Embed Size (px)
Citation preview

D.O.I: http:doi.org/10.4127/jbe.2012.0058
RHONA MARTIN1*, DUNCAN S. BUCHAN1, KERI S. KULIK2, LON KILGORE1, JULIEN S. BAKER1.
1 Health and Exercise Sciences, School of Science, Universityof the West of Scotland, Hamilton, ML3 0JB, UK.
2 Department of Health & Physical Education, Indiana Universityof Pennsylvania, Indiana, PA 15705, United States of America.
ABSTRACT
The purpose of this study was to examine the currenthealth status of a sample of Scottish youth in relation tophysical fitness. A sample of 76 children aged 10.2 ± 0.56years had indices of fatness, physical activity, cardio-res-piratory fitness and muscular fitness assessed. A high per-centage of participants were found to have unhealthy lev-els of cardio-respiratory fitness and explosive strength(82.9% and 81.6%, respectively). A positive (β = 0.242) al-though weak (R2 = 0.39) overall relationship was observedbetween physical activity and cardio-respiratory fitness,though was stronger in the boys than the girls (R2 =0.725 vs. R2 = 0.347). The data suggests that interven-tions improving physical activity participation, weight sta-tus and physical fitness are essential prior to adolescencein order to improve health and well-being.
KEY WORDS: Health, Overweight, Fitness testing, Fitness levels.
BBIOLOGY OF IOLOGY OF EXERCISEXERCISEVOLUME 8.2, 2012
Card
io-res
piratory f
itnes
s an
d mus
cular
fitne
ss l
evels
ofSc
ottis
h yo
uth
and
their
asso
ciations
with
phy
sica
l ac
tivity

INTRODUCTION
The increasing prevalence of obesity is now considered a global concern(48). Throughout the Western world, obesity is the 5th leading risk factor formortality (48) with the prevalence of poor weight status in youth appearing toincrease for all ages (13, 28). Within the United Kingdom (UK), obesity levelshave doubled in the last twenty-five years with 20-25% of youth presently hav-ing a Body Mass Index (BMI) which classifies them as overweight (6). WithinScotland, the percentage is even greater with recent figures suggesting that ap-proximately 33% of children aged between 7 and 11 years are overweight (43).
Regular participation in physical activity is known to reduce the risk of obesi-ty (37) and the likelihood of developing chronic diseases such as; cardiovascu-lar disease (CVD), hypertension and type II diabetes (2, 13, 37). Nonetheless anddespite the well-established benefits of being active, youth are increasinglyadopting sedentary lifestyles (5) with many failing to achieve minimal activityguidelines (11, 47). Recent findings in Scottish populations suggest a worryingtrend with 30-35% of Scottish youth aged between 2 and 15 years seemingly un-able or undesiring to meet minimal activity guidelines for health (43) of one hourof moderate to vigorous physical activity per day (47). The importance of achiev-ing daily physical activity recommendations for health is expressed by Ortegaand colleagues (35), who found that Swedish youth who achieved daily physicalactivity recommendations were at decreased risk of CVD risk factors comparedto those who did not achieve recommended levels of physical activity.
It has been argued that physical fitness is a more significant marker ofhealth status in youth than physical activity (20, 35, 36), although both areknown to be associated with future cardiovascular disease (CVD) risk inadulthood 34). Increasing physical activity participation has been associat-ed with increased cardio-respiratory fitness and reduced risk of CVD inyouth (7, 33). While it is known that healthy levels of cardio-respiratory andmuscular fitness are linked to a healthier cardiovascular profile during child-hood and adolescence and tend to track into adulthood (7, 13, 33, 34), lim-ited evidence exists on the physical fitness status of Scottish youth. Phys-ical fitness is not a single concept but rather consists of several individualinterrelated and measurable constructs representing most of the bodiesfunctions (muscular, cardio-respiratory, motor, metabolic and morphologi-cal) (34). Unsurprisingly, measures of physical fitness are now consideredto be important markers of health status, CVD risk and early mortality (7,13, 34).Thus, the purpose of this pilot investigation was to evaluate thephysical fitness status of Scottish youth as they move into secondaryschool education. The findings here may reveal important clues as towhether the physical activity guidelines proposed in Scotland are achievingtheir desired aims of improving the health status of young individuals.
34 JBE – VOL. 8.2, 2012

