Embed Size (px)
Citation preview
Chapter 9. Benign Prostate Disorders
INTRODUCTIONThe prostate is an organ linked inextricably with the endocrine system. During thedevelopment of the prostate, epithelium and mesenchyme are under the control oftesticular androgens, and interact to form an organised secretory organ. Furthermore,many of the disease processes are attributed to, and therapies aimed at the manipu-lation of, the endocrine system. The gland resides in the true anatomical pelvis andforms the most proximal aspect of the urethra. It has been stated that the prostategland is the male organ most commonly afflicted with either benign or malignantneoplasms [1]. Therefore, it is an organ with which every physician and surgeon needbe familiar. We will focus on benign prostatic hyperplasia (BPH), the most prevalentof benign disorders affecting the prostate.
EMBRYOLOGYThe development, growth and cytodifferentiation of the prostate are androgen de-pendent and occur via reciprocal mesenchymal-epithelial interactions, the latter re-ferring to a cell-cell interaction initiated during embryonic periods in which mes-enchyme (undifferentiated connective tissue) induces epithelial development, whilethe epithelium reciprocally induces mesenchymal differentiation [2].
In the developing prostate, urogenital sinus mesenchyme acting under the influenceof testicular androgens induces ductal morphogenesis, the expression of epithelialandrogen receptors, regulates epithelial proliferation and specifies the expression ofprostatic-lobe specific secretory proteins. Reciprocally, the developing prostatic ep-ithelium induces the differentiation and morphological patterning of smooth musclein the urogenital sinus mesenchyme [2]. In the prostate, it is traditional to considerandrogens as promoters of growth, while activin and TGFβ are regarded as potentgrowth inhibitors These factors do not act independently, however, and cross-talkoccurs between the signalling pathways at a sub-cellular level [3].
The first step in development of the prostate begins with the urogenital sinus mes-enchyme signalling to the epithelium, causing it to form epithelial buds. Androgensthen induce bud elongation, branching and epithelial differentiation [3]. Prenatally,the androgen receptor (AR) is expressed only in the mesenchyme, not in the ep-ithelium. Initial epithelial development is thus controlled via paracrine interactionswhere activation of stromal androgen receptors stimulates growth factors and in-duces growth in adjacent prostatic epithelial cells [4].
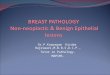
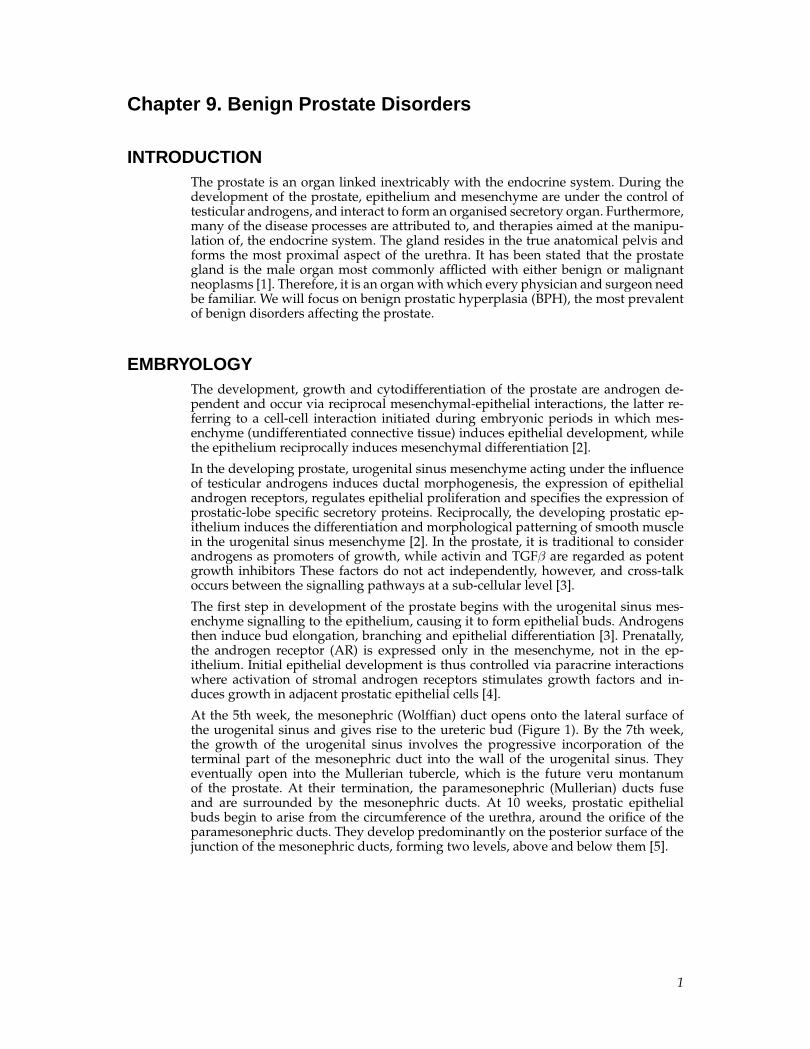
At the 5th week, the mesonephric (Wolffian) duct opens onto the lateral surface ofthe urogenital sinus and gives rise to the ureteric bud (Figure 1). By the 7th week,the growth of the urogenital sinus involves the progressive incorporation of theterminal part of the mesonephric duct into the wall of the urogenital sinus. Theyeventually open into the Mullerian tubercle, which is the future veru montanumof the prostate. At their termination, the paramesonephric (Mullerian) ducts fuseand are surrounded by the mesonephric ducts. At 10 weeks, prostatic epithelialbuds begin to arise from the circumference of the urethra, around the orifice of theparamesonephric ducts. They develop predominantly on the posterior surface of thejunction of the mesonephric ducts, forming two levels, above and below them [5].
1
Chapter 9. Benign Prostate Disorders
Figure 1. The embryological origin and development of the prostatic urethra andthe prostate (adapted from Delmas [5]).
During the fetal period at about 6 months, multiple outgrowths arise from the pro-static portion of the urethra, particularly the posterior surface of the urethra, andgrow into the surrounding mesenchyme. Glandular epithelium of the prostate dif-ferentiates from the endodermal cells of the urethra, and the associated mesenchymeinto which the outgrowths grow differentiates into the dense stroma and smoothmuscle fibres of the prostate. In contrast, the outgrowths situated on the anterior sur-face regress and are replaced by fibromuscular tissue. This region becomes the futureanterior commissure of the prostate [5, 6].
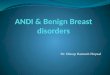
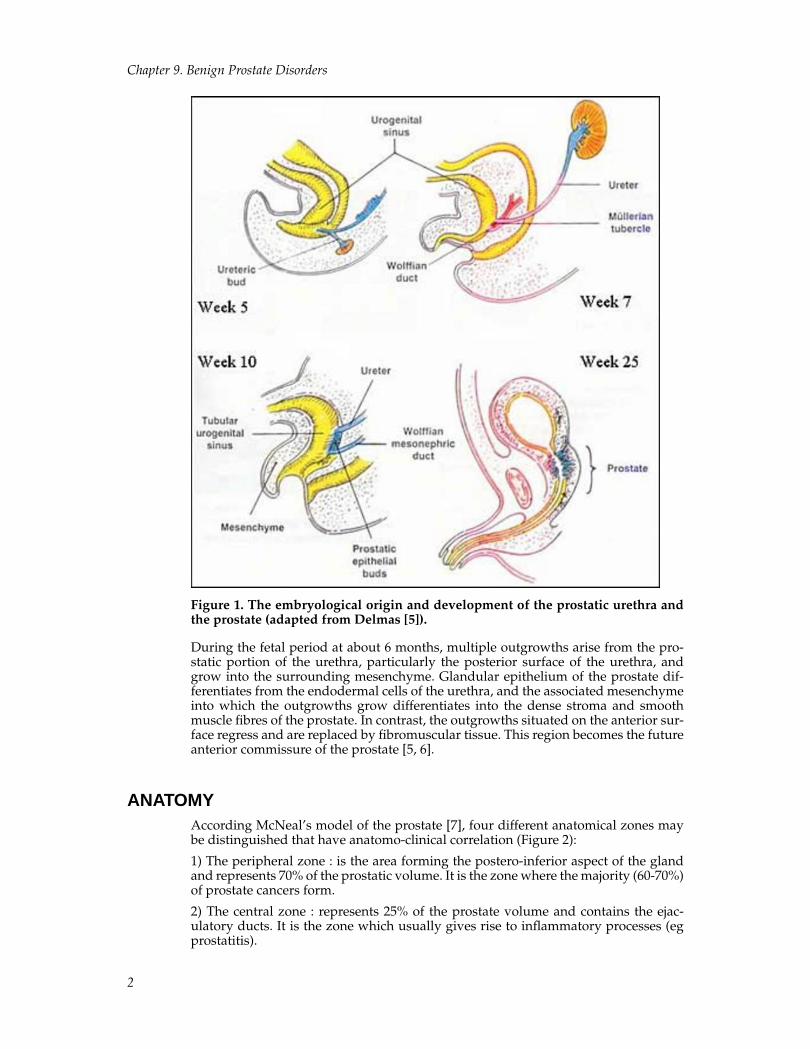
ANATOMYAccording McNeal’s model of the prostate [7], four different anatomical zones maybe distinguished that have anatomo-clinical correlation (Figure 2):
1) The peripheral zone : is the area forming the postero-inferior aspect of the glandand represents 70% of the prostatic volume. It is the zone where the majority (60-70%)of prostate cancers form.
2) The central zone : represents 25% of the prostate volume and contains the ejac-ulatory ducts. It is the zone which usually gives rise to inflammatory processes (egprostatitis).
2
Chapter 9. Benign Prostate Disorders
3) The transitional zone : this represents only 5% of the total prostatic volume. This isthe zone where benign prostatic hypertrophy occurs and consists of two lateral lobestogether with periurethral glands. Approximately 25% of prostatic adenocarcinomasalso occur it this zone.
4) The anterior zone : predominantly fibromuscular with no glandular structures.
The prostate weighs approximately 20g by the age of 20 and has the shape of aninverted cone, with the base at the bladder neck and the apex at the urogenital di-aphragm [8].The prostatic urethra does not follow a straight line as it runs throughthe centre of the prostate gland but it is actually bent anteriorly approximately 35degrees at the verumontanum (where the ejaculatory ducts joins the prostate) [9].
Figure 2. 1= Peripheral Zone, 2= Central Zone, 3= Transitional Zone, 4= AnteriorFibromuscular Zone. B= Bladder, U= Urethra, SV= Seminal Vesicle (adapted fromAlgaba[10]).
The Prostate “Capsule”It is widely accepted that an anatomically incomplete Denonvilliers’ fascia exists inthe region of the apex and some authors have questioned if an apical margin is a truepositive margin because the “capsule” of the prostate is deficient at the apex. Anotherimportant factor is the ‘detrusor apron’, a continuation of the anterior bladder wallwith the pubis, which constitutes a large portion of the anterior fibromuscular stroma. This stroma covers the entire anterior and anterolateral surface of the glandularprostate,
Kiyoshima and colleagues have extensively studied the prostate anatomy in 79 spec-imens to determine if a capsule does exist[11]. They found that Denonvilliers’ fas-cia and the prostatic capsule adhered tightly at the center of the posterior aspect in77 cases (97%). A smooth transition from the prostatic capsule to the anterior fibro-muscular stroma was observed in all cases. No prostatic capsule was independentlyrecognized at the anterior aspect in around 90% of cases because the prostatic tissuewas not distinct from the anterior fibromuscular stroma. In most cases (85%), the lat-eral pelvic fascia connected and fused with the anterior fibromuscular stroma, andcovered the outermost regions of the lateral and anterior surfaces. Also, the lateralpelvic fascia and the prostatic capsule were separated by adipose tissue in 41 cases(52%), whereas they adhered in 38 cases (48%).[11] In summary, there is a thickeningof the periphery of the prostate that some may regards as a “capsule”, but it is neither
3

Chapter 9. Benign Prostate Disorders
complete nor consistent amongst prostates and in many cases is difficult to discernfrom surrounding fascial layers.
Neurovascular anatomyThe autonomic nerves from the pelvic (inferior hypogastric) plexus supply theprostate. The plexus may be found two finger breadths lateral to the thirdanterior sacral foramina, lying deep to a line drawn from third sacral vertebra, theconventional level of the recto-sigmoid junction, and the palpable posterior superiorsurface of the pubic symphysis[12]. The prostatic “capsule” is covered by numerousnerve fibers and ganglia, which form a true periprostatic nerve network[13]. A studyof twenty autopsied prostates of different age (forties, fifties, sixties and seventies)and not having cancer has given insight into the more general neuranatomy ofthe prostate[14]. Most densely innervated was the prostate region bordering onthe neurovascular bundles (as discussed above), followed by the regions close tothe seminal vesicles and posterior capsule. Innervation was found to be relativelylow at the apex, dense in the inner zones and most rich in the outer regions. Theperipheral zone was more densely innervated than the transitional zone, while leastinnervation was found in BPH tissue. A further finding was that a decrease in nervedensity across all zones was demonstrated with increasing patient age.
Derived from the hypogastric plexus are the neurovascular bundles travelling adja-cent to (and within Denovilliers’ fascia) laterally on the prostate up to and includingthe apex. The role of these nerves in erectile function have been explored widely,particularly by Walsh[15-17] in the context of radical retropubic prostatectomy forcancer. The original assumption was that this neurovascular bundle is gathered atthe rectolateral side of the prostate[18]. However, research at several institutions inAustralia has demonstrated that the autonomic neurovascular bundles extend later-ally around the prostate and converge toward the apex but are in fact not a singlenerve but a plexus that has many divisions scattered throughout Denovilliers’ fascia,including medially towards the midline[19, 20]. It has been stated that one fifth to onequarter of nerves can be found along the ventral circumference of the prostatic cap-sule[18] and that only around half of prostates will have a definitive neurovascularbundle (in addition to the more scattered nerves as discussed)[11].
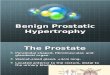
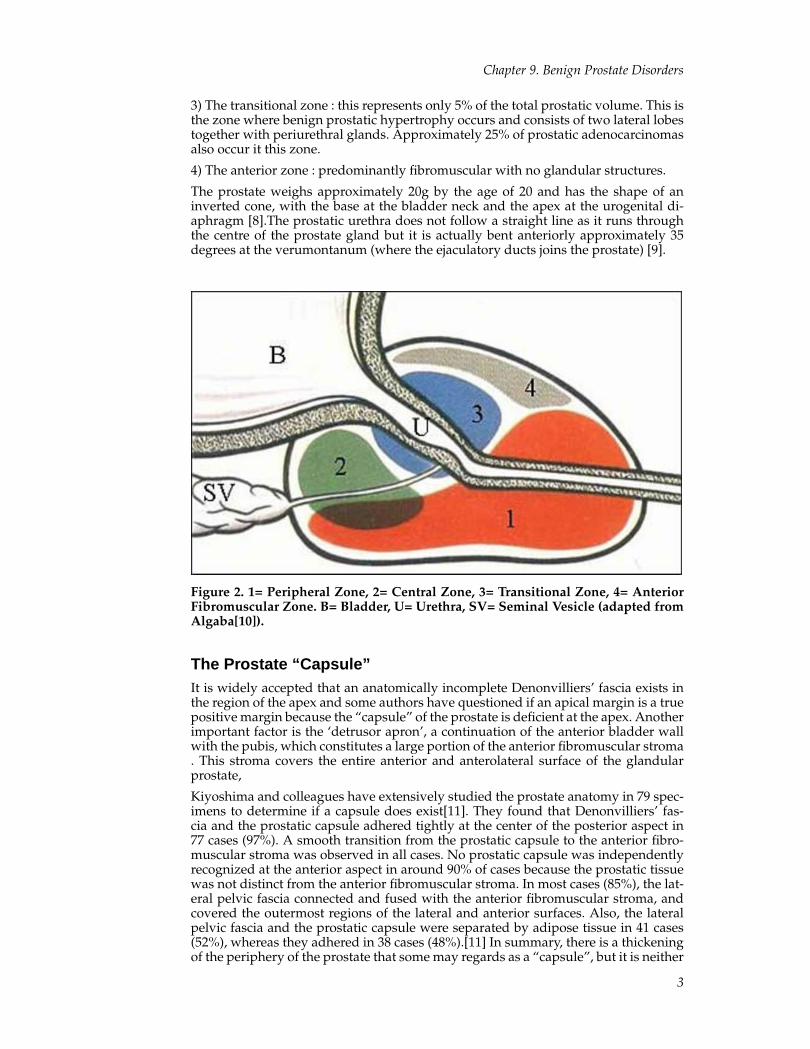
HISTOLOGYThe prostate consists of stromal and epithelial elements. Smooth muscle cells, fibrob-lasts and endothelial cells are in the stroma and the epithelial cells are secretory cells,basal cells and neuroendocrine cells (Figure 3).
4
Chapter 9. Benign Prostate Disorders
Figure 3. Histology of a prostate gland affected by benign prostatic hyperplasia.
The columnar secretory cells are tall with pale to clear cytoplasm. These cells stainpositively with prostate specific antigen[21]. Basal cells are less differentiated thansecretory cells and so are devoid of secretory products such as prostate-specific anti-gen (PSA)[22]. Finally, neuroendocrine cells are irregularly distributed throughoutducts and acini, with a greater proportion in the ducts .The prostate has the greatestnumber of neuroendocrine cells of any of the genitourinary organs[23]. Glands arestructured with open and closed cell types with the open type facing the inside ofthe duct having a monitoring role over its contents. Most cells contain serotonin butother peptides present include somatostatin, calcitonin, gene-related peptides andkatacalcin[21]. The cells co-express PSA and prostatic acid phosphatase. Their func-tion is unclear but it is speculated that these cells are involved with local regulationby paracrine release of peptides[21].Prostatic ducts and acini are distinguished by ar-chitectural pattern at low power magnification. The prostate becomes more complexwith ducts and branching glands arranged in lobules and surrounded by stroma withadvancing age
5
Chapter 9. Benign Prostate Disorders
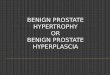
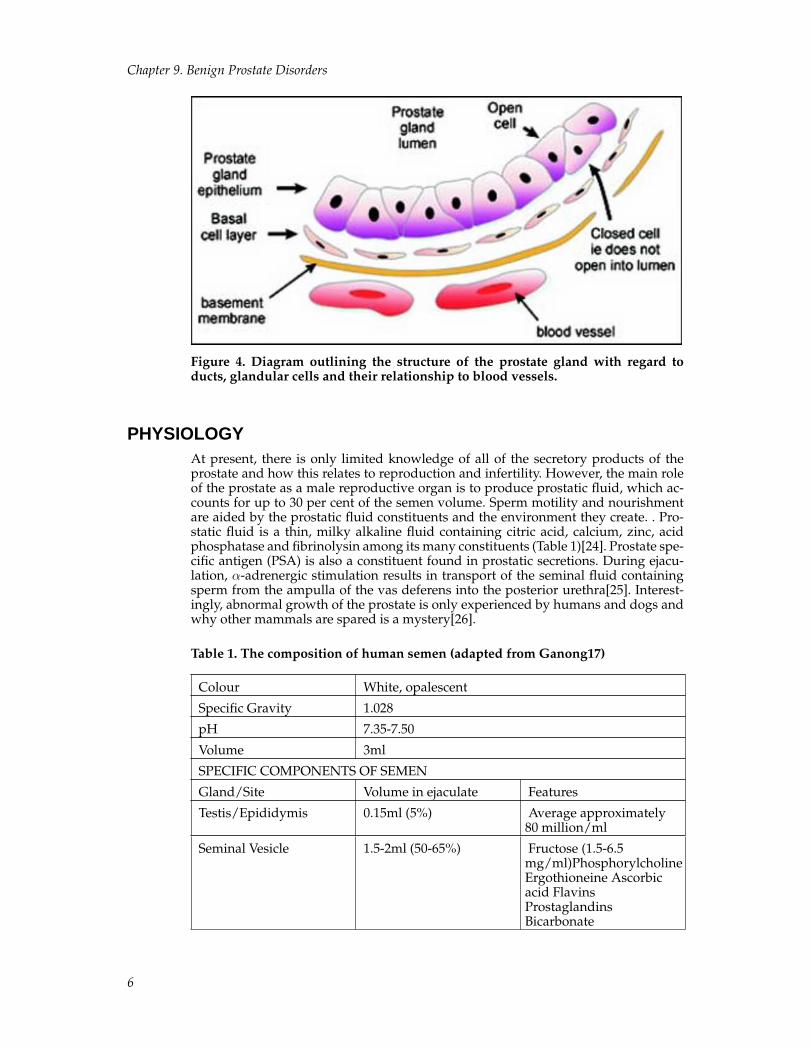
Figure 4. Diagram outlining the structure of the prostate gland with regard toducts, glandular cells and their relationship to blood vessels.
PHYSIOLOGYAt present, there is only limited knowledge of all of the secretory products of theprostate and how this relates to reproduction and infertility. However, the main roleof the prostate as a male reproductive organ is to produce prostatic fluid, which ac-counts for up to 30 per cent of the semen volume. Sperm motility and nourishmentare aided by the prostatic fluid constituents and the environment they create. . Pro-static fluid is a thin, milky alkaline fluid containing citric acid, calcium, zinc, acidphosphatase and fibrinolysin among its many constituents (Table 1)[24]. Prostate spe-cific antigen (PSA) is also a constituent found in prostatic secretions. During ejacu-lation, α-adrenergic stimulation results in transport of the seminal fluid containingsperm from the ampulla of the vas deferens into the posterior urethra[25]. Interest-ingly, abnormal growth of the prostate is only experienced by humans and dogs andwhy other mammals are spared is a mystery[26].
Table 1. The composition of human semen (adapted from Ganong17)
Colour White, opalescent
Specific Gravity 1.028
pH 7.35-7.50
Volume 3ml
SPECIFIC COMPONENTS OF SEMEN
Gland/Site Volume in ejaculate Features
Testis/Epididymis 0.15ml (5%) Average approximately80 million/ml
Seminal Vesicle 1.5-2ml (50-65%) Fructose (1.5-6.5mg/ml)PhosphorylcholineErgothioneine Ascorbicacid FlavinsProstaglandinsBicarbonate
6
Chapter 9. Benign Prostate Disorders
Prostate 0.6-0.9ml (20-30%) ProstateSpermineCitricAcidCholes-terol,phospholipidsFibrinolysin,fibrinogenaseZincAcidphosphateaseProstate-specific
Bulbourethral Glands < 0.15ml (<5%) Clear mucus
ENDOCRINE CONTROL OF PROSTATIC GROWTHIt is becoming clear that intraprostatic signalling systems are important for the reg-ulation of cell proliferation and extracellular matrix production in prostatic stroma.Central to this premise is the balance between factors such as tumour growth fac-tor β 1 (TGFb1), that induces extracellular matrix production, suppresses collagenbreakdown and cell proliferation and factors such as fibroblast growth factor 2 andinsulin-like growth factors that are mitogenic in the stromal compartment[28].Otherendocrine pathways are being investigated and there is experimental data suggestingan abnormality in the insulin-like growth factor axis playing a role in the pathogene-sis of BPH[29].
Other data has emerged on the relationship between connective tissue growth factor(CTGF) expression and fibronectin (FN) synthesis after transforming growth factor-β-1 (TGF-β1) stimulation in human prostate stromal cells. CTGF appears to play acrucial role in extracellular matrix production as a TGF-β1 downstream mediator inhuman prostate stromal cells, suggesting that CTGF blockade is likely to be a thera-peutic target against benign prostatic hyperplasia.[30]
TestosteroneProstatic epithelial cells express the androgen receptor[31]. From the beginning ofembryonic differentiation to pubertal maturation and beyond, androgens are a pre-requisite for the normal development and physiological control of the prostate[32].Androgens also help maintain the normal metabolic and secretory functions of theprostate. They are also implicated in the development of benign prostatic hyperpla-sia (BPH) and prostate cancer. Androgens do not act in isolation and other hormonesand growth factors are being investigated[33].
Androgens also interact with prostate stromal cells which release soluble paracrinefactors that are important in the growth and development of the prostate epithelium[4]. These paracrine pathways may be critical in regulation of the balance betweenproliferation and apoptosis of prostate epithelial cells in the adult[33].
The appropriate balance between testosterone and its 5 α reduced metabolites arekey to normal prostate physiology (note the metabolic pathways for androgenmetabolism are described in the Chapter 2 on Androgens by D Handelsman). Themetabolism of testosterone to dihydrotestosterone (DHT) and its aromatisation toestradiol are recognised as the key events in prostatic steroid response.
7
Chapter 9. Benign Prostate Disorders
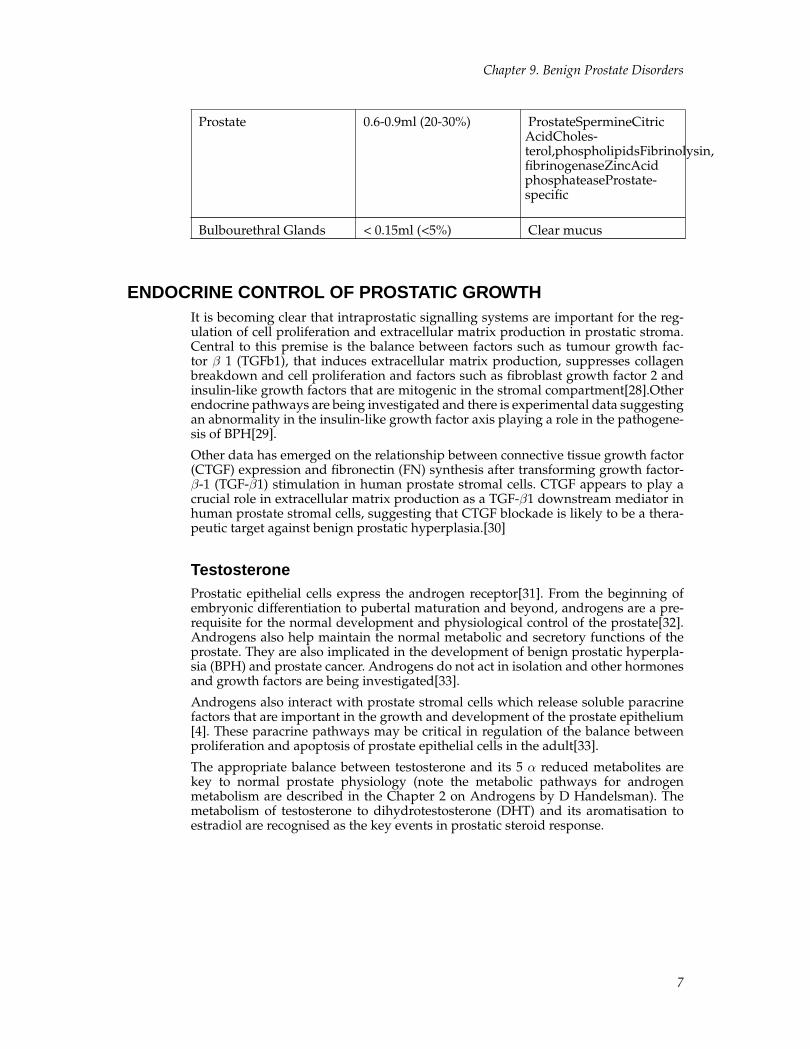
Figure 5. Conversion of testosterone to dihydrotestosterone (DHT) by 5α-reductase
Testosterone, to be maximally active in the prostate, must be converted todihydrotestosterone (DHT) by the enzyme 5α-reductase (Figure 5)[34]. DHT has amuch greater affinity for the androgen receptor than does testosterone [35, 36]. DHTis about twice as potent as testosterone in studies of rats at equivalent androgencconcentrations[37].DHT due to its greater affinity for the androgen receptormay have effects intraprostatically independent of serum fluctuations in serumtestosterone levels. [35, 36].
The impact of serum androgen manipulation on prostate tissue hormone levels innormal men is unknown. Studies of men with prostate cancer have suggested thatprostatic androgens are preserved in the setting of castration. Tissue androgens mightstimulate prostate growth, producing adverse clinical consequences.[38] In a smallstudy of healthy subjects, despite a 94% decrease in serum T with medical castration,intraprostatic T and dihydrotestosterone levels remained 20-30% of control values,and prostate cell proliferation, apoptosis, and androgen-regulated protein expressionwere unaffected. [38] Future therapies may need to take such findings into account ifthey are reproduced.
DHT concentrations may remain similar to those in young men in the prostate ofelderly men, despite the fact that serum testosterone levels may decline with age[34].In the prostate, the total level of testosterone is 0.4 ng/g and the total of DHT is 4.5ng/g[39]. The total concentration of testosterone in the blood (18.2nnmol/L[27]) isapproximately 10 times higher than that of DHT. Circulating DHT, by virtue of its lowserum plasma concentration and tight binding to plasma proteins, is of diminishedimportance as a circulating androgen affecting prostate growth[26].
EstrogenA role for estrogens in the prostate pathology of the ageing male appears likelywith accumulating evidence that estrogens, alone or in combination with androgens,are involved in inducing aberrant growth and/or malignant change. Animal mod-els have supported this hypothesis in the canine model, where estrogens “sensitize”the ageing dog prostate to the effects of androgen[40]. The evidence is less clear inhumans. Estrogens in the male are predominantly the products of peripheral arom-atization of testicular and adrenal androgens[41]. While the testicular and adrenalproduction of androgens declines with ageing, levels of total plasma oestradiol donot decline. This has been ascribed to the increase in fat mass with ageing (the pri-mary site of peripheral aromatization) and to an increased aromatase activity withageing. However, free or bioavailable estrogens may decline due to an increase in sexhormone binding globulin, which could translate to lower intraprostatic levels of thehormone. The potentially adverse effects of oestrogens on the prostate may be due toa shift in the intra-prostatic estrogen:androgen ratio with ageing.
Estrogen, which acts through estrogen receptors (ER) α and β, has been implicated inthe pathogenesis of benign and malignant human prostatic tumors[42-44]. As stated
8

