Embed Size (px)
Citation preview

Annual Rheumatology &
Therapeutics Review for
Organizations & Societies

Safety of Biologics

Biologics* in Rheumatoid Arthritis
* Tofacitinib & Apremilast are not biologics
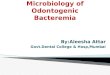
Agent Biologic Target Construct
Infliximab TNF Chimeric MAb
Etanercept TNF IgG-p75 receptor
Adalimumab TNF Human MAb
Goliumumab TNF Human MAb
Certolizumab TNF Peg-Fab’
Abatacept T-cell costimulation IgG-CTLA4 fusion
Rituximab B-cells Chimeric MAb
Anakinra IL-1 IL-1 receptor antagonist
Tocilizumab IL-6 Anti-IL6 receptor MAb

Mouse
Human
Chimeric
monoclonal
antibody
CDR
Infliximab
Human
recombinant
antibodies
Adalimumab
Humanized Fab’ fragment
Etanercept
Human recombinant
receptor/Fc fusion
protein
Fc
Receptor
Constant 2
Constant 3
PEG PEG
Certolizumab
VL VH
CL
CH1
Golimumab
TNFα Inhibitors
Adapted from Tracey D et al. Pharmacol Ther. 2008;117:244-279

Other Biologic Agents
Woodrick RS and Ruderman EM Nature Rev Rheumatol. 7:639-52 (2011)

vs
Risks of RA • Extra-articular disease
• Deformity/Disability
• Comorbidities
• Infections
• Mortality
Risks of Biologics • Injection site/infusion reactions
• Serious infections
• Opportunistic infections
• Lymphoma/neoplasia
• Autoimmune/lupus/MS
• Exacerbation of CHF
Making Sense of Safety

Summary from Product Label
Doubling of SIE* Rate With Biologic Use
SIE Rates (PI) Biologic Placebo
Anakinra 2% 1%
Adalimumab 2% 1%
Etanercept 1% 1%
Infliximab 5.3% 3.4%
Golimumab 1.9% 2.2%
Certolizumab 3% 1%
Abatacept 3% 1.9%
Rituximab 2% 1%
Tocilizumab 3.6 / 100py 1.5 / 100py SIE: Serious Infectious Event
HUMIRA (adalimumab) [package insert]. Chicago, IL; Abbott Laboratories; 2008; ENBREL (etanercept) [package insert]. Thousand Oaks, CA;
Immunex Corporation; 2006; REMICADE (infliximab) [package insert]. Malvern, PA; Centocor, Inc; 2007.

Rate
occu
rrin
g i
n R
A
po
pu
lati
on
6,7
Seri
ou
s i
nfe
cti
on
s (
even
ts/1
00 P
Y)
2
4
6
8
0
ETA4
4.2
IFX1
6
RTX5
4.7
ABA6
3.9
MTX7,8
3.8
ADA3
4.65
TCZ2
5.2
Rheumatoid Arthritis:
Serious Infections (RA Clinical Trials)
1. FDA Safety Review (online). 2. Smolen JS et al. Lancet. 2008;371:987-97. 3. Burmester G et al. Arthritis Rheum. 2008;59:32-41. 4. Zeichner JA et al. JAAD. 2006;54:S120-1. 5. Emery P et al. Arthritis Rheum. 2006;54:1390-400. 6. BMS document for abatacept (BMS-188667) Biological License Application 125118; 7. Singh G et al. Arthritis Rheum. 2002;46;2287-93; 8. Doran M et al. Arthritis Rheum. 2002;46:2287-93;

Biologic Comparative risks per 1000
(95%CI)
Control assumed risk = 26
Relative effect
OR (95% CI)
NNTH
(95% CI)
Abatacept 15 (8 - 28) 0.57 (0.30-1.08) NS
Adalimumab 29 (19 – 43) 1.12 (0.73-1.70) NS
Anakinra 28 (12 – 63) 1.08 (0.47-2.50) NS
Certolizumab 86 (41 – 172) 3.51 (1.59-7.79) 17 (7-68)
Etanercept 28 (19 – 39) 1.06 (0.74-1.51) NS
Golimumab 33 (19 – 59) 1.29 (0.71-2.35) NS
Infliximab 37 (26 – 54) 1.45 (0.99-2.13) NS
Rituximab 25 (17 – 38) 0.97 (0.64-1.48) NS
Tocilizumab 40 (22 – 73) 1.58 (0.85-2.94) NS
All biologics 31 (24 – 39) 1.19 (0.94-1.52) NS
Serious Infections with Biologics
Singh JA, et al. Cochrane Database Syst Rev. 2011 Feb 16;(2):CD008794.

Serious Infections With Anti-TNF Treatment
Frequency of Serious Infections in Anti-TNF-treated Patients
Observational RA Population N Rate/100
Pt-Yrs
Adjusted
Relative
Rate*
RABBIT: Listing et al., Arthritis Rheum 2005
64(9):1274–9 858 6.3 2.2
BSRBR: Dixon et al., Arthritis Rheum 2007;
56(9): 2896–2904 8659 5.5 1.2
ARTIS: Askling et al., Ann Rheum Dis 2007;
66:1339–44 4167 5.4* 1.4
Curtis JR, et al., Arthritis Rheum 2007;
56:1125–33 2393 2.9** 1.9
Schneeweiss S, et al., Arthritis Rheum
2007; 56(6):1754-64 469 2.2 1.0
* Compared with MTX- or DMARD-treated patients with RA

RCTs of TNF inhibitors in High Risk Patients#
SIE Outcomes
Study, yr Drug No. Wks DMARD
+Placebo
DMARD +
TNFi
STAR
2003 Adalimumab 636 24 1.3% 1.9%
START
2006 Infliximab 1084 22 1.7%
1.7% 3mg
(5% 10mg)
Weisman
2007 Etanercept 535* 16 3.9% 3.0%
# must have >1 comorbidity (eg, DM, COPD) *1000 pt study closed enrollment after 3.5 yrs for slow accrual
Usual doses did not increase the risk of SIE in patients w/ comorbidities.
Higher dose infliximab significantly increased SIE events
Furst, J Rheumatol. 2003 Dec;30(12):2563-71 Westhovens, Arthritis Rheum. 2006 Apr;54(4):1075-86 Weisman ME, et al. Rheumatology 2007:46:1122

Do TNF Inhibitors / Hospitalizations?
Wolfe, Arthritis Rheum. 2006;54:628-34. Curtis, Arthritis Rheum. 2007 56:1125-33.
Schneeweiss. Arthritis Rheum. 2007 56:1754-64. Suissa, Pulm Pharmacol Ther. 2008;21:234.
Grijalva CJ et al. JAMA. 2011 Nov 6
Author Type of
Hospitalization N RR 95%CI
Wolfe Pneumonia 16,788
1.2
0.8
1.1
0.9-1.4
0.6-1.0
0.6-1.8
Curtis Bacterial infx 5326 1.9 1.3-2.8
Schneweiss Bacterial infx 15,597 1.0 0.6-1.7
Suissa COPD 15,771 0.62 0.43-0.89
Grijalva SIE 10,484 1.05 0.91-1.21