METHODS
Subjects
A sample of 76 children (36 boys and 40 girls) aged 10.2 ± 0.6 yearswere randomly selected from a primary school in the West of Scotland. In-formation concerning the aims of this study and their involvement was pro-vided to participants and their parents/guardians. Only participants who re-turned both the consent and consent forms were eligible to participate.Participants were informed that they were free to withdraw from this studyat any time and without explanation. All data collected was kept anony-mous. Ethical approval for this study was granted by the University of theWest of Scotland’s Ethics Committee.
Physical Measures
Stature and mass were measured barefoot while wearing light clothing.Stature was measured to the nearest 0.1cm using a portable Seca sta-diometer (Seca Ltd. Brimingham UK). Mass was recorded to the nearest0.1kg using a Seca 880 digital scale (Seca Ltd. Brimingham UK). Both in-struments were calibrated prior to assessments to ensure accuracy of mea-surement. BMI was calculated as weight/height2 (kg/m2). Participants werecategorized as either obese, overweight or normal weight according to In-ternational BMI cut-off values (8, 9).
The 20m multi-stage fitness test (MSFT) was used to assess cardio-res-piratory fitness and was performed in accordance with standard procedures(25). Briefly, participants were instructed to run back and forth in a straightline between cones set 20m apart while keeping in time with the audio sig-nals from a CD. The initial speed was 8.5 km/h and increased by 0.5 km/hevery level. Participants were encouraged to keep going for as long aspossible. The test was terminated when the participant failed to reach the20 m mark coincident with the audio signal on two consecutive occasionsor when the participant stopped due to volitional fatigue. The last test stagecompleted was recorded for each participant. Maximal oxygen uptake(V02max) was then estimated using the Barnett et al equation (4):
VO2max = 24.4 – 5.0 × G – 0.8 × A + 3.4 × S
Where A is the age of the participant, G is gender (0 = male, 1 = fe-male) and S is the final speed (S = 8 + 0.5 x last stage completed).
Standard procedures for the standing board jump (SBJ) as explained inthe EUROFIT handbook (14) were used to assess lower limb explosive
CARDIO-RESPIRATORY FITNESS AND MUSCULAR FITNESS LEVELS 35

strength. Briefly, participants were instructed to jump a maximal horizontaldistance from a static starting position. A two footed take off and landingposition was used. Participants were instructed to swing their arms andbend their knees to provide a forward drive. The score was measured asthe distance from the take-off line to the heel closest to the take-off line af-ter the jump and was measured to the nearest 0.1cm.
Physical activity levels were assessed using a valid and reliable PhysicalActivity Questionnaire for Children (PAQ-C) (Crocker 10, 24). Participantswere asked to complete the questionnaire at home with help and guidancefrom their parent/guardian. The questionnaire involved participants recallingtheir physical activity participation from the previous week (previous sevendays). Participation was scored on a scale of 1-5 and provided an indica-tion of activity levels within this cohort. For this study, a score of less than2.5 indicated low physical activity participation and a score of more than2.5 indicated high physical activity participation.
Maturation status was estimated using the Tanner sexual maturationstaging (45). Using average age maturation guidelines proposed by Strangand Stray, pubic hair growth was estimated for each participant accordingto age (46). For females and males under the age of 9.5 years, guidelinessuggest pubic hair growth will be at Tanner stage 1. For females aged 9.5to 14.5 years and males aged 9.5 to 13.5 years, guidelines suggest pubichair growth to be at Tanner stage 2. These estimations were determinedwith parents doing a comparative to photographs and not assessed by theresearchers.
All performance measures were obtained at the same time of day tominimise the effects of diurnal variation. In addition, all measures were col-lected after familiarisation trials, with no physical activity 24 hours prior toexperimental data collection.
Statistical data analysis
Data was analysed using the Statistical Package for the Social Sciences(SPSS) version 17.0. The level of significance was set a priori at P≤0.05throughout. Mean ± SD was calculated for all measurements. Bonferroni-adjusted t-tests for two independent means were used to assess differ-ences between two means. Standardized coefficient regression modelswere used to determine the direction, significance and strength of the re-lationship between physical activity and cardio-respiratory fitness. The di-rection of the relationship was represented by a “β” value and an “R2” val-ue indicated the strength of the relationship.
36 JBE – VOL. 8.2, 2012