Chapter 9. Benign Prostate Disorders
above benign prostatic hyperplasia is thought to originate in the transitional zone(TZ) and prostate cancer the peripheral zone (PZ) of the prostate. Receptor stud-ies have found ER-α and ER-β types distributed in human normal and hyperplas-tic prostate tissues, using in situ hybridization and immunohistochemistry. ER-α ex-pression was restricted to stromal cells of the PZ. In contrast, ER-β was expressedin the stromal and epithelial cells of PZ as well as TZ. These findings suggest thatestrogen may play a crucial role in the pathogenesis of benign prostatic hyperpla-sia through ER-β[43]. Investigations are ongoing and could result in a new range oftherapies directed against BPH and prostate cancer. Dietary phytoestrogens (in soyand other vegetables) or selective estrogen receptor modulators are currently beinginvestigated with regard to their role in the development of BPH and prostate can-cer[41]. Such ER modifiers may oppose some of the effects of natural oestrogen bymodulating ER receptors, thus reducing the local impact of androgens that need ac-tive ER receptors, effectively making them anti-androgenic compounds however thisrequires more investigation[45].
Benign Prostatic Hyperplasia (BPH)Benign Prostatic Hyperplasia (BPH) is an age-related and progressive neoplastic con-dition of the prostate gland[46]. BPH may only be defined histologically. BPH in theclinical setting is characterised by lower urinary tract symptoms (LUTS, see Table2). There is no causal relationship between benign and malignant prostatic hypertro-phy[47]. Clinically apparent BPH represents a considerable health problem for oldermen, due to the negative effects it has on quality of life (QOL). A recent study hasdemonstrated an overall prevalence of 10.3%, with an overall incidence rate of 15 per1000 man-years, increasing with age (3 per 1000 at age 45-49 years, to 38 per 1000 at75-79 years). For a symptom free man at age 46, the risk of clinical BPH over the com-ing 30 years, if he survives, is 45%[48]. The true prevalence and incidence of clinicalBPH will vary according to the criteria used to describe the condition. It is crucialto acknowledge that LUTS can exist without signs of BPH – as the symptoms canbe caused by variations in the sympathetic nervous stimulation of prostatic smoothmuscle, variability of prostatic anatomy (viz., enlarged median lobe of the prostate),and the variable effects of bladder physiology from the obstruction and aging.
There have been several studies demonstrating the fact that clinical BPH is a progres-sive disease. The Olmsted county study[49] showed that with each year there weredeteriorations in symptom scores, peak flow rates, and increases in prostate volumesbased on transrectal ultrasound scanning (TRUS). The risk of acute urinary retention(AUR) increased with flow rates below 12 ml/sec and with glands greater than 30ml.Studies have also demonstrated that those with larger prostates (>40 ml) and withserum PSA greater than 1.4 ng/ml were more likely to develop acute urinary reten-tion[50]. Treatment however has changed with the advent of effective non-surgicaltherapies. Between 1992-1998 there has been a significant lengthening of the periodbetween first diagnosis of LUTS secondary to clinical BPH and surgery, associatedwith the earlier and increased use of specific medical treatments [51]. From the pa-tients perspective the goals of therapy are to improve quality of life, reduce symp-toms, and avoid surgery while ensuring safety from the complications of BPH [52].
Risk Factors for BPHThe only clearly defined risk factors for BPH are age and the presence of circulatingandrogens. BPH does not develop in men castrated before the age of forty [53]. Butother factors may influence the prevalence of clinical disease. These include:
9
Chapter 9. Benign Prostate Disorders
GeneticsClinical BPH appears to run in families. If one or more first degree relatives are af-fected, an individual is at greater risk of being afflicted by the disorder [54]. In a studyby Sanda et al [55] the hazard-function ratio for surgically treated BPH amongst firstdegree relatives of the BPH patients as compared to controls was 4.2 (95% CI, 1.7 to10.2). The incidence of BPH is highest and starts earliest in blacks than Caucasiansand is lowest in Asians [47]. Interestingly, despite having larger prostate glands, theage-adjusted risk of BPH was the same for blacks as for whites (RR = 1.0, 95% Cl 0.8-1.2) [56]. Furthermore, in an Asian population, men presenting with BPH are likelyto have higher symptom scores than blacks or Caucasians [57].
DietDiet has been reported as a risk factor for the development of BPH. Large amountsof vegetables and soy products in the diet may explain the lower rate of BPH inthe orient when compared to westernized countries. In particular, certain vegetablesand soy are said to be high in phyto-oestrogens, such as genestin, that have ant-androgenic effects by an as yet determined mechanism on the prostate in vitro [58].
The study of migrant populations with their heterogeneous exposures to the en-vironment, increases the probabilities of identifying potential risk factors for BPH.Therefore, the association of alcohol, diet, and other lifestyle factors with obstructiveuropathy was investigated in a cohort of 6581 Japanese-American men, examinedand interviewed from 1971 to 1975 in Hawaii. After 17 years of follow-up, 846 inci-dent cases of surgically treated obstructive uropathy were diagnosed with BPH. Totalalcohol intake was inversely associated with obstructive uropathy (P < 0.0001). Therelative risk was 0.64 (95% confidence interval: 0.52-0.78) for men drinking at least25 grams of alcohol per month compared with nondrinkers. Among the 4 sourcesof alcohol, a significant inverse association was present for beer, wine, and sake, butnot for spirits. No association was found with education, number of marriages, orcigarette smoking. Increased beef intake was weakly related to an increased risk (p =0.047), while no association was found with the consumption of 32 other food itemsin the study [59].
Other Risk FactorsIt has not been possible to delineate any other risk factors for BPH such as coronaryartery disease, liver cirrhosis or diabetes mellitus. There is also no causal relationshipbetween prostatic malignancy and benign hyperplasia [47].
PATHOPHYSIOLOGY OF BPH
Natural HistoryBPH is a histological diagnosis but its clinical manifestations occur after growth hasoccurred to such a degree and in such a strategic location within the gland, namelythe transitional zone, that it impairs bladder emptying and results in LUTS. One cantherefore consider the natural history of BPH as involving three phases:
(i) The pathological or first phase of BPH is asymptomatic and involves a progressionfrom microscopic to macroscopic BPH. Microscopic BPH will develop in almost allmen if they live long enough but in only about half will progress to macroscopicBPH. This would suggest that additional factors are necessary to cause microscopicto progress to macroscopic BPH [60]. The pathological phase involves developmentof hyperplastic changes in the transitional zone of the prostate [61].
10

Chapter 9. Benign Prostate Disorders
(ii) The clinical or second phase of BPH involves the progression from pathologicalto ‘clinical BPH’ which is synonymous with the development of LUTS. Only aboutone half of patients with macroscopic BPH progress to develop clinical BPH [60].BPH consists of mechanical and dynamic components and it is these components thatare responsible for the progression from pathological to clinical BPH [62]. In clinicalBPH, the ratio of stroma to epithelium is 5: 1 whereas in the case of asymptomatichyperplasia the ratio is 2.7:1. A significant contribution is therefore made by stromato the infravesical obstruction of BPH [63]. While there is wide variability in prostategrowth rates on an individual level, prostate volume appears to increase steadily atabout 1.6% per year in randomly selected community men [64].
(iii). There is probably a third phase, during which clinical BPH progresses. This pro-gression may be defined as a deterioration of clinical variables such as lower urinarytract symptoms (LUTS), health-related quality of life and peak flow rate, increasedprostate size, or unfavourable outcomes such as acute urinary retention and BPH-related surgery [65]. However, there is evidence from longitudinal studies[49, 66],and to a lesser extent from the placebo arms of large controlled studies[67, 68], thatclinical BPH is a progressive disease. Symptom worsening is by far the most fre-quently occurring progression event. Identifying those patients at risk of BPH pro-gression is crucial to optimize their management [65].
AetiologySeveral theories have been proposed to explain the etiology of the pathological phaseof BPH. The major theories include the hypotheses that pathological BPH is dueto[69-71]: 1) Dihydrotestosterone (DHT) hypothesis- a shift in prostatic androgenmetabolism that occurs with aging, which leads to an abnormal accumulation of di-hydrotestosterone, thus producing the enlarged prostate. This is supported by thefauilure of BPH development in men castrated before puberty.
2) Embryonic reawakening theory- assumes a reawakening of the embryonic induc-tion potential of prostatic stroma. In summary, a change in the prostatic stromal-epithelial interaction that occurs with aging occurs, which leads to an inductive effecton prostatic growth.
3) Stem cell theory featuring an increase in the total prostatic stem cell numberand/or clonal expansion of the stem cells into amplifying and transit cells thatoccurs with aging.
4) Inflammatory theory- Prostatic inflammation may contribute to prostate growthdue to the induction of cell growth due to the presence of inflammatory markers andagents stimulating growth.
DISEASE MANIFESTATIONS OF BPH
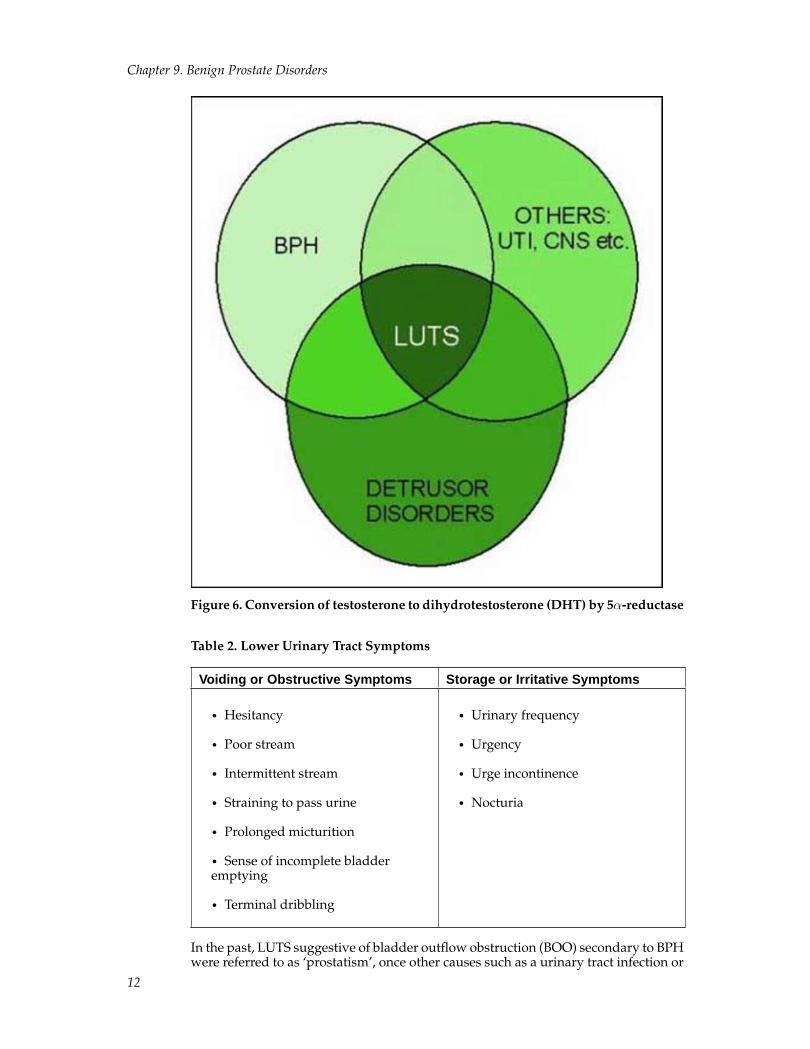
Lower Urinary Tract Symptoms (LUTS)Lower urinary tract symptoms (LUTS) suggestive of BPH are highly prevalent andthe majority of LUTS in men is produced by BPH, but may be contributed to by a va-riety of conditions (Fig. 5). LUTS are traditionally divided into voiding or obstructiveand storage or irritative symptoms (Table 2). Voiding symptoms are more common,however it is storage symptoms that are most bothersome and have a greater impacton a patient’s life[72, 73]. The prevalence of clinical BPH rises with age and approxi-mately 25% of men age 40 or over will suffer from LUTS [74].
11
Chapter 9. Benign Prostate Disorders
Figure 6. Conversion of testosterone to dihydrotestosterone (DHT) by 5α-reductase
Table 2. Lower Urinary Tract Symptoms
Voiding or Obstructive Symptoms Storage or Irritative Symptoms
• Hesitancy
• Poor stream
• Intermittent stream
• Straining to pass urine
• Prolonged micturition
• Sense of incomplete bladderemptying
• Terminal dribbling
• Urinary frequency
• Urgency
• Urge incontinence
• Nocturia
In the past, LUTS suggestive of bladder outflow obstruction (BOO) secondary to BPHwere referred to as ‘prostatism’, once other causes such as a urinary tract infection or
12

Chapter 9. Benign Prostate Disorders
prostate cancer were excluded. The pathology behind the symptoms was thought tobe obstruction due to prostatic gland enlargement alone. However, today it is recog-nised that voiding/obstructive symptoms result from direct urinary flow obstructionwhilst storage/irritative symptoms appear to be due to secondary bladder dysfunc-tion [76].
This concept has been further refined in that obstructive symptoms are thought toresult not only from mechanical obstruction due to glandular enlargement, but alsodynamic obstruction secondary to contraction of the smooth muscle of the prostate,urethra and bladder neck. This dynamic obstruction is a result of sympathetic ner-vous system mediated stimulation of α-1adrenoceptors. Storage symptoms appearto be caused by detrusor instability related to detrusor muscle changes in response toobstruction, such as bladder wall hypertrophy and collagen deposition in the blad-der[77, 78]. The role of adrenoceptor subtypes in the bladder in this process is cur-rently being investigated. Adrenoceptors may be further sub-divided into α
1Aand
α1D
subtypes, with α1A
predominant in the prostate and α 1D in the bladder. Thusblockade of α
1Amay be necessary for reduction of obstruction whereas the blockade
of α1D
may be required to relieve storage symptoms [79] (see below).
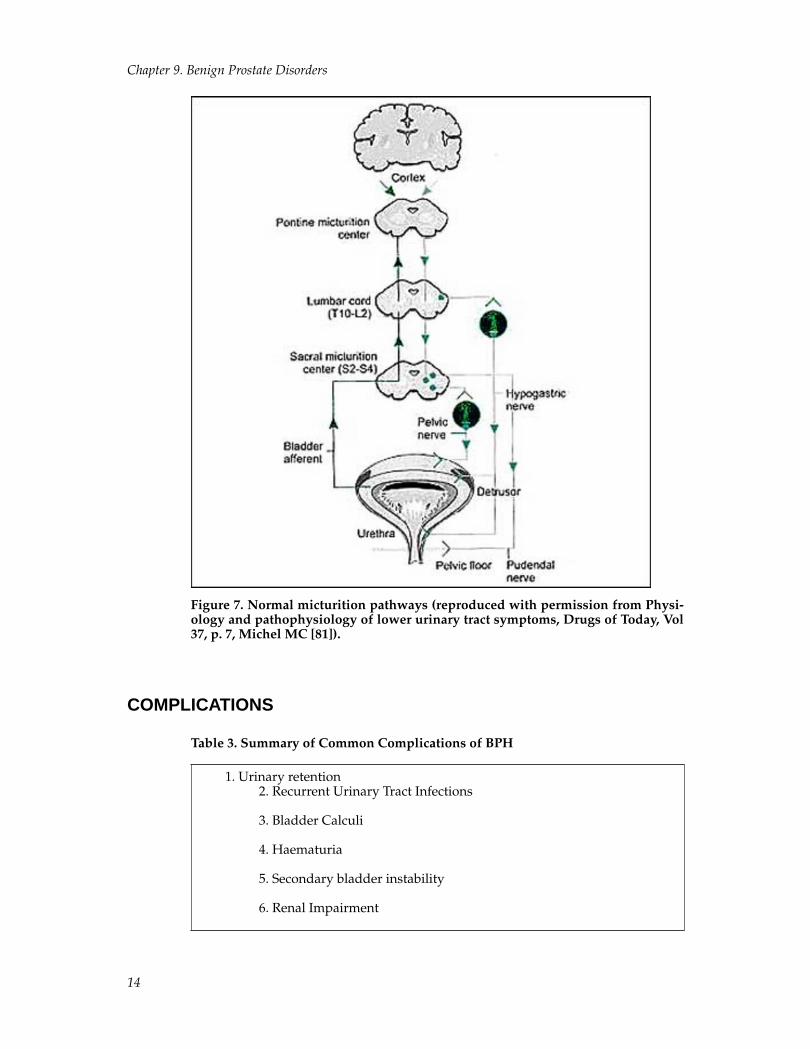
New research has also suggested that the aetiology of LUTS related to BPH is evenmore complex than outlined above with extra-prostatic mechanisms such as bladderwall ischaemia and changes in the central nervous system being implicated [80]. Nor-mal lower urinary tract function is complex, and theoretically any disruption of thepathway for micturition (Figure 7 below) may lead to LUTS [81].
It is also worth noting the relationship between LUTS and sexual dysfunction, withsexual dysfunction being highly prevalent in men with LUTS [82]. By sexual dys-function, we refer to decreased libido, erectile dysfunction, decreased ejaculation andother ejaculation disorders. Kassabian [83] expands on the relationship and agreeswith Leilefeld et al [84] in suggesting that the relationship is coincidental and bothare common in the ageing male.
13
Chapter 9. Benign Prostate Disorders
Figure 7. Normal micturition pathways (reproduced with permission from Physi-ology and pathophysiology of lower urinary tract symptoms, Drugs of Today, Vol37, p. 7, Michel MC [81]).
COMPLICATIONS
Table 3. Summary of Common Complications of BPH
1. Urinary retention2. Recurrent Urinary Tract Infections
3. Bladder Calculi
4. Haematuria
5. Secondary bladder instability
6. Renal Impairment
14