SIE w/ Rituximab, Abatacept and Anakinra in RCTs
Source Biologic SIE Biologic(%) SIE Placebo(%) ORs (95% CI)
Edwards et al, 2004
RTX
6/121 (4.9) 1/40 (2.5)
1.45
(0.56 - 3.73)
Emery et al, 2006 4/316 (1.2) 2/149 (1.3)
Cohen et al, 2006 7/308 (2.3) 3/209 (1.4)
Total 17/745 (2.3) 6/398 (1.5)
Moreland et al, 2002
ABAT
1/90 (1.11) 0/32 (0)
1.35
(0.78 - 2.32)
Kremer et al, 2005 1/220 (0.45) 2/119 (1.7)
Genovese et al, 2005 6/258 (2.3) 3/133 (2.2)
Kremer et al, 2006 13/433 (3.0) 5/219 (2.3)
Weinblatt et al, 2006 28/959 (2.9) 8/482 (1.6)
Total 49/1960 (2.5) 18/985 (1.8)
Bresnihan et al, 1998
ANAK
5/351 (1.42) 1/121 (0.82)
2.75
(0.90 - 8.35)
Cohen et al, 2002 0/345 (0) 0/74 (0)
Cohen et al, 2004 2/250 (0.80) 2/251 (0.8)
Schiff et al, 2004 23/1116 (2.0) 1/283 (0.3)
Total 30/2062 (1.4) 4/729 (0.5)
Salliott C Ann Rheum Dis. 2009 January; 68(1): 25–32.

TNF Inhibitors and Risk of Septic Arthritis
• BSRBR: 191 septic arthritis among 11,881 anti-TNF and 3673
DMARD Rx patients
• Infectious risk greatest early
• Risk Factors: Prior joint replacement
0
0.0
00.0
10
.02
Cu
mu
lative
ha
za
rd f
un
ctio
n
Etanercept
Adalimumab
Follow-up (years)
Infliximab
nbDMARD
1 2 3
Ann Rheum Dis 2011 Oct;70(10):1810-4

0
10
20
30
40
50
60
70
80
90
100
Cum
ula
tive f
req
uen
cy o
f seri
ous in
f
% of severe
infections/
cycle
3 months 6 months 9 months 12 months
Duration between RTX infusion and serious infections
1st Cycle
2nd Cycle
Real World Infections (SIE) w/ Rituximab
• French AIR Registry
• 1303 pts (1.2 yr F/U)
• 82 SIE in 78 pts
• 5.0 SIE/100 pt-yrs
• ~50% w/in 1st 3 mos
• Predictors (OR):
– Chr. Lung Dz (3.0)
– Cardiac Insuff (3.0)
– Xtra-Artic Dz (2.9)
– HypoIgG before RTX (4.9)
Gottenberg JR, et al. Arthritis Rheum 2010

Serious Infection Risk Over Time
Decreased rate of serious infection over time in Japanese cohorts. Perhaps
better patient selection and/or monitoring?
Sakal R et al. Rheumatol Int. Published On-Line 2014

Infection Risk with RA Therapies
• Serious bacterial infections
– Incidence with biologics > DMARDs
– No direct comparisons between biologics agents
– Skin, soft tissue, and joints more common sites of infection
• Combined biologic therapy contraindicated
– Increased serious infectious events (SIEs) with combined use
– SIE etanercept + anakinra, 3.7%–7.4% vs etanercept alone, 0%
– SIE abatacept/biologic, 5.8% vs biologic alone, 1.6%
Furst DE et al. Ann Rheum Dis. 2007;66:2-22.
Genovese MC et al. Arthritis Rheum. 2004;50:1412-1419.
Weinblatt M et al. Arthritis Rheum. 2006;54:2807-2816.

RA and Serious Infections
The best predictors of serious infection
events (SIE) and infectious deaths:
1. RA severity/disease activity
2. Corticosteroid therapy
3. Comorbid diseases: CHF, CRF, IDDM,
COPD, etc.
4. Cutaneous barrier breakdown
(ulcers, wounds)
5. Joint surgery
Kaandorp CJ, Arthritis Rheum 1995;38:1819-25 Doran Fl. Arthritis Rheum 2002;46:2287-93

Community-acquired Pneumonia (CAP) in Elderly
11,241 individuals > 65 yrs, followed 2002 - 2005
CAP/1000 person-yrs
Elderly 14.0
Immunocompromised 30.9
Chronic lung disease 46.5
Long-term steroid Rx 40.1
NDB: 16,788 RA pts 17
Risk factors (HR ~2-4) Age, Pred, DM, MI, Lung Dz
Infectious risk is driven by age, severity, steroids, comorbidity
Vila-Corcoles A,; EPIVAC Study Group. Respir Med. 2008 Wolfe F, et al. Arthritis Rheum 54:628-34, 2006

Treatment Related Risk of SIE in RA
0
1
2
3
4
5
6
TNFi Pred High dose Pred
Hazard
ratio
Penn NDB Tenn

TNF inhibitors and Selected SIE in Elderly RA Medicare and Pharmacy Claims database
Age, gender
Adjusted HR
TN
F
Pneumonia 1.4 (0.7–2.9)
Bacteremia 1.0 (0.5–2.1)
Osteomyelitis 1.0 (0.3–4.3)
ST
ER
OID
Pneumonia 2.4 (1.3–4.2)
Bacteremia 2.9 (1.8–4.5)
Osteomyelitis 1.5 (0.6–4.1)
*HR compared with MTX initiation (alone or in combination)
Conclusions: • No increased risk in infections in patients on anti-TNF compared to MTX • Prednisone use confers significant, dose-related risk of infection
Schneeweiss S, et al. Arthritis Rheum. 2007;56:1754-64 .

Risk of Infection/Hospitalization with TNFi
• Retrospective cohort study: 4 US databases (1998–2007)
• SIE event rate in RA: TNFi 8.17 vs DMARD 7.66 per 100 pt-y; adj. HR 1.09 (95% CI 0.94–1.25)
• TNFi did not ↑ SIE/hospitalization, but IFX did ↑ SIE risk
SIE Hosp HR RA IBD SpA
TNFi 1.05 (0.91–1.21)
1.10 (0.83–1.46)
1.05 (0.76–1.45)
Prednisone 0–4 mg/d 1.32 1.09 1.13
Prednisone 5–10 mg/d 1.78 0.93 2.01
Prednisone >10 mg/d 3.95 1.38 2.77
Overall TNFi use not assoc with increased SIE (but IFX was) Prednisone increases
SIE risk in RA and SpA, but not IBD
NS
Courtesy TREG 2012
NS
Grijalva CJ, et al. ACR 2011, Chicago, #801

Serious Infection and Baseline
Disease Activity
• Data from BSRBR*
– DMARD n=1365
– ETN n=3470
• DAS28 ≤5: IR = 27.1/1000 pt-y
• DAS28 >6 & ≤7:IR=40.5/1000 pt-y
• DAS28 >8: IR = 64.2/1000 pt-y
• For every 1 point DAS28
– HR for SIE 17%
– HR 1.17 (95% CI 1.08–1.27, P<0.001)
– No difference between ETN or DMARD
Disease activity, not medication, determines risk of SIE
Infe
cti
on
rate
per
1000 p
t-y
20
60
≤4 6 7
DAS28
DMARD
ETN
TOTAL
40
≥8
80
70
50
30
10
0
5
BSRBR – British Society for Rheumatology Biologics Registers Emery P, et al. ACR 2011, Chicago, #429
Courtesy TREG 2012

