Embed Size (px)
Citation preview

Kidney International, Vol. 61 (2002), pp. 564–569
Cerebral blood flow and vasodilatory capacity in anemiasecondary to chronic renal failure
YASUO KUWABARA, MASAYUKI SASAKI, HIDEKI HIRAKATA, HIROFUMI KOGA,MAKOTO NAKAGAWA, TAO CHEN, KOICHIRO KANEKO, KOUJI MASUDA, andMASATOSHI FUJISHIMA
Departments of Clinical Radiology and Second Internal Medicine, Graduate School of Medical Sciences,Kyushu University, Fukuoka, Japan
Cerebral blood flow and vasodilatory capacity in anemia sec- hypoxia, which thus increases cerebral blood flow (CBF)ondary to chronic renal failure. [1, 2]. However, if CBF does not increase adequately,
Background. Our previous study reported that cerebral oxy- the cerebral oxygen extraction fraction (OEF) may in-gen extraction fraction (OEF) increased in hemodialysis pa-crease in compensation so that the oxygen metabolismtients with anemia. The increased OEF suggests that the cere-of the brain can be maintained. We have already re-bral vasodilatory capacity might be impaired in these patients.
To clarify this issue, we measured the CO2 response in patients ported that both CBF and OEF increased in anemicwith anemia secondary to chronic renal failure (CRF) using patients on hemodialysis, and decreased after the correc-positron emission tomography (PET).
tion of anemia with recombinant human erythropoietinMethods. Ten anemic patients with CRF (6 females and 4[3]. These results suggest that the cerebral vasodilatorymales) and 6 age-matched normal controls were studied. The
underlying diseases of CRF were glomerulonephritis in 8 pa- capacity might be impaired in anemic patients who aretients, systemic lupus erythematosus (SLE) in one patient, and on hemodialysis. To clarify this issue, we measured thehypertension in one patient; in this cohort, 5 patients were on cerebrovascular response to hypercapnia (CO2 response)hemodialysis treatment and the remaining 5 patients were in
induced by 5% CO2 inhalation using O-15 H2O positrona pre-hemodialysis state. The cerebral blood flow (CBF) wasmeasured by the O-15 H2O bolus injection method with each emission tomography (PET) in patients who were ane-patient in a resting state and during 5% CO2 inhalation. The mic secondary to CRF. Then we studied correlation ofCO2 response was estimated as the percentage change of CBF the cerebrovascular reactivity with CBF, OEF, cerebralper 1 mm Hg change of PaCO2.
metabolic rate for oxygen (CMRO2) and cerebral bloodResults. The CO2 response was significantly attenuated in ane-volume (CBV) with each subject at rest.mic patients with CRF in comparison to the normal controls,
and it inversely correlated with the severity of anemia. Therewas no significant difference in the CO2 response between thehemodialysis and pre-hemodialysis patients. The CO2 response METHODSsignificantly correlated with CBF and the cerebral metabolic
The subjects consisted of ten anemic patients withrate for oxygen (CMRO2) at rest, however, it did not correlateCRF, six females and four males aged 42- to 70-years-with OEF and cerebral blood volume (CBV).
Conclusions. The present study revealed the existence of a old, and six age-matched normal controls. The underlyingreduced cerebral vasodilatory capacity in anemic patients with diseases of CRF were glomerulonephritis in eight patients,CRF, suggesting that chronic hypoxic brain damage might play
systemic lupus erythematosus (SLE) in one patient anda role in the impaired cerebrovascular response to CO2.hypertension in one patient. Among the patients, five wereon hemodialysis therapy (hemodialysis), and the remain-ing five never underwent hemodialysis (pre-hemodialy-Chronic renal failure (CRF) causes secondary anemiasis). Antihypertensive drugs were discontinued threedue to a decrease in the erythropoietin production. Thedays before PET study was performed in the hyperten-decrease in cerebral oxygen supply results in brain tissuesive patients. None of patients showed any neurologicaldeficits at the time of PET study, and none had a historyKey words: oxygen extraction fraction, brain oxygen metabolism, he-
modialysis, hypoxic brain damage, cerebrovascular CO2 response. of transient ischemic attack or stroke. Either computedtomography (CT) or magnetic resonance imaging (MRI)Received for publication June 27, 2001was performed in four out of the ten patients. Threeand in revised form September 5, 2001
Accepted for publication September 6, 2001 patients showed multiple small white matter lesions onMRI without neurological signs. The remaining patient 2002 by the International Society of Nephrology
564

Kuwabara et al: Cerebral vasodilatory capacity in anemia 565
showed no organic lesions on CT. Mild cerebral atrophy to be the maximal O2 supply [11]. Arterial O2 contentwas calculated with oxygen saturation and Hb:was observed in one out of these four patients. The pa-
tients were divided into two groups according to the de-O2 supply � CBF � arterial O2 content
gree of anemia (namely, mild anemia, Hb 8.5 to 11 g/dL,and severe anemia, Hb �8.5 g/dL) groups, and further The statistical analysis was performed by one-waydivided into the on hemodialysis and pre-hemodialysis analysis of variance (ANOVA) and the post-hoc un-groups. The normal controls consisted of six healthy paired t test or Welch t test with unequal variance.volunteers who were social workers or medical doctors.