RESULTS
Descriptive characteristics of this cohort are presented in Table 1. Nosignificant differences (p > 0.05) were found between gender in age (p =0.06), height (p = 0.605), weight (p = 0.691) and BMI (p = 0.337). Themajority (78.9%) of participants fell into Tanner stage 2 for sexual matura-tion and the remaining 21.1% fell into Tanner stage 1. The percentage ofobese participants was 12.9%. Almost double the amount of girls wereobese than boys (15% and 8.4%, respectively). The percentage of over-weight participants was 23.4% and was similar in both girls and boys(23.5% and 23.3%, respectively). The prevalence of low physical activity inall participants was 38.2% with boys reporting more activity than girls,61.2% vs. 65%, respectively. No significant differences (p > 0.05) in phys-ical activity levels between genders was noted though boys had signifi-cantly greater p ≤ 0.05 cardio-respiratory and explosive strength levelsthan girls (Table 2).
Table 1. Descriptive characteristics of participants.
All Boys Girls P value
Number (n) 76 36 40Age (years) 10.2 ± 0.56 10.3 ± 0.49 9.85 ± 0.59 0.06 Height (cm) 138 ± 7.27 138 ± 6.56 138 ± 7.91 0.605Weight (kg) 33.3 ± 9.23 32 ± 9.02 34.1 ± 9.51 0.691BMI(kg m-2) 17.9 ± 3.57 17.4 ± 3.44 18.4 ± 3.69 0.337
Physical Activity status (n/%)High Physical Activity 28/ 38.2 14/ 38.8 14/ 35Low Physical Activity 48/ 61.8 22/ 61.2 26/ 65
Tanner Stage: (n/%)1 16/ 21.1 4/ 11.2 12/ 302 60/ 78.9 32/ 88.8 28/ 70
Physical activity level was found to be positively, and significantly (p≤0.05) associated with cardio-respiratory fitness in all participants (Table3). To further examine this relationship the sample was split into genders.Although a positive and significant association between physical activity
CARDIO-RESPIRATORY FITNESS AND MUSCULAR FITNESS LEVELS 37

and cardio-respiratory fitness was seen for both genders, the relationshipwas stronger in boys than in girls (Table 3).
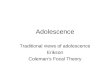
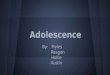
The number of participants failing to meet recommended levels forhealthy cardio-respiratory fitness is displayed in Figure 1. A large percent-age of participants reported unhealthy cardio-respiratory fitness levels(82.9%) although the boys appeared to have a lower percentage of un-healthy cardio-respiratory fitness levels (77.8%) than the girls (87.5%). Fig-ure 2 displays the proportion of participants reporting unhealthy levels ofexplosive strength. A large percentage of participants were associated withunhealthy explosive strength levels (81.6%). Although boys presented ahigher mean value of explosive strength than girls, similar results were ob-served in failure to meet cut off levels in both groups.
Table 2. Independent T-test for measures of physical fitness and phys-ical activity within gender. Means and standard deviation pro-vided.
Boys (n = 36) Girls (n = 40) P Value
Cardio-respiratory fitness (20MSFT) 33.07 ± 6.5 29.74 ± 5.57 0.019*(mL · kg–1 · min–1)
Explosive strength 1.32 ± 0.24 1.15 ± 0.25 0.004*(SBJ) (m)
Physical activity 2.39 ± 0.53 2.17 ± 0.54 0.30(PAQ-C score)
Note *= Significance p ≤ 0.05
DISCUSSION
The main finding of the study indicates that the majority of youth studiedpossessed poor health in relation to physical fitness, obesity and physical ac-tivity participation. Other important findings of this study are that gender dif-ferences exist in measures of physical fitness and that physical activity maynot directly affect levels of cardio-respiratory fitness, particularly in girls.
Physical activity is well known to help in the prevention of developing
38 JBE – VOL. 8.2, 2012