Risk of Infection Augmented by Steroid
Dose, Biologics and Comorbidities
SIE risk augmented by Steroids, TNF inhibitor, comorbidity, prior SIE
Estimated Serious Infections per 100 Patient Years based on Risk Factors
• age >60 years, • chronic lung disease • chronic renal disease • high number of treatment • prior serious infections.
Strangfeld A, et al. Ann Rheum Dis. 2011 Nov;70(11):1914-20. Courtesy TREG 2012

RABBIT: Calculating the Risk of Serious
Infection (SIE) in the Next 12 Months
RA patient #1
47 yr. old woman has no
comorbidities, 2 prior DMARD
failures, has 3 tender and 3
swollen joints, HAQ = 0.5, and
takes MTX and prednisone 10
mg qday
SIE Risk = 1.4%
SIE Risk = 2.6% *calculated from http://www.biologika-register.de
RA patient #2
62 yr. old woman with COPD and
prior pneumonia has failed 6 prior
DMARDs/biologics, has 6 tender
and 6 swollen joints and HAQ=1.2
while taking leflunomide and
prednisone15 mg qday
SIE Risk = 28.4%
SIE Risk = 45.2%
Risk Calculated from Risk Factors
Age Pred # priorDMARDs Prior SIE Current Biologic
Cush JJ. ACR Drug Safety Quarterly 2013; 4 (4):1-3 Zinck A, Ann Rheum Dis.2013 Jun 28 Epub

High Risk RA Patients
Patient Profiling: SIE Risk Factors
• Elderly
• Hx of pneumonia
• Hx of septic arthritis
• Hx of smoking
• Hx of comorbidities – esp chronic lung disease
• > 10 mg/day prednisone
• Multiple DMARD failures
• High disease activity
• Those requiring higher TNFi doses
• Cytotoxics, cyclosporine

Serious Infections Are Usually Multifactorial
• RA (inflammation/debility)
• Comorbidities
• Steroid use
• Advanced age
• Biologic use
– small, significant 1-2X risk
– occurs early (1st 6 mos)
• Inflammation augmented;
• Depletion of susceptibles
– higher doses (TNFi)
RA Activity
Comorbid
Diseases
Drugs
(steroids, biologics)

Summary
• Best way to avoid serious infections:
– Employ screening measures (when possible)
– Rigorous Patient selection
– Vaccination where appropriate
– Avoid or lower corticosteroid use
– Maintain optimal disease control
– Monitor signs and symptoms periodically

½ life 5x ½ life
102 hrs 21d
(3wk)
210 hrs 44d
(6wk)
2 wks 70d
(10 wk)
How Long Before Major Planned Surgery
Would You Cease/Hold TNFi?
How long would you
stop before surgery?
etanercept 1.72 wks
infliximab 4.05 wks
adalimumab 2.47 wks
Cush JJ. Ann Rheum Dis 2005;64 Suppl 4:iv18-23.

Perioperative Infectious Risk
• 37,137 patients; 50,359 orthopedic
surgeries over 8 y
• Inflammatory arthritis (IRD) vs other
• 422 perioperative infections
– 2% in IRD vs 0.8% in “other”
– OR: 2.58; 95%CI 1.9, 3.5; P<0.001
• Periop infections higher with TNFi
– OR: 2.6; 1.1, 6.2; P=0.027
• 10x higher risk within 1 dose interval
(OR 10.0) (81% inflix)
Risk in relation to When TNFi D/C
IFX
3–5 mg/kg
BW
-200 0
Time-lag of last dose (days)
-250 -150 -100 -50
Infection
No infection
ADA
40 mg
-200 0 -250 -150 -100 -50
Infection
No infection
ETN
50 mg
-200 0 -250 -150 -100 -50
Infection
No infection
ETN
25 mg
-200 0 -250 -150 -100 -50
Infection
No infection
Orthopedic surgery appears safer
after 1 skipped dose
Scherrer CB, et al. ACR 2012, Washington, # 1669. Courtesy TREG 2012

Surgery - Recommendations
• Surgical site infx risk higher w/ TNF inhib
(OR 5.3-5.7)
• Risk of infection is greatest: after administration
(peak drug levels?) or when TNFi Rx washed-out
(inflammation risk)
1. Do not do surgery at peak drug levels
2. Do not do surgery at nadir of therapy
3. Suspend TNFi for one dosing interval (or 4 wks)
– Etanercept > 1 week
– Adalimumab > 2-4 weeks
– Infliximab > 4-8 weeks * Synthesis of 7 retrospective studies Mornohara M, et al. Mod Rheumatol. 2011 Feb 12. Giles JT, et al. Arthritis Rheum 2006;55(2):333-7.
Den Broeder AA. J Rheumatol. 2007;34(4):689-95. Dixon W, et al EULAR 2007, OP0215

Tuberculosis Risk
TB Risk Augmented by:
• Host factors (HIV, Prison)
• Geography/environment
• Exposure
• Drugs (TNFi > biologics)
• Number needed to Harm
– 681 (95% CI 143,14706)
compared to control
RA
+TNF
Relative Risk
9
2
1
30
Korea Sweden
RA
No TNF
RA
No TNF
RA
+TNF
NL NL
TNFi risk
4-9 x in low
risk populat.
TNFi risk
30 x in high
risk populat.
1. Winthrop K. EULAR 2005, #SP0005; 2. Askling J, et al. Arthritis Rheum 52:1986-92, 2005 3. Seong SS, et al. 2007 Apr;34(4):706-11; 4. Singh JA, et al. Cochrane Reviews 2011

Latent Tuberculosis
Risk Factor LTBI Prevalence
Close TB contact 37%
Homeless 13-32%
IV Drug users 14-28%
Foreign born 19%
Prisoners 2-17%
Progression LTBI to Active TB
Risk Factors RR
HIV 9.9
Close TB Contact 6.1
CXR TB findings 5.2
Pred > 15mg/d 2.8
CRF 2.4
TNF inhibitor 2.0
IDDM (poor control) 1.7
Smoking 1.5
Horsburgh CR, Rubin EJ, NEJM 2011: 364: 15

0
2
4
6
8
10
2 4 6 8 10 12 14 16 18 20 22 24 26 28 >28
Weeks of Infliximab Exposure
Num
ber
of cases
TB Following Infliximab Exposure
*Data reported for 57 patients, most of whom had received monthly infusions of infliximab.
Keane J, et al. N Engl J Med. 2001;345:1098-1104.