Positron emission tomography was performed with aRESULTSHEADTOME-III device, which had a spatial resolution
Mean values for age, arterial hemoglobin, hematocrit,of 8.2 mm in full-width at half maximum and simultane-arterial systolic and diastolic blood pressures, and PaCO2ously obtained five contiguous slices 15 mm apart. Theat rest and during 5% CO2 inhalation in each group aresubjects were placed in a supine position on the bed inshown in Table 1. The Hb and Hct levels in the patienta semi-dark room. A small canula was placed in the fem-groups were significantly lower than those of the controloral or ulnar artery for arterial blood sampling. A trans-subjects, although there were no significant differencesmission scan with a Ge-68/Ga-68 ring source was ob-between the patients on hemodialysis and pre-hemodial-tained for each patient for attenuation correction. CBFysis patients. PaCO2 increased by 5 to 7 mm Hg and sys-was measured by the O-15 H2O bolus-injection methodtolic arterial blood pressure increased by about 20 mm Hg[4, 5], with the subject in a resting state and during theduring the 5% CO2 inhalation. The diastolic blood pres-inhalation of 5% CO2 with air at a 15 minute interval.sure at rest and the systolic pressure during 5% CO2In the O-15 H2O PET study, 740 MBq of O-15 H2Oinhalation in the pre-hemodialysis patients were signifi-was infused as a bolus and the scan was started whencantly higher than those on hemodialysis.radioactivity appeared on a monitor for the head. The
The average values for the CO2 response and CBF,data were collected for 75 seconds in each scan. ArterialOEF, CMRO2 and CBV at rest in the normal control andblood was continuously drawn at a rate of 15 mL/minpatient groups are shown in Table 2. The CO2 responsefor two minutes, and radioactivity was recorded by asignificantly decreased in all patient groups in compari-beta-ray detector system using a plastic scintillator (1.1son to that in the normal controls. The average valuecm thick and 5.1 cm in diameter). The dispersion andfor CO2 response was the lowest in the severe anemiatime delay of the input function were corrected accordinggroup, although there were no significant differences into the method of Iida et al [6]. The fixed time constantCO2 response between the hemodialysis and pre-hemo-(10 s) was used for the dispersion correction. CMRO2
dialysis patients.and OEF also were measured by the O-15 steady-stateCerebral blood flow at rest was significantly higher inmethod [7–10]. For the CBV measurement, a fixed ratio
both the severe anemia and hemodialysis patients thanof the central/peripheral hematocrit (0.85; Hct) was usedthat in the normal controls. Baseline CBF was also sig-[9]. The O-15 H2O and O-15 steady-state PET studiesnificantly higher in the severely anemic patients than thatwere performed on the same day. CBF at rest was mea-in the mild anemic patients. There were no significantsured first, and then CBF during inhalation of 5% CO2
differences in CBF between the hemodialysis and pre-was measured at an interval of 15 minutes. Subsequently,hemodialysis patients. OEF was slightly higher in theOEF, CMRO2 and CBV were measured by the O-15
steady-state method. Hemodialysis was performed in the patient groups than in the normal controls, however,this difference was not significant. CMRO2 significantlymorning the day before the PET study was performed
