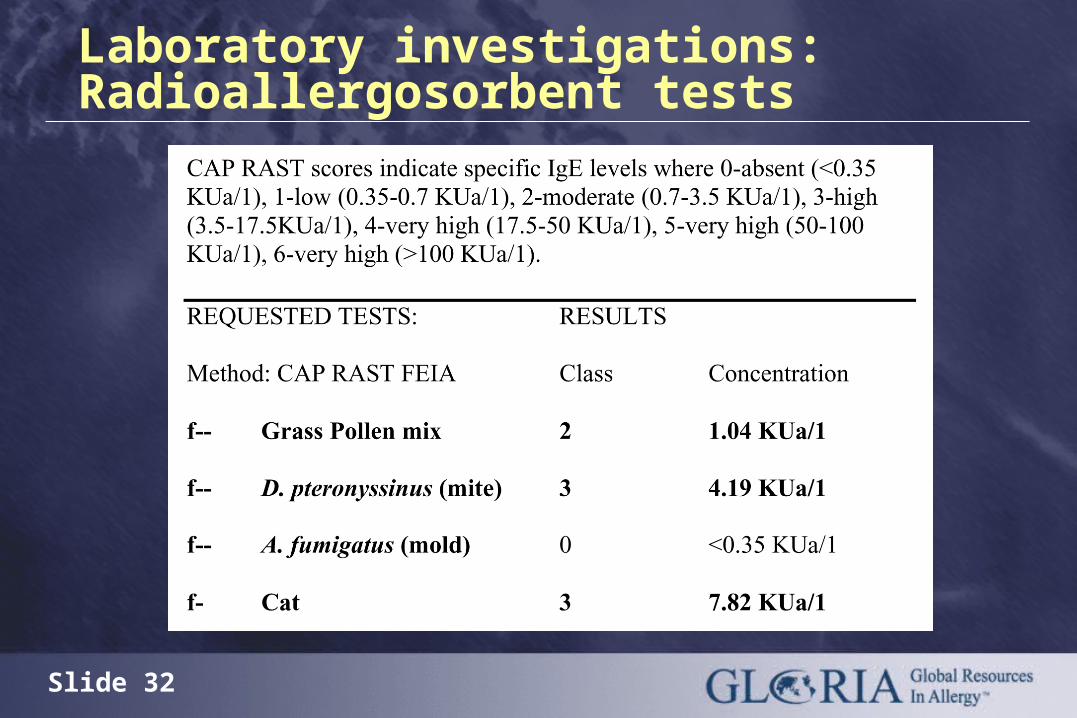
Laboratory investigations: Radioallergosorbent tests
Slide 33
Different cell types infiltrate the conjunctiva
AAC, IAC, SAC, PAC
• Mast cells
• Eosinophils
• Neutrophils
GPC, VKC, AKC
• T cells
• Eosinophils
• Mast Cells
• Neutrophils
Slide 34
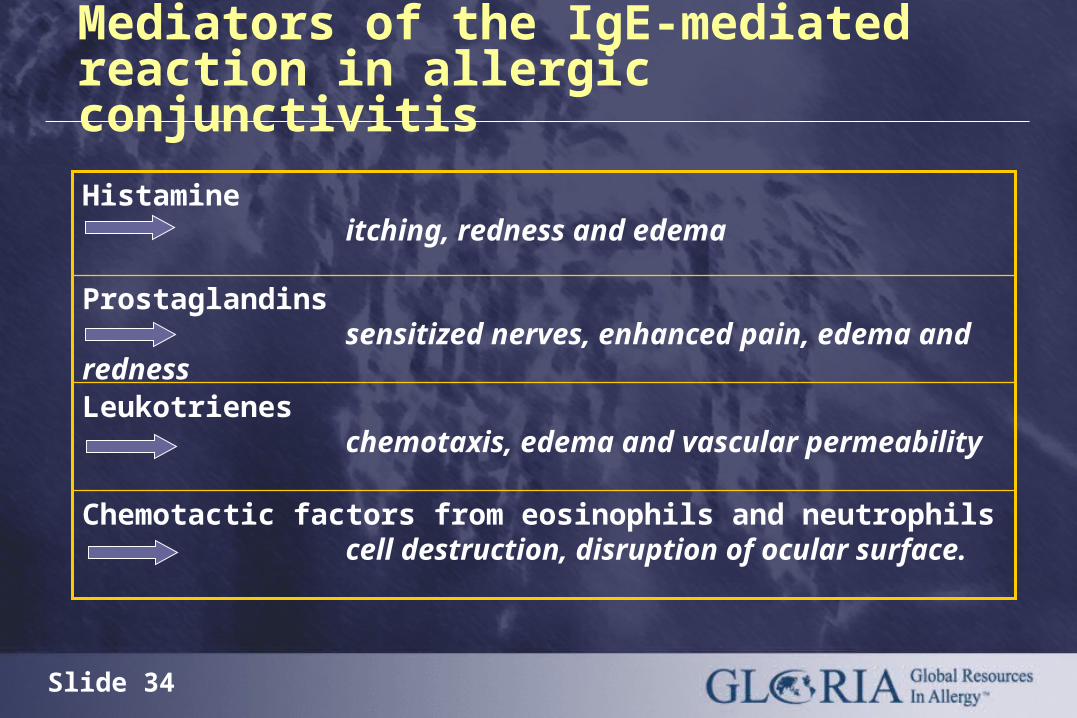
Mediators of the IgE-mediated reaction in allergic conjunctivitis
Chemotactic factors from eosinophils and neutrophils cell destruction, disruption of ocular surface.
Leukotrienes chemotaxis, edema and vascular permeability
Prostaglandins sensitized nerves, enhanced pain, edema and redness
Histamine itching, redness and edema