TB Screening Before Adalimumab Therapy
in North America and Europe
# cases 7 27
Exposure
(pt-yrs)
534 14,010
1.3
0.19
0.0
0.5
1.0
1.5
2.0
Pre-Screening Post-screening
Eve
nts
pe
r 1
00
-pt-
yrs
# cases 5 22
Exposure
(pt-yrs)
5919 8091
0.08
0.27
0.0
0.5
1.0
1.5
2.0
US/Canada Europe/Australia
Eve
nts
pe
r 1
00
-pt-
yrs
Perez J, et al. EULAR 2005, #OP0093

TB Screening Protocols in Spain
Carmona L, et al. Arthritis Rheum 52:1766-72 (2005)
Patient-years of
exposure to TNF
antagonists
No. of active
TB cases
Active TB rate
per 100,000
(95% Cl)
All TB cases
Pre-OR 6,126 32 522 (369-738)
Post-OR 1,699 2 117 (29-470)
IRR recommendations‡ - - 0.22 (0.03-0.88)
TB cases with RA only
Pre-OR 4,780 27 564 (387-823)
Post-OR 1,049 1 95 (13-676)
IRR recommendations‡ 0.17 (0.004-1.02)

Non-Tuberculous Mycobacterial (NTM) Infections
are More Common than mTB
• 29,500 new users of TNF inhibitors
among 3 databases (2000-07)
• 24 new NTM and 11 TB cases
• NTM Sx: fever cough malaise
• Most common sites: pulm, LN, skin,
soft tissues
• NTM more common than TB among
these RA patients
0
10
20
30
40
50
60
70
80
Rate
pe
r 1
00
,000
pt-
yrs
Rate per 100,000 pt-yrs
US TB TB NTM
Winthrop KL, et al. ACR 2010, Atlanta, #404 Winthrop KL, et al. Emerg Infect Dis. 2009 Oct;15(10):1556-61.
• Medwatch: 239 NTM reports, 105
(44%) met NTM disease criteria
• Median age 62 yrs; 65% female, and
70% had RA
• Assoc. w/ inflix (n = 73), etan(n=25),
ADA (n = 7)
• 44% extrapulmonary
• MAI 50%
• 9% died

Who Should Undergo PPD Testing?
Per Product labeling
– All TNF inhibitors
– Abatacept
– Tocilizumab
– Leflunomide
– Tofacitinib
NOT REQUIRED
– MTX
– Anakinra
– Rituximab
– Apremilast
Given likelihood of progression to biologic use, screening at
initiation of MTX therapy may be an efficient approach

Screening for Mycobacterium Tuberculosis Infection
1. Everyone should be screened for LTBI prior to TNFi use (PPD, IGRA)
2. IGRA indicated? When available; when there is a hx of BCG vaccine
3. BCG vaccinated should be tested for LTBI; positive results most likely mean infx
4. Either PPD or IGRA positivity is evidence of infection
5. PPD are good for up to a week (72 hrs is optimal)
6. Concordance between PPD & IGRA is poor (kappa ~0.3)
7. 2 step TST is only rec in health care workers at the time of hire
8. CXR is only helpful in diagnosing active TB (not screening)
9. PPD testing should be repeated or done periodically (twice & when risk changes)
6-10% of patients originally negative will be positive on repeat (anergy vs new?)
10. Pts w/ documented hx of adeq. Rx LTBI or active TB can safely recv TNFi Rx
11. Pts w/ secondary LTBI (PPD or IGRA) should have culture to exclude active TB
12. LTBI: “preventive anti-tuberculous therapy must be initiated before giving TNFi”
13. Surprisingly low frequency of INH hepatitis in our pts (Labs monthly x3)
14. Guidelines do not recommend screening for MTX, DMARDs (PI says yes LEF)
Cush JJ, Winthrop K, Dao K, Chaisson R. ACR Drug Safety Quarterly June 2010

TST vs IFN Gamma Releasing Assays
in Low Risk Populations
TST IGRA
Use Low risk
pop.
↑risk recent infx
BCG hx
Unreliable pt
Sensitivity 90-100% 80-90%
Specificity 29-39% 56-83%
PPV 2.7-3.1% 4-8%
NPV 99-100 99-100
TST+ IGRA+ ++
LTBI Horsburgh CR, Rubin EJ, NEJM 2011: 364: 15
Bartalesi Eur Respir J 2009; 33:586-593

Utility of Repeated TB Testing
• 411 pts on TNFi Rx (11/00 - 6/09)
from LA county hospital
• New PPD positives
– ~10% on annual testing
• Most initially anergic
• Some are new infections
• 7/30 Culture positive
• Conclusion: Repeat testing for
TB appears to be useful
• New TB infection is possible
411 on TNFi
382
Baseline TST
282
TST negative
149 rescreen x 1
74 rescreens x 2
11 rescreens x 3
100
TST+ (INH)
21+
8+
1+
30 Cooray D, et al. ACR 1153, 2009

Serial Quantiferon-TB gold testing: conversions detected over
2 years in the CT-P13 biosimilar development programme
• CT-P13 (IFX) approved by EMA in 17 countries (PLANETAS & PLANETRA RCTs)
• QFT at Week 0, 62 and 110 low risk vs Weeks 14, 30, 54, 62, 110 high-risk nations
• 476 enrolled: 458 were QFT‒ at baseline 16.6% (n=76) conversion to QFT+
• 73% Rx for
LTBI
• 9 neg ReTest
Countries
by risk
TB incidence
per/100,000
Secondary
conversion
Week 62
converts
Week 110
converts
Very low 0‒19 9.3% 9.3% 0
Low 20‒49 11.4% 8.5% 3%
Intermediate 50‒124 21.7% 19.6% 2.1%
High >125 52% 48% 4%
Serial QFT assessments do identify
new cases of LTBI or active RA. The
risk of new conversions depends on
residence and endemic risk
Park W, et al. EULAR 2014, Paris, #FRI0281

New Issues with TB Testing
• Worry about nTM more than mTB
• Everyone gets Tested – TST/PPD or IGRA
• Super Positives always indicate infection
• +Test Sxs + CXR + Culture (if on TNFi)
• Do repeat x 1 and when risk changes
– IGRA not valid as repeat
• “Indeterminant” repeat
– 5%: most due to Steroid use (turn negative w/ Rx)
• Shorter regimens (RIF x 4m) preferred to INH x9

Opportunistic Infections: Case Reports
• Histoplasmosis1
– 10 cases, 9 with infliximab
• Listeriosis2
– 15 cases, 14 with infliximab
• Sporotrichosis3
– Single case report
• Aspergillosis4
– Case report following loading dose of infliximab - Proposed source: construction at medical center
• Pneumocystis5
– 10 cases with infliximab, 3 deaths
• CNS Toxoplasmosis6
– 4 cases
• Coccidiomycosis7
– 13 cases with infliximab 1. Lee et al., A & R, 2002; 2. Slifman et al., A & R, 2003; 3. Gottlieb et al., Clin Infect Dis, 2003; 4. De Rosa et al., IDSA, 2002;
5. Velayos and Sandborn, Inflam Bowel Dis 2004; 6. Lassoued et al., Semin Arthritis Rheum 2007; 7. Bergstrom et al., A & R, 2004

High Death Rates with Opportunistic
Infections and Biologic Use
• Rare events
• Severity of the disease (both RCTs/Practice)
– More comorbidity in Practice
– Contributions of steroids and other agents?
• Severity of SIE/opportunistic infection
– Unusual presentations
• More disseminated & localized infections
– Delays in diagnosis
• SAE & SIE closely monitored/reported in RCTs
Tsiodras S, et al. Mayo Clin Proceed 2008; 83:181

Fungal and Opportunistic Infections
with Biologic Use
• NO Screening measures!!
– RELY ON SUSPICION AND SIGNS AND
SYMPTOMS
• Patients living in endemic areas are at risk
• Opportunistic infection are severe and deadly
– Rare events, unusual presentations & delays in
diagnosis
• More disseminated & localized infections
• FDA : ‘Clinicians should consider initiating empiric
fungal therapy while evaluating at-risk individuals
with undiagnosed systemic illnesses’ Diak P et al., FDA 2008
Tsiodras S, et al. Mayo Clin Proceed 2008; 83:181