risk factors of CVD such as; obesity, hypertension, type II diabetes and lowphysical fitness (34, 40). The present data indicates that over 60% of par-ticipants reported low levels of physical activity, a finding much greaterthan that seen in the 2010 Scottish Health Survey (43). In that study, onethird of Scottish youth included were identified with inadequate levels ofphysical activity. The present finding, if extrapolated across the whole ofScotland, suggests that nearly twice as many youth are inactive as pro-posed by the Scottish Executive. Furthermore, youth in this study are lessphysically active than Danish, Flemish, Portuguese, Spanish, Swedish andEstonian youth (3, 32, 33, 35, 39), where on average one out of threeyouth were associated with low physical activity participation. This is a dis-turbing finding as participation in regular physical activity or achieving ad-equate levels of physical activity is widely accepted to track into adulthoodand reduce the risk of adulthood obesity and CVD (15, 30, 34). It mighttherefore be suggested that the youth in this study are at higher risk of be-coming obese adults and of developing current and future CVD than pro-posed by the Scottish Executive and their European equivalents, as a re-sult of having low physical activity participation.
Table 3. Standardized coefficient regression analysis (β), standard er-ror of estimate (SEM), significance (P value) and Adjusted R2
for Physical activity and Cardio-respiratory fitness in gender.
n β P value Adjusted R2 SEM
All 76 0.242 0.092 0.39 0.496Boys 36 0.856 0.000* 0.725 0.278Girls 40 0.603 0.000* 0.347 0.438
Note *– significance when p ≤ 0.001
Low physical activity or reduction in physical activity has been associat-ed with increased risk of childhood overweight and obesity (21). Unsurpris-ingly, results of the study presented here revealed similar trends in over-weight and obesity levels to low physical activity levels, with approximately40% of participants being classed as either overweight or obese. This find-ing reveals that two out of five youth in this study were in these categories,a finding slightly higher than reported in the 2009 Scottish health survey,where only one third of 2 to 15 year olds were classed as over-weight/obese (43). Furthermore, the prevalence of overweight and obesity
CARDIO-RESPIRATORY FITNESS AND MUSCULAR FITNESS LEVELS 39

in this study is substantially higher when compared to studies of Swedish(33) and Flemish youth (7) where the prevalence of overweight and obesi-ty was only 12.6% and 7.4%, respectively. This comparison suggests thatScottish youth may be four times more likely to be overweight or obese byBMI standards than other European youth. Furthermore, girls in this studywere almost twice as likely to be classified as obese than boys, stronglysuggesting that girls are more at risk of becoming obese adults and de-veloping future CVD than their male counterparts (15, 30).
The relationship between physical activity and physical fitness is well doc-umented (17-19,23). However, the literature remains unclear in respect to theamount of physical activity needed to elicit changes in cardio-respiratory fit-ness (37). A significant (p =0.000) however weak (R2=0.39) relationship be-tween physical activity and cardio-respiratory fitness was observed in thisstudy, supporting the finding of Kemper & Koppes, (23). This suggests thatincreasing physical activity may not be beneficial for improving cardio-respi-ratory fitness. On this note, a gender specific analysis of this relationship in-dicated that the female participants were the cause of this weak overall rela-tionship as the male participants demonstrated a much stronger relationshipthan the females (R2=0.725 and R2= 0.347, respectively). Suggesting that, in-creasing physical activity in the girls may not be beneficial for improving car-dio-respiratory fitness, as higher levels of physical activity did not directly re-flect high cardio-respiratory fitness in girls. Whereas, increasing physicalactivity in the boys may be beneficial for improving cardio-respiratory fitness.It would be worthwhile in later studies to examine and quantify the volumeand intensity characteristics of the reported physical activity to further explorethis discrepancy in previous and present data.
Cardio-respiratory fitness has been suggested to be the most importantindicator of health in youth (34). A meta-analysis which reviewed the 20mMSFT results in over 100 studies involving 37 countries indicated Europeanyouth from Italy, Greece, Portugal, America, Brazil and Singapore reportedthe poorest levels of cardio-respiratory fitness on a worldwide perspective(34). These low levels of fitness are proposed to persist into adulthood (26).Supporting this view, four out of five (82.9%) participants in this presentstudy possessed poor cardio-respiratory fitness which may associate themwith future unhealthy cardiovascular outcomes. The majority of participantsin this study are at risk of maturing into adulthood with poor cardio-respira-tory fitness (26), resulting in an increased risk of future CVD (16, 39). Girlsin this study presented a higher incidence of unhealthy cardio-respiratory fit-ness than males (87.5% and 77.8%, respectively). This result supports thefindings of Mota et al., (29) who reported a higher prevalence of unhealthycardio-respiratory fitness in Portuguese girls than boys (28% and 19%, re-spectively). Thus, girls may present a higher risk of developing future CVDthan boys due to a higher prevalence of unhealthy cardio-respiratory fitness
40 JBE – VOL. 8.2, 2012