in hemodialysis patients. This study was approved by decreased in both patients with severe anemia and hemo-dialysis, compared to that that in the normal controls.the committee for the clinical application of cyclotron
producing radionuclides in Kyushu University Hospital, CMRO2 was significantly lower in the severely anemicpatients than that in the mildly anemic patients. CBVand informed consent was obtained from all patients
before undergoing the PET study. showed no significant difference between the patientgroups and the normal controls.The regions of interest (ROI) over the cerebral hemi-
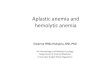
spheres were set at a level of 50 mm above the orbitomet- The relationship between the CO2 response and arte-rial hematocrit was well correlated (r � 0.79, P � 0.001;eral line. CO2 response was expressed as the percent
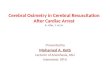
change of CBF per 1 mm Hg of PaCO2. The cerebral O2 Fig. 1). Figure 2 shows correlations between the CO2
response with CBF at rest (Fig. 2A), OEF (Fig. 2B),supply was calculated by the following equation. TheCBF value was corrected by PaCO2 based on the cereb- CMRO2 (Fig. 2C) and CBV (Fig. 2D). The CO2 response
correlated significantly with CBF at rest (r � �0.66, P �rovascular response rate to hypercapnia, and the cerebralO2 supply at a level of 80 mm Hg of PaCO2 was assumed 0.01) and CMRO2 (r � 0.68, P � 0.001), while it did not

Kuwabara et al: Cerebral vasodilatory capacity in anemia566
Table 1. The age, hemoglobin (Hb), hematocrit (Hct), PaCO2 at the resting state and during 5% CO2 inhalation, systolic and dyastolicblood pressures in the control subjects, mild and severe anemic patients, and patients on hemodialysis and pre-hemodialysis
PaCO2 mm Hg
Arterial blood pressure mm Hg
At rest 5% CO2 loadAge Hb Hct
Group years g/dL % At rest 5% CO2 load Systolic Diastolic Systolic Diastolic
Control (N�6) 56�10 13.0�1.4 38.5�4.2 41.3�4.4 46.5�4.9 127�16 68�11 145�23 80�13Mild anemia (N�5) 49�8 10.3�0.8c 31.6�3.5b 37.8 �4.0 44.2�2.8 142�24 80�23 166�26 83�25Severe anemia (N�5) 54�10 6.8�1.1d 20.8�3.0d 39.3 �3.2 45.2�3.2 137�42 69�21 156�41 80�22Hemodialysis (N�5) 46�7 8.1�2.6b 25.4�8.7b 39.7 �2.6 45.0�1.3 125�30 58�12 139�22 67�13Pre-hemodialysis (N�5) 57�8 9.0�1.5c 27.0�4.3c 37.3 �4.1 44.4�4.1 154�30 91�15a 184 �26a 97�15
Data are mean � SD.a 5% significant; b 2% significant; c 1% significant; d 0.1% significant compared with the control based on the t test or Welch t test
Table 2. Average values of the cerebrovascular response to hypercapnia (CO2 response), cerebral blood flow (CBF), oxygen extractionfraction (OEF), cerebral metabolic rate for oxygen (CMRO2), and cerebral blood volume (CBV)
CO2 response CBF at rest OEF CMRO2 CBV%/mm Hg mL/min/100 mL % mL/min/100 mL mL/100 mL
Control (N�6) 5.26�0.82 37.0�5.5 42.2�3.3 2.43�0.22 4.23�0.57Mild anemia (N�5) 2.99�1.06b 43.8�5.4 45.0�6.3 2.22�0.32 4.28�0.79Severe anemia (N�5) 2.02�0.93c 55.9�7.1b 46.8 �3.4 1.63�0.36b 3.94 �0.34Hemodialysis (N�5) 2.41�1.08b 52.5�9.4a 46.9 �6.4 1.74�0.41a 4.21 �0.73Pre-hemodialysis (N�5) 2.60�1.18b 47.2�8.2 44.9�3.3 2.12�0.44 3.95�0.33
Data are mean � SD.a 2% significant; b 1% significant; c 0.1% significant compared with the control based on the t test or Welch t test
0.001), and it also decreased in both the hemodialysis(P � 0.01) and pre-hemodialysis (P � 0.05) patients incomparison to the normal controls.