Listeriosis and Biologics
• Analysis of FDA AERS 2004 – 2011
• 266 cases or Listeria monocytogenes
– Median Onset time 184 days
– Mortality rates 11.1% (ADA) – 27.3% (RTX)
• Presents w/ fever, fatigue, myalgias, GI symptoms (N/V/D),
meningitis and other CNS symptoms
Drug Use • INFL (77.1%), ETN (11.7%)
• ADA (9.8%), GOL (0.4%)
• Rituximab (4.1 %)
• Abatacept (0.4 %)
• Steroids (56%) MTX (31.6%)
Indications • 47.7 % Rheumatologic
• 38% IBD
• 3.4 % Hematological dz
• 10.5 % Other s
Bodro M, Eur J Clin Microbiol Infect Dis. 2013 Apr 9. [Epub ahead of print]

CDC: Shingles, Zoster Vaccine & RA
• Shingles: 1 million/yr (1/3 life risk)
• Zostavax: since 2006
– 51% reduction in VZV, 67% reduction in PHN (postherpetic neuralgia)
• Indicated in adults > 60 yrs
• OK in on MTX, AZA, pred <20/d
• NOT for acute zoster or PHN
• NOT w/ Recombinant biologics
• Give 2 wks before, 4 wks after anticipated immunosuppression
Cush, Calabrese, Kavanaugh ACR HOTLINE 2008

Herpes Zoster and RA
• Incidence of HZ in seniors with
RA = 6.5 events/1000 pt-y1
– Prednisone increases the risk1
• Anti-TNF increases risk of HZ
infection compared to DMARD2
– HR: 2.2 (1.4–3.6)
• Current DMARD, steroid use and TNFi increase risk of H. zoster infection
• Consider VZV vaccination in all RA patients
≤5 mg/day 1.77 (1.56–2.01)
6–9 mg/day 1.61 (1.26–2.05)
10–19mg/day 2.13 (1.82–2.49)
≥20 mg/day 2.90 (2.44–3.44)
Past use 1.39 (1.27–1.52)
Risk of H. zoster
Infection2
0 1 3 4 5
5
0
2
Follow up (years)
Cu
mu
lative
in
cid
en
ce
p
er
100 p
ts f
ollo
wed u
p
INF
ADA
ETN
DMARD
P=NS
1Widdifield J, et al. ACR 2010, Atlanta, #341; 2Galloway J, ibid, #421. SLIDE COURTESY OF TREG2010

Biologics and Vaccination
• RA patient have lower responses than controls
• Humoral responses to influenza and pneumococcal vaccines are not affected by prednisone, MTX, TNF inhibitors, abatacept
• Blunted vaccine responses with rituximab
– Give vaccination prior to use of rituximab (tocilizumab)
• PDR: says do not vaccinate with live vaccines
• Live vaccine use requires cessation of Biologic for >4 weeks and waiting for 2-4 weeks after vaccination before starting the biologic agent
Fomin I, et al. Ann Rheum Dis 65: 191-4, 2006 Kapetanovic MC, et al. Rheumatol 45:106-11, 2006

Inactive Vaccines* Live Vaccines
Influenza (IM)
Typhoid (IM)
Tetanus/diptheria/pertussis
Pneumococcal (23/7valent)
Human papilloma virus
Hepatitis B
Hepatitis A
Hemophilus influenza B
Meningococcus
Rabies
Influenza (nasal)
Typhoid (po)
Yellow fever
Varicella [Varivax] [Zostavax]
Measles, mumps, rubella (MMR)
BCG (bacillus Calmette-Guerin)
Polio (po)
Smallpox
Anthrax
HPV (Gardisil): approved for use in girls age 9-26 yrs. Not indicated in older Or Pts with active HPV warts or Cervical Cancer H Zoster: recommended for >60 yrs who are immunocompetent, w/ prior H Zoster, “anticipated immunosuppression”. Cautioned against use w/ TNFi (but pre, MTX OK)
* component / toxoids / inactivated / killed) Kavanaugh, A Curr Opin Rheumatol 2009

Can you Treat Resolved HBV w/ TNFi?
(HBsAg-, HBcAb+)
• TNFi Rx pts may not be adequately HBV tested (~25%)
• HBV activation can occur w/ HBsAg+;
• Risk may also occur w/ resolved infx HBsAg-, HBcAb+ (± anti-HBsAb+)
• TNFi can be safely used in pts with resolved HBV infection
• Screening for HBV, HCV and monitoring of LFTs is strongly advised
Reactivation risk in inactive HBV (HBsAg-, HBcAb+)
Author/ year N Reactivation
Charmin 2009 21 0/21
Bobbio 2009 69 0/69
Chung 2009 8 1/8
Vassilopoulous 2010 19 1/19
Caporali 2010 67 0/67
Cassano 2011 62 0/62
= 2/246 had
reactivation w/ TNFi
exposure
Vaughn Inflamm Bowel Dis. 2011 Sep 26; Charpin Arthritis Res Ther. 2009;11:R179 Bobbio-Pallavicini F, et al. ACR 2009; Vassilopoulous ARD 69:1372, 2010; Caporali R. Arth Care Res 62:749, 2010; Cassano J Biol Regul Homeost Agents. 2011;25:285

Indication HBsAg
Status Rx Exposure
HBV reactivation
No Lamivudine Prophylaxis
RA 9
CD 8
SpA 5
18/20 +
(2 NA)
14 INF
5 ETA
1ADA
3 ADA/ETA
6 wks - > 2 yrs 14/22
+ Lamivudine Prophylaxis
RA 3
CD 1
SpA 2
6/6 +
3 INF
1 ETA
2 INF/ADA
7 mos - > 2 yrs 0/6
HBsAg+ and TNF Inhibition
Aliment Pharmacol Ther. 2010 Jan;31(1):20-34..

Risk of Hepatitis B Reactivation
• Abatacept in RA – 8 patients found to
be HBsAg+
– 4 recv etanovir no reactivaton
– 4 recv NO Anti-Viral Rx 4/4
reactivation
• RTX in CD20(+) Diffuse lg B-cell
lymphoma
• Rx w/ CHOP vs R-CHOP.
• 104 pts between 2003-2006
• ?RTX in pts who resolved HBV infx
(neg. HBsAg; postive HB core
• reactivation only in RTX pts (24%)
46 pts HBsAg neg/HBc pos
CHOP R-CHOP
N 25 21
Reactiv-ation 0 5
Caution w/ HBcAb+ and intense
immunosuppression
Avoid biologics or use antiviral
prophylaxis if HBsAg+
Kim PS, et al. ACR 2011, Chicago #2238;
Yeo W, J Clin Oncol. 2009 27:605

Strategy in HBV Infected Patients Requiring
Immunosuppression
• Screen high risk patients
• HBV Screen : (HBsAg, anti-HBc and follow up
with HBV-DNA viral load if appropriate
• HBsAg + CAUTION; Avoid biologics
– TNF inhibitors, RTX, abatacept
– Refer to hepatology for pre-emptive anti-viral Rx
• Resolved HBV infection (HBsAg- and HBcAb+)
may receive biologics w/ caution
• Caution in those w/ most intense forms of
immunosuppression who are HBcAb + patients
Winthrop KL, Calabrese LH. Ann Rheum Dis. 2011;70:1701-3