levels. This difference between genders could partially be explained by thefact that boys tend to participate in vigorous intensity physical activity morethan girls (12, 41), resulting in greater improvements in cardio-respiratory fit-ness and lower associations with unhealthy cardio-respiratory fitness (1, 35).
Figure 1: Percentage of participants failing to achieve cut off values asproposed by The Cooper Institute (46) for cardio-respiratory fitness.
Figure 2: Percentage of participants failing to achieve cut off values asproposed by The Committee of Experts on Sports Research (14) andACSM (1) for explosive strength.
CARDIO-RESPIRATORY FITNESS AND MUSCULAR FITNESS LEVELS 41
Boys
Girls
All
77.8
87.5
82.9
Participants with unhealthy cardio-respiratory fitness (%)
72 74 76 78 80 82 84 86 88 90
Boys
Girls
All
83.3
80
81.6
Participants with unhealthy Explosive strength (%)
78 79 80 81 82 83 84

Recently, the focus of muscular fitness has shifted from a sports perfor-mance focus (31) to a health related focus (16, 22, 27, 42). This presentstudy indicates that 86.2% of the studied population sample demonstratedan unhealthy explosive strength level, meaning that four out of five youth inthis study may be at additional CVD and metabolic risk. This finding maybe due to the low physical activity participation rates among participants inthis study. Martinez-G mez et al., (27) found an association between totalphysical activity, physical activity intensity and muscular fitness. They foundthat low levels of total physical activity as well as low intensity physical ac-tivity reflect low levels of muscular fitness, where as high levels of totalphysical activity and vigorous intensity physical activity reflected higher lev-els of muscular fitness. Suggesting that participating in adequate levels ofphysical activity, more specifically vigorous physical activity, may be bene-ficial for achieving healthy muscular fitness.
CONCLUSION
The results of this study may indicate that overweight/obesity, low phys-ical activity and unhealthy physical fitness levels of Scottish youth demon-strate a worryingly low health status compared with other European youth.A large number of subjects in this current study failed to achieve minimalcriteria for health, indicative of an increased risk of current and future CVDrisk factors. Results of this study indicated that girls in this study weremore obese and less physically fit than the boys meaning that they are ata higher disease risk than boys, and are at a greater risk of retaining thatrisk and persistent low fitness into adulthood. Results also suggested thatincreasing physical activity levels may not directly or sufficiently improvecardio-respiratory fitness in all participants. This is especially apparentwhen considering this association in girls. These findings indicate that de-veloping physical activity interventions to promote healthy and correctphysical activity habits, reduce overweight/obesity and improve physical fit-ness, particularly in girls, requires more attention within the youth of Scot-land.
REFERENCES
1. American College of Sports Medicine (7th ed). ACSM’s Guidelines forExercise Testing and Prescription. Philadelphia, Whaley, MW. 2006.
2. Andersen LB, Harro M, Sardinha LB et al. Physical activity andclustered cardiovascular risk in children: a cross-sectional study (TheEuropean Youth Heart Study). Lancet 368(9532): 299-304, 2006.
42 JBE – VOL. 8.2, 2012