Chapter 9. Benign Prostate Disorders
Urinary Retention (Acute and Chronic)As prostate volume increase with age, the likelihood of acute urinary retention (AUR)and symptom severity both increase while urinary flow rates fall. In one study ofmore than 2000 men, those with a maximum urinary flow rate (Qmax) <12 ml/s hada 4 times greater risk for AUR than did men with a Qmax >12ml/s [85]. AUR is usu-ally painful and necessitates the insertion of a per urethral indwelling or suprapubicurinary catheter.
If the urinary retention is not dealt with in a timely fashion, the detrusor musclebecomes distended and damaged, contributing to poor detrusor function and an in-ability to adequately empty the bladder. The retention of urine becomes painless overtime, and the sequelae of retained urine such as recurrent UTI, calculi and renal im-pairment may develop.
Furthermore, a situation of overflow incontinence may develop whereby the bladderautomatically empties once the volume reached exceeds its new, larger capacity. Thepassage of urine is typically uncontrolled, and this may often be the first presentationfor someone with advanced BPH. The bladder remains full despite the emptying,which is only partial.
In situations of chronic retention, there is no guarantee that by relieving the bladderoutflow obstruction, the detrusor will return to normal functioning. These patientsoften need to use intermittent self catheterisation or have permanent drainage to keeptheir bladder empty and to reduce damage to the upper urinary tract, even afterdefinitive treatment for BPH.
Recurrent lower Urinary Tract Infection (UTI)Perhaps the best host defence against infection in the lower urinary tract is the nor-mal flow of urine and bladder emptying that accompanies normal urinary tract func-tioning. In BPH, bladder outflow obstruction results in disruption of this mechanismwith retention and pooling of urine in the bladder, giving organisms the opportunityto multiply rather than be flushed out. Despite this logical assumption, there is littleevidence in the literature to support this theory. Nevertheless, men with significantclinical BPH are probably at risk of UTI, and men with UTI should be assessed forsigns of BPH.
Bladder Calculi (stones)In developed countries, the most prevalent cause of bladder calculi is bladder out-let obstruction owing to BPH [86].Of those who undergo prostate surgery for BPH,approximately 2% of all patients are found to have bladder stones [87]. Stones oc-cur in this situation due to urinary stasis combined with high urinary solute con-centrations, which leads to crystal precipitation [88]. Chronic infection with urease-producing organisms may predispose to the development of stones and rarely stonespass from the upper tract to act as a nidus in the bladder [88] . Bladder calculi as-sociated with BPH remain an absolute indication for transurethral resection of theprostate (TURP)[89, 90] because of the risk or recurrence of stone formation. How-ever, the necessity of surgery is being challenged by the expanding use of medicalmanagement in treating BPH [90].
HaematuriaThe incidence of haematuria with BPH is uncertain however, in a retrospective re-view of almost 4000 patients undergoing TURP, Mebust et al [89] noted that haema-turia was an indication for surgery in 12% of patients. It is hypothesised that BPH,with its increased acinar and stromal cell proliferation, stimulates increased vascular-ity via angiogenesis. These new and prolific vessels may be easily disrupted leading
15

Chapter 9. Benign Prostate Disorders
to recurrent bleeding [91].This is supported by Foley et al [92] who found the mi-crovessel density to be higher in those patients with BPH having haematuria afterhistological studies. It is also hypothesised that 5-α reductase inhibitors may reduceangiogenesis and theoretically, reduce prostate bleeding. Thus finasteride, has beensuggested as an option in treating the problem of haematuria[93-95].
Detrusor (Bladder) InstabilityThe definition of detrusor instability is the development of a detrusor contractionwhich exceeds 15cm H
2O at a bladder volume of less than 300ml [96]. Detrusor
instability is not a specific term related to BPH, but implies LUTS secondary to adetrusor problem. These symptoms are normally storage related and consist of ur-gency, frequency, urge incontinence and nocturia. In BPH, the normal dynamics ofthe bladder are altered due to detrusor muscle stretching as a result of retention ofurine and contraction against an obstructed outlet. Although not completely under-stood, some of the detrusor instability may be related to changes at the adrenoceptorslevel, rather than just from obstruction and its consequences alone. In normal blad-der physiology, β-adrenoceptors are believed to be involved in the relaxation of thebladder during storage of urine [80]. In some patients, however, the administration ofnoradrenaline leads to contraction of the detrusor muscle which may be blocked byα-1 adrenoceptor antagonist [97]. This implies the presence of α-adrenoceptors in thedetrusor muscle in at least some patients. Furthermore, α-adrenoceptor antagonistshave been shown to relieve storage and voiding symptoms in men without obstruc-tion and storage symptoms in women[80, 98-101]. α adrenoceptor subtypes in thehuman bladder are predominantly of the α
1Dand α
1Atype. In animal models, the α
1Dreceptors become more abundant with obstruction[102], and it may be speculated
that this is the case in humans and that these receptors, once up-regulated, play a rolein storage symptoms [80].
Renal insufficiencyRenal insufficiency results from obstructive uropathy secondary to the bladder out-let obstruction of BPH. In an analysis of patients receiving treatment for BPH, 13.6%(range 0.3-30%) had renal insufficiency [87]. Certainly, an abnormal creatinine is anindication to further investigate the upper urinary tract with imaging. Obviously,other concurrent causes of renal insufficiency need to be excluded. Those patientswith renal insufficiency undergoing surgery are at increased risk (25%) of postoper-ative complications such as acute renal failure and urosepsis compared to patientswithout (17%) insufficiency [89].
Elevated Prostate Specific Antigen (PSA)As BPH is a true hyperplasia, more cells produce a greater amount of PSA[103]. It hasbeen suggested that many PSA elevations detected and investigated in clinical prac-tice may in fact be due to BPH leading Stamey to controversially argue that PSA is abetter marker of BPH than of prostate cancer[103, 104]. One approach to distinguishthe two conditions when PSA is elevated is to perform a free-to-total PSA ratio: morefree PSA than complexed PSA suggests BPH rather than prostate cancer. A ratio ofaround 20% or greater for free PSA is considered more likely to represent BPH thancancer[105]. PSA is discussed further in the investigations section below.
Quality of LifeIn terms of complications of BPH, quality of life (QOL) issues have gained more at-tention since the landmark paper of Girman et al over a decade ago[106]. They high-
16

Chapter 9. Benign Prostate Disorders
lighted in their study of several thousand men that moderate to severe urinary symp-toms have a significant impact on men’s lives in terms of degree of bother, worry,interference with daily living, and psychological well-being. The impact of BPH onQOL has been highlighted in many recent studies[107, 108] and such studies con-tinue to be important in raising awareness of BPH in the community and the abilityof men to seek treatment for BPH. Comprehensive surveys of men, such as the Menin Australia Telephone Survey (MATeS), provide contemporaneous data that men areinterested in their health and the QOL impact of problems such as LUTS secondaryto BPH[109, 110].
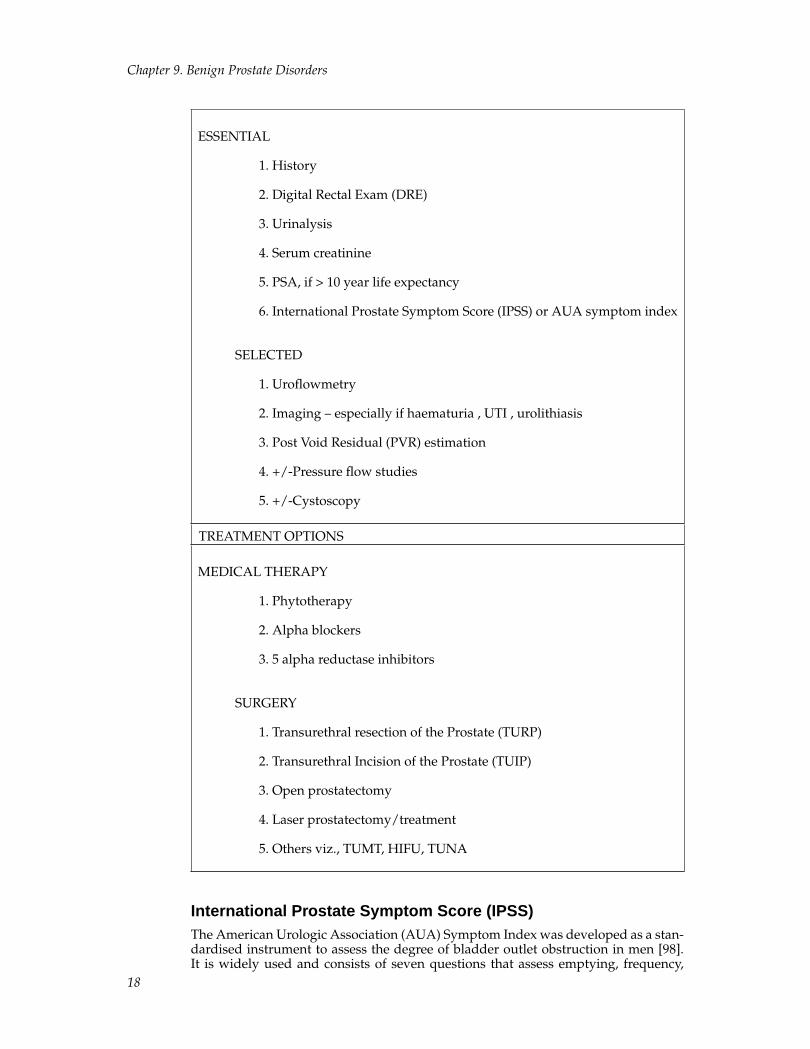
HISTORYA comprehensive medical history must be evaluated and should include the use ofa voiding diary, the International Prostate Symptom Score and a discussion of therole of prostate specific antigen (PSA) testing[111]. An outline of the evaluation andtreatment options for LUTS is shown in Table 4 and is discussed in greater depthbelow[112, 113]. Previous urological disease should be documented including previ-ous urological surgery, UTI, bladder or renal calculi, renal disease and penoscrotalpathology. Any risk factors for surgery such as diabetes mellitus, immunosuppres-sion, ischaemic heart disease, respiratory problems, smoking as well as a comprehen-sive list of medications should be noted. In particular, the use of antihypertensivesmust be noted as any α-blocker treatment initiated could potentially cause severehypotension.
As discussed in the section on differential diagnosis, consideration needs to be givento neurologic causes of voiding dysfunction such as stroke or Parkinson’s disease.
Table 4. A Summary of Diagnosis and Treatment Options in BPH
EVALUATION of LUTS
17
Chapter 9. Benign Prostate Disorders
ESSENTIAL
1. History
2. Digital Rectal Exam (DRE)
3. Urinalysis
4. Serum creatinine
5. PSA, if > 10 year life expectancy
6. International Prostate Symptom Score (IPSS) or AUA symptom index
SELECTED
1. Uroflowmetry
2. Imaging – especially if haematuria , UTI , urolithiasis
3. Post Void Residual (PVR) estimation
4. +/-Pressure flow studies
5. +/-Cystoscopy
TREATMENT OPTIONS
MEDICAL THERAPY
1. Phytotherapy
2. Alpha blockers
3. 5 alpha reductase inhibitors
SURGERY
1. Transurethral resection of the Prostate (TURP)
2. Transurethral Incision of the Prostate (TUIP)
3. Open prostatectomy
4. Laser prostatectomy/treatment
5. Others viz., TUMT, HIFU, TUNA
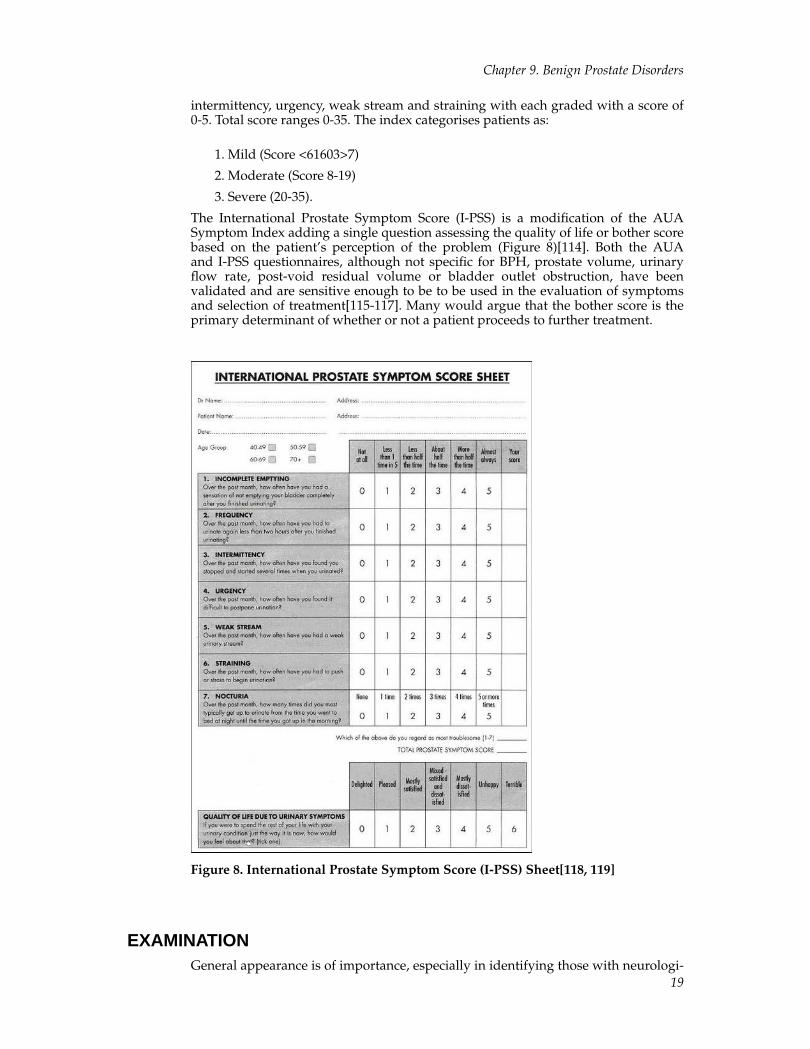
International Prostate Symptom Score (IPSS)The American Urologic Association (AUA) Symptom Index was developed as a stan-dardised instrument to assess the degree of bladder outlet obstruction in men [98].It is widely used and consists of seven questions that assess emptying, frequency,
18
Chapter 9. Benign Prostate Disorders
intermittency, urgency, weak stream and straining with each graded with a score of0-5. Total score ranges 0-35. The index categorises patients as:
1. Mild (Score <61603>7)
2. Moderate (Score 8-19)
3. Severe (20-35).
The International Prostate Symptom Score (I-PSS) is a modification of the AUASymptom Index adding a single question assessing the quality of life or bother scorebased on the patient’s perception of the problem (Figure 8)[114]. Both the AUAand I-PSS questionnaires, although not specific for BPH, prostate volume, urinaryflow rate, post-void residual volume or bladder outlet obstruction, have beenvalidated and are sensitive enough to be to be used in the evaluation of symptomsand selection of treatment[115-117]. Many would argue that the bother score is theprimary determinant of whether or not a patient proceeds to further treatment.
Figure 8. International Prostate Symptom Score (I-PSS) Sheet[118, 119]
EXAMINATIONGeneral appearance is of importance, especially in identifying those with neurologi-
19

Chapter 9. Benign Prostate Disorders
cal disease (eg. past stroke, Parkinson’s disease) or other major co-morbidities (obe-sity, severe osteoarthritis, diabetes) that may impact on treatment or further inves-tigation. An abdominal examination should identify those in marked urinary reten-tion, any abnormal masses and previous surgical scars. A careful assessment of thescrotum and its contents as well as the penis is also warranted to exclude any otherpathology. The digital rectal examination (DRE) is important in identifying prostaticabnormalities, including clinically apparent prostate carcinoma[120]. Prostate size,texture and tenderness should all be assessed, as should anal tone. Any nodulesshould be carefully noted. Constipation may also be a contributing factor to urinaryretention and anal tone should also be recorded.
DIFFERENTIAL DIAGNOSIS OF BPHIt is important to acknowledge that the diagnosis of BPH often relies on surrogatemeasures until a histological diagnosis is confirmed. These range from clinical (symp-tom scores), physiological (uroflowmetry), anatomical (prostatic volume on DRE orTRUS) and biochemical (PSA values) measurement. Although all of these measure-ments capture some component of BPH, none of them is specific for BPH[121] whichis itself a histological diagnosis. Surrogate measures are likely to represent a con-tinuum of disease severity without the existence of a threshold. Thus, differentialdiagnoses need to always be considered and where appropriate, excluded. In table5 below, some of the more obvious differential diagnoses are listed, but will not beexamined in detail.
Table 5. Differential diagnoses for LUTS
Inflammatory Conditions
1. Urinary Tract Infection
2. Prostatitis
3. Bladder Calculi
4. Interstitial Cystitis
5. Tuberculous Cystitis
Neoplastic Conditions
1. Prostate cancer
2. Bladder transitional cell carcinoma (usually CIS)
3. Urethral cancer
20

Chapter 9. Benign Prostate Disorders
Neurological Conditions
1. Parkinson’s disease
2. Stroke
3. Multiple Sclerosis
4. Cerebral Atrophy
5. Shy-Drager Syndrome
Other Causes of Urinary Obstruction
1. Urethral stricture
2. Severe phimosis
3. Bladder neck dyssynergia
4. External sphincter dyssynergia
PROSTATITISProstatitis is a common condition that must be excluded from other causes of LUTSand is a common cause of visits to primary care physicians and urologists. It maypresent as an acute bacterial infection or may be chronic, occasionally progressingto a debilitating illness. In practice, the clinical diagnosis of prostatitis depends onthe history and physical examination, but there is no characteristic physical findingor diagnostic laboratory test. Patients with prostatitis experience considerable mor-bidity and may remain symptomatic for many years. Unfortunately, there is limitedunderstanding of the pathophysiology and optimal treatment for most patients.
Prostatitis has been sub-classified and an abbreviated version is in table 6.
Table 6. The National Institute of Health (USA) Consensus Classification of Pro-statitis Syndromes
1. Acute bacterial prostatitis2. Chronic bacterial prostatitis
3. Chronic prostatitis/chronic pelvic pain syndrome
a. Inflammatory
b. Non-inflammatory
4. Asymptomatic inflammatory prostatitis
21

Chapter 9. Benign Prostate Disorders
Acute Prostatitis.Clinical features suggestive of acute prostatitis (Type 1, in Table 6 above) include dy-suria and urinary frequency as well as perineal pain (Table 7). Systemic symptomssuch as fever, rigors, myalgia and sweats are often a feature. On examination, the pa-tient is normally febrile, and may be overtly septic depending on the infection sever-ity. A digital rectal exam finds an extremely tender prostate which is often intolerableto the patient. An abscess is occasionally palpated.
Table 7. Clinical symptoms in prostatitis (adapted from Lobel94)
Genital symptoms
1. Dribbling
2. Inguinal pain
3. Testicular pain
4. Retropubic pain
5. Perineal pain
6. Urethral Burning
General Symptoms
1. Backache
2. Sweating
3. Tiredness
4. Cold feet
Investigations should include a mid-stream urine sample for microscopy, culturefor bacteria, and antibiotic sensitivity. The most common organisms are typicaluropathogenic bacteria such as Escherichia coli. Blood cultures for bacteria andantibiotic sensitivity should also be considered. Prostatic massage is usuallycontraindicated in patients with acute prostatitis due to pain and the risk ofprecipitating sepsis. A treatment regime is highlighted in Table 8. If there is failure torespond to therapy, evaluation for a prostatic abscess using a tran-srectal ultrasoundscan or computed tomography scan may be required. If necessary, perineal ortransurethral drainage of an abscess may be undertaken. At least 4 weeks ofantibiotic therapy is recommended in all patients to try to prevent chronic bacterialprostatitis. Following resolution of acute prostatitis, the urinary tract should beinvestigated for any structural problems[123, 124].
Table 8. Treatment of Acute Prostatitis
22

Chapter 9. Benign Prostate Disorders
1. Hydration
2. Rest and hospitalisation if severe
3. Empirical therapy with antibiotic until urine culture and sensitivitiesavailable
4. For patients requiring parenteral therapy antibiotics covering thelikely organisms: broad spectrum cephalosporins, for example, cefuroxime,cefotaxime, or ceftriaxone plus gentamicin
5. Oral treatment according to sensitivitiesQuinolones, such asciprofloxacin or norfloxacin For patients intolerant of, or allergic to,quinolones: trimethoprim or co-trimoxazole;
6. Analgesics, such as non-steroidal anti-inflammatory drugsSuprapubic catheterisation if catheterisation needed – per urethral cathetersmay precipitate abscess formation
Chronic ProstatitisAs the presentation may be localised to the genital region or non-specific (see Table 7)a careful history and examination along with specialised diagnostic tests are neededto identify this condition. Investigations may involve prostatic massage to express or-ganisms and/or white blood cells for analysis. Urine sample collection is often donein phases to aid in the localisation process: first void urethral urine; mid-stream blad-der urine; post-prostatic massage sample. Urine microscopy and quantitative cultureis then undertaken. Semen analysis for excessive white blood cell numbers may alsobe indicative of chronic prostatitis. A serum prostate specific antigen measurementmay be undertaken and is often raised, especially in acute prostatitis or in an ac-tive phase of chronic prostatitis. Trans-rectal ultrasound is considered but not rec-ommended to differentiate the different forms of chronic prostatitis. Urinary tract lo-calisation procedures (culture of first void urethral urine; mid-stream bladder urine;post-prostatic massage samples of urine correlating to urethra, bladder and prostate)although theoretically correct, are often not used in clinical practice[123, 124].
The various classifications of chronic prostatitis are listed in Table 6. Patients withchronic bacterial prostatitis (type II prostatitis) experience recurrent episodes of bac-terial urinary tract infection caused by the same organism, usually E. coli, anotherGram-negative organism, or enterococcus. Between symptomatic episodes of bac-teriuria, lower urinary tract cultures can be used to document an infected prostategland as the focus of these recurrent infections. Acute and chronic bacterial prostati-tis represent the best understood, but least common, prostatitis syndromes[123, 124].
Unfortunately, more than 90% of symptomatic patients have chronicprostatitis/chronic pelvic pain syndrome (type III). This term recognizes thelimited understanding of the causes of this syndrome for most patients andthe possibility that organs other than the prostate gland may contribute to thissyndrome. Urological pain (normally in the perineum or associated with voiding orintercourse) is now recognised as a primary component of this syndrome. Activeurethritis, urogenital cancer, urinary tract disease, functionally significant urethralstricture, or neurological disease affecting the bladder must be excluded. Patientswith the inflammatory subtype (type IIIA) of chronic prostatitis/chronic pelvic painsyndrome have leukocytes in their expressed prostatic secretions post prostatemassage urine or in semen.
23