Patients who should NOT receive
TNF inhibitors!
Infectious Scenario Comment
1. Active Hepatitis* HBsAg+ at greatest risk
2. Nontuberculous
mycobacterial (NTM)
infection*
Despite anti-mycobact. Rx,
never fully eradicate NTM
3. Invasive fungal infection* Difficult to fully eradicate,
reactivation common
4. Intravesicular BCG
treatment
TNF inhibitor use may
potentially lead to
mycobacterial infection
* if absolutely necessary, consider chronic prophylaxis w/ biologic

TNF Inhibitor Use
Difficult Situations
Not Safe to Use Probably Safe to Use
Hepatitis B*
Atypical mycobacterial
infx*
Invasive fungal infection*
Pts receiving BCG therapy
Resolved HBV
(HBcAb+)
Prior treated
LTBI/mTB
Hepatitis C
HIV+
* If absolutely necessary, consider chronic prophylaxis with TNFi

Progressive Multifocal
Leukoencephalopathy (PML)
• Rare fatal demyelinating disorder JC polyomavirus
• PML Sxs: hemiparesis, cognitive/AMS, discoordination, apathy. – Dx: MRI lesions, PCR of CSF
• @risk: conditions that affect cell-mediated immunity – AIDS, Leukemia/ lymphoma , organ transplants, chemotherapy
– FDA Warns of Rituximab, Efalizumab, Natalizumab, Mycophenolate
• Autoimmune pts (noHIV/Cancer), incidence = 0.2 per 100,000 – Rheumatoid arthritis
= 0.4 per 100,000
– SLE = 4.0 per 100,000
• Role testing for JC virus?
Exposed N Rx Death
Biologics 15 14 RTX (4 mono)
6 TNF inhib* 7/10
DMARDs 19 14 Alkylating Rx
14/34 AZA 6/34MMF 10/19
* 5 prior to RTX use FDA Drug S afety Newsletter Fall 2007 Molloy, Calabrese. Arthritis Rheum. 2012 Sep;64(9):3043-51

Multifocal Leukoencephalopathy
With Selected Rheumatic Diseases
• Incidence & risk factors for PML in pts RA, PsA, PSO, JIA, IBD, AS
• Claims data from Medicare and Medicaid Services from 2000–2009.
• 53 PML cases were identified among 2,030,578 patients with
autoimmune diseases
– Prevalence of 2.6 per 100,000 patients.
– Most PML cases HIV and/or Cancer.
– Nine PML cases had received biologic prior to PML hosp.
• 6 had HIV or Cancer
• 3 were previously exposed to rituximab or 6 infliximab
– Autoimmune pts without HIV/Cancer, incidence = 0.2 per 100,000
• Rheumatoid arthritis = 0.4 per 100,000
• SLE = 4.0 per 100,000
• FDA Warnings: Rituximab, Efalizumab, Natalizumab, Mycophenolate
Bharat A, et al. Arthritis Care Res 2012; 64:612–615 Molloy E, et al Arthritis Rheum. 2009;60:3761-5.

Cancer & Biologic Therapies
What is the Concern?
• Prior Hx of Lymphoma
• Prior Hx of Any Cancer
• Family Hx of Cancer
• Cancer onset while on biologic Rx
• Does continued biologic use alter
cancer mortality

TNF Inhibitor Package Inserts
• More malignancies (lymphomas) where noted in TNFi treated patients compared to placebo treated patients.
• Lymphoma & other malignancies, some fatal, have been reported in children/adolescent pts treated with TNFi.
• Risks and benefits of TNFi should be considered prior to initiating therapy in pts with a known malignancy (other than successfully treated non-melanoma skin CA) or when continuing a TNFi in pts who develop a malignancy.
• Acute & chronic leukemia has been reported w/ post-marketing TNFi use; RA pts may be at higher risk (~2-fold) for leukemia.
• Role of TNF blocker in developing malignancies is not known.
• Pts on chronic immunosuppressives or Pso pt w/ Hx PUVA should be examined for presence of NMSC before/during Rx...
HUMIRA [package insert]. Abbott Laboratories; 2011; ENBREL Amgen 2011; REMICADE and SIMPONI Centocor, Inc; 2011; CIMZIA, UCB,
2011;

Other Biologics Package Inserts
• Rituximab: is indicated for Rx of CD20+ NHL
– PI does not discuss further neoplastic risk w/ RTX
• Abatacept: in PCT overall malignancies were similar b/w ABA
& placebo pts (1.3 vs 1.1%).
– But more cases of lung CA ABA (4) vs Placebo (0)
– Lymphoma SIR = 3.5
• Tocilizumab:
– In PCT overall malignancies were similar b/w TCZ & placebo pts
(1.32 vs 1.37/100 pt yrs)
• Tofacitinib:
– 11 solid tumors and 1 lymphoma in 3328 pts, 0 in 809 placebo pts
– Post-viral lymphoproliferative disorders seen in transplant studies
RITUXAN, Genentech 2011; ORENCIA BMS 2011; ACTEMRA, Roche 2011; XELJANZ Pfizer 2014

Lung
Lymphoma
Melanoma
NMSC
Colon
Breast
RA
Rheumatoid Arthritis and Neoplasia
• Cancer Not Increased in RA – Decreased rates of adenocarcinoma
(colon), Breast cancer
– Increased rates of lung cancer,
melanoma and nonmelanomatous
skin cancers
• Increased lymphoma risk: – Long-standing, active RA
– Older
– Rx w/ immunosuppressive therapy
– Patients receiving TNF inhibitors

Lymphoma Risk Rises w/ Increasing Activity
181
65
OR
(9
5%
CI)
6055504540353025201510
9 / 11 / 34 7 / 38 14 / 36 16 / 39
Case / Controls* Odds ratio (OR) and 95% confidence interval (CI)
9 / 36 18 / 38 27 / 36 35 / 37 226 / 37
50
Re
lative
Ris
k
Years
Lymphona
Cancer
overall
3.5
4
3
2.5
2
1.5
1
0.5
0
≥10 4-<10 0-<3 0-<3 3-<6 6-10y
Lymphoma Risk Begins After RA Onset
RA onset
Smedby KE, et al. J Intern Med. 2008 Dec;264(6):514-27. Hellgren Arthritis Rheum. 2010 May;62(5):1252-8

Solid Tumor Risk with TNF Inhibitors
Cush, Dao, Kay. Drug Safety Quarterly. 2012.