DISCUSSION
Several investigators have studied the cerebral hemo-dynamic changes in anemic patients with CRF [1, 2,12–14]. Heyman, Patterson and Jones used the N2O tech-nique and reported that CBF was normal in uremic pa-tients with minimal vascular involvement [12], while us-ing the same technique, Scheinberg reported increasedCBF in uremic patients [13], which was probably due toassociated anemia. Using the Xe-133 inhalation method,Mathew et al [1] and Vorstrup et al [2] reported anincrease in CBF in patients with dialysis encephalopathyand in anemic patients on long-term hemodialysis, re-Fig. 1. Relationship between the carbon dioxide (CO2) response and
hematocrit (Hct) levels. A close correlation is observed (r � 0.79, P � spectively. We also have reported that both the CBF0.001). and OEF in hemodialysis patients, measured by the O-15
steady state method and PET, increased before and de-creased after anemia was corrected with recombinanthuman erythropoietin [3]. Our present study, togethersignificantly correlate with either OEF (r � �0.37) orwith the previous study, found a significant increase inCBV (r � 0.22).CBF in patients with severe anemia that can be explainedThe cerebral O2 supply at rest and at hypercapniaby both brain tissue hypoxia and a reduction of blood(maximal dilation) is revealed in Table 3. There was aviscosity. It remains controversial as to which mechanismsignificant decrease in the cerebral O2 supply at rest inworks more dominantly. However, according to the studythe severe anemic patients in comparison to the normalby Waschke et al [abstract; J Cereb Blood Flow Metabcontrols (P � 0.05). The maximal O2 supply to the brain
significantly decreased in severe anemic patients (P � 15(Suppl 1):S73, 1995], the change in viscosity per se did

Kuwabara et al: Cerebral vasodilatory capacity in anemia 567
Fig. 2. Correlations between carbon dioxide(CO2) and cerebral blood flow (CBF), oxygenextraction fraction (OEF), cerebral metabolicrate for oxygen (OMRO2), and cerebral bloodvolume (CBV). (A) The correlation betweenCO2 response and CBF at rest. The cerebro-vascular response was significantly correlatedwith CBF at rest (r � �0.66, P � 0.01). (B)The correlation between CO2 response andOEF. No significant correlation was observedbetween them (r � �0.37, NS). (C ) The corre-lation between CO2 response and CMRO2.The cerebrovascular response was signifi-cantly correlated with CMRO2 (r � 0.68, P �0.001). (D) The correlation between CO2 re-sponse and CBV. There was no significantcorrelation between them (r � 0.22, NS).
Table 3. Cerebral oxygen supply at rest and at maximal vasodilation supply at rest was relatively well preserved by the com-pensatory increase in CBF, although it significantly de-Cerebral oxygen supply
mL/min/100 mL creased in the severely anemic patients. However, theAt rest At maximal dilationa calculated maximal O2 supply based on the CO2 response
was severely depressed in the patient groups. These re-Control (N�6) 6.24�0.94 18.9�3.76Mild anemia (N�5) 5.93�1.09 13.7�4.64 sults also indicate that these anemic patients are suscepti-Severe anemia (N�5) 4.92�0.87b 8.94�1.92d
ble to hypoxia regarding conditions of high O2 demand.Hemodialysis (N�5) 5.36�1.18 10.7�3.84c
Oxygen extraction fraction (OEF) is an indicator ofPre-hemodialysis (N�5) 5.49 �1.08 11.9�4.91b
the uncoupling of the blood flow to the energy metabo-Data are mean � SD.a At 80 mm Hg of PaCO2 lism, and the increased OEF means that CBF or cerebralb 5% significant; c 1% significant; d 0.1% significant compared with the control O2 supply is insufficient for the O2 demand of the brain.based on the t test or Welch t test
If CBF increases adequately, then the cerebral O2 supplybecomes sufficient to meet the O2 demand, and thereaf-ter OEF returns to normal. As a result, an increase in
not change the hypoxia-induced increase in CBF. As a OEF indicates that cerebral vasodilatory capacity is im-result, the brain tissue hypoxia due to insufficient O2 paired. In the present study, the mean value for OEFdelivery to the brain is thought to be a more important was about 10% higher in the patient groups than infactor to increase CBF in anemic patients. the normal controls; however, there was no significant