Chapter 9. Benign Prostate Disorders
In contrast, patients with the non-inflammatory subtype of chronic prostatitis (typeIII B) have no evidence of inflammation. In essence, they have no evidence of activeinfection nor of inflammation on available investigative techniques taken at a par-ticular point in time. Repeat investigations are therefore done to be sure adequatesampling has been undertaken. This condition may be difficult to treat and requiresintensive counselling, information and reassurance to the patient to be successfullymanaged[124].
Finally, asymptomatic inflammatory prostatitis (type IV) is diagnosed in patientswho have no history of genitourinary tract pain complaints. It is often an inciden-tal finding on prostatic biopsy done for other reasons (eg a raised PSA). Treatment isusually not required.
Treatment of chronic prostatitisAll patients should have investigations as outlined above. A summary of treatmentoptions is included (Table 9).Those patients with chronic prostatitis secondary tobacterial infection (type II) require a prolonged course of antibiotics (often up to 3months) and should then be re-cultured to ensure eradication of the organism. Someurologists argue that these patients should also have investigation of their urinarytract by way of cystoscopy and at minimum, an ultrasound to ensure no anatomicalabnormality that may be responsible.
Patients with asymptomatic prostatitis (IV) require no treatment but those with theinflammatory (IIIA) and non-inflammatory (IIIB) are more difficult.
Patients with type IIIA disease have excessive leucocytosis in their specimens but nobacteria. However, because their symptoms may be due to a pathogen that is difficultto isolate, a further course of antibiotics (6-12 weeks) with coverage of chlamydiaand ureaplasma[122] is indicated. If this antibiotic course is not therapeutic, thenconcentration should be focus on anti-inflammatory medications (which may be usedin conjunction with the course of antibiotics). If anti-inflammatory treatment fails,then patients should be treated as below, for type IIB.
Current treatment for Type IIIB patients requires multiple therapies. Triple therapywith high dose α-blocker (3 month minimum), analgesia and muscle relaxant (benzo-diazepines).Initially, a narcotic analgesic should be changed to a non-steroidal anti-inflammatory (NSAID) if a response occurs after 2 weeks. The NSAID should becontinued for at least 6 weeks, but stopped if there is no response at 2 weeks. If thetriple treatment fails, other avenues must be explored, including biofeedback, relax-ation exercises psychotherapy and lifestyle changes (soft cushions, cease bike-riding).The focus is on improving quality of life and minimising symptoms, not curing thedisease[122].
Table 9. Management and Treatment of Chronic Prostatitis
24
Chapter 9. Benign Prostate Disorders
1. Oral and written patient education2. Pharmacological treatment for chronic bacterial prostatitis chosen
according to antimicrobial sensitivities Quinolones, such as: ciprofloxacin;ofloxacin; norfloxacin For those allergic to quinolones: minocycline;doxycycline; trimethoprim; co-trimoxazole
3. Other treatments for chronic bacterial prostatitis: radicaltransurethral prostatectomy or total prostatectomy in carefully selectedpatients.
4. Empirical Treatments for chronic abacterial prostatitis
5. Treat as for chronic bacterial prostatitis with a quinolone ortetracycline
6. Alpha Blockers: terazosin, alfuzosin
7. Non-steroidal anti-inflammatory drugs
8. Stress management. Referral for psychological assessment asappropriate; diazepam. Note: benzodiazepines are considered but notrecommended in clinical practice because of dependency
9. Adequate follow-up and counselling, often with professional support
10. Cernilton (pollen extract)
11. Bioflavonoid quercetin
12. Transurethral microwave thermotherapy
Note: allopurinol (chronic abacterial prostatitis) is considered but furtherstudies are needed before recommending it.
INVESTIGATIONS of LUTSAs outlined by Tubarro et al[111], the aim of investigations for LUTS should be three-fold: (1) to evaluate the possible relationship between prostatic enlargement, lowerurinary tract symptoms and signs of bladder outlet obstruction; (2) to quantify theseverity of benign prostatic enlargement-related symptoms and signs and (3) to ruleout the presence of a prostate cancer.
UrinalysisUrinalysis is used to screen for urinary tract infection as a cause of LUTS in order toidentify those with microscopic or macroscopic haematuria. A formal urine culturemay be undertaken if the analysis was suspicious for infection.
Post-void residual urine volume (PVRU)Although there is a high degree of intra-individual variation in the PVRU it maystill provide valuable information with regard to bladder emptying. It may not dis-tinguish adequately between bladder outlet obstruction or poor detrusor function
25
Chapter 9. Benign Prostate Disorders
and the United States guidelines on BPH suggest it is an optional investigation be-cause of this variability [87] . Greater than 300ml is considered a potential risk factorfor upper urinary tract dilatation and renal impairment[125]. The PVRU does havethe advantage of being used as a monitoring investigation in those opting for non-surgical therapy for BPH. It is readily and quickly performed in the office or hospitalsetting using portable ultrasound equipment.
Serum CreatinineMost guidelines on investigation of BPH recommend this investigation and anelevated serum creatinine would be an indication to evaluate the upper urinarytract[113].
Upper Urinary Tract ImagingUrinary tract ultrasound or computerised tomography are appropriate modalities.Most would consider upper tract imaging as mandatory if haematuria was presentand recommend it if there was a history of urolithiasis, urinary tract infection or renalinsufficiency. Intravenous pyelography still has a role in certain cases, as other modal-ities do not outline the anatomy of the collecting system with such definition[111].
UrodynamicsUrodymanics is a general term for a collection of investigations useful in quantifyingthe activity of the lower urinary tract during micturition[126]. Complete pressure-flow urodynamics are complex and usually involves fluoroscopy, video recording,bladder and rectal pressure measurement, as well as an assessment of urine flow.The simplest urodymamics are pressure-flow studies, requiring only voiding into ameasuring device to obtain flow rates, and may easily be done in the office setting.
With regard to the investigation and diagnosis of conditions underlying LUTS, whenconsidering inexpensive, safe and completely reversible treatments, one may opt toavoid urodynamics studies initially. However, when considering irreversible, expen-sive or potentially morbid therapy, such studies are considered mandatory. Manypatients will not have urodynamics studies based on the first premise above[126].However, in reality, many surgeons and physicians will have simple pressure-flowstudies easily available and will perform these as part of an initial consultation. Morecomplex studies require time and are costly, and so should be reserved for particularsituations as discussed below.
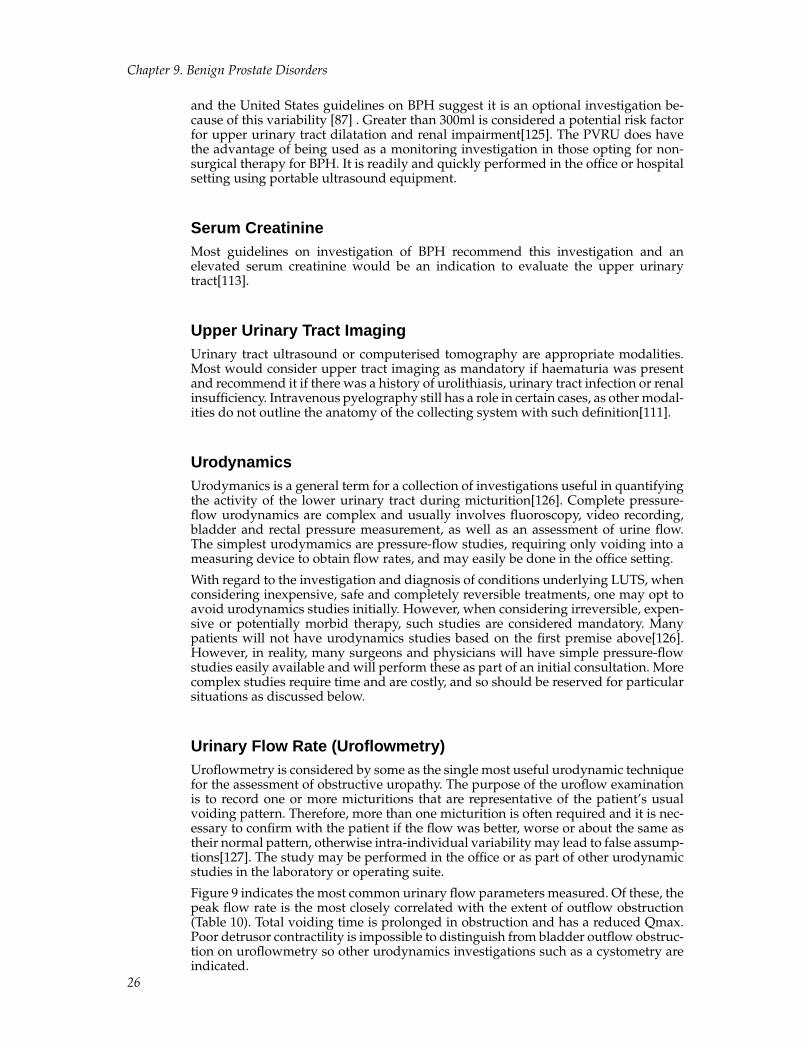
Urinary Flow Rate (Uroflowmetry)Uroflowmetry is considered by some as the single most useful urodynamic techniquefor the assessment of obstructive uropathy. The purpose of the uroflow examinationis to record one or more micturitions that are representative of the patient’s usualvoiding pattern. Therefore, more than one micturition is often required and it is nec-essary to confirm with the patient if the flow was better, worse or about the same astheir normal pattern, otherwise intra-individual variability may lead to false assump-tions[127]. The study may be performed in the office or as part of other urodynamicstudies in the laboratory or operating suite.
Figure 9 indicates the most common urinary flow parameters measured. Of these, thepeak flow rate is the most closely correlated with the extent of outflow obstruction(Table 10). Total voiding time is prolonged in obstruction and has a reduced Qmax.Poor detrusor contractility is impossible to distinguish from bladder outflow obstruc-tion on uroflowmetry so other urodynamics investigations such as a cystometry areindicated.
26
Chapter 9. Benign Prostate Disorders
Figure 9. Uroflowmetry in a normal individual- diagram above and actual readingbelow.
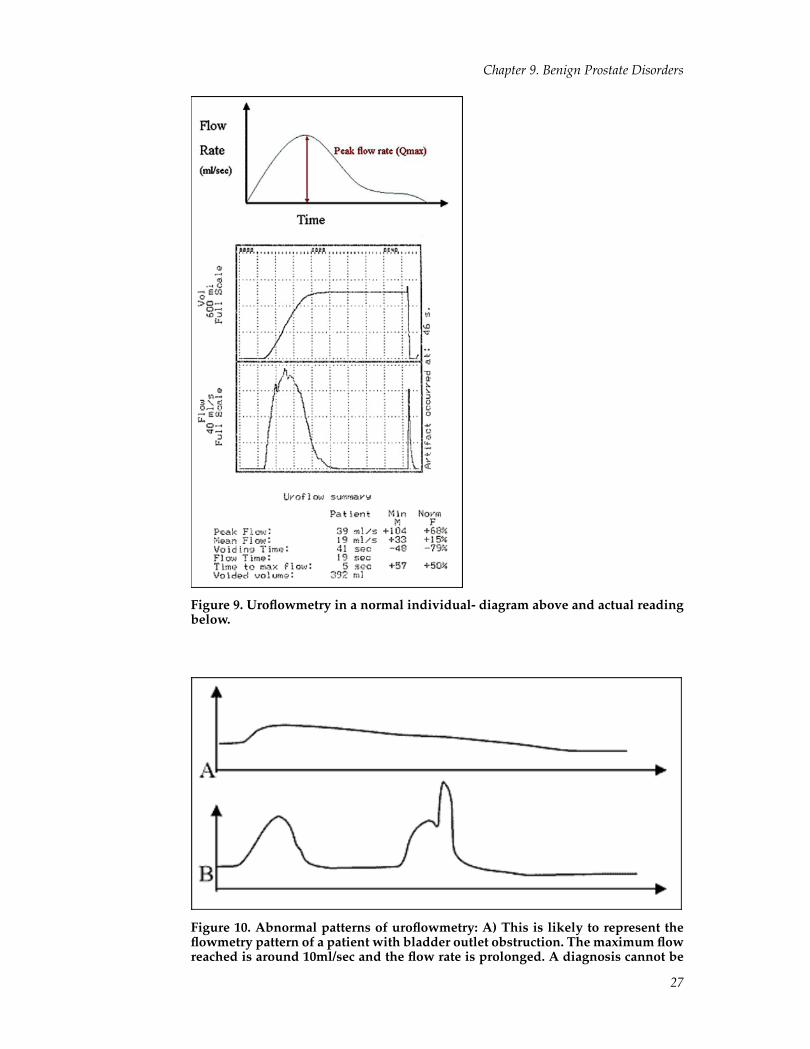
Figure 10. Abnormal patterns of uroflowmetry: A) This is likely to represent theflowmetry pattern of a patient with bladder outlet obstruction. The maximum flowreached is around 10ml/sec and the flow rate is prolonged. A diagnosis cannot be
27
Chapter 9. Benign Prostate Disorders
made from this reading alone but is certainly characteristic of someone with ob-structed voiding and having normal detrusor muscle function. B) This pattern ofintermittent flow usually represents abdominal straining in an attempt to over-come outflow obstruction. The peak flow rate may be normal or high, especially ifoutlet resistance is reduced.
Table 10. Interpretation of Uroflowmetry Results
Flow rate- Qmax Interpretation
>15ml/sec Unlikely to be significant obstruction
<10ml/sec Likely to be significant obstruction orweak detrusor activity
10-15ml/sec Equivocal
Urodynamics- presssure-flow studiesVarious measurements may be used to define detrusor pressures (e.g.Abram-Griffiths nomogram) and urethral sphincter pressures as an aid to diagnosisin specific circumstances. This is relevant in patients with LUTS who have hada stroke (or other neurologic disease) where bladder function may have sensorydeficits or unstable detrusor contractions, that may need alternate management.Nevertheless, detrusor instability is not considered a negative factor with respect tothe outcome of BPH surgery[111], provided it is adequately managed. Some haveeven suggested that the detection of detrusor instability in patients with LUTS isonly of minor diagnostic importance[128].
There is no evidence that pressure-flow studies should be mandatory prior to surgical(or medical) intervention. However, prior to transurethral resection of the prostate(TURP) it has been recommended that the following patients undergo pressure-flowstudies:
1. Previous unsuccessful invasive treatment of LUTS
2. Elderly men (>80 years old), because of the risk of alternate pathology otherthan bladder outlet obstruction and operative morbidity
3. Younger men (less than 50 years old) because of the risk of retrograde ejacula-tion and alternate diagnosis
4. Neurogenic bladder suspected
5. Previous radical pelvic surgery
6. Post void residual of greater than 300ml (not on one reading)[129]
UrethrocystoscopyThe performance of this investigation depends on patient history and proposed sur-gical intervention. It is necessary where there is a history of microscopic or macro-scopic haematuria to exclude bladder tumours or stones. A history of urethral stric-tures, bladder tumours or prior lower urinary tract surgery should also prompt thisinvestigation. Surgeons may also use urethroscystoscopy when planning differentsurgical treatments or invasive therapies.
28
Chapter 9. Benign Prostate Disorders
Transrectal ultrasound scanning (TRUS)Compared to TRUS, methods of determining prostate size such as DRE, urethrocys-toscopy and retrograde urethrography are poor[130]. It is often conducted in unisonwith biopsies of the prostate for suspected carcinoma, but is also a useful tool forassessing the size of an enlarged prostate so that the best mode of management maybe undertaken, such as open versus endoscopic surgery. Two planes of measurementare needed to mainatain accuracy and reproducibility with a common formula usedbeing: W x W x H x pi/6.[131]
The amount of prostate actually protruding into the bladder (i.e median lobe) onultrasound may also be important in predicting response to medical treatment afteran episode of retention (more protrusion, increased risk of failing trial of void).[132]
Serum Prostate Specific Antigen (PSA)Currently PSA is not recommended as part of the diagnostic workup for BPH andit is currently used in the context of case finding, staging, treatment response andmonitoring of prostate cancer in patients.[133-135] It may have a role in populationbased-screening for prostate cancer in the future once larger studies mature.[135] Aninteresting observation by Stamey and colleagues from 1317 consecutive men under-going radical prostatectomy at Stanford University during the past 20 years has beenthe reduction in size of prostate cancers identified by PSA testing 1983. Thus, withdownward stage migration, a PSA taken in today’s environment now likely repre-sents benign prostate enlargement rather than prostate.[104]
Following on from this, recommendations have been made concerning the role ofPSA in the patient with BPH [136]. This statement acknowledged that PSA levelsare used as part of the decision-making process in men presenting with LUTS inthe context of excluding prostate cancer and thus testing for it would be part of anyconsultation in any case. As outlined previously, distinguishing the two conditionswhen PSA is elevated may be aided by a free-to-total PSA ratio. A ratio of around 20%or greater for free PSA is considered more likely to represent BPH than cancer[105].
Furthermore, the consensus panel contended that PSA may be used as a surrogate forprostate volume and potentially a biomarker for disease progression (as it increasesalong with patient symptoms and deciding who may benefit from medical treatment.For example, it was emphasised that men with a PSA of ≥1.5ng/ml should be con-sidered to be at increased risk of BPH progression. To support such assumptions in apractical sense in men with BPH, those with a higher PSA have been found to benefitgreatest from 5 α-reductase treatment (along with those men having larger prostates)[137]. More data on such uses of PSA in men with BPH is likely to emerge in thefuture.
TREATMENT OF BPH- OVERVIEWThe primary aim of any treatment for BPH in the vast majority of men is to relievebothersome obstructive and irritative symptoms[138] (Table 2). Treatment is oftenundertaken on an elective basis for such patients. Those in whom complications ofBPH occur have treatment done urgently as a matter of course. A range of treatmentoptions are available and may be tailored to the needs of every individual, takinginto account their disease manifestations, success rates of treatment, possible compli-cations and patient preference.
There is persistent deterioration in BPH symptom severity and an increase in prostatevolume, risk of acute urinary retention and need for prostatic surgery overall in un-treated patients with BPH over time.[139] Much of the evidence for such progressionin BPH has arisen from large community studies such as those discussed below (Sec-tion 9.20). In addition, such studies have demonstrated a cumulative incidence in
29
Chapter 9. Benign Prostate Disorders
severity of symptoms (LUTS) and a decrease in urinary flow rate (Qmax) in mennot treated for BPH. Some groups of men who are more likely to experience diseaseprogression have risk factors such as:
1. Prostate volume- large baseline volume
2. Age- older at higher risk
3. Qmax- poor maximum urinary flow rate
4. PSA- higher levels increasing risk
5. Increased symptom severity [136, 139, 140]
In summary the physician can predict the risk of progression from the patient’s clin-ical profile based on the parameters immediately above. After predicting risk, themost appropriate treatment should be established by balancing the benefits of treat-ment against the possible risks and bother resulting from adverse events[140].
Such assumptions on parameters for BPH progression have recently been challengedin reviewing the large community Olmstead County study data , but further analysisfrom large cohorts would be needed to refute their value.[141]
For a sixty year old man, over a lifetime, there is approximately a one in four risk ofdeveloping acute urinary retention [142] and almost a third will require BPH-relatedsurgery[143]. However, BPH is a slowly progressing condition with the average de-cline in peak urine flow rate of 0.2ml/sec/year and an average increase in prostatevolume of 1-2cc per year. Larger prostates tend to suffer faster growth rates.[144].Hence the primary aim of any treatment for BPH in the vast majority of men is torelieve bothersome obstructive and irritative symptoms that developps slowly overtime [138] (table 3). Treatment is often undertaken on an elective basis for such pa-tients. Conversely, those in whom complications of BPH occur have treatment doneurgently as a matter of course. A range of treatment options are available and maybe tailored to the needs of every individual, taking into account their disease mani-festations, success rates of treatment, possible complications and patient preference.
WATCH AND WAIT/LIFESTYLE CHANGEMany men who presenting with LUTS are often seeking a full assessment of theirprostatic health rather than immediate treatment of symptoms that may not be ex-ceptionally bothersome. People with mild symptoms may wish to pursue lifestylechanges as a way of improving their quality of life but with the option of review ifsuch measures fail or symptoms worsen. Furthermore, when an adequate history istaken, hidden agendas such as fear of prostate cancer may even be revealed and fearsallayed.
Often drinking habits may be responsible for symptoms such as nocturia, where con-siderable fluid volumes are consumed in the evening. Reducing fluid intake maydiminish nocturia and evening urgency. Furthermore, caffeine and alcohol acting asdiuretics, can further exacerbate LUTS. Simple shifts in daily fluid intake may fulfilpatient expectations and result in satisfactory outcomes. Voiding diaries are usefulfor making patients aware of drinking habits and may be the catalyst for initiatingand monitoring changes. Bladder retraining (by using timed voiding, strengtheningpelvic floor exercises and monitoring oral intake) is also an option in some individu-als, once a voiding diary has been examined.
Medications may also play a role with LUTS. Measures such as diuretic restriction inevenings often prevents nocturia and frequency, provided the diuretic can be takenearlier in the afternoon.
It is important to discuss options with the patient and that they are made aware thatthe possibility of damage to their upper urinary tract or to the detrusor muscle mayresult if their symptoms deteriorate and they do not seek medical attention.
30

Chapter 9. Benign Prostate Disorders
PHYTOTHERAPY FOR BPHPhytotherapy, or the use of plant extracts, is becoming widely used in the manage-ment of many medical conditions including BPH (Table 11)[145]. Often these agentsare promoted to aid “prostatic health” and a significant proportion of men try them.Factors also contributing to their widespread use include the perception that they aresupposedly ”natural” products; the presumption of their safety (although this is notadequately proven); their alleged potential to assist in avoiding surgery, and even theunproven claim that they may prevent prostate cancer. The widespread availabilityof these products (without prescription) in vitamin shops, supermarkets, pharmaciesand over the internet has contributed to their usage and reflects the demand for thesephytotherapeutic agents. The mechanisms of action are poorly understood but havebeen proposed to be (1) anti-inflammatory, (2) inhibitors of 5α-reductase, and morerecently (3) through alteration in growth factors[146].
Phytotherapy although promising, lacks long-term, good quality clinical data[147].Nevertheless, because there is a large placebo effect associated with treatment ofvoiding symptoms, the use of herbal products that have few or no side effects maybe a reasonable first-line approach for many patients[148]. However, patients shouldbe counselled that the efficacy, mechanisms of action and long term effects of theseagents are not known and they must be aware of the limitations before proceed-ing[149].
The most popular phytotherapeutic agents are extracted from the seeds, barks andfruits of plants. Products may contain extracts from one or more plants and differentextraction procedures are often used by manufacturers. Thus the composition andpurity of any one product may differ even if they both originated from the sameplant. Basic research on one product may not be easily transferred to another makingthe gathering of data and giving of advice difficult[150].
[Table 11, TBD]
Saw Palmetto Berry (Serenoa repens)Extracts from the berries of the American dwarf palm (saw palmetto) are the mostpopular and widely available plant extracts used to treat symptomatic BPHtoday[151, 152]. At least eight possible mechanisms of action for saw palmettohave been advocated including anti-androgenic properties, anti-inflammatoryproperties and the induction of apoptosis to name a few[150]. It is most commonlybelieved that saw palmetto works as a naturally occurring 5 α reductase inhibitor,blocking the conversion of testosterone to dihydrotestosterone (see below in medicaltherapies section), as demonstrated in several in vitro studies [148, 153-156].
Thus, saw palmetto may be expected to reduce prostate size. However, this is not thecase in several trials using saw palmetto in men with BPH[157, 158]. The only trial toshow in vivo effects of saw palmetto involved needle biopsies of the prostate gland,before and after treatment with saw palmetto or placebo. Although the mechanism isunclear, there was a significant increase in prostatic epithelial contraction in the sawpalmetto group[159].
In a meta-analysis of 18 randomised studies relating to saw palmettto extracts, almost3000 men with BPH were studied and the authors concluded that “the evidence sug-gests that saw palmetto improves urologic symptoms and flow rates but that furtherresearch is needing using standardised preparations to determine long term effec-tiveness”[145]. When analysing flow rate and symptom score alone from this meta-analysis, the effect of seronoarepens was to increase the flow rate by a further 2.28ml/sec (standard error SE 0.29) over placebo which gave an increase of 1.09 ml/sec(SE 0.45). Serenoarepens also reduced the IPSS by 4.7 (SE 0.41), which is comparableto that found with finasteride and tamsulosin[160]. Many studies are currently un-derway to try and further delineate the role of saw palmetto extracts. One such studyby Hruby et al. monitored progression rates in men with mild symptoms of blad-der outflow obstruction (IPSS<8) receiving serenoa repens and found that they were
31

Chapter 9. Benign Prostate Disorders
significantly reduced as compared to patients on watchful waiting and a matchedgroup of patients on placebo. One third of patients on watchful waiting and placeboprogressed over the study period suggesting that phytotherapy may be an option inpatients at risk for progression, defined as having a PSA > 1.5 ng/mL and an enlargedtransitional zone volume (>25ml) on TRUS[161].
In summary, saw palmetto studies have shown improved symptom scores comparedto placebo but generally no change in flow rates[162]. Overall there is a real paucityof well performed, adequately powered, and placebo controlled trials in the use ofphytotherapy in clinical BPH. It is generally well tolerated at a dose of 320 mg/day,but its efficacy has not been compared with α blockers regarding efficacy, and has notbeen shown to reduce complications of BPH with long term use. Finally the productquality and purity cannot always be assured.
A recent randomised controlled study by Bent et al has mounted a strong argumentagainst the use of saw palmetto extract for symptomatic BPH.[163] The trial com-pared 160mg of saw palmetto extract against placebo in 225 men with moderate tosevere LUTS. The follow-up period was 12 months with changes in symptom indexand flow rates as end points with saw palmetto being no better than placebo and infact flow rate deteriorated (0.42ml/min) and there was a negligible improvement insymptom index of 0.68 points in the saw palmetto group.
One particular extract of saw palmetto, (Permixon, Pierre Fabre Medicament, Castres,France), has had all of its clinical data assessed in a meta analysis[164].This includedall 14 randomized clinical trials and three open-label trials, involving 4280 patients.In the randomized controlled trials, the mean placebo effect on peak urinary flowrate was an increase of 1.20 mL/s. The estimated effect of saw palmetto was a furtherincrease of 1.02 mL/s (P = 0.042). Further, a mean reduction symptom score (IPSS)for saw palmetto was 4.78.
In summary, saw palmetto studies have shown modestly improved symptom scorescompared to placebo but generally no change in flow rates[162, 163]. Overall thereis a paucity of well performed adequately powered, placebo controlled trials in theuse of phytotherapy in LUTS/BPH. It is generally well tolerated at a dose of 320mg/day, but has not been compared with α blockers regarding efficacy, and has notbeen shown to reduce complications of BPH with long term use. The product qualityand purity of saw palmetto cannot always be assured. This is continually raised as anissue[165] along with the recommended dosage required, and such differences needto be resolved if comparisons across studies are ever to be made.
African plum tree (Pygeum africanum)Extracts come from the bark of the African plum tree. It is hypothesised, based on invitro observation, that it acts on the prostate through inhibition of fibroblast growthfactors, has anti-estrogenic effects and inhibits chemotactic leukotrienes. No strongclinical data exists of its efficacy although trials are in progress[146, 149].
Pumpkin Seed (Cucurbita pepo)Dried or fresh seeds have been taken to relieve symptoms. Phytosterols are thought tobe amongst the active compounds. Side effects have not been reported but evidenceis lacking with no current clinical trials[166].
Rye Pollen (Secale cereale)This is prepared from rye grass pollen extract. In a systematic review summarizingevidence from randomised and clinically controlled trials[138], rye pollen was foundto be well tolerated but only achieved modest improvement in symptom outcomes
32

