Embed Size (px)
Citation preview
Case conference 9/18/2008
• 29 yo single male• CC: overdose• Past medical history
– Schizoaffective disorder– DM II– Alcohol abuse history
• Habits– Current smoker with 15 pk yr history,
history of alcohol abuse – none currently• Meds
– Bupropion SR– Clozapine– Gemfibrozil– Glipizide– Ibuprofen– Lorazepam prn– Metformin– Simvastatin
§ HPI and Hospital courseú On 8/10/08, pt took an OD of seroquel, felt remorseful, and sought
medical care. At outside ED, initially did well but became increasingly agitated which was not responsive to various initial attempts at sedation. Ultimately given lorazepam, valium, benadryl, and cogentin. Became sedated and hypoxic requiring intubation. Over following 2 days, unable to extubate as sedation could only be maintained with high doses of propofol.
ú Transferred to Abbott. Ongoing issues with significant agitation with any weaning of sedation. Psychiatry was consulted and felt the agitation was likely due to his underlying psychiatric illness. Numerous sedative modalities were tried in an effort to lighten his sedation without him developing significant agitation. These included various combinations of IV propofol, IV haloperidol, IV lorazepam, IV dexmedetomidine and IV midazolam.
ú On two occasions he did well enough to be extubated but shortly afterwards developed significant tachycardia and tachypnealeading to significant distress and had to be reintubated. Neurology was consulted to ensure there was no neurological process. He had imaging of his brain, lumbar puncture and EEG which were unremarkable.
– Ultimately the decision was made to initiate oral clozapine under the guidance of psychiatry. His doses were titrated up quickly. Over the next few days as the other modalities of sedation were lightened he was less and less agitated. He was extubated successfully 8/28/2008.
– Of note, the patient initially had a normal calcium level but as the hospitalization progressed his calcium slowly increased into the low 11 range and ionized calcium to 1.52. Phos normal.
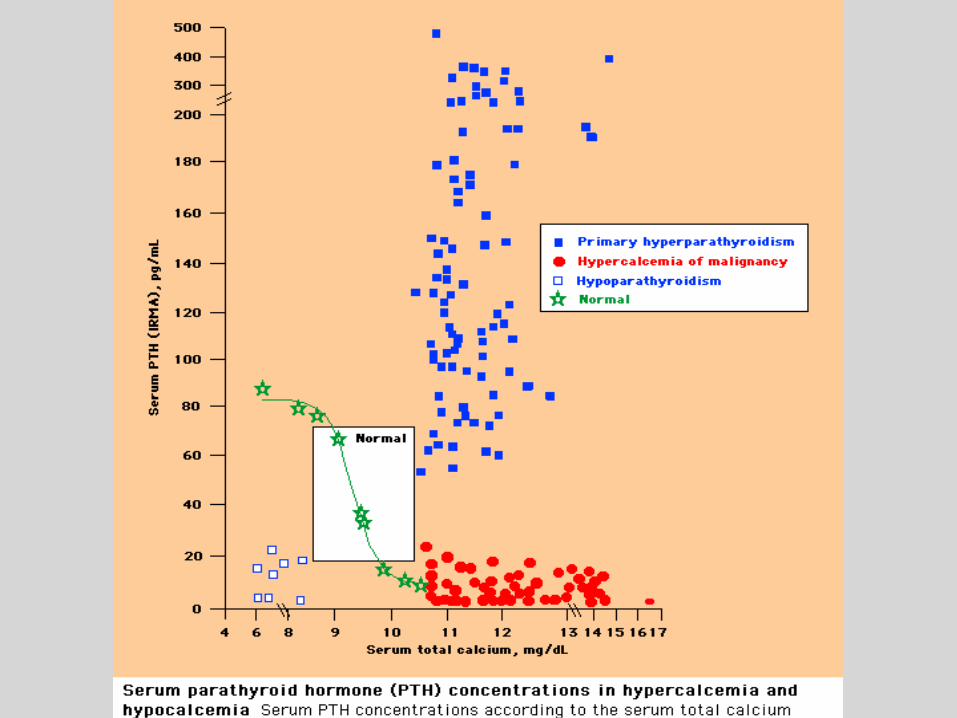
– Nephrology and endocrinology differential diagnosis included primary hyperparathyroidism, hypercalcemia of malignancy, meds, adrenal insufficiency, granulomatous disease (sarcoid), immobilization hypercalcemia, Vit D intoxication, Vit A abnormality, FHH.