Thus far, very few reports have been published on increase in OEF. We also studied the correlation be-cerebral vasoreactivity in anemic patients with CRF. tween CO2 response and OEF, and, contrary to our pre-Gottstein, Held and Sedlmeyer reported that the cere- diction, no significant correlation was observed betweenbrovascular response decreased in the induced hemodi- them. The reason for lack of correlation is not clear, butlution [15], and Heyman, Patterson and Jones described the CO2 response can decrease without increased OEF.increased cerebral vascular resistance in uremic patients In addition, a wide variation was observed in the re-[12]. Our present study demonstrated that the CO2 re- sponse rate in higher OEF group (Fig. 2).sponse decreased in both mild and severe anemic pa- The CO2 response consistently decreased in all groupstients with CRF, and closely correlated with the severity of patients. However, the mechanism of the decreased
CO2 response seems to be complex in anemic patientsof anemia (Fig. 1). On the other hand, the cerebral O2

Kuwabara et al: Cerebral vasodilatory capacity in anemia568
with CRF. Hypertension, one of the major complications sponse correlated well with CMRO2 [22]. As a result,of the CRF, causes arteriosclerosis [16]. As a result, chronically exposed hypoxic brain damage, including in-hypertension may reduce the cerebral vasodilatory ca- sufficient CBF due to cerebrovascular changes, is consid-pacity in our patients, although the systolic and diastolic ered to play a very important role in the decreased cereb-blood pressures of the patient groups were not signifi- rovascular CO2 response. Neurological tests revealed thecantly higher than those of the normal controls. The relationship between the memory function and the dura-blood pressure at admission was not significantly high tion of dialysis [23]. The treatment of anemia with recom-(data not presented). Hemodialysis also may affect the binant human erythropoietin improved brain and cogni-cerebral structure and hemodynamics. Cusmano and Sa- tive function after normalization of Hct levels [24]. Thesevazzi reported that cerebral cortical atrophy was ob- results indicate the importance of early detection andserved on CT in 56.5% of hemodialyzed patients, and treatment of anemia in CRF patients.the degree of atrophy also correlated with the duration Our present study shows that there is a decrease inof hemodialysis [17]. Gottlieb et al reported that CBF the cerebral vasodilatory capacity in anemic patients withdecreased after hemodialysis [14]. However, we could CRF. These findings will be helpful for better under-not find any difference in CO2 response between the pre- standing the pathophysiology and management of thesehemodialysis and hemodialysis patients. patients.
There seem to be two major explanations for the de-creased CO2 response in anemic patients with CRF. One ACKNOWLEDGMENTSis that the resistant vessels already have been dilated
We express our thanks to Mr. Toshimitsu Fukumura for the produc-fully by the brain tissue hypoxia, and thus they could not tion of O-15 H2O and Ms. Naoko Kinukawa for assistance in performing
the statistical analysis of the PET data.dilate any further extent with the hypercapnia stimuli. Toconfirm this hypothesis, we searched for a correlation of
Reprint requests to Yasuo Kuwabara, M.D., Department of Clinicalthe CO2 response with CBV at rest, and found none. It Radiology, Graduate School of Medical Sciences, Kyushu University,is well known that the primary vascular adaptation to Maidashi 3-1-1, Higashi-ku, Fukuoka 812-8582, Japan.
E-mail: [email protected] is an increase in capillary density [18]. However,the change in CBV is rheologically smaller than that of
REFERENCESCBF in the response to vasodilator (Hagen-Poiseuille equa-tion). In addition, the increased CBV may be masked 1. Mathew RJ, Rabin P, Stone WJ, Wilson WH: Regional cerebral
blood flow in dialysis encephalopathy and primary degenerativeby methodological problems. The ratio of the central/dementia. Kidney Int 28:64–68, 1985peripheral hematocrit may change with the levels of pe-
2. Vorstrup S, Lass P, Waldemar G, et al: Increased cerebral bloodripheral hematocrit [19]. We used a fixed ratio of 0.85, flow in anemic patients on long-term hemodialytic treatment.