Chapter 9. Benign Prostate Disorders
and did not significantly improve objective measures such as peak and mean uri-nary flow rates. Again, several mechanisms of action have been proposed includingan improvement in detrusor activity, a reduction in prostatic urethral resistance, in-hibition of 5 α-reductase activity and an influence on androgen metabolism in theprostate[167].
Other extractsSouth African Star Grass (Hypoxis rooperi), Opuntia (Cactus flower), stinging nettleand Pinus (Pine flower) have also been studied and used, however the data num-bers are small and the types of trials do not allow conclusions to be drawn at thisstage[146].
MEDICAL THERAPY FOR BPHIn 1986 Caine[168] proposed that infravesical obstruction in men with symptomaticBPH comprised both static and dynamic components. The static component of ob-struction is related primarily to the mechanical obstruction caused by the enlargingprostatic adenoma whereas the dynamic component is principally determined by thetone of the prostatic smooth muscle. Two avenues for pharmacotherapy have there-fore evolved, namely shrinking the prostate tissue or relaxing the smooth muscle ofthe prostate. Medical therapy is now first-line treatment for most men with symp-tomatic benign prostatic hyperplasia[169]. They are non-invasive, reversible, causeminimal side effects, and significantly improve symptoms [90, 170].
Prostatic smooth muscle tone is under the influence of the autonomic nervous sys-tem. Thus any pharmacologic agent that may interfere with the functioning of thissystem could alter resistance in smooth muscle tone.
There are 3 main components to clinically significant BPH: static, dynamic and de-trusor muscle components as outlined above. The dynamic component is associ-ated with an increase in smooth muscle tone of the prostate. These smooth mus-cle cells contract under the influence of noradrenergic sympathetic nerves, therebyconstricting the urethra[171].Prostatic tissue contains high levels of both α
1and α
2adrenoceptors – 98% of the α
1adrenoceptors are associated with stromal elements
of the prostate[172]. Thus α1-receptor blockers relax smooth muscle, resulting in re-
lief of bladder outlet obstruction that enhances urine flow [96]. Different subtypes ofα
1receptors have been identified with α
1Athe predominant. Two α
1A-adrenoceptors
generated by genetic polymorphism have been identified with different ethnic distri-butions but similar pharmacologic properties [46].
It was demonstrated in 1978 that phenoxybenzamine, a nonselective α1/α
2blocker,
was effective in relieving the symptoms of BPH[173]. Side effects were significant andincluded dizziness and palpitations. Many of the side effects of the α-blockers weremediated by α
2-receptors[174].Thus, α
1selective antagonists such as terazosin, dox-
azosin and prazosin and were developed that had fewer side effects than phenoxy-benzamine [76]. Doxazosin, alfuzosisn and terazosin have gained favour in clinicalpractice because they are longer acting than prazosin. Due to side effects, many α
1selective antagonists need to be titrated and are often started at the lowest dose and
built up over time to the maximal dose or a dose where clinical effects are satisfactory.
Prazosin (titrated up to 5mg day) has been shown to significantly increase flow ratesby 36-59% compared to placebo 6-28% but 17% of men discontinued the drug due toside effects such as dizziness (21%), headache (14%), syncope (3.4%) and retrogradeejaculation (13%).
Alfuzosin (5 mg bid or10 mg daily) has shown symptom score reduction of 31-65%(compared to placebo 18-39%) and flow rate increases of 22-54% (compared toplacebo 10-30%). Hence the results were similar to those of prazosin but with only
33
Chapter 9. Benign Prostate Disorders
3-7% discontinuations due to dizziness (3-7%), headache (1-6%) and syncope (<1%)[175, 176].
Terazosin (2-10mg) had a symptom score reduction of 40-70% (compared to placebo16-58%) and improved flow rates 19-40% (placebo 5-46%). Between 9-15 % of mendiscontinued the drug, related to dizziness (10-20%), headache (1-7%), asthenia (7-10%), syncope (0.5-1.0%) and postural hypotension (3-9%). Thus terazosin was effec-tive and superior to placebo in reducing symptoms and increasing the peak urinaryflow rate. The effect of terazosin on the peak urinary flow rate was apparent in stud-ies as soon as 8 weeks of therapy. Most importantly, the effect of terazosin on symp-toms and peak urinary flow rate was independent of the baseline prostate size for therange of prostate volumes reported[177].
Tamsulosin (0.4 mg once daily dose) is a selective α blocker for the α1A
subtype whichpredominates in the human prostate, 12 times greater affinity for the receptors in theprostate than in the aorta thereby reducing side effects mediated through blood ves-sels receptors such as in the aorta. Symptom score were reduced by 20-50% ( placebo18-30%), flow rates improved 20-45% ( placebo 5-15%) but only 3-7% of men discon-tinued drug because of dizziness (3-20%), headache (3-20%), syncope (0.3%) and ret-rograde ejaculation 5-10%. The rate of retrograde ejaculation was much higher thanalfuzosin but the blood pressure lowering side effects are less with tamsulosin[178].
Doxazosin (4-12mg/day) is a selective α1-adrenoceptor antagonist, and produced a
significant increase in maximum urinary flow rate (2.3 to 3.6 ml. per sec) at dosesof 4 mg, 8 mg and 12 mg, and in average flow rate compared with placebo. The in-crease in maximum flow rate was significantly greater than placebo within 1 weekof initiating therapy and the drug significantly decreased patient-assessed total, ob-structive and irritative BPH symptoms. Blood pressure was significantly lower withall doxazosin doses compared with placebo. Adverse events, primarily mild to mod-erate in severity, were reported in 48% of patients on doxazosin compared to 35% onplacebo, with only 11% discontinuing treatment (a similar number to placebo). Themain side effects were dizziness (15-24%), headache (12%) and hypotension (5-8%)and abnormal ejaculation (0.4%)[179, 180].
In a meta-analysis, all α1-adrenoceptor antagonists seem to have similar efficacy in
improving symptoms and flow rates[181]. The difference between α 1-adrenoceptorantagonists is related to their side effect profile. Overall, alfuzosin and tamsulosinappear to be better tolerated than doxazosin, terazosin and prazosin[182]. Comparedto finasteride (5 α-reductase inhibitor), the α-blockers have a more rapid onset ofaction, are effective independent of prostate size, and show greater improvements insymptom scores but similar improvements in flow rate improvements. It is importantto understand most studies show symptom score improvements of 2-3 points andflow rate improvements of 1-2 ml/sec.
Table 12. Commonly Used Alpha-Blockers
Nonselective alpha blockers• Phenoxybenzamine
• Nicergoline
• Thymoxamine
Selective alpha1 blockers• Prazosin
• Alfuzosin
34
Chapter 9. Benign Prostate Disorders
Super-selective alpha1 blockers• Tamsulosin
Long-acting alpha1 blockers• Terazosin
• Doxazosin
α reductase inhibitorsThe enzyme 5-α reductase is crucial in the pathway of testosterone action (figure5). In target cells for androgens, including those of the prostate, testosterone under-goes 5-α reduction by the enzyme 5-α reductase. Within the prostate, 90% of testos-terone is converted to dihydrotestosterone (DHT) [87, 183]. There are 2 isoforms ofthe enzyme 5 –α reductase which are encoded by separate genes[184]. Type 1 isoen-zyme is expressed highly in the skin, liver, hair follicles and sebaceous glands andprostate whereas type 2 is responsible for male virilisation of the male fetus. It re-sides in prostate, genital skin, facial and scalp follicles[185, 186].
DHT once created, enters the nuclei initiating transcription of messenger RNA(mRNA) which then synthesises proteins such as enzymes in the cytoplasm.Inhibitors of this enzyme potentially decrease serum and intra-prostaticdihydrotestosterone levels, thus reducing prostatic tissue growth.
Finasteride and DutasterideFinasteride was the first of these to be trialled in humans and was shown to decreaseDHT levels[187]. It acts on the type 2 isoenzyme of 5-α reductase and has been theonly available 5 α-reductase inhibitor. Dutasteride is also available and it blocks bothisoenzymes of 5 α-reductase[169, 188]. Dutasteride shows a 60-fold greater inhibitionof the type 1 isoenzyme compared with finasteride and is also active against the type2 isoform [34, 169]. Further studies are needed to gain a more clear understanding ofany clinically significant differences between dutasteride and finasteride[188]. Finas-teride reduces serum DHT levels by 65-70% and prostatic levels by 85-90%, althoughthe intraprostatic levels of testosterone are reciprocally elevated.
Because 5-α reductase inhibitors work by reducing prostatic tissue volume, baselineprostate size has a significant impact on the efficacy of 5-α reductase inhibitors, withlarger glands (>50cc) more likely to respond[189, 190]. After treatment for one year,there is a significant decrease (17-30%) in total gland size with the greatest size re-duction in the periurethral component of the prostate (with finasteride), which hasthe greatest impact on obstructive symptoms [87], [191, 192]. Both transition and pe-ripheral zone volumes are equally affected by dutasteride.[193] There is a 60-70%decrease in DHT concentration , 25% decrease in prostate volume , a 13-30% symp-tom score reduction vs placebo 4-20% , flow rate improvement of 7-20% vs placebo3-15%. Furthermore, there were more pronounced changes with larger prostates >40cc , decreased libido in 10% , ejaculatory dysfunction 7.7% and impotence (15.8%), they reduced risk of AUR (50%) and the need for surgery (30%).
There is some evidence that patients on finasteride experience fewer serious compli-cations associated with the progression of BPH compared with those prescribed anα blocker, such as acute urinary retention or undergoing BPH-related surgery, butmore prospective data is needed[194]. Adverse events associated with finasterideinclude decreased libido, ejaculation disorders and erectile dysfunction but over-all are uncommon, with approximately 4% of patients discontinuing treatment forsuch events[169, 195]. Finasteride has also developed a role in the treatment of BPH-
35
Chapter 9. Benign Prostate Disorders
related haematuria although its role in reduction of perioperative bleeding is not welldefined [93, 169].
Prostate Cancer Prevention Trial (PCPT)More recently, as part of the Prostate Cancer Prevention Trial (PCPT) involving over18,000 men, it was concluded that finasteride delays the appearance of prostate can-cer whilst reducing the risk of urinary problems. However, there was an increasedrisk of high grade prostate cancer (Gleason score 7 or greater) leading to the discon-tinuation of this study. Thus the benefits needs to be weighed against the sexual sideeffects and the potential increased risk of high-grade prostate carcinoma[196]. Fur-ther recent analysis of the PCPT has highlighted the finding that finasteride therapysignificantly reduced the risk of prostate cancer by 24.8% (p <0.001) compared withplacebo[197]. Authors have now stated that the initial finding of increased incidenceof high-grade cancer in the finasteride arm compared with placebo was controver-sial. They now contend that the increase in incidence of high-grade disease observedin finasteride-treated subjects is not a histopathologic effect. They argue that a num-ber of potential biases have been identified, including increased detection rate dueto prostate volume reduction and improved prostate-specific antigen specificity andsensitivity for detecting prostate cancer. Thus the new analysis has concluded thatthere was an improved detection of overall prostate cancer as well as high-gradeprostate cancer in men treated with finasteride, rather than an increase in risk com-pared with placebo. Further analyses of the data from the PCPT together with otherclinical findings strongly suggest that the increase in high-grade tumours in the fi-nasteride arm is an artefact.[197] The impact of this new analysis is yet to be realisedand may lead to finsateride becoming more favored in the treatment of BPH andpotentially to prevent prostate cancer.
Summary of medical treatmentThe first line of medical treatment is an α-blocker, as the majority of patients treatedhave a prostate volume of less than 40ml. In men with larger prostates (greater than40cc), finasteride alone or in combination with an α-blocker would be appropriate.Patients who are likely to respond to finasteride will do so at the same relative mag-nitude as an α-blocker, but it will take a longer period of time (months as opposedto weeks). This is likely to be a reduction in 20-30% symptoms and a 1-2ml per sec-ond increase in urinary flow[195]. Side-effect profiles of medical treatments are alsoimportant, as discussed above. For example, with regard to sexual function, tamsu-losin has an increased risk of retrograde ejaculation and finasteride increases sexualdysfunction [83]. These may be important factors in choosing therapies.
MAJOR STUDIES OF MEDICAL TREATMENT OF BPHThe medical treatment of clinical BPH has come under increasing scrutiny throughlarger trials. Such trials have been the impetus for the introduction of medical therapyinto clinical practice. Some of these larger trials have been selected and are discussedbelow.
VETERANS AFFAIRS STUDYIn the Veterans Affairs Cooperative Studies Benign Prostatic Hyperplasia StudyGroup [66], a total of 1,229 subjects with clinical BPH were randomized to 1 year ofplacebo, finasteride, terazosin or drug combination. The primary outcome measureswere the AUA symptom score and the peak urinary flow rate. The percentage ofsubjects who rated improvement as marked or moderate with placebo, finasteride,
36

Chapter 9. Benign Prostate Disorders
terazosin and combination was 39, 44, 61 and 65%, only the latter two were superiorto placebo.
There was no significant relationship between baseline prostate volume and treat-ment response to finasteride or with the other treatments (terazosin or combination).There was a significant but weak relationship between change in AUA symptomscore and peak flow rate in the finasteride and combination groups. The symptomresponses with terazosin were not related to peak flow rate or baseline prostate vol-ume. In men with clinical BPH finasteride and placebo are equally effective, whileterazosin and combination are significantly more effective. In men with clinical BPHand large prostates the advantage of finasteride over placebo in terms of symptomreduction, impact on bother due to symptoms and quality of life was small at best,while the advantage of terazosin (alone or in combination with finasteride) over fi-nasteride alone and placebo was highly significant. The authors concluded that α
1blockers, such as terazosin, should be first line medical treatment for BPH [66]. An-
other arm of this study observing surgical treatment versus watchful waiting is dis-cussed below.
PLESS STUDYThe Proscar Long-term Efficacy and Safety Study (PLESS) was a 4-year, randomized,double-blind, placebo-controlled trial assessing the efficacy and safety of finasteride5mg (Proscar<61668>) in 3040 men, aged 45 to 78 years, with symptomatic BPH, en-larged prostates on TRUS volume criteria, and no evidence of prostate cancer[67, 68].Finasteride use reduced the risk of developing acute urinary retention by 57% andthe need for BPH-related surgery by 55%[198] in comparison to placebo. A modifiedAUA symptom score was used (because trial was undertaken prior to formal AUAbeing developed) and showed a reduction in mean score of 3 for finasteride and 1.2for placebo, starting at a level of 15 for both groups [68]. Compared with placebo,men treated with finasteride experienced an increased incidence of new drug-relatedsexual adverse events (erectile dysfunction, decreased libido, ejaculation disorder)only during the first year of therapy with 4% of men discontinuing because of suchevents [67].
PREDICT TRIALThe Prospective European Doxazosin and Combination Therapy (PREDICT) Trialwas constructed to evaluate the efficacy and tolerability of the selective α
1-adrenergic
antagonist doxazosin and the 5α-reductase inhibitor finasteride, alone and in com-bination, for the symptomatic treatment of benign prostatic hyperplasia. It was aprospective, double-blind, placebo-controlled trial involving 1095 men aged 50 to 80years. The dose of finasteride was 5 mg/day. Doxazosin was initiated at 1 mg/day,and titrated up to a maximum of 8 mg/day over approximately 10 weeks accordingto the response of the maximal urinary flow rate (Qmax) and IPSS. An intent-to-treat analysis of 1007 men showed doxazosin and doxazosin plus finasteride com-bination therapy produced statistically significant improvements in total IPSS andQmax compared with placebo and finasteride alone. Finasteride alone was not sig-nificantly different statistically from placebo with respect to Qmax or total IPSS. Thetreatments were generally well tolerated. They concluded that doxazosin was effec-tive in improving urinary symptoms and urinary flow rate in men with benign pro-static hyperplasia, and was more effective than finasteride alone or placebo. The ad-dition of finasteride did not provide further benefit to that achieved with doxazosinalone[179].
OLMSTED COUNTY STUDY, USAThe Olmsted County study (Minnesota, USA) of urinary symptoms and health sta-
37

Chapter 9. Benign Prostate Disorders
tus among men during 10,000 person-years of followup [49]. In this study, whichfollowed for 12 years a randomly selected cohort of 2115 men aged 40-79 years, therewas an average increase in the IPSS of 0.18 points per year, ranging from 0.05 for menin their fifties to 0.44 for those in their seventies. There was also a decrease in peakflow rate of 2% per year and a median prostate growth of 1.9% per year. The cumula-tive incidence of AUR was low (2.7% over 4 years). This is an excellent longitudinalstudy but clearly one weakness was the repeat contact and availability of urologicalmeasurements during the study period that may have influenced treatment decisionsin the study cohort. Despite this the data demonstrated that treatment is commonin elderly men with nearly one in four receiving treatment in the eighth decade oflife. Furthermore, men with moderate to severe lower urinary tract symptoms, im-paired flow rates or enlarged prostates were more likely to undergo treatment, withincreases in risk of similar magnitude to those associated with adverse outcomes,such as acute urinary retention.
A recent analysis of the data has also demonstrated a relationship of BPH diagnosisand PSA testing. From 1987 to 1997, 2,330 cases of BPH were identified represent-ing an age adjusted, corrected incidence for BPH among male residents of OlmstedCounty of 854.7 per 100,000 men. While the incidence of BPH increased from 1987 to1992, coinciding with the introduction of serum prostate specific. It appears that theintroduction of serum PSA testing as a screening tool for prostate cancer along withthe advent of less invasive alternatives, including pharmacological therapy, have hada significant impact on the incidence of diagnosed BPH in the last decade.[199]
MTOPS STUDY AND PREDICTORS OF CLINICAL PROGRESSIONThe Medical Therapy of Prostatic Symptoms (MTOPS) study is a double-masked,placebo-controlled, multi-center, randomized clinical trial with 4 study arms 1)placebo; 2) doxazosin (4 to 8 mg); 3) finasteride (5 mg) and 4) combination of bothdoxazosin and finasteride. 3047 men were randomized equally to the 4 groups.Baseline parameters analyzed included age at randomization, transrectal ultrasound(TRUS) volume, AUA symptom score, Qmax, PVRU and PSA. Reduction in the riskof BPH progression was analyzed by one covariate at a time regression models ofabsolute risk of BPH progression versus baseline covariates. Groups comparedwere combination versus doxazosin, combination versus finasteride and finasterideversus doxazosin[200]. The full results are yet to be published.
A small part of the study focused on the routinely available measure of serum PSA,in an attempt to predict a patient’s future risk of BPH clinical progression, acute uri-nary retention and BPH-related invasive therapy, permitting an informed decisionconcerning the value of medical therapy over watchful waiting[201]. In MTOPS, 737patients were assigned to placebo and followed for an average of 4.5 years. Clini-cal progression of BPH was pre-defined as either a 4-point increase in AUA symp-tom score, acute urinary retention, incontinence, renal insufficiency or recurrent UTI.The need for BPH-related invasive therapy was a secondary outcome. These data aresummarised in Table 13, where those having a lower PSA, had a lower rise in symp-tom score, and a reduced risk of acute urinary retention or invasive treatment com-pared to those with a higher PSA. The sub-group with the highest baseline PSA wasalso likely to have larger prostate glands, making the findings intuitive. However,as with many such findings, translating an individual PSA to a population study isdifficult, as other factors will determine progression or regression of symptoms, notjust PSA.
In summary, only the treatment arms containing 5 α reductase inhibitor (finasteride)were associated with long term reductions in the risk of invasive therapy for BPH oracute urinary retention (Table 13). The reduction in risk of BPH progression was 67%with combination treatment and similar in the doxazosin (39%) or finasteride (34%)only arms. The risk reduction for acute urinary retetntion was 79% for combined ver-sus 31% for doxazosin and 67% for finasteride. A similar spread of reduction in needfor surgery was found being 69%, 8% and 64%. Doxazosin monotherapy was able
38
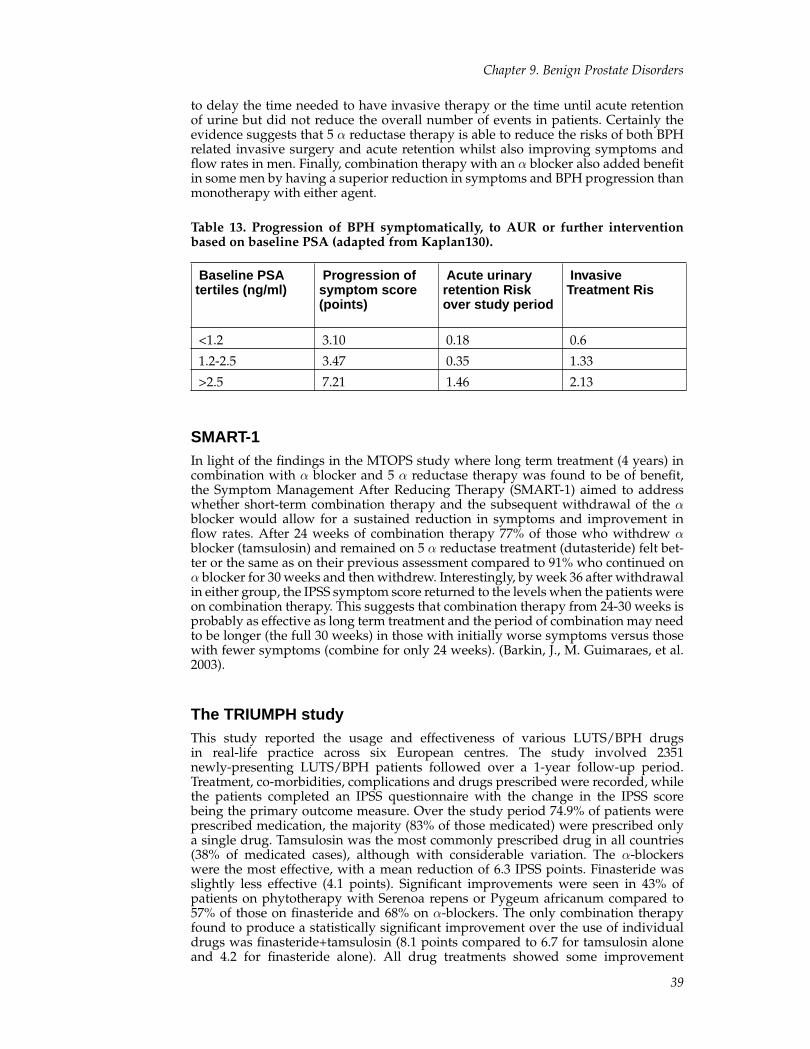
Chapter 9. Benign Prostate Disorders
to delay the time needed to have invasive therapy or the time until acute retentionof urine but did not reduce the overall number of events in patients. Certainly theevidence suggests that 5 α reductase therapy is able to reduce the risks of both BPHrelated invasive surgery and acute retention whilst also improving symptoms andflow rates in men. Finally, combination therapy with an α blocker also added benefitin some men by having a superior reduction in symptoms and BPH progression thanmonotherapy with either agent.
Table 13. Progression of BPH symptomatically, to AUR or further interventionbased on baseline PSA (adapted from Kaplan130).
Baseline PSAtertiles (ng/ml)
Progression ofsymptom score(points)
Acute urinaryretention Riskover study period
InvasiveTreatment Ris
<1.2 3.10 0.18 0.6
1.2-2.5 3.47 0.35 1.33
>2.5 7.21 1.46 2.13
SMART-1In light of the findings in the MTOPS study where long term treatment (4 years) incombination with α blocker and 5 α reductase therapy was found to be of benefit,the Symptom Management After Reducing Therapy (SMART-1) aimed to addresswhether short-term combination therapy and the subsequent withdrawal of the αblocker would allow for a sustained reduction in symptoms and improvement inflow rates. After 24 weeks of combination therapy 77% of those who withdrew αblocker (tamsulosin) and remained on 5 α reductase treatment (dutasteride) felt bet-ter or the same as on their previous assessment compared to 91% who continued onα blocker for 30 weeks and then withdrew. Interestingly, by week 36 after withdrawalin either group, the IPSS symptom score returned to the levels when the patients wereon combination therapy. This suggests that combination therapy from 24-30 weeks isprobably as effective as long term treatment and the period of combination may needto be longer (the full 30 weeks) in those with initially worse symptoms versus thosewith fewer symptoms (combine for only 24 weeks). (Barkin, J., M. Guimaraes, et al.2003).
The TRIUMPH studyThis study reported the usage and effectiveness of various LUTS/BPH drugsin real-life practice across six European centres. The study involved 2351newly-presenting LUTS/BPH patients followed over a 1-year follow-up period.Treatment, co-morbidities, complications and drugs prescribed were recorded, whilethe patients completed an IPSS questionnaire with the change in the IPSS scorebeing the primary outcome measure. Over the study period 74.9% of patients wereprescribed medication, the majority (83% of those medicated) were prescribed onlya single drug. Tamsulosin was the most commonly prescribed drug in all countries(38% of medicated cases), although with considerable variation. The α-blockerswere the most effective, with a mean reduction of 6.3 IPSS points. Finasteride wasslightly less effective (4.1 points). Significant improvements were seen in 43% ofpatients on phytotherapy with Serenoa repens or Pygeum africanum compared to57% of those on finasteride and 68% on α-blockers. The only combination therapyfound to produce a statistically significant improvement over the use of individualdrugs was finasteride+tamsulosin (8.1 points compared to 6.7 for tamsulosin aloneand 4.2 for finasteride alone). All drug treatments showed some improvement
39
Chapter 9. Benign Prostate Disorders
over watchful-waiting for most patients over the study period: the α-blockerswere found to be the most effective. There were marked national differences inprescribing patterns, both in individual drug choice and in the use of combinationtherapies[203].
SURGICAL TREATMENT OF BPHThe indications for prostatectomy, by open approach or TURP are listed in Table 13.At present approximately 90% of prostatectomies are done by TURP. Open prostatec-tomy should be considered when a gland is estimated to weigh more that 75g, wherelarge bladder calculi exist that may not be dealt with endoscopically, where largebladder diverticulae requiring repair exist, if complex urethral conditions or whenorthopaedic abnormalities prevent positioning in lithotomy for TURP. Contraindica-tions to open prostatectomy include a small fibrous gland, prostate adenocarcinoma,previous prostatectomy or other surgery of the pelvis preventing access[204].
Table 14. Indications for Prostatectomy
1. Acute Urinary Retention
2. Recurrent or persistent urinary tract infections
3. Significant bother from LUTS secondary to bladder outflowobstruction not responding to medical therapy
4. Recurrent haematuria known to be of prostatic origin
5. Bladder Calculi
Transurethral resection of the prostate (TURP)TURP remains the most common surgical treatment for BPH[205]. TURP involveseither regional or general anaesthesia, with most patients spending a minimum ofone night in hospital. TURP involves surgically debulking the periurethral and tran-sitional zones of the prostate to relieve obstruction. Debulking is done by electro-cautery in the standard TURP through endoscopic instruments introduced into theurethra and bladder. Tissue is resected in small pieces until the adenoma is removedand a new channel for passage in the prostatic urethra created, much like fashion-ing a pumpkin for Halloween with the capsule left behind. Despite using electro-cautery, there are mild to severe degrees of haemorrhage, depending on the glandsize. However transfusions are rarely needed and the procedure is relatively free oflife-threatening complications and most patients experience satisfactory resolutionof their micturition symptoms. Studies on urinary peak flow rates and invasive pres-sure flow have demonstrated the superiority of TURP over minimally invasive ther-apies[206]. Complications of TURP include failure to void (6%), haemorrhage requir-ing transfusion (1-4%), clot retention (3%), infection (2%), bladder neck contractureor urethral stricture (6%), transurethral resection syndrome (2%), and rarely incon-tinence [89, 207, 208]. Transurethral resection syndrome is secondary to dilutionalhyponatraemia caused by absorption of the intravesical fluid uses in the TURP. Itis manifest by nausea, vomiting, hypertension, bradycardia and confusion[209]. Therisk increases with larger glands and longer resection times (greater than 1 hour).The TURP must be abandoned safely with diuretics administered quickly and fur-ther treatment initiated if there is no resolution.
Retrograde ejaculation is reported to occur in almost all patients undergoing TURP40
Chapter 9. Benign Prostate Disorders
as the normal bladder neck mechanism which contracts to allow antegrade ejacu-lation is surgically resected. Other studies have reported only 50% men with suchsymptoms.
Erectile dysfunction (ED) may be associated with TURP either via thermal nerve in-jury or emotional stress and was reported in early studies at a rate of 4-40%. This hasnow been shown to be an overestimation [83, 210]. The rate of ED in the AUA Co-operative study was found to be 13% in 1000 men [89]. The study also demonstratedan increase of around 20% of ED in the untreated group with BPH. Although ED isoften quoted as a side effect of TURP, Kassabian concluded that TURP (or even anyother surgical therapy) did not appear to have a long term effect on erectile functionor libido [83].
There has been one randomised controlled trial (Veterans Affairs Cooperative StudyGroup, see above) comparing TURP to “watchful waiting” or reassurance[207]. Thisdemonstrated that TURP showed greater benefit with 66% of patients having a de-crease in symptoms post TURP compared to 28% who were undergoing ‘watchfulwaiting”. TURP remains the ‘gold standard’ by which other surgical (and even med-ical) treatments are measured [83].
Open ProstatectomyThis is the oldest, most invasive therapy for BPH[211]. It is commonly done througha transvesical approach, but may be done retropubically. Early complications of thisoperation include haemorrhage, blood transfusion, sepsis and urinary retention withthe most common late complication being bladder neck stricture (2-3%)[204]. TURPhas lower perioperative morbidity but open prostatectomy produces equivalent, ifnot superior improvement with a similar or lower re-operation rate[212]. Sexual dys-function is not likely to be altered by the surgery [83, 213] however ED is still quotedat 3-5% risk[204]. Retrograde ejaculation occurs in 90% patients. Other complicationsof surgery such as deep vein thrombosis, myocardial infarction and stroke are lessthan 1%[204].
Minimally Invasive Surgical TherapiesMinimally invasive therapies for BPH have evolved in the past decade with the goalbeing to achieve symptomatic improvement that is durable, without the morbidityassociated with surgery or the long-term side effects or compliance issues associ-ated with medical therapies[206]. The aim of such treatments is to achieve resultssimilar to TURP but with minimal anaesthesia and hospitalisation. An overview ofrandomised controlled trials in 2000 by Tubaro et al[214] comparing minimally in-vasive and invasive modalities of treatment found re-treatment rates to be higher inthe minimally invasive group .They concluded that none of the minimally invasivetreatments were superior to TURP from a cost and benefit standpoint and that TURPremains the gold standard of treatment. Some view such treatments as in-betweenmedical and TURP, so their role is not completely defined, and we await long termdata on all proposed therapies.
Transurethral incision of the prostate
A similar approach to a TURP is used except that no surgical debulking is under-taken. Between one and three incisions are made into the prostate at the level of thebladder neck back almost to the insertion of the ejaculatory ducts. This releases the“ring” of BPH tissue at the bladder neck, creating a larger opening. There is a re-duced risk of morbidity such as haemorrhage. In some instances, ejaculation may bepreserved in younger men, especially if one incision is made. The procedure onlyworks if the tissue in the periurethral area is not too bulky, otherwise a “ball-valve”
41