3. Ara I, Moreno LA, Leiva MT, Gutin B and Casaj s JA. Adiposity,physical activity, and physical fitness among children from Aragon,Spain. Obesity 15(8): 1918-24, 2007.
4. Barnett A, Chan L and Bruce I. A preliminary study of the 20-mmultistage shuttle run as a predictor of peak V02 in Hong KongChinese students. Pediat Exerc Sci 5: 442–50, 2001.
5. Boreham C and Riddoch C. (2001). The physical activity, fitness andhealth of children. J Sports Sci 12: 915–29, 2001.
6. British Heart Foundation. Couch Kids: The Nation’s Future. London:British Heart Foundation, 2009.
7. Castillo-Garz n M J, Ortega FB and Gutierrez-Sainz A. AMediterranean diet is not enough for health: Physical fitness is animportant additional contributor to health for the adults of tomorrow.World Rev Nutr Diet 97: 114-38, 2007.
8. Cole TJ, Bellizzi MC, Flegal KM and Dietz WH. Establishing a standarddefinition for child overweight and obesity worldwide: internationalsurvey BMJ 320: 1240-43, 2000.
9. Cole TJ, Flegal KM, Nicholls D and Jackson AA. Body mass index cutoffs to define thinness in children and adolescents: internationalsurvey. BMJ 335: 194, 2007.
10. Crocker, P. R. E., Bailey, D. A., & Faulkner, R. A. Measuring generallevels of physical activity: preliminary evidence for the Physical Activi-ty Questionnaire for Children. Med Sci Sports Exerc 29(1): 1344-49,1997.
11. Department of Health (2011). New Physical Activity Guidelines. UnitedKingdom, Department of Health, 2011.
12. Duncan MWL, Al-Nakeeb Y and Nevill A. The impact of Socio-Economic Status on the physical activity levels of British secondaryschool children. PESS 7: 30-44, 2002.
13. Eisenmann JC. Physical activity and cardiovascular disease risk factorsin children and adolescents: an overview. Can J Cardiol 1(20):295–301, 2004.
14. EUROFIT. Handbook for the EUROFIT Test of Physical Fitness.Strasbourg: Committee for the Development of Sport, Committee ofExperts on Sports Research, 1993.
15. Freedman DS, Khan LK, Dietz WH, Srinivasan SR and Berenson GS.Relationship of childhood obesity to coronary heart disease risk factorsin adulthood: the Bogalusa Heart Study. Pediatrics 108(3): 712-8,2001.
16. Garc a-Artero E, Ortega FB, Ruiz JR et al. Lipid and metabolic profilesinadolescents are affected more by physical fitness than physicalactivity (AVENA study). Rev Esp Cardiolo 60: 581-88, 2007.
17. Gutin B, Barbeau P and Owens SL. Effects of exercise intensity on
CARDIO-RESPIRATORY FITNESS AND MUSCULAR FITNESS LEVELS 43

cardiovascular fitness, total body composition, and visceral adiposityof obese adolescents. Am J Clin Nutr 75: 818-25, 2002.
18. Gutin B, Yin Z, Humphries MC and Barbeau P. Relations of moderateand vigorous physical activity to fitness and fatness in adolescents.Am J Clin Nutr 81: 746-50, 2005.
19. Hands B, Larkin D, Parker H, Straker L and Perry M. The relationshipamong physical activity, motor competence and health-related physicalfitnessnin 14-year-old adolescennts. Scan J Med Sci Sport 19: 625-33,2009.
20. Hurtig-Wennlöf A, Ruiz JR, Harro M and Sjöström M. Cardiorespirato-ry fitness relates more strongly than physical activity to cardiovasculardisease risk factors in healthy children and adolescents: the EuropeanYouth Heart Study. Eur J Cardiovasc Prev Rehabil 14(4): 575-581,2007.
21. Janssen I and LeBlanc AG. Systematic review of the health benefits ofphysical activity and fitness in school-aged children and youth. Int JBehav Nutr Phys Act 7: 40, 2010.
22. Kay SJ and Fiatarone-Singh MA. The influence of physical activity onabdominal fat: a systematic review of the literature. Obesity Rev 7:183-200, 2006.
23. Kemper HG and Koppes, LL. Linking physical activity and aerobic fit-ness: are we active because we are fit, or are we fit because we areactive? Pediat Exerc Sci 18: 173-81, 2006.
24. Kowalski K, Crocker P and Faulkner R. (1997). Validation of the phys-ical activity questionnaire for older children. Pediatric Exercise Science9: 174–86, 1997.
25. Leger LA, Mercier D, Gadoury C and Lambert J. The multistage 20metre shuttle run test for aerobic fitness. J Sports Sci 9: 93-101, 1988.
26. Malina, R. M. Physical activity and fitness: pathways from childhood toadulthood. Am J Hum Biol 13: 167-72, 2001.
27. Mart nez-G mez D, Welk GJ, Puertollano MA, del-Campon J, MoyaJM, Marcos A and Veiga OL. Associations of physical activity with MFin adolescents. Scan J Med Sci Sport 21: 310–317, 2011.
28. Mesa JL, Ruiz JR, Ortega FB et al. Aerobic physical fitness in relationto blood lipids and fasting glycaemia in adolescents: Influence ofweight status. Nutr Meta Cardiovas 16: 285-93, 2006.
29. Mota J, Vale S, Martins C, Gaya A, Moreira C, Santos R and Ribeiro JC.Influence of muscle fitness test performance on metabolic risk factorsamong adolescent girls. Diabetology & Metabolic Syndrome 2(42): 2010.
30. Must A, Jacques PF, Dallal GE, Bajema CJ and Dietz WH. Long-termmorbidity and mortality of overweight adolescents: A follow-up of theHarvard Growth Study of 1922 to 1935. New Engl J Med 327(19):1350-5, 1992.