J Cereb Blood Flow Metab 12:745–749, 1992because we could not directly measure the ratios for3. Hirakata H, Yao H, Osato S, et al: CBF and oxygen metabolismindividual subjects. This may have underestimated the
in hemodialysis patients: Effects of anemia correction with recom-CBV value with the patient at rest. Another explanation binant human EPO. Am J Physiol 262:737–743, 1992is that the degree of hypoxia-induced organic brain dam- 4. Huang SC, Carson RE, Phelps ME: Quantitative measurement
of local cerebral blood flow in humans by positron emission tomog-age may reduce the cerebral vasodilatory capacity, andraphy and 15O-water. J Cereb Blood Flow Metab 3:141–153, 1983chronic hypoxia causes various structural alterations. In 5. Kanno I, Iida H, Miura M, et al: A system for cerebral blood
addition, a high CBF increases the delivery of uremic flow measurement using an H215O autoradiographic method and
positron emission tomography. J Cereb Blood Flow Metab 7:143–toxins to the brain, and thus may cause brain tissue dam-153, 1987age [20]. A pathological study revealed neuronal loss
6. Iida H, Kanno I, Miura S, et al: Error analysis of a quantitativeor degeneration without focal glial proliferation or a cerebral blood flow measurement using H2
15O autoradiographyand positron emission tomography, with respect to the dispersionthickening of the wall of arterioles, although no specificof the input function. J Cereb Blood Flow Metab 6:536–545, 1986change to this condition was observed (abstract; Olsen
7. Frackowiak RSJ, Lenzi GL, Jones T, Heather JD: Quantita-S, Acta Psychiatr Scand 36(Suppl):119–122, 1961). In the tive measurement of regional cerebral blood flow and oxygen me-present study, multiple small white matter lesions were tabolism in man using 15O and positron emission tomography:
theory, procedure and normal values. J Comput Assist Tomogr 4:demonstrated in three out of four patients who under-727–736, 1980went an MRI examination. The presence of white matter 8. Lammertsuma AA, Jones T: Correction for the presence of intra-
lesions in these patients indicates organic brain damage, vascular oxygen extraction ratio in the brain: 1. Description of themethod. J Cereb Blood Flow Metab 3:416–424, 1983although white matter lesions also can be observed in
9. Phelps ME, Huang SC, Hoffman EJ: Validation of tomographicvarious other conditions [21]. CMRO2 shows a close rela-measurement of cerebral blood volume with C-11 labeled carboxy-
tionship with organic brain damage: CMRO2 decreased hemoglobin. J Nucl Med 20:328–334, 197910. Kuwabara Y, Ichiya Y, Sasaki M, et al: Cerebral blood flow andin both the severe anemia and hemodialysis patients in
vascular response to hypercapnia in hypertensive patients with leu-comparison to the normal controls, and the CO2 responsekoaraiosis. Ann Nucl Med 10:293–298, 1996
significantly correlated with CMRO2. Fujishima et al, 11. Harper AM, Glass HI: Effect of alteration in the arterial carbondioxide tension on the blood flow through the cerebral cortexusing the N2O technique, also reported that CO2 re-

Kuwabara et al: Cerebral vasodilatory capacity in anemia 569
at normal and low arterial blood pressures. J Neurol Neurosurg to hypoxia in the rat. Oxygen Transport to Tissue XIX. New York,Plenum Press, 1997, pp 163–167Psychiatry 28:449–452, 1965
19. Levin VA, Ausman JI: Relationship of peripheral venous hemato-12. Heyman A, Patterson JL, Jones RW: Cerebral circulation andcrit to brain hematocrit. J Appl Physiol 26:433–437, 1969metabolism in uremia. Circulation 3:558–563, 1951
20. Marsh JT, Brown WS, Wolcott D, et al: rHuEPO treatment13. Scheinberg P: Effects of uremia on cerebral blood flow and metab-improves brain and cognitive function of anemic dialysis patients.olism. Neurology 4:101–105, 1951Kidney Int 39:155–163, 199114. Gottlieb D, Midworf B, Rubinger D, Melamed E: The regional
21. Awad IA, Johnson PC, Stetzler RF, Hodak JA: Incidental sub-cerebral blood flow in patients under chronic hemodialytic treat-cortical lesions identified on magnetic resonance imaging in thement. J Cereb Blood Flow Metab 7:659–661, 1987elderly. II. Postmortem pathological correlations. Stroke 17:1090–15. Gottstein U, Held K, Sedlmeyer I: Cerebral and peripheral blood1097, 1986flow as affected by induced hemodilution, in Hemodilution: Theo- 22. Fujishima M, Scheinberg P, Busto R, Reinmuth OM: The relation
retical Basis and Clinical Application, Basel, S. Karger, 1972, p 247 between cerebral oxygen consumption and cerebral vascular reac-16. Kannel WB, Wolf P, Dawber TR: Hypertension and cardiac tivity to carbon dioxide. Stroke 2:251–257, 1971
impairments increase stroke risk. Geriatrics 33:71–83, 1978 23. Gilli P, De Bastiani P: Cognitive function and regular dialysis17. Cusmano F, Savazzin GM: Cerebral computed tomography in treatment. Clin Nephrol 19:188–192, 1983
uremic and hemodialyzed patients. J Comput Assist Tomogr 4: 24. Marsh JT, Brown WS, Wolcott D, et al: rHuEPO treatment567–570, 1986 improves brain and cognitive function of anemic dialysis patients.
Kidney Int 39:155–163, 199118. LaManna JC, Harik SI: Brain metabolic and vascular adaptations