Embed Size (px)
Citation preview
P.O. Box 2925 Riyadh – 11461KSATel: +966 1 2520088 ext 40151Fax: +966 1 2520718
CA
SE R
EPO
RT
Received 20 October 2012; revised 9 December 2012; accepted 28December 2012.Available online 8 January 2013
⇑ Corresponding author. Address: Department of Cardiology, NationalInstitute of Cardiovascular Diseases, Dhaka 1207, Bangladesh. Mobile:+880 1712564487.
E-mail address: [email protected] (A.K.M.M. Islam).Chiari network: A case report andbrief overview
Email: [email protected]: www.sha.org.sa
1016–7315 � 2013 King Saud University.
Production and hosting by Elsevier B.V