Chapter 9. Benign Prostate Disorders
mechanism of adenoma may develop. Laser may be used for incisions of the prostate,as well as standard electrocautery[215].
Laser therapy for benign prostatic hyperplasia
Laser energy may be used to produce coagulation necrosis, vaporisation of tissueor resection of tissue[216]. Laser as an energy source has an advantage of standardelectrocautery by being relatively bloodless and does not carry the risk of hypona-traemia, which may rarely occur via absorption of irrigant in a standard TURP[215,217]. There are several evolving therapies for BPH involving lasers (see table x be-low) including Holmium laser resection of the prostate (HoLRP) and Holmium laserenucleation of the prostate (HoLEP) as well as more minimally invasive laser thera-pies. In well-trained hands, HoLEP may be performed on large glands where it maybe advantageous having no limit on resection time and also on fully anticoagulatedpatients with the only drawback being the use of a morcellator to remove the resectedtissue that is too large to pass out the resectoscope[218]. Holmium laser ablation ofthe prostate (HoLAP) utilising tissue vaporisation is rarely performed because theother methods, HoLEP and HoLEP are superior. The most recent addition to the lasertreatments is the KTP laser which utilises transurethral photoselective vaporisationof the prostate (TPVP)[219]. The KTP laser is said to be absorbed more strongly byhaemoglobin than water because of its wavelength and so can heat and vaporise tis-sue rather than have energy scatter and have better vaporisation. A recent trial ofTPVP against standard TURP, produced equivalent improvements in flow rates andIPSS with reduced adverse events but long-term follow- up is needed to assess thedurability of these results[220].
Table 15. Lasers and their use in transurethral treatments of BPH
Laser Type CommonName
Wavelength Penetrationand effect
TransurethralProceduresfor BPH
Holmium:yttrium-aluminium-garnet
Ho:YAG orHolmium
2100nm,InvisibleInfrared
0.5mm,Cutting >Vaporisation
1. Holmiumlaserenucleation ofthe prostate(HoLEP)
2. Holmiumlaser re-sectionof theprostate(HoLRP)
3. Holmiumlaserablationof theprostate(Ho-LAP)
42
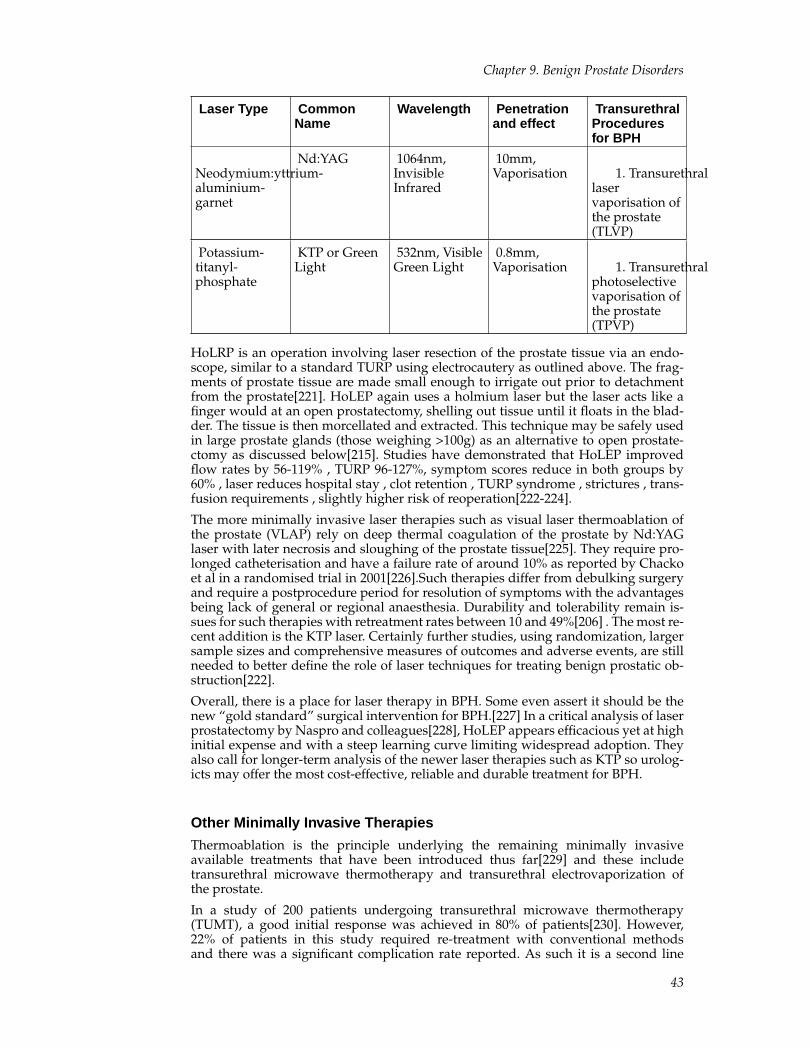
Chapter 9. Benign Prostate Disorders
Laser Type CommonName
Wavelength Penetrationand effect
TransurethralProceduresfor BPH
Neodymium:yttrium-aluminium-garnet
Nd:YAG 1064nm,InvisibleInfrared
10mm,Vaporisation 1. Transurethral
laservaporisation ofthe prostate(TLVP)
Potassium-titanyl-phosphate
KTP or GreenLight
532nm, VisibleGreen Light
0.8mm,Vaporisation 1. Transurethral
photoselectivevaporisation ofthe prostate(TPVP)
HoLRP is an operation involving laser resection of the prostate tissue via an endo-scope, similar to a standard TURP using electrocautery as outlined above. The frag-ments of prostate tissue are made small enough to irrigate out prior to detachmentfrom the prostate[221]. HoLEP again uses a holmium laser but the laser acts like afinger would at an open prostatectomy, shelling out tissue until it floats in the blad-der. The tissue is then morcellated and extracted. This technique may be safely usedin large prostate glands (those weighing >100g) as an alternative to open prostate-ctomy as discussed below[215]. Studies have demonstrated that HoLEP improvedflow rates by 56-119% , TURP 96-127%, symptom scores reduce in both groups by60% , laser reduces hospital stay , clot retention , TURP syndrome , strictures , trans-fusion requirements , slightly higher risk of reoperation[222-224].
The more minimally invasive laser therapies such as visual laser thermoablation ofthe prostate (VLAP) rely on deep thermal coagulation of the prostate by Nd:YAGlaser with later necrosis and sloughing of the prostate tissue[225]. They require pro-longed catheterisation and have a failure rate of around 10% as reported by Chackoet al in a randomised trial in 2001[226].Such therapies differ from debulking surgeryand require a postprocedure period for resolution of symptoms with the advantagesbeing lack of general or regional anaesthesia. Durability and tolerability remain is-sues for such therapies with retreatment rates between 10 and 49%[206] . The most re-cent addition is the KTP laser. Certainly further studies, using randomization, largersample sizes and comprehensive measures of outcomes and adverse events, are stillneeded to better define the role of laser techniques for treating benign prostatic ob-struction[222].
Overall, there is a place for laser therapy in BPH. Some even assert it should be thenew “gold standard” surgical intervention for BPH.[227] In a critical analysis of laserprostatectomy by Naspro and colleagues[228], HoLEP appears efficacious yet at highinitial expense and with a steep learning curve limiting widespread adoption. Theyalso call for longer-term analysis of the newer laser therapies such as KTP so urolog-icts may offer the most cost-effective, reliable and durable treatment for BPH.
Other Minimally Invasive Therapies
Thermoablation is the principle underlying the remaining minimally invasiveavailable treatments that have been introduced thus far[229] and these includetransurethral microwave thermotherapy and transurethral electrovaporization ofthe prostate.
In a study of 200 patients undergoing transurethral microwave thermotherapy(TUMT), a good initial response was achieved in 80% of patients[230]. However,22% of patients in this study required re-treatment with conventional methodsand there was a significant complication rate reported. As such it is a second line
43
Chapter 9. Benign Prostate Disorders
option only at this stage[231]. In a further study of high energy TUMT versus TURP,the IPSS improved in the TUMT group by 60% in year 1 however by 3 years, theimprovement was not as apparent, being only 43% on IPSS.. Again, the re-treatmentrate was 20% at 3 years. Voiding flow rate as measured by uroflowmetry improvedby 64% at year 1, but this reduced to 29% by the end of year 3. This may becompared to the “gold-standard” TURP which had an IPSS reduction of 80-85%that remained stable over the 3 years, with a re-treatment rate of only 13%.Voiding flow rates improved by 214% in the TURP group and remained stablewhilst re-treatments were generally for complications (eg. strictures or bladderneck contractures) rather than treatment failures[232]. Note that with lower energyTUMT protocols there is much less improvement in IPSS scores and voiding flowrates, and with 50-60% pre-treatment rates[233].
Transurethral electrovaporization of the prostate (TUVT) has had promising results.In a study of 235 men randomised to TURP or TUVT, both groups achieved IPSSreductions of around 12 points and improvements in Qmax of 10ml/sec[234]. How-ever, TUVT did not lead to a reduction in postoperative morbidity or shorter hospitalstays.
Intraprostatic stents
In keeping with the principles of minimal invasion, a stent or coil is placed into theurethra at the point of maximal obstruction under local anaesthesia, endoscopic andradiographic guidance. Stents may be temporary/biodegradable or permanent. Al-though effective in the short term, they do have a significant complication rate raisingconcerns over safety and large randomised controlled trials are needed to establishtheir long term efficacy and their true role in the management of BPH [208, 235, 236].
Future Treatments : Botulinum Toxin
Evidence from the use of botulinum toxin in other lower urinary tract disorders ofmuscle spasticity (e.g. detrusor hyperreflexia, detrusor sphincter dyssynergia) hasled to its expanded application in non-neurogenic conditions such as idiopathic de-trusor overactivity, detrusor underactivity[237, 238] and has now led to preliminarystudies in men with BPH[239, 240] . Although its mechanism of action in the prostateis unclear, botulinum toxin A has been shown to block the release of neurotransmit-ters such as acetylcholine at the neuromuscular junction as well as in autonomic neu-rons [241]. There may also be significant inhibitory effects on urethral norepinephrinerelease[242] and intraprostatic injection of botulinum toxin A induces selective den-ervation and subsequent atrophy of the glands via apoptosis [243]. Thus due to thehyperplasia of connective and smooth muscular tissue in BPH, the prostate wouldseem to be an ideal location for botulinum toxin to have a pharmacological and clin-ical effect and we await more data.[244]
MEASURING OUTCOMES AND EFFECTIVENESS OFTREATMENTWhen considering the effectiveness of any treatment for BPH, one must consider theefficacy and tolerability of invasive or medical therapies (ie. the effect on both subjec-tive symptoms and urinary flow and incidence of adverse effects), the long-term ef-fectiveness, the impact on daily life activities (quality of life) and the costs[245]. Largescale randomised controlled trials provide information on the tolerability and effi-cacy of treatment options and evidence-based databases such as Cochrane reviews,may further analyse evidence-based data from multiple trials (Table 15).
44
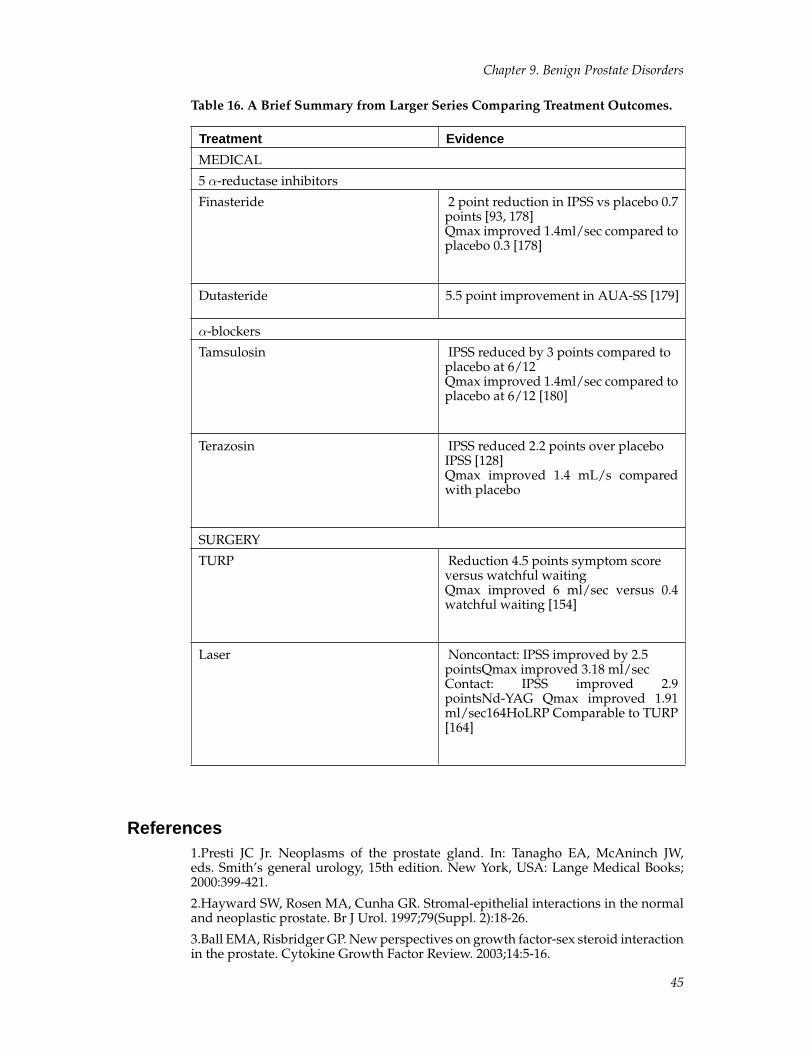
Chapter 9. Benign Prostate Disorders
Table 16. A Brief Summary from Larger Series Comparing Treatment Outcomes.
Treatment Evidence
MEDICAL
5 α-reductase inhibitors
Finasteride 2 point reduction in IPSS vs placebo 0.7points [93, 178]Qmax improved 1.4ml/sec compared toplacebo 0.3 [178]
Dutasteride 5.5 point improvement in AUA-SS [179]
α-blockers
Tamsulosin IPSS reduced by 3 points compared toplacebo at 6/12Qmax improved 1.4ml/sec compared toplacebo at 6/12 [180]
Terazosin IPSS reduced 2.2 points over placeboIPSS [128]Qmax improved 1.4 mL/s comparedwith placebo
SURGERY
TURP Reduction 4.5 points symptom scoreversus watchful waitingQmax improved 6 ml/sec versus 0.4watchful waiting [154]
Laser Noncontact: IPSS improved by 2.5pointsQmax improved 3.18 ml/secContact: IPSS improved 2.9pointsNd-YAG Qmax improved 1.91ml/sec164HoLRP Comparable to TURP[164]
References1.Presti JC Jr. Neoplasms of the prostate gland. In: Tanagho EA, McAninch JW,eds. Smith’s general urology, 15th edition. New York, USA: Lange Medical Books;2000:399-421.
2.Hayward SW, Rosen MA, Cunha GR. Stromal-epithelial interactions in the normaland neoplastic prostate. Br J Urol. 1997;79(Suppl. 2):18-26.
3.Ball EMA, Risbridger GP. New perspectives on growth factor-sex steroid interactionin the prostate. Cytokine Growth Factor Review. 2003;14:5-16.
45
Chapter 9. Benign Prostate Disorders
4.Cuntha GR, Alarid ET, Turner T, et al. Normal and abnormal development of themale urogenital tract. Role of androgens, mesenchymal-epithelial interactions andgrowth factors. J Androl. 1992;13:465-475
5.Delmas V, Dauge MC. Embryology of the prostate- current state of knowledge. In:Khoury S CC, Murphy G, Denis L, ed. Prostate cancer in questions. Edinburgh, UK:ICI publications; 1991:16-17.
6.Moore KL. The developing human. Philadelphia, USA: W.B. Saunders Company;1988.
7.McNeal JE. The zonal anatomy of the prostate. Prostate. 1981;2::35-49.
8.Berry SW, Coffey DS, Walsh PC, et al. The development of human benign prostatehyperplasia with age. J Urol. 1984;132:474-479.
9.McNeal JE. Normal and pathologic anatomy of the prostate. Urology. 1981;17(suppl):11-16.
10.Algaba F. Lobar division of the prostate. In: Khoury S CC, Murphy G, Denis L, ed.Prostate cancer in questions. Edinburgh, UK: ICI publications; 1991:16-17.
11.Kiyoshima K, Yokomizo A, Yoshida T, Tomita K, Yonemasu H, Nakamura M, OdaY, Naito S, Hasegawa Y. Anatomical features of periprostatic tissue and its surround-ings: A histological analysis of 79 radical retropubic prostatectomy specimens. Jpn JClin Oncol. 2004;34:463-468
12.Ali M, Johnson IP, Hobson J, Mohammadi B, Khan F. Anatomy of the pelvic plexusand innervation of the prostate gland. Clin Anat. 2004;17:123-129
13.Benoit G, Merlaud L, Meduri G, Moukarzel M, Quillard J, Ledroux M, Giuliano F,Jardin A. Anatomy of the prostatic nerves. Surg Radiol Anat. 1994;16:23-29
14.Powell MS, Li R, Dai H, Sayeeduddin M, Wheeler TM, Ayala GE. Neuroanatomyof the normal prostate. Prostate. 2005;65:52-57
15.Walsh PC. Radical retropubic prostatectomy with reduced morbidity: Ananatomic approach. NCI Monogr. 1988:133-137
16.Walsh PC, Quinlan DM, Morton RA, Steiner MS. Radical retropubicprostatectomy. Improved anastomosis and urinary continence. Urol Clin North Am.1990;17:679-684
17.Walsh PC, Lepor H, Eggleston JC. Radical prostatectomy with preservation of sex-ual function: Anatomical and pathological considerations. Prostate. 1983;4:473-485
18.Eichelberg C, Erbersdobler A, Michl U, Schlomm T, Salomon G, Graefen M, Hu-land H. Nerve distribution along the prostatic capsule. Eur Urol. 2006
19.Kourambas J, Angus DG, Hosking P, Chou ST. A histological study of denonvil-liers’ fascia and its relationship to the neurovascular bundle. Br J Urol. 1998;82:408-410
20.Syme DB, Corcoran NM, Bouchier-Hayes DM, Costello AJ. Hope springs eternal:Cavernosal nerve regeneration. BJU Int. 2006;97:17-21
21.Epstein JL. Non-neoplastic diseases of the prostate. In: Bostwick DG EJUSP, 1stEdition, ed. St louis, USA. Mosby-Year Book Inc: 307-340; 1997.
22.Warhol MJ, Longtine JA. The ultrastructural localization of prostatic specific anti-gen and prostatic acid phosphatase in hyperplastic and neoplastic human prostates.J Urol. 1985;134:607-613
23.Di Sant’Agnese PA. Neuroendocrine differentiation in human prostatic carcinoma.Hum Pathol. 1992;23:287-296
24.Donkervoort T, Sterling A, van Ness J, Donker PJ. A clinical and urodynamic studyof tadenan in the treatment of benign prostatic
hypertrophy. Eur Urol. 1977;3:218-225
46
Chapter 9. Benign Prostate Disorders
25.Brawer MK, Kirby R. Prostate specific antigen, 2nd edn. Oxford, UK: Health PressLimited; 1999.
26.Partin AW, Rodriguez R. The molecular biology, endocrinology, and physiology ofthe prostate and seminal vesicles. In: Walsh PC, ed. Campbell’s urology. Philadelphia:Saunders; 2002:1237-1296.
27.Ganong W. Review of medical physiology. Stamford: Appleton and Lange; 1997.
28.Eaton CL. Aetiology and pathogenesis of benign prostatic hyperplasia. Curr OpinUrol. 2003;13:7-10
29.Luo J, Dunn T, Ewing C, et al. Gene expression signature of benign prostatic hy-perplasia revealed by cdna microarray analysis. Prostate. 2002;51:189-200.
30.Suzuki K, Obara K, Kobayashi K, Yamana K, Bilim V, Itoi T, Takahashi K. Role ofconnective tissue growth factor in fibronectin synthesis in cultured human prostatestromal cells. Urology. 2006;67:647-653
31.Marengo SR, Chung LW. An orthotopic model for the study of growth factors inthe ventral prostate of the rat: Effects of epidermal growth factor and basic fibroblastgrowth factor. J Androl. 1994;15:277-286
32.Cooke PS, Young P, Cunha GR. Androgn receptor expression in developing malereproductive organs. Endocrinology. 1991;128:2867-2873
33.Gao J, Arnold JT, Isaacs JT. Conversion from a paracrine to an autocrine mecha-nism of androgen-stimulated growth during malignant transformation of prostaticepithelial cells. Cancer Res. 2001;61:5038-5044
34.Bartsch G, Rittmaster RS, Klocker H. Dihydrotestosterone and the concept of5alpha-reductase inhibition in human benign prostatic hyperplasia. World J Urol.2002;19:413-425
35.Wright AS, Douglas RC, Thomas LN, et al. Androgen-induced regrowth in the cas-trated rat ventral prostate: Role of 5alpha-reductase. Endocrinology. 1999;140:4509-4515.
36.Grino PB, Griffin JE, Wilson JD. Testosterone at high concentrations interacts withthe human androgen receptor similarly to dihydrotestosterone. Endocrinology.1990;126:1165-1172.
37.Wright AS, Thomas LN, Douglas RC, et al. Relative potency of testosterone anddihydrotestosterone in preventing atrophy and apoptosis in the prostate of the cas-trated rat. J Clin Invest. 1996;98:2558-2563.
38.Page ST, Lin DW, Mostaghel EA, Hess DL, True LD, Amory JK, Nelson PS,Matsumoto AM, Bremner WJ. Persistent intraprostatic androgen concentrationsafter medical castration in healthy men. J Clin Endocrinol Metab. 2006;91:3850-3856
39.Forti G, Salerno R, Moneti G, Zoppi S, Fiorelli G, Marinoni T, Natali A, CostantiniA, Serio M, Martini L, et al. Three-month treatment with a long-acting gonadotropin-releasing hormone agonist of patients with benign prostatic hyperplasia: Effects ontissue androgen concentration, 5 alpha-reductase activity and androgen receptor con-tent. J Clin Endocrinol Metab. 1989;68:461-468
40.Barrack ER, Berry SJ. DNA synthesis in the canine prostate; effects of androgeninduction and estrogen treatment. Prostate. 1987;10:45-56.
41.Gooren LJ, Toorians AW. Significance of oestrogens in male (patho)physiology.Ann Endocrinol (Paris). 2003;64:126-135
42.Risbridger GP, Bianco JJ, Ellem SJ, McPherson SJ. International congress on hor-monal steroids and hormones and cancer: Oestrogens and prostate cancer. EndocrRelat Cancer. 2003;10:187-191
43.Tsurusaki T, Aoki D, Kanetake H, Inoue S, Muramatsu M, Hishikawa Y, Koji T.Zone-dependent expression of estrogen receptors alpha and beta in human benignprostatic hyperplasia. J Clin Endocrinol Metab. 2003;88:1333-1340
47
Chapter 9. Benign Prostate Disorders
44.Steiner MS, Raghow S. Antiestrogens and selective estrogen receptor modulatorsreduce prostate cancer risk. World J Urol. 2003;21:31-36
45.Jenkins DJ, Kendall CW, D’Costa MA, Jackson CJ, Vidgen E, Singer W, SilvermanJA, Koumbridis G, Honey J, Rao AV, Fleshner N, Klotz L. Soy consumption and phy-toestrogens: Effect on serum prostate specific antigen when blood lipids and oxidizedlow-density lipoprotein are reduced in hyperlipidemic men. J Urol. 2003;169:507-511
46.Shibata K, Hirasawa A, Moriyma N, et al. Alpha1a-adrenoceptor polymorphism:Pharmacological characterization and association with benign prostatic hypertrophy.Br J Pharm. 1996;118:1403-1408.
47.Ekman P. The prostate as an endocrine organ: Androgens and estrogens. ProstateSuppl. 2000;10:14-18
48.Verhamme KM, Dieleman JP, Bleumink GS, van der Lei J, Sturkenboom MC, Art-ibani W, Begaud B, Berges R, Borkowski A, Chappel CR, Costello A, Dobronski P,Farmer RD, Jimenez Cruz F, Jonas U, MacRae K, Pientka L, Rutten FF, van SchayckCP, Speakman MJ, Tiellac P, Tubaro A, Vallencien G, Vela Navarrete R. Incidence andprevalence of lower urinary tract symptoms suggestive of benign prostatic hyperpla-sia in primary care--the triumph project. Eur Urol. 2002;42:323-328
49.Jacobsen SJ, Jacobson DJ, Girman CJ, Roberts RO, Rhodes T, Guess HA, LieberMM. Treatment for benign prostatic hyperplasia among community dwellingmen: The olmsted county study of urinary symptoms and health status. J Urol.1999;162:1301-1306
50.Marberger MJ, Andersen JT, Nickel JC, Malice MP, Gabriel M, Pappas F, MeehanA, Stoner E, Waldstreicher J. Prostate volume and serum prostate-specific antigen aspredictors of acute urinary retention. Combined experience from three large multi-national placebo-controlled trials. Eur Urol. 2000;38:563-568
51.Clifford GM, Logie J, Farmer RD. How do symptoms indicative of bph progressin real life practice? The uk experience. Eur Urol. 2000;38 Suppl 1:48-53
52.Lowe FC. Goals for benign prostatic hyperplasia therapy. Urology. 2002;59:1-2
53.Moore RA. Benign prostatic hypertrophy and carcinoma of the prostate. Occur-rence and experimental production in animals. Surgery. 1944;16:152-167.
54.Sanda MG, Beaty TH, Strutzman RE, et al. Genetic susceptibility of benign pro-static hyperplasia. J Urol. 1994;152:115-119.
55.Sanda MG, Beaty TH, Stutzman RE, Childs B, Walsh PC. Genetic susceptibility ofbenign prostatic hyperplasia. J Urol. 1994;152:115-119
56.Sidney S, Quesenberry CP, Jr., Sadler MC, Guess HA, Lydick EG, Cattolica EV.Incidence of surgically treated benign prostatic hypertrophy and of prostatecancer among blacks and whites in a prepaid health care plan. Am J Epidemiol.1991;134:825-829
57.Choi J, Ikeguchi EF, Lee SW, Choi HY, Te AE, Kaplan SA. Is the higher prevalenceof benign prostatic hyperplasia related to lower urinary tract symptoms in koreanmen due to a high transition zone index? Eur Urol. 2002;42:7-11
58.Geller J, Sionit L, Partido C, Li L, Tan X, Youngkin T, Nachtsheim D, Hoffman RM.Genistein inhibits the growth of human-patient bph and prostate cancer in histocul-ture. Prostate. 1998;34:75-79
59.Chyou PH, Nomura AM, Stemmermann GN, Hankin JH. A prospective study ofalcohol, diet, and other lifestyle factors in relation to obstructive uropathy. Prostate.1993;22:253-264
60.Isaacs JT, Coffey DS. Etiology and disease process of benign prostatic hyperplasia.The Prostate Supplement. 1989;2:33-50.
61.McNeal JE. Origin and evaluation of benign prostatic enlargement. Invest Urol.1978;15:340-345.
48
Chapter 9. Benign Prostate Disorders
62.Caine M. The present role of alpha-adrenergic blockers in the treatment of benignprostatic hypertrophy. J Urol. 1986;136:1-4
63.Akduman B, Crawford ED. Terazosin, doxazosin, and prazosin: Current clinicalexperience. Urology. 2001;58:49-54
64.Rhodes T, Girman CJ, Jacobsen SJ, Roberts RO, Guess HA, Lieber MM. Longitudi-nal prostate growth rates during 5 years in randomly selected community men 40 to79 years old. J Urol. 1999;161:1174-1179
65.Fitzpatrick JM. The natural history of benign prostatic hyperplasia. BJU Int.2006;97 Suppl 2:3-6; discussion 21-22
66.Lepor H, Williford WO, Barry MJ, Haakenson C, Jones K. The impact of medicaltherapy on bother due to symptoms, quality of life and global outcome, and factorspredicting response. Veterans affairs cooperative studies benign prostatic hyperpla-sia study group. J Urol. 1998;160:1358-1367
67.Wessells H, Roy J, Bannow J, Grayhack J, Matsumoto AM, Tenover L, Herlihy R,Fitch W, Labasky R, Auerbach S, Parra R, Rajfer J, Culbertson J, Lee M, Bach MA,Waldstreicher J. Incidence and severity of sexual adverse experiences in finasterideand placebo-treated men with benign prostatic hyperplasia. Urology. 2003;61:579-584
68.Bruskewitz R, Girman CJ, Fowler J, Rigby OF, Sullivan M, Bracken RB, FusilierHA, Kozlowski D, Kantor SD, Johnson EL, Wang DZ, Waldstreicher J. Effect of finas-teride on bother and other health-related quality of life aspects associated with be-nign prostatic hyperplasia. Pless study group. Proscar long-term efficacy and safetystudy. Urology. 1999;54:670-678
69.Isaacs JT, Coffey DS. Etiology and disease process of benign prostatic hyperplasia.Prostate Suppl. 1989;2:33-50
70.Bosch RJ. Pathogenesis of benign prostatic hyperplasia. Eur Urol. 1991;20 Suppl1:27-30
71.Sciarra A, Di Silverio F, Salciccia S, Autran Gomez AM, Gentilucci A, Gentile V.Inflammation and chronic prostatic diseases: Evidence for a link? Eur Urol. 2007
72.Peters TJ, Donovan JL, Kay HE, et al. The international continence society ’be-nign prostatic hyperplasia study’: The bothersomeness of urinary symptoms. J Urol.1997;157:885-889
73.Scarpa RM. Lower urinary tract symptoms (luts): What are the implications forthe patients? Eur Urol. 2001;40(Suppl. 4):12-20.
74.Garraway WM, Collins GN, Lee RJ. High prevalence of benign prostatic hypertro-phy in the community. Lancet. 1991;338:469-471.
75.Bates P, Bradley WE, Glen E, Melchior H, Rowan D, Sterling A, Hald T. The stan-dardization of terminology of lower urinary tract function. Eur Urol. 1976;2:274-276
76.Lepor H. Alpha1-adrenoceptor selectivity: Clinical or theoretical benefit? Br J Urol.1995;76 (Suppl. 1):57-61.
77.Welch G, Kawachi I, Barry MJ, et al. Distinction between symptoms of voiding andfilling in benign prostatic hyperplasia: Findings from health professionals follow-upstudy. Urology. 1998;1998
78.Abrams P. New words for old: Lower urinary tract symptoms for ’prostatism’.BMJ. 1994;308:929-930.
79.Puppo P. Do we know everything about alpha-blockade in the management oflower urinary tract symptoms? Eur Urol. 2001;39 Suppl 2:38-41
80.Price D. Potential mechanisms of action of superselective alpha1-adrenoceptor an-tagonists. Eur Urol. 2002;40(Suppl. 1):5-11.
81.Michel MC. Physiology and pathophysiology of lower urinary tract symptoms.Drugs of Today. 2001;37 (Suppl.D):7-11
49
Chapter 9. Benign Prostate Disorders
82.Van Moorselaar R, Emberton M, Harving N, Matzkin H, Hartung R, Alcaraz A, El-hilali M, Vallancien G, group A-os. Alfuzosin 10mg once daily improves sexual func-tion in men with luts and concomitant sexual dysfunction. J Urol. 2003;169 (Suppl4):478
83.Kassabian VS. Sexual function in patients treated for benign prostatic hyperplasia.Lancet. 2003;361:60-62
84.Leliefeld HH, Stoevelaar HJ, McDonnell J. Sexual function before and after varioustreatments for symptomatic benign prostatic hyperplasia. BJU Int. 2002;89:208-213
85.Jacobsen SJ, Jacobsen DJ, Girman CJ, et al. Natural history of prostatism: Risk fac-tors for acute urinary retention. J Urol. 1997;158:481-487.
86.Douenias R, Rich M, Badlani M, et al. Predisposing factors in bladder calculi: Areview of 100 cases. Urology. 1991;37:240-243.
87.McConnell JD. Benign prostatic hyperplasia. J Urol. 1994;152:459-460.
88.Westenberg A, Harper M, Zafirakis H, et al. Bladder and renal stones: Manage-ment and treatment. Hospital Medicine. 2002;63:34-41.
89.Mebust WK, Holtgrewe HL, Cockett ATK, et al. Transurethral prostatectomy: Im-mediate and postoperative complications. A cooperative study of 13 partcipating in-stitutions evaluating 3885 patients. J Urol. 1989;141:243-247.
90.O’Connor RC, Laven BA, Bales GT, et al. Nonsurgical management of benign pro-static hyperplasia in men with bladder calculi. Urology. 2002;60:288-291
91.Marshall S, Narayan P. Treatment of prostatic bleeding: Suppression of angiogen-esis by androgen deprivation. J Urol. 1993;149:1553.
92.Foley SJ, Bailey DM. Microvessel disease in prostatic hyperplasia. BJU Int.2000;85:70-73.
93.Kashif KM, Foley SJ, Basketter V, Holmes SA. Haematuria associated with bph-natural history and a new treatment option. Prostate Cancer Prostatic Dis. 1998;1:154-156
94.Saez C, Cgonzalez-Baena AC, Japon MA, et al. Regressive changes in finasteride-treated human hyperplastic prostate correlate with an upregulation of tgf-beta recep-tor expression. Prostate. 1998;37:84-90.