Lymphoma with TNF Antagonists
Clinical Trials
Etanercept Infliximab Adalimumab
N
Pt-Yrs
3389
(8336)
1298*
(2458)
2468
(4870)
Lymphoma (N) 9 4 10
Hodgkin's/
Non-Hodgkin's† 3/6 1/3 1/9
SIR Lymphoma
(95% CI) 3.47
(1.6–6.59)
6.4
(1.7–16.3)
4.35
(2.6–10.0)
*Rheumatoid arthritis only. †Majority diffuse large B cell.
FDA 2003

Cases, no.
(%)
Controls, no.
(%)
Unadjusted OR
(95% CI)*
Inflammatory
activity
Low 94 (25) 278 (74) 1 (referent)
Medium 196 (52) 94 (25) 7.7 (4.8-12.3)
High 86 (23) 4 (1) 71.3 (24.1-211.4)
Functional class
I 34 (9) 138 (37) 1 (referent)
II 185 (49) 204 (54) 3.9 (2.4-6.3)
III 105 (28) 31 (8) 13.8 (7.2-26.2)
IV 52 (14) 3 (1) 67.5 (18.9-239.8)
Lymphoma Risk in RA Associated with
Disease Activity and Functional Class
Baecklund E, Arthritis Rheum 2006;54:692-701

BSRBR –
Incident Cancers from >14,000 RA pts C
um
ula
tive
In
cid
en
ce
16%
14%
12%
10%
8%
6%
4%
2%
0%
0 1Years since registration
2 3 4
DMARD
Anti-TNF
10735 pts TNF exposed
WG Dixon et al. Arthritis Care & Research 2010;62:755-763.

0
10
20
30
40
50
60
70
80
90
100
TNFi DMARD
Cru
de
Recu
rre
nce
rate
/10
00
pt-
yrs
RABBIT: Risk of Incident and Recurrent CA
• 2001-06: 5279 pts enrolled
• No increase in cancer on TNFi in
nested case control study
• Prior malignancy in 122 pts
– 67 received biologic
• 9 recurrence of tumor (13.4%)
– 55 received DMARD
• 5 recurrence of tumor (9.1%)
• CA risk w/ age, activity, COPD
Strangfeld A, et al. Arthritis Res Ther. 2010;12(1):R5.

ARTIS Registry: TNF Inhibitor Therapy in RA and Overall Malignancy Risk
• 66,995 Swedish RA 1998 - 2006
• 6,403 treated with TNF inhibitor
• Followed for up to 8 years for a
primary cancer
• Conclusions
– Lower mortality risk among patients
treated with TNF inhibitor therapy
compared to biologic-naïve patients
– Lack of trend in overall cancer risk
following TNF therapy, either from
time since initiation or with cumulative
exposure
Time since Start of First TNF Inhibitor (years)
0
0.2
0.6
0.4
1.0
1.2
1.4
1.6
Mortality Risk in TNF Inhibitor–treated vs. Biologic-naïve Patients
RR
0
0.2
0.6
0.4
0.8
1.0
1.2
Cancer Risk from Start of TNF Inhibitor Therapy
RR
<1 1-2 2-3 3-4 4-5 5+ 0
0.2
0.6
0.4
0.8
1.0
1.2
Cancer Risk from TNF Inhibitor Cumulative Exposure
RR
0.8
J Askling et al. Ann Rheum Dis 2008;67(Suppl II):52;
LTH Jacobsson. Ann Rheum Dis 2008;67(Suppl II): 183.

Risk of Lymphoma
• 3 cohorts of patients
– Swedish nationwide inpatient registry (prevalence cohort)
– Incident cohort of early RA
– TNF-related cohort
• All cohorts were linked to nationwide cancer registry
RA cohort n RA patient type RR vs general
population
Adjusted RR vs
prevalent RA
In-patient
registry 53,067 Prevalent 1.9 (1.7–2.1) 1.0
Early RA 3703 Incident 2.0 (1.0–3.5) 0.8 (0.4–1.4)
ARTIS* 4160 Anti-TNF
treated 2.9 (1.3–5.5) 1.1 (0.6–2.1)
ARTIS = TNF inhibitor-treated cohort, identified within framework of a structured
monitoring program for biologics in RA
Askling J, et al. Ann Rheum Dis, 2005.

Hepatosplenic T Cell Lymphoma
• HSTCL: very rare, aggressive, often fatal NHL
– Affects kids and young adults (<30yrs) - usually fatal
– <200 documented cases in literature
– Common w/ transplant, AZA, cyclosporine (not MTX)
– Sxs: HSmegaly, fever, purpura, cytopenia, LFTs (-LN)
– Associated with AZA, 6MP
• Infliximab: 6 cases; 5 deaths (all post-marketing)
– All with Crohn’s disease; all on AZA, 6MP
– Ages 12 – 31 years; 5 Male, 1 Female
• Adalimumab: 8 cases, 4 deaths
– 2 RA: 61 & 70 yrs age
http://www.fda.gov/Drugs/DrugSafety/ucm250913.htm

Cancer Outcome in RA Pts
Rx w/ TNF Inhib.
RA 78,483
TNFi+ 8,562 TNF- 69921
1st CA 314 1st CA 4650
Dead 113
(37%)
Dead 256
(44%)
TNFi+ RR 95% CI
All death 1.1 0.8-1.6
Colon 0.7 0.34-1.58
Breast 0.7 0.05-10.2
Prostate 0.6 0.11-2.96
Lung 0.8 0.54-2.39
Melanoma 1.3 0.31-5.29
• Swedish biologics register 1999-2007
• 3 RA Registries: Swedish RA registry,
ARTIS biologics register, Swedish
Cancer register
• TNFi RR of death = 1.1 (95 CI: 0.8-1.6)
– 0.8 (95%CI, 0.5-1.2)
Raaschou P, Askling J. Arthritis Rheum. 2011 Jul;63(7):1773-5.

Tofacitinib and Lung Cancer Risk
FDA Advisory Committee Meeting, 2013

Tofacitinib Overall Cancer Risk
FDA Advisory Committee Meeting, 2013

Tofacitinib: Malignancy Analysis
• RCTs of tofacitinib (previous slide)
• 107 malignancies (excluding non-
melanoma skin cancer [NMSC])
• Most common: lung breast cancer
• 10 lymphomas
• Overall IR for all malignancies
(excluding NMSC): 0.85 (95% CI
0.70–1.02); lymphomas: 0.08
(0.04–0.14)
• Standardized IR (SIR) lung cancer:
1.91 (1.22–2.84), breast cancer: 0.77
(0.46–1.20)
• SIR vs SEER
– All malignancies: 1.08 (0.89, 1.31)
– Lymphomas: 2.58 (1.24, 4.74)
0.5
1.0
1.5
0-6
0.0
2.0
6-12 12-18
Time period (months)
Rate
/10
0 p
t-y o
f observ
ation
(95%
CI)
18-24 24-30 30-36 36-42 >42
UPDATE 2014
Mariette X, et al. EULAR 2014, Paris, #THU0147

Is there a Cancer Risk w/ Biologics?
Cancer Risk
From Rheumatoid From TNFi
Cancer overall None None
Lung,Skin,Lymphoma Increased Increased
Melanoma, Leukemia Possibly increased Possibly increased
Breast, Colon Decreased Decreased
Recurrence rates ??? Unchanged
Is it RA or the Drug ?
Arthritis Res Ther. 2010 Jan 8;12(1):R5 Smitten A, et al. Arthritis Res Ther. 2008;10:R45., Askling J, et al EULAR 2007, Barcelona, #OP0013 Dixon WG, et al. ACR 2008, San Francisco #1264 Hawkins-Holt,Hochberg, Cohen, Michaud,Wolfe ACR 2003 Abstr 806

Reducing Risk of Neoplasia
Neoplasia Measures to Risk/Monitor
Cancer Screening Health maintenance
Skin Cancers Hx, skin examinations
Lymphoma Pt. selection: age, activity, hx
Breast cancer Self exams, mammography
Prior Cancer Time, Oncologic F/U, Screens
Rheums should treat RA; Leave cancer to the oncologist
(can the oncologist manage RA?)