Slide 35
Modes and sites of action of allergic conjunctivitis therapies
Mast cell
B cell
T cell
(mast cell) Eosinophil
IL-4
IL-3, -5
GM-CSF
VCAM-1
IgE
Immediate symptoms• Itch, redness, edema,chemotaxis, edema, vascular permeability
•Sensitized nerves, enhanced pain, edema, redness
Chronic symptoms•cell destruction
•disruption of ocular surface
HistamineLeukotrienesProstaglandins
Allergen
Allergen avoidance
Immuno-therapy
AntihistaminesOlopatadine
Sodium cromoglycateOlopatadine
Steroids
Eosinophil and Neutrophil chemotactic factors:
Anti-IgE
Slide 36
Treatment of allergic conjunctivitis: Allergen avoidance
Allergen avoidance and environmental control
are the
first steps in the
management of allergic disease

Slide 37
Treatment of allergic conjunctivitis: Allergen avoidanceHouse dust mites:
• Provide adequate ventilation todecrease humidity
• Wash bedding regularly at 60°C• Encase pillow, mattress and quilt in allergen
impermeable covers• Dispose of feather bedding • Use vacuum cleaner with HEPA filter (when available)• Replace carpets with linoleum or wooden floors• Remove curtains, pets and stuffed toys from bedroom• Provide adequate ventilation to decrease humidity
Slide 38
Treatment of allergic conjunctivitis: Allergen avoidance
Pollen
• Very difficult to avoid!
• Remain indoors with windows closed at peak pollen times
• Wear sunglasses and hat outdoors
• Use air-conditioning, where possible
• Install car pollen filter

Slide 39
Treatment of allergic conjunctivitis: Allergen avoidance
Pet Allergens
• Exclude pets from bedrooms and, where possible, from home
• Vacuum carpets, mattresses and upholstery regularly
• Wash pets regularly
Slide 40
Treatment of allergic conjunctivitis: Allergen avoidance
Cockroach Allergens
• Eradicate cockroaches with appropriate insecticide
• Eliminate dampness, cracks in floors, ceilings, cover food; wash surfaces, floors, fabrics to remove allergen
© 1998-2003 Troy Bartlett
Slide 41
Molds
• Ensure dry housing
• Use ammonia to remove mold from bathrooms and other wet spaces
Treatment of allergic conjunctivitis: Allergen avoidance
Slide 42
Treatment of allergic conjunctivitis:Non-pharmacological therapy
Allergen avoidance including physical barriers, eg, hat, sunglasses, allergen-impermeable pillow and mattress covers
Cold compresses
Preservative-free tears
Slide 43
Topical NSAIDs
• Ketorolac – of limited effectiveness
Vasoconstrictors
• Not recommended for regular use
Pharmacotherapy of allergic conjunctivitis:Topical NSAIDs, Vasoconstrictors