95.Monti S, Sciarra F, Adaqmo EV, et al. Prevalent decrease in the egf content in theperiurethral zone of bph. J Am. 1997;18:488-494.
96.Jepsen JV, Bruskewitz RC. Clinical manifestations and indications for treatment.In: Lepor H, ed. Prostatic diseases. Philadelphia: WB Saunders; 2000:127-142.
97.Andersson K-E. Pharmacology of lower urinary tract smooth muscles and penileerectile tissues. Pharmacol Rev. 1993;45:253-308.
98.Barry MJ, Fowler FJ, Jr., O’Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK,Cockett AT. The american urological association symptom index for benign prostatichyperplasia. The measurement committee of the american urological association. JUrol. 1992;148:1549-1557; discussion 1564
99.Kakizaki H, Koyanagi T. Current view and status of lower urinary tract symptomsand neurogenic lower urinary tract dysfunction. BJU Int. 2000;85(Suppl. 2):25-30
100.Lepor H, Nieder A, Feser J, et al. Effect of terazosin on prostatism in men withnormal and abnormal peak urinary flow rates. Urology. 1997;49:476-480
101.Serels S, Stein M. Prospective study comparing hyoscyamine, doxazosin andcombination therapy for treatment of urgency and frequency in women. NeurourolUrodynam. 1998;17:31-36.
102.Hampel C, Dolber PC, Savic SL, et al. Changes in a1 adrenergic receptor (ar)subtype gene expression during bladder outlet obstruction of rats (abstract). J Urol.2000;163:228
50
Chapter 9. Benign Prostate Disorders
103.Stamey TA, Johnstone IM, McNeal JE, Lu AY, Yemoto CM. Preoperative serumprostate specific antigen levels between 2 and 22 ng./ml. Correlate poorly with post-radical prostatectomy cancer morphology: Prostate specific antigen cure rates appearconstant between 2 and 9 ng./ml. J Urol. 2002;167:103-111
104.Stamey TA, Caldwell M, McNeal JE, Nolley R, Hemenez M, Downs J. Theprostate specific antigen era in the united states is over for prostate cancer: Whathappened in the last 20 years? J Urol. 2004;172:1297-1301
105.Prestigiacomo AF, Stamey TA. Clinical usefulness of free and complexed psa.Scand J Clin Lab Invest Suppl. 1995;221:32-34
106.Girman CJ, Epstein RS, Jacobsen SJ, Guess HA, Panser LA, Oesterling JE, LieberMM. Natural history of prostatism: Impact of urinary symptoms on quality of life in2115 randomly selected community men. Urology. 1994;44:825-831
107.Chartier-Kastler E, Chapple CR. Luts/bph in clinical practice: The importance ofnocturia and quality of sleep. BJU Int. 2006;98 Suppl 2:3-8
108.Haltbakk J, Hanestad BR, Hunskaar S. How important are men’s lower urinarytract symptoms (luts) and their impact on the quality of life (qol)? Qual Life Res.2005;14:1733-1741
109.de Kretser DM, Cock M, Holden C. The men in australia telephone survey(mates) - lessons for all. Med J Aust. 2006;185:412-413
110.Holden CA, Jolley DJ, McLachlan RI, Pitts M, Cumming R, Wittert G,Handelsman DJ, de Kretser DM. Men in australia telephone survey (mates):Predictors of men’s help-seeking behaviour for reproductive health disorders. Med JAust. 2006;185:418-422
111.Tubaro A, Trucchi A, Miano L. Investigation of benign prostatic hyperplasia. Cur-rent Opinion in Urology. 2003;13:17-22.
112.de la Rosette JJ, Alivizatos G, Madersbacher S, Perachino M, Thomas D, Des-grandchamps F, de Wildt M. Eau guidelines on benign prostatic hyperplasia (bph).Eur Urol. 2001;40:256-263; discussion 264
113.Roehrborn CG, Bartsch G, Kirby R, Andriole G, Boyle P, de la Rosette J, Perrin P,Ramsey E, Nordling J, De Campos Freire G, Arap S. Guidelines for the diagnosis andtreatment of benign prostatic hyperplasia: A comparative, international overview.Urology. 2001;58:642-650
114.Recommendations of the International Science Committee. The evaluation andtreatment of lower urinary tract symptoms suggestive of benign prostatic obstruc-tion. Paris: Proceedings of the 4th International Consultation on BPH; 1997.
115.Chai TC, Belville WD, McGuire EJ, et al. Urological association voiding symptomindex: Comparison of unselected and selected samples of both sexes. J Urol. 1993;150.
116.Lepor H, Machi G. Comparison of aua symptom index in unselected males andfemales between fifty-five and seventy-nine years of age. Urology. 1993;42.:36-40
117.Barry MJ. Evaluation of symptoms and quality of life in men with benign pro-static hyperplasia. Urology. 2001;58:25-32
118.Yalla SV, Sullivan MP, Lecamwasam HS, DuBeau CE, Vickers MA, Cravalho EG.Correlation of american urological association symptom index with obstructive andnonobstructive prostatism. J Urol. 1995;153:674-679; discussion 679-680
119.Jensen KM, Jorgensen TB, Mogensen P. Long-term predictive role of urodynam-ics: An 8-year follow-up of prostatic surgery for lower urinary tract symptoms. Br JUrol. 1996;78:213-218
120.Roehrborn CG, Sech S, Montoya J, Rhodes T, Girman CJ. Interexaminer reliabilityand validity of a three-dimensional model to assess prostate volume by digital rectalexamination
is there a place for combination medical therapy? Urology. 2001;57:1087-1092
51
Chapter 9. Benign Prostate Disorders
121.Souverein PC, Erkens JA, de la Rosette JJ, Leufkens HG, Herings RM. Drug treat-ment of benign prostatic hyperplasia and hospital admission for bph-related surgery.Eur Urol. 2003;43:528-534
122.Lobel B, Rodriguez A. Chronic prostatitis: What we know, what we do not know,and what we should do! World J Urol. 2003;21:57-63
123.Society AfGM-MSSaMSftSoVD-DS. 2002 national guideline for the managementof prostatitis. 2002
124.Krieger JN, Nyberg L, Jr., Nickel JC. Nih consensus definition and classificationof prostatitis. Jama. 1999;282:236-237
125.Boyle P, Gould AL, Roehrborn CG. Prostate volume predicts outcome of treat-ment of benign prostatic hyperplasia with finasteride: Meta-analysis of randomizedclinical trials. Urology. 1996;48:398-405
126.Rovner ES, Wein AJ. Practical urodynamics, part 1. AUA Update Series.2002;21:146-151
127.Feneley MR, Dunsmuir WD, Pearce J, Kirby RS. Reproducibility of uroflow mea-surement: Experience during a double-blind, placebo-controlled study of doxazosinin benign prostatic hyperplasia. Urology. 1996;47:658-663
128.van Verooij GEPM, Eckhardt MD, Gisolf KWH, et al. Data fromfrequency-volume charts versus filling cystometric estimated capacities andprevalence of instability in men with lower urinary tract symptoms suggestive ofbenign prostatic hyperplasia. Neurourol Urodyn. 2002;10:106-111
129.Hakenberg OW, Pinnock CB, Marshall VR. Preoperative urodynamic and symp-tom evaluation of patients undergoing transurethral prostatectomy: Analysis of vari-ables relevant for outcome. BJU Int. 2003;91:375-379
130.Chen SS, Hong JG, Hsiao YJ, et al. The correlation between clinical outcome andresidual prostatic weight ratio after transurethral resection of the prostate for benignprostatic hyperplasia. BJU Int. 2000;85:79-82.
131.Eri LM, Thomassen H, Brennhovd B, Haheim LL. Accuracy and repeatability ofprostate volume measurements by transrectal ultrasound. Prostate Cancer ProstaticDis. 2002;5:273-278
132.Mariappan P, Brown DJ, McNeill AS. Intravesical prostatic protrusion is betterthan prostate volume in predicting the outcome of trial without catheter in whitemen presenting with acute urinary retention: A prospective clinical study. J Urol.2007;178:573-577; discussion 577
133.Eastham JA. Prostate-specific antigen doubling time as a prognostic marker inprostate cancer. Nat Clin Pract Urol. 2005;2:482-491
134.Leach FS, Koh MS, Chan YW, Bark S, Ray R, Morton RA, Remaley AT. Prostatespecific antigen as a clinical biomarker for prostate cancer: What’s the take homemessage? Cancer Biol Ther. 2005;4:371-375
135.Pinsky PF, Kramer BS, Crawford ED, Grubb RL, Urban DA, Andriole GL, Chia D,Levin DL, Gohagan JK. Prostate volume and prostate-specific antigen levels in menenrolled in a large screening trial. Urology. 2006;68:352-356
136.Bartsch G, Fitzpatrick JM, Schalken JA, Isaacs J, Nordling J, Roehrborn CG. Con-sensus statement: The role of prostate-specific antigen in managing the patient withbenign prostatic hyperplasia. BJU Int. 2004;93 Suppl 1:27-29
137.Eri LM, Tveter KJ. Treatment of benign prostatic hyperplasia. A pharmacoeco-nomic perspective. Drugs Aging. 1997;10:107-118
138.MacDonald R, Ishani A, Rutks I, Wilt T J. A systematic review of cernilton for thetreatment of benign prostatic hyperplasia. BJU Int. 2000;85:836-841
139.Fitzpatrick JM. Psa measurement in the treatment of bph. BJU Int. 2004;93 Suppl1:2-4
52
Chapter 9. Benign Prostate Disorders
140.Trachtenberg J. Treatment of lower urinary tract symptoms suggestive of benignprostatic hyperplasia in relation to the patient’s risk profile for progression. BJU Int.2005;95 Suppl 4:6-11
141.Burke JP, Rhodes T, Jacobson DJ, McGree ME, Roberts RO, Girman CJ, LieberMM, Jacobsen SJ. Association of anthropometric measures with the presence and pro-gression of benign prostatic hyperplasia. Am J Epidemiol. 2006;164:41-46
142.Boyle P. Some remarks on the epidemiology of acute urinary retention. Arch ItalUrol Nefrol Androl. 1998;70:77-82
143.Glynn RJ, Campion EW, Bouchard GR, Silbert JE. The development of benignprostatic hyperplasia among volunteers in the normative aging study. Am J Epi-demiol. 1985;121:78-90
144.Sullivan M, Bell R, Reynard J, Keoghane S. How to pass the frcs(urol) - part 2.Urology Today. 2005;10
145.Wilt TJ, Ishani A, MacDonald R, et al. Saw palmetto extracts for treatment ofbenign prostatic hyperplasia: A systematic review. JAMA. 1998;280:1604-1609.
146.Lowe FC, et al. Phytotherapy in the treatment of benign prostatic hyperplasia:An update. Urology. 1999;53:671-678
147.Foley, Charlotte L, Kirby J, et al. 5 alpha-reductase inhibitors: What’s new? Cur-rent Opinion in Urology. 2003;13:31-37.
148.Gerber GS. Phytotherapy for benign prostatic hyperplasia. Current Urology Re-ports. 2002;3:285-291.
149.Fagelman E, Lowe FC. Herbal medications in the treatment of benign prostatichyperplasia (bph). Urol Clin North Am. 2002;29:23-29, vii
150.Dreikorn K. The role of phytotherapy in treating lower urinary tract symptomsand benign prostatic hyperplasia. World J Urol. 2002;19:426-435.
151.Dreikorn K. Other medical therapies. Proceedings of the fourth international con-sultation on benign prostatic hyperplasia (bph). In: Paris, ed. Paris: July: 2-5; 1997.
152.Lowe FC, Dreikorn K, A B, et al. Review of recent placebo controlled trials utliz-ing phytotherapeutic agents for treatment of bph. Prostate. 1998;37:187-193.
153.Delos S, Lehle C, Martin PM. Inhibition of the activity of basic 5-alpha reductase(type 1) detected in du 145 cells and expressed in insect cells. J Steroid Biochem MolBiol. 1994;48:347-352
154.Bayne CW, Grant ES, Chapman K. Characterisation of a new coculture model forbph which expresses 5-alpha reductase types 1 and 2: The effects of permixon on dhtformation [abstract]. J Urol. 1997;157(Suppl 4):755.
155.Carilla E, Briley M, Fauran F. Binding of permixon, a new treatment for prostaticbenign hyperplasia, to the cytosolic androgen receptor in the rat prostate. J SteroidBiochem. 1984;20:521-523
156.Sultan C, Terraza A, Devillier C. Inhibition of androgen metabolism and bindingby liposterolic extract of ’serenoa repens b’ in human foreskin fibroblasts. J SteroidBiochem. 1984;20:515-519
157.Carraro JC, JP R, Koch G. Comparison of phytotherapy (permixon) with finas-teride in the treatment of benign prostate hyperplasia: A randomized internationalstudy of 1098 patients. Prostate. 1996;29:231-240.
158.Braeckman J. The extract of serenoa repens in the treatment of benign prostatichyperplasia: A multicenter open study. 1994;55:776-785
159.Marks LS, Partin AP, Epstein JL. Effects of a saw palmetto herbal blend in menwith symptomatic benign prostatic hyperplasia. J Urol. 2000;163:1451-1456
160.Boyle P, C R, Lowe F, Roehrborn C. Meta-analysis of permixon in treatment ofsymptomatic benign prostatic hyperplasia: An update (abstract). J Urol. 2003;169(Suppl 4):334-335
53
Chapter 9. Benign Prostate Disorders
161.Hruby S, Djavan B, Reissigl A, Chaudr A, Alavi S, Anagnostou T, Bagheri F, HarikM, Remzi M, Marberger M. Progression delay in men with mild symptoms of blad-der outlet obstruction: A prospective comparative study of phytotherapy, watchfulwaiting, and placebo (abstract). J Urol. 2003;169 (Suppl 4):332
162.Gerber GS, Kuznetsov D, Johnson BC, Burstein JD. Randomized, double-blind,placebo-controlled trial of saw palmetto in men with lower urinary tract symptoms.Urology. 2001;58:960-964; discussion 964-965
163.Bent S, Kane C, Shinohara K, Neuhaus J, Hudes ES, Goldberg H, Avins AL. Sawpalmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354:557-566
164.Boyle P, Robertson C, Lowe F, Roehrborn C. Updated meta-analysis of clinicaltrials of serenoa repens extract in the treatment of symptomatic benign prostatic hy-perplasia. BJU Int. 2004;93:751-756
165.Debruyne FM. Medical management of bph: The debate continues. Eur Urol.2006;50:416-417
166.Carbin BE, Larsson B, Lindahl O. Treatment of benign prostatic hyperplasia withphytosterols. Br J Urol. 1990;66:639-641.
167.Fagelman E, Lowe FC. Herbal medications in the treatment of benign prostatichyperplasia (bph). Urol Clin North Am. 2002;29:23-29, vii
168.Caine M. The present role of alpha-adrenergic blockers in the treatment of benignprostatic hypertrophy. J Urol. 1986;136:1-4
169.Foley CL, Kirby J. 5 alpha-reductase inhibitors: What’s new? Current Opinion inUrology. 2003;13:31-37.
170.Zaida A, Rosenblum M, Crawford ED. Benign prostatic hyperplasia: Anoverview. Urology. 1999;53:1-6
171.Oesterling JE. Benign prostatic hyperplasia: Medical and minimally invasivetreatment options. N Engl J Med. 1995;332:99-109.
172.Kobayashi S, Tang R, Shapiro E, et al. Characterisation of human alpha1 adreno-ceptor using radioligand receptor binding on slide-mounted tissue section. J Urol.1993;150:2002-2006.
173.Caine M, Perlberg S, Meretyk S. A placebo controlled double blind study of theeffect of phenoxybenzamine in benign prostatic obstruction. Br J Urol. 1978; 50:551-554.
174.Foglar R, Shibata K, Horie K, et al. Use of recombinant alpha1-adrenoceptors tocharacterise subtype selectivity of drugs for the treatment of prostatic hypertrophy.Eur J Pharmacol. 1995;288:201-207.
175.Roehrborn CG. Efficacy and safety of once-daily alfuzosin in the treatment oflower urinary tract symptoms and clinical benign prostatic hyperplasia: A random-ized, placebo-controlled trial. Urology. 2001;58:953-959
176.Michel MC, Flannery MT, Narayan P. Worldwide experience with alfuzosin andtamsulosin. Urology. 2001;58:508-516
177.Boyle P, Robertson C, Manski R, Padley RJ, Roehrborn CG. Meta-analysis of ran-domized trials of terazosin in the treatment of benign prostatic hyperplasia. Urology.2001;58:717-722
178.Wilt TJ, MacDonald R, Nelson D. Tamsulosin for treating lower urinary tractsymptoms compatible with benign prostatic obstruction: A systematic review of effi-cacy and adverse effects. J Urol. 2002;167:177-183
179.Kirby RS, Roehrborn C, Boyle P, Bartsch G, Jardin A, Cary MM, Sweeney M,Grossman EB. Efficacy and tolerability of doxazosin and finasteride, alone or in com-bination, in treatment of symptomatic benign prostatic hyperplasia: The prospectiveeuropean doxazosin and combination therapy (predict) trial. Urology. 2003;61:119-126
54
Chapter 9. Benign Prostate Disorders
180.Gillenwater JY, Conn RL, Chrysant SG, Roy J, Gaffney M, Ice K, Dias N. Doxa-zosin for the treatment of benign prostatic hyperplasia in patients with mild to mod-erate essential hypertension: A double-blind, placebo-controlled, dose-response mul-ticenter study. J Urol. 1995;154:110-115
181.Ishizuka O, Nishizawa O, Hirao Y, Ohshima S. Evidence-based meta-analysis ofpharmacotherapy for benign prostatic hypertrophy. Int J Urol. 2002;9:607-612
182.Djavan B, Marberger M. A meta-analysis on the efficacy and tolerability ofalpha1-adrenoceptor antagonists in patients with lower urinary tract symptomssuggestive of benign prostatic obstruction. Eur Urol. 1999;36:1-13
183.Norman RW, Coakes KE, Wright AS, et al. Androgen metabolism in men receiv-ing finasteride before prostatectomy. J Urol. 1993;150:1736-1739
184.Russell DW, Wilson JD. Steroid 5 alpha-reductase: Two genes/two enzymes.Annu rev Biochem. 1994;63:25-61
185.Thigpen AE, Silver RI, Guileyardo JM, et al. Tissue distribution and ontogeny ofsteroid 5 alpha-reductase isoenzyme expression. J Clin Invest. 1993;92:903-910
186.Aumuller G, Eicheler W, Renneberg H, et al. Immunocytochemical evidence fordifferential subcellular localization of 5 alpha-reductase isoenzymes in human tis-sues. Acta Anat. 1996;156:241-252
187.Coptcoat MJ. The management of advanced prostate cancer, 1st edition. OxfordUK: Blackwell Science Ltd; 1996.
188.Dolder CR. Dutasteride: A dual 5-alpha reductase inhibitor for the treatment ofsymptomatic benign prostatic hyperplasia. Ann Pharmacother. 2006;40:658-665
189.Zimmern P. Medical treatment modalities for lower urinary tract symptoms:What are the relevant differences in randomised controlled trials? Eur Urol. 2000;38Suppl 1:18-24
190.Roehrborn CG. Meta-analysis of randomized clinical trials of finasteride. Urol-ogy. 1998;51:46-49
191.Stoner E, and the Finasteride Study Group. Three-year safety and efficacy dataon the use of finasteride in the treatment of benign prostatic hyperplasia. Urology.1994; 43:284-294.
192.Strauch G, Perles P, Vergult G. Comparison of finasteride (proscar) and serenoarepens (permixon) in the inhibition of 5-alpha reductase in healthy male volunteers.Eur Urol. 1994;26:247-252
193.Marks LS, Roehrborn CG, Wolford E, Wilson TH. The effect of dutasteride on theperipheral and transition zones of the prostate and the value of the transition zoneindex in predicting treatment response. J Urol. 2007;177:1408-1413
194.Boyle P, Roehrborn C, Harkaway R, Logie J, De La Rosette J, Emberton M. 5-alpha reductase inhibitors provide superior benefits to alpha blockers by preventingaur and surgery (abstract). J Urol. 2003;169 (Suppl 4):479
195.Kaplan SA. 5alpha-reductase inhibitors: What role should they play? Urology.2001;58:65-70; discussion 70
196.Thompson IM, Goodman PJ, Tangen CM, Lucia MS, Miller GJ, Ford LG, LieberMM, Cespedes RD, Atkins JN, Lippman SM, Carlin SM, Ryan A, Szczepanek CM,Crowley JJ, Coltman CA, Jr. The influence of finasteride on the development ofprostate cancer. N Engl J Med. 2003
197.Akdunian B, Crawford E.D. The pcpt: New findings, new insights, and clinicalimplications for the prevention of prostate cancer. European Urology Supplements.2006;5:634-639
198.Albertsen PC, Pellissier JM, Lowe FC, Girman CJ, Roehrborn CG. Economic anal-ysis of finasteride: A model-based approach using data from the proscar long-termefficacy and safety study. Clin Ther. 1999;21:1006-1024
55
Chapter 9. Benign Prostate Disorders
199.Sarma AV, Jacobson DJ, McGree ME, Roberts RO, Lieber MM, Jacobsen SJ. Apopulation based study of incidence and treatment of benign prostatic hyperplasiaamong residents of olmsted county, minnesota: 1987 to 1997. J Urol. 2005;173:2048-2053
200.Kaplan SA, Roehrborn CG, McConnell JD, Kreder KJ, Lieber ML, Jacobs SC,Slawin KM, Bautista OM, Burrows PK, Nyberg LM, Kusek JW. Baseline symptoms,uroflow, and post-void residual urine as predictors of bph clinical progression in themedically treated arms of the mtops trial (abstract). J Urol. 2003;169 (Suppl 4):332h
201.McConnell JD, Roehrborn CG, Slawin KM, Lieber MM, Smith JA, Kaplan SA,Bautista O, Burrows PK, Nyberg LM, Kusek JW. Baseline measures predict the riskof benign prostatic hyperplasia clinicalprogression in placebo-treated patients (ab-stract). J Urol. 2003;169 (Suppl 4):332
202.Kaplan S, Garvin D, Gilhooly P, Koppel M, Labasky R, Milsten R, Reddy P, Rosen-berg S, Sussman D, White C, Lee M, Pappas F, Waldstreicher J. Impact of baselinesymptom severity on future risk of benign prostatic hyperplasia-related outcomesand long-term response to finasteride. The pless study group. Urology. 2000;56:610-616
203.Hutchison A, Farmer R, Verhamme K, Berges R, Navarrete RV. The efficacy ofdrugs for the treatment of luts/bph, a study in 6 european countries. Eur Urol. 2006
204.Han M, Alfert H, J.„ Partin AW. Retropubic and suprapubic open prostatectomy.In: Walsh PC, ed. Campbell’s urology. Philadelphia: Saunders; 2002:1423-1434.
205.Lu-Yao GL, Barry MJ, Chang CH, et al. Transurethral resection of the prostateamong medicare beneficiaries in the united states: Time trends and outcomes.Prostate patient outcomes research team (port). Urology. 1994;44:692-696
206.Blute M, Ackerman SJ, Rein AL, Beusterien K, Sullivan EM, Tanio CP, Strauss MJ,Manyak MJ. Cost effectiveness of microwave thermotherapy in patients with benignprostatic hyperplasia: Part ii--results. Urology. 2000;56:981-987
207.Wasson JH, Reda DJ, Bruskewitz RC, Elinson J, Keller AM, Henderson WG. Acomparison of transurethral surgery with watchful waiting for moderate symptomsof benign prostatic hyperplasia. The veterans affairs cooperative study group ontransurethral resection of the prostate. N Engl J Med. 1995;332:75-79
208.Ogiste JS, Cooper K, Kaplan SA. Are stents still a useful therapy for benign pro-static hyperplasia? Curr Opin Urol. 2003;13:51-57
209.Fitzpatrick JM, Mebust WK. Minimally invasive and endoscopic managementof benign prostatic hyperplasia. In: Walsh PC, ed. Campbell’s urology. Philadelphia:Saunders; 2002:1379-1422.
210.Parsons CI. Impotence following transurethral resection of the prostate. In: RaiferJ, ed. Common problems in infertility and impotence. Chicago: Year Book Medical;1990.
211.Jepsen J, Bruskewitz R. Recent developments in the surgical management of be-nign prostatic hyperplasia. Urology. 1998;51(Suppl. 4A):23-31.
212.Serretta V, Morgia G, Fondacaro L, Curto G, Lo bianco A, Pirritano D, Melloni D,Orestano F, Motta M, Pavone-Macaluso M. Open prostatectomy for benign prostaticenlargement in southern europe in the late 1990s: A contemporary series of 1800 in-terventions. Urology. 2002;60:623-627
213.Gacci M, Bartoletti R, Figlioli S, Sarti E, Eisner B, Boddi V, Rizzo M. Urinary symp-toms, quality of life and sexual function in patients with benign prostatic hypertro-phy before and after prostatectomy: A prospective study. BJU Int. 2003;91:196-200
214.Tubaro A, Vicentini C, Renzetti R, Miano L. Invasive and minimally invasivetreatment modalities for lower urinary tract symptoms: What are the relevant dif-ferences in randomised controlled trials? Eur Urol. 2000;38 Suppl 1:7-17
56
Chapter 9. Benign Prostate Disorders
215.Aho TF, Gilling PJ. Laser therapy for benign prostatic hyperplasia: A review ofrecent developments. Current Opinion in Urology. 2003;1:39-44.
216.AUA Practice Guidelines Committee. The american urological association 2003guideline on management of benign prostatic hyperplasia (2003). Chapter 1: Diagno-sis and treatment recommendations. J Urol. 2003;170:530-547
217.Elzayat EA, Elhilali MM. Laser treatment of symptomatic benign prostatic hyper-plasia. World J Urol. 2006;24:410-417
218.Kim SC, Matlaga BR, Kuo RL, Watkins SL, Kennett KM, Gilling PJ, Lingeman JE.Holmium laser enucleation of the prostate: A comparison of efficiency measures attwo institutions. J Endourol. 2005;19:555-558
219.Malek R, Nahen K. Photoselective vaporisation of the prostate: Ktp laser therapyof obstructive benign prostatic hyperplasia. AUA Update Series. 2004;23:154-159
220.Bouchier-Hayes DM, Anderson P, Van Appledorn S, Bugeja P, Costello AJ. Ktplaser versus transurethral resection: Early results of a randomized trial. J Endourol.2006;20:580-585
221.Gilling P, Cass C, Cresswell M, et al. The use of the holmium laser in the treatmentof bph. J Endourol. 1996;10:459-461
222.Hoffman RM, MacDonald R, Slaton JW, Wilt TJ. Laser prostatectomy versustransurethral resection for treating benign prostatic obstruction: A systematicreview. J Urol. 2003;169:210-215
223.Gilling PJ, Mackey M, Cresswell M, Kennett K, Kabalin JN, Fraundorfer MR.Holmium laser versus transurethral resection of the prostate: A randomized prospec-tive trial with 1-year followup. J Urol. 1999;162:1640-1644
224.Hurle R, Vavassori I, Piccinelli A, Manzetti A, Valenti S, A. V. Holmium laserenucleation of the prostate combined with mechanical morcellation in 155 patientswith benign prostatic hyperplasia. Urology. 2002;60:449-453
225.Costello A, Bowsker W, Bolton G, et al. Laser ablation of prostate in patients withbenign prostatic hyperplasia. Br J Urol. 1992;69:603-608
226.Chacko K, Donovan J, Abrams P, et al. Turp or laser therapy for men with acuteurinary retention: The clasp randomised trial. J Urol. 2001;166:166-171
227.Kuntz RM. Laser treatment of benign prostatic hyperplasia. World J Urol.2007;25:241-247
228.Naspro R, Salonia A, Cestari A, Guazzoni G, Suardi N, Colombo R, Rigatti P,Montorsi F. A critical analysis of laser prostatectomy in the management of benignprostatic hyperplasia. BJU Int. 2005;96:736-739
229.Bostwick DG, Larson TR. Transurethral microwave thermal therapy: Pathologicfindings in the canine prostate. Prostate. 1995;26:116-122.
230.Thalmann G N, Mattei A, Treuthardt C, Burkhard FC, Studer UE. Transurethralmicrowave therapy in 200 patients with a minimum followup of 2 years: Urodynamicand clinical results. J Urol. 2002;167:2496-2501
231.Klingler HC. New innovative therapies for benign prostatic hyperplasia: Anyadvance? Curr Opin Urol. 2003;13:11-15
232.Floratos DL, Kiemeney LA, Rossi C, Kortmann BB, Debruyne FM, de La RosetteJJ. Long-term followup of randomized transurethral microwave thermotherapy ver-sus transurethral prostatic resection study. J Urol. 2001;165:1533-1538
233.Ramsey EW, Dahlstrand C. Durability of results obtained with transurethral mi-crowave thermotherapy in the treatment of men with symptomatic benign prostatichyperplasia. J Endourol. 2000;14:671-675
234.McAllister WJ, Karim O, Plail RO, Samra DR, Steggall MJ, Yang Q, Fowler CG.Transurethral electrovaporization of the prostate: Is it any better than conventionaltransurethral resection of the prostate? BJU Int. 2003;91:211-214
57