SIE Risk Reduction with Biologic Rx
Patients @ Risk Screening Measure Prevention
Pneumonia
Elderly, hx of
pneumonia, tobacco,
comorbidity, steroid use
Patient history,
Physical Exam, CXR
if Signs/Sxs
Pneumovax
Smoking
cessation,
steroid, COPD
Rx
Tuberculosis High risk groups, +PPD PPD,
IFN releasing assay
Prophylax or Rx
TB; steroid
Opportunistic
infections
High risk groups
(Endemic, Prior OI)
CXR if Signs/Sxs or
endemic
Avoid biologic or
use chronic
prophylaxis;
Empiric Rx

TNF Inhibitors and Serious Skin
Reactions Following anti-TNF Use
FDA data – 1998-2006 (2002-2006 for adalimumab)
EM SJS TEN Death
– Etanercept: 22 pts 13 4 5 1
– Infliximab: 21 pts 15 5 1 1
– Adalimumab: 8 pts 5 2 - -
• Most pts (>2/3) took TNFi for treatment of RA
• ~50% of etan/inflix pts needed hospitalization
• Median onset since 1st dose: 28 to 60 days
EM – erythema multiforme; SJS – Stevens-Johnson syndrome;
TEN – toxic epidermal necrolysis
US Food and Drug Administration. FDA Drug Safety Newsletter. Winter 2008;1(2).

Psoriasis as a Complication of
TNF Inhibitor Use
• Hundreds of case reports have shown psoriasis to be an adverse
event associated with anti-TNF therapy
– Occurs w/ all marketed TNF agents
– Reported in RA, IBD, SpA, PSO
• ~1 per 1000 pt-years TNFi exposure
• 50% pustular
• 40% plaque
• scalp, erythrodermic variants
• Majority improve psoriasis w/ TNFi D/C
– 1/3 improve w/ continued therapy
or change in TNF blocker
Harrison, et al. Ann Rheum Dis. 2009;68:209-15.; FDA Bulletin 2009.;
Cullen. Aliment Pharmacol Ther. 2011; 34:1318-27. Ko. J Dermatolog Treat. 2009;20:100-8

TNF Inhibitors and CHF
Study Name RENAISSANCE RECOVER ATTACH
TNF Inhib Etanercept Etanercept Infliximab
N=
(NYHA)
925
(NYHC 2-4)
1123
(NYHC 2-4)
150
(NYHC 3-4)
Rx Placebo,
25 mg BIW,TIW
Placebo
25 mg qwk,BIW
Placebo, 5 or 10 mg/kg
@ wk 0, 2 & 6
Duration Med 12.7 mos. Median 5.7mos 28 weeks
Death Rates
Placebo 14.2%
ETANBIW 17.9%
ETANTIW 19.8%
Placebo 8.8%
ETANQWK 5.9%
ETANBIW 7.2%
Placbo 5 mg/kg 10 mg/kg
wk28 0 2.0% 5.9%
wk54 8.2% 8.0% 15.7%
CHF Hosp NA NA Placebo 5 mg/kg 10 mg/kg
wk28 10.2% 6.0% 21.6%
Concerns? TIW dose group more problems.
NYHA Class II are NOT at lower risk 10 mg/kg @ higher risk

New Onset CHF in Clinical Trials
Etanercept
(3389)
Infliximab
(>1600)
Adalimumab
(2045)
Active Drug 2 0.2% 0.1 %
Placebo
Controls 2 2.1% 0.5%

Reduced CV Risk with MTX + TNF Blockade
• 1829 RA pts w/o CAD (1/01–3/08)
• MTX users (n=1119) vs nonusers
(710) vs TNFi users (588) or TNFi
nonusers (n=1241)
Incident CAD (events/1000 pt-y)
Nonuser User 1-y HR 2-y HR
MTX 37.5 17.6 0.54* 0.33*
TNFi 32.1 11.8 0.54# 0.24*
HR user vs nonuser : * P<0.001; #P=0.03
MTX + TNFi independently associated with 46% reduction in CAD; longer use (>2 y)
associated with greater (67–76%) benefit
1.0
0.20
0.30
0.0
0.05
0.15
0.25
20 40 60 100 80 0 120
Time (mo)
Pro
bab
ilit
y o
f
develo
pin
g C
AD
1.0
0.20
0.30
0.0
0.05
0.15
0.25
20 40 60 100 80 0 120
Time (mo)
MTX never use
MTX use 22 mo
MTX use >22 mo
TNFi never use
TNFi use 17 mo
TNFi use >17 mo
Bozaite-Gluosniene R, et al. ACR 2011, Chicago, #719

Tofacitinib: Integrated safety in RA
clinical trials
• Phase 2, Phase 3, and LTE studies according to duration of Tofa exposure
• 5671 patients, 12,664 pt-y of cumulative Tofa exposure (all doses); median
exposure 2.4 years
IR events/
100 pt-y IR
Discrete 6-month period of exposure to Tofa (month)
0–6 6–12 12–18 18–24 24–30 30–36 36–42 >42
SAE 10.27 10.77 10.44 12.08 10.42 10.02 8.45 7.34 8.82
SI 2.93 2.57 3.42 3.16 3.19 2.93 2.86 2.81 1.89
Herpes
zoster 4.22 4.20 4.69 4.23 4.38 3.99 5.07 3.88 2.11
Malignancy 0.85 0.70 0.66 0.94 1.04 0.83 1.00 0.79 1.04
Lymphoma/
LPD 0.06 0.04 0.09 0.00 0.06 0.14 0.08 0.00 0.12
MACE 0.46 0.58 0.36 0.59 0.62 0.41 0.13 0.00 0.00
Cohen S, et al. EULAR 2014, Paris, #OP0154

Safety Issues With Biologic DMARDs
• Serious infections
• Opportunistic infections (TB)
• Autoantibodies and autoimmune
reactions, including lupus-like syndromes
• Malignancies

TNFi: Pregnancy is a
Relative Contraindication
1. Preg NOT a boxed warning
2. Preg NOT a contraindication
3. Pregnancy Category B – There are no adequate and well-
controlled studies of SIMPONI in pregnant women. Because
animal reproduction and developmental studies are not
always predictive of human response, it is not known whether
SIMPONI can cause fetal harm when administered to a
pregnant woman or can affect reproduction capacity.
SIMPONI should be used during pregnancy only if clearly
needed.
4. Encouraged to enroll such pts with OTIS pregnancy registry
1-877-311-8972
Package insert on TNFi

Other Safety Issues in TNF Inhibitor Use
• Hematologic events
– There have been rare reports of pancytopenia, leukopenia,
thrombocytopenia and neutropenia – including aplastic anemia
– Some cases have been fatal
• Autoimmunity
– Formation of autoantibodies has occurred with anti-TNF therapy
– Rarely, lupus-like syndrome may develop
• Data showed that 2 pts out of 3046 pts treated with adalimumab
developed signs suggestive of new-onset lupus-like condition
• Pts improved after discontinuation of therapy
ENBREL (etanercept) package insert. REMICADE (infliximab) package insert. HUMIRA (adalimumab) package insert.