31. Olds T, Tomkinson G, Leger L and Cazorla G. Worldwide variation inthe performance of children and adolescents: an analysis of 109studies of the 20-m shuttle run test in 37 countries. J Sports Sci 24:1025-38, 2006.
32. Ortega F B, Ruiz JR, Castillo MJ et al. Low level of physical fitness inSpanish adolescents. Relevance for future cardiovascular health(AVENA study). Rev Esp de Cardiol 58: 898-909, 2005.
33. Ortega FB, Ruiz JR, Hurtig-Wennlöf A and Sjöström, M. (2007).Physically active adolescents are more likely to have a healthiercardiovascular fitness level independently of their adiposity status. TheEuropean Youth Heart Study. Rev Esp Cardiol 61: 123-9, 2007.
34. Ortega FB, Ruiz JR, Castillo MJ and Sjöström M. Physical fitness inchildren and adolescence: a powerful marker of health. Int J Obesity,32: 1-11, 2008.
35. Ortega FB, Artero EG, Ruiz JR et al. Reliability of health-relatedphysical fitness tests in European adolescents: The HELENA Study. IntJ Obesity 32: S49-S52, 2008.
36. Ortega FB, Ruiz JR., Hurtig-Wennlof A, Vicente-Rodriguez G, Rizzo NS,Castillo MJ and Sjöström M. Cardiovascular fitness modifies the asso-ciations between physical activity and abdominal adiposity in childrenand adolescents: the European Youth Heart Study. BJSM 44(4): 256-62, 2010.
37. Parizkovâ J and Hills A. Childhood obesity: prevention andmanagement. Boca Raton, CRC Press, 2001.
38. Ruiz JR, Rizzo NS, Hurtig-Wennlof A, Ortega FB, Warnberg J andSjostrom M. Relations of total physical activity and intensity to fitnessand fatness in children: the European Youth Heart Study. Am J ClinNutr 84(2): 299-303, 2006.
39. Ruiz JR, Ortega FB, Meusel D et al. Cardiorespiratory fitness isassociated with features of metabolic risk factors in children. Shouldcardiorespiratory fitness be assessed in a European health monitoringsystem? The European Youth Heart Study. J of Pub Health 4: 94-102,2006.
40. Ruiz JR and Ortega FB. Physical activity and cardiovascular diseaserisk factors in children and adolescents. Current Cardiovascular RiskReports 3(4): 281-7, 2009.
41. Sallis JF and Owen N. Physical activity and behavioral medicine. CA,SAGE Publications, 1999.
42. Sayer AA, Syddall HE, Dennison EM et al. Hertfordshire cohort. Gripstrength and the metabolic syndrome: findings from the hertfordshirecohort study. QJM 100: 707-13, 2007.
43. Scottish Governement. Scottish Health Survey 2009. Endinburgh, TheScottish Government, 2011.
CARDIO-RESPIRATORY FITNESS AND MUSCULAR FITNESS LEVELS 45

44. Strang J and Story M. Adolescent Growth and Development. In StrangJ, ad Story M (eds). Guidelines for Adolescent Nutrition Services. USDepartment of Health and Human Services; Rockville, MD, 2005.
45. Tanner JM. Growth at adolescence.Oxford, Blackwell ScientificPiblications, 1962.
46. The Cooper Intitiute. Standards for Healthy Fitness Zone. Texas, TheCooper Institiute for Areobics Reseach, 2010.
47. World Health Organisation. Global Recommendation on PhysicalActivity for Health. Geneva, World Health Organization, 2010.
48. World Health Organisation. Health Statistics: Causes of death 2008summary tables; Geneva, World Health Organization, 2011.
Address for correspondence:Rhona Martin BSc (Hons)University of the West of ScotlandHamilton, UKML3 0JB Email: [email protected]:01698283100.Investigations were carried out at:University of the West of Scotland,HamiltonML3 0JB, UK.
46 JBE – VOL. 8.2, 2012