Chapter 9. Benign Prostate Disorders
235.Traxer O, Anidjar M, Gaudez F, Saporta F, Daudon M, Cortesse A, Desgrand-champs F, Cussenot O, Teillac P, Le Duc A. A new prostatic stent for the treatment ofbenign prostatic hyperplasia in high-risk patients. Eur Urol. 2000;38:272-278
236.Gajewski JB, Chancellor MB, Ackman CF, Appell RA, Bennett J, Binard J, BooneTB, Chetner MP, Crewalk JA, Defalco A, Foote J, Green B, Juma S, Jung SY, Lin-senmeyer TA, Macaluso JN, Jr., Macmillan R, Mayo M, Ozawa H, Roehrborn CG,Schmidt J, Shenot PJ, Stone A, Vazquez A, Killorin W, Rivas DA. Removal of urolumeendoprosthesis: Experience of the north american study group for detrusor-sphincterdyssynergia application. J Urol. 2000;163:773-776
237.Smith CP, Somogyi GT, Boone TB. Botulinum toxin in urology: Evaluation usingan evidence-based medicine approach. Nat Clin Pract Urol. 2004;1:31-37
238.Patel AK, Chapple CR. Botulinum toxin injection therapy in the management oflower urinary tract dysfunction. Int J Clin Pract Suppl. 2006:1-7
239.Kuo HC. Prostate botulinum a toxin injection--an alternative treatment for benignprostatic obstruction in poor surgical candidates. Urology. 2005;65:670-674
240.Chuang YC, Chiang PH, Yoshimura N, De Miguel F, Chancellor MB. Sustainedbeneficial effects of intraprostatic botulinum toxin type a on lower urinary tractsymptoms and quality of life in men with benign prostatic hyperplasia. BJU Int.2006;98:1033-1037; discussion 1337
241.Chuang YC, Tu CH, Huang CC, Lin HJ, Chiang PH, Yoshimura N, ChancellorMB. Intraprostatic injection of botulinum toxin type-a relieves bladder outlet obstruc-tion in human and induces prostate apoptosis in dogs. BMC Urol. 2006;6:12
242.Smith CP, Franks ME, McNeil BK, Ghosh R, de Groat WC, Chancellor MB, Somo-gyi GT. Effect of botulinum toxin a on the autonomic nervous system of the rat lowerurinary tract. J Urol. 2003;169:1896-1900
243.Doggweiler R, Zermann DH, Ishigooka M, Schmidt RA. Botox-induced prostaticinvolution. Prostate. 1998;37:44-50
244.Antunes AA, Srougi M, Coelho RF, de Campos Freire G. Botulinum toxin for thetreatment of lower urinary tract symptoms due to benign prostatic hyperplasia. NatClin Pract Urol. 2007;4:155-160
245.Speakman M. Lower urinary tract symptoms suggestive of benign prostatic ob-struction: What is the available evidence for rational management? Eur Urol. 2001;39(Suppl 3):6-12
58