Slide 44
Pharmacotherapy of allergic conjunctivitis: Topical antihistamines
Topical antihistamines
• azelastine, emedastine, levocabastine
Topical antihistamine plus vasoconstrictor
• antazoline-naphazoline, cetirizine-pseudoephedrine, pheniramine-naphazoline
Slide 45
Pharmacotherapy of allergic conjunctivitis
Once daily administration
Rapid onset and 24 hour duration of action
No sedation
No interaction with alcohol, foods, drugs
Additive anti-allergic activities
Properties required of ideal new generation oral antihistamines
Slide 46
Pharmacotherapy of allergic conjunctivitis: Oral antihistamines
Less effective than topical therapies
Beware unwanted effects of ‘dry eye’
If indicated for multiple allergic symptomatology, select non-sedating oral antihistamines:
loratadine, fexofenadine, cetirizine
Slide 47
Pharmacotherapy of allergic conjunctivitis: Topical mast cell stabilizers
Preventative: Do not work immediately
DSCG: Debatable effectiveness
Nedocromil: Twice daily
Lodoxamide: Highly potent, rapid relief, additional anti-eosinophilic effect
Pemirolast: Twice or four times daily dosing, effective for itch
Slide 48
Pharmacotherapy of allergic conjunctivitis: Dual-action antihistamine/mast cell stabilizer
Olopatadine: Highly effective, comfortable
Ketotifen: Approved for itch
Azelastine: Approved for itch
Slide 49
Pharmacotherapy of allergic conjunctivitis: Topical corticosteroids
Topical corticosteroid therapy must be prescribed and monitored, preferably by an ophthalmologist because:
• It is only appropriate for treatment of severe allergic ocular disease – not for intermittent/seasonal allergic conjunctivitis
• Prolonged use can lead to secondary bacterial infection, glaucoma and cataracts
Slide 50
Pharmacotherapy of allergic conjunctivitis: Specific allergen immunotherapy (allergen vaccination)
Must be administered by allergy specialist centre with resuscitation facilities
Helpful in managing persistent allergic rhinitis and atopic keratoconjunctivitis
Of value in patients with multi-organ symptoms of IgE-mediated allergic sensitization
Risk-to-benefit ratio must be considered in all cases
Highly effective in selected patients
Slide 51
Pharmacotherapy guidelines for persistent/perennial allergic conjunctivitis
Topical mast cell stabilizer, or
Dual action antihistamine/ mast cell stabilizer
Consider immunotherapy/ vaccination at specialist center
Step 1
Step 2

Slide 52
Pharmacotherapy guidelines for intermittent/seasonal allergic conjunctivitis
Topical antihistamine and/or topical NSAID
Step 1
Step 2
Step 3
Topical antihistamine with vasoconstrictors
Dual action antihistamine/mast cell stabilizer
Therapy may be increased in a step-wise fashion until adequate control is achieved, or commenced at Step 3
Slide 53
Pharmacotherapy of allergic disease: Future directions – Anti IgE
>75% of allergic asthmatics have rhinitis; >40% of allergic rhinitis patients have allergic conjunctivitis
Humanized monoclonal antibodies against IgE, e.g., omalizumab are effective for treatment of moderate to severe asthma. Such therapy:
(cont’d on next slide)
Slide 54
• Decreases free IgE levels and down-regulates IgE receptors on basophils
• Inhibits the late phase allergic reaction following allergen bronchial challenge
• Preliminary study indicates omalizumab is effective for nasal and ophthalmic symptoms of intermittent and perennial allergic rhinitis
• Ongoing studies to determine the effect of omalizumab in atopic dermatitis may have implications for treatment of AKC
Pharmacotherapy of allergic disease: Future directions- Anti IgE, cont’d.
Slide 55
Persistent or worsening ocular allergy
Persistent or worsening eye symptoms not responsive
to therapy are an indication for urgent referral to a
physician who specializes in allergic eye disease.