• iPTH 40 (normal range 15-65 pg/ml), Repeat iPTH high at 84.
• TSH normal• Vit D level 22 pg/ml (normal)• SPEP/Ufix negative
– Labs consistent with primary hyperparathyroidism.
– Pt treated with IV fluids. Briefly treated with Lasix to treat hypervolemia. Goal was to avoid Lasix if possible as it temporarily causes calciuresis, but with any volume depletion, the proximal tubule will take up far more calcium in the long run than is lost by blocking the loop with Lasix.
– Sestamibi scan showed increased uptake in the lower right parathyroid gland consistent with a parathyroid adenoma –however evaluated by ENT and it was felt scan was equivocal.
– U/S showed a right thyroid nodule but no discrete parathyroid mass– 24 hour urine calcium 191mg– Endocrine feels not c/w familial hypocalciuric hypercalcemia as
these pts usually have 24-hour urine calciums less than 100 mg/24h.
– ENT feels there is no evidence of a parathyroid adenoma. Recommended follow up U/S of thyroid in 6 months with outpatient follow up of calcium levels.
72 yo female with fatigue and aches
Case conference 9/18/08
HPI
• PMD 3/08 with generalized weakness, fatigue and aches. Found Cr 2.0 and calcium 15 -> admitted. No antacids, calcium or vitamin D supps. Negative SPEP/UPEP. PTH-related peptide, intact PTH, and TSH normal. 25-hydroxyvitamin D low 19 (25-80). CXR negative. Renal consulted. Rx with IV fluids, lasix, pamidronate. On lasix and spironolactone PTA for chronic LE edema Spironolactone stopped. Ca 10.7 and Cr 1.5 at discharge.
HPI cont.
• Outpt PET/CT showed a few pulm micronodules, a small left pleural effusion and right thyroid calcification without abnormal PET activity.
• Outpt mammogram, colonscopy negative.
• Readmitted 5/08 with LE and periorbital edema, DOE, dry cough, dry eyes. Allegra helpful for resp sx PTA.
HPI cont.
• Ca 10.7, Cr 1.19, alb 3.7, UA neg prot• lasix increased from 40 mg qd to BID.• Thyroid US showed multiple nodules and
FNA benign.• Smear with lympho- and mono-cytoses and
flow cytometry c/w a reactive lymphocytosis• TTE with mild concentric LVH, LAE, and
moderate pulmonary hypertension.• ACE level 118 U/L (7-46)
HPI, cont• Readmitted 8/08 with slowly progressive fatigue,
lethargy, decreased concentration, constipation and bone pain.
• Mayo as an outpatient since 6/08. Highly suspecting sarcoid. Optho eval without evidence sarcoid. Repeat CT chest without area amenable to bx or bronch. Pulm felt sarcoid highly likely and started prednisone 40 mg qd with bactrim proph day of admit. She was driving home from Mayo and got a phone call stating her calcium and creat were high and to go to the ED.
PMHX
• Hypertension• Chronic LE edema• HyperCa++• Thyroid Nodules• Moderate Pulmonary Hypertension• Lymphocytosis • Multiple Pulmonary Nodules• Renal insufficiency
Meds
• LASIX 20 MG BID• METOPROLOL SR 100 MG QD • KCL SR 20 MEQ BID• PREDNISONE 40 mg QD • BACTRIM PROPH
EXAM• BP 163/94, P 74,T 97.4, RR 18,SpO2 96%• EYES: sclera injected bilaterally • HEENT: normal• NECK: Normal, no thyroid nodule or goiter appreciated • RESP: Normal • CV: s1, s2 without m/r/g. No JVD. Trace LE edema to mid shin • ABD: Normal • MS: Normal • LYMPH: no cervical or inguinal LAD • SKIN: normal • NEURO: oriented x 3 with somewhat slower responses. CN
intact. UE and LE motor intact.
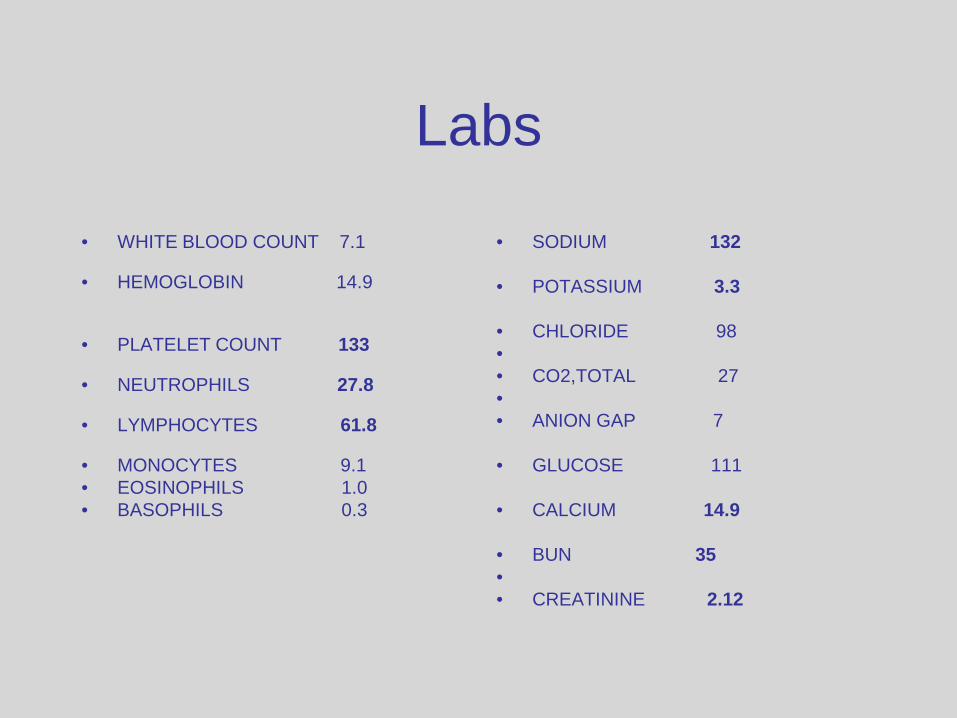
Labs
• WHITE BLOOD COUNT 7.1
• HEMOGLOBIN 14.9
• PLATELET COUNT 133
• NEUTROPHILS 27.8
• LYMPHOCYTES 61.8
• MONOCYTES 9.1• EOSINOPHILS 1.0• BASOPHILS 0.3
• SODIUM 132
• POTASSIUM 3.3
• CHLORIDE 98•• CO2,TOTAL 27•• ANION GAP 7
• GLUCOSE 111
• CALCIUM 14.9
• BUN 35•• CREATININE 2.12
Assessment/Plan
• Hypercalcemia likely due to sarcoid –hydrate, lasix 20 mg IV q12 hours, consider pamidronate when renal function stabilizes, continue prednisone
• ARF – likely due to hyperCa++. Follow with IVF
Hospital Course
• Calcium improved, thinking clearer• Some sob, weight gain, crackles, and sinus
brady with pauses. Stopped IVF. • Cards eval – d/c metoprolol. Consider
cardiac MRI for sarcoid eval when renal function improved. r/o OSA
• Discharged HD #4. Creat 1.88, Ca++ 11.3• Increased lasix 60 qam and 40 qpm
Hypercalcemia
Etiology of Hypercalcemia
• Increased intestinal absorption– Ca intake, Vit D (CGD, lymphoma)
• Increased bone resorption– HPTH, malignancy, Paget’s
• Miscellaneous– Lithium, Thiazides, Familial
Major Causes
• Ambulatory– Hyperparathyroidism ( 90% )
• Hospitalized– Malignancy ( 65% ) & HPTH ( 25% )
• Milk Alkali Syndrome– Due to dyspepsia & osteoporosis Tx– 12 % of hospitalizations
Calcium Intake
• Small intestine• Stimulated by Vitamin D metabolites• Intake alone is a rare cause of
hypercalcemia– Unless combined with decreased urine
excretion• Renal failure & Milk Alkali Syndrome
Calcium Intake
• Renal failure– Hyperphosphatemia treatment– Calcitriol
• Milk Alkali Syndrome– Calcium carbonate or milk– Hypercalcemia, metabolic alkalosis, renal
insuff– Distal tubule reabsorption
Hypervitaminosis D
• Increased absorption & resorption• Exogenous vs. endogenous calcitriol• Calcitriol vs. calcidiol & vitamin D• Chronic granulomatous disorders
– Sarcoidosis– Lymphoma– Tuberculosis
Bone Resorption
• Primary & secondary hyperparathyroidism
• Malignancy• Hyperthyroidism• Immobilization• Paget’s• Hypervitaminosis A
Primary Hyperparathyroidism
• Most common in 5th- 6th decade• Usually due to a parathyroid adenoma• Diffuse hyperplasia ---> MEN I or II• Elevations may be mild or intermittent• Women 2-3x more likely• PTH-related protein secretion
Malignancy
• Local resorption of bone induced by metastasis
• Mediated by cytokines, OAF, PTH-rp– Different mechanism than in lymphoma
• Squamous cell of the lung, breast cancer, multiple myeloma, and renal cell carcinoma are the most common
Miscellaneous Causes
• Hyperthyroidism ( 10-20% )• Immobilization• Paget’s Disease• Lithium• Thiazides• FHH (autosomal dominant)
Signs & Symptoms
• Related to the severity & rapidity of rise• Mild elevations generally asymptomatic
– Often accidentally discovered• Mild MS changes ---> stupor & coma• Abdominal pain, N & V• Polyuria & reduced GFR• Calcium oxalate stones
Diagnosis
• Assess clinical data & draw a PTH level– Malignancy ROS– Family history (MEN)– History of PUD or pancreatitis– Symptoms of hypercalcemia
• PTHrP• Vit D metabolites
Diagnosis
• High-normal or elevated PTH– Primary Hyperparathyroidism– Lithium
• Low-normal or low PTH– All other causes
Diagnosis
• If normal levels of PTH & PTH-rp• No evidence of malignancy• Vitamin D metabolites
– Calcidiol & calcitriol• Elevated in Vitamin D intoxication• Calcitriol also elevated in
granulomatous disease & lymphoma
Diagnosis
• SPEP/UPEP– Multiple myeloma
• TSH• Vitamin A• Serum phosphate• Urinary calcium excretion
– Hyperparathyroidism– Humoral hypercalcemia of malignancy
• PTHrP related
Diagnosis
• Urinary Calcium level• High or high-normal
– Hyperparathyroidism– Malignancy
• Relative hypocalciuria (< 100 mg/day)– Milk Alkali– Thiazides– FHH
Treatment
• Mild Hypercalcemia <12 mg/dL– Does not require immediate treatment– Avoid aggravating factors
• Thiazide• Lithium• Volume depletion• Bedrest• High calcium diet
Treatment
• Moderate Hypercalcemia 12-14 mg/dL– Asymptomatic or mild symptoms do not
require immediate treatment– Avoid aggravating factors– Acute rise or change in sensorium require
treatment
Treatment
• Severe hypercalcemia >14 mg/dL– Volume expansion
• Initial rate 200-300 mL/hr• Adjust to UOP 100-150 mL/hr
– Renal failure or CHF• Consider furosemide
– Calcitonin• 4 IU/kg initial dose, repeat Ca in several hours• If response then 4-8 IU/kg Q6-12hr
Treatment
• Calcitonin and saline works fast, decrease Ca in 12 to 48 hrs
• Zoledronic Acid– 4mg IV over 15 mins
• Pamidronate– 60 to 90 mg IV over 2 hours
• Lymphoma, sarcoid, CGD– Low calcium diet, steroids, treat underlying
dz
Treatment
• H.D. if severe hypercalcemia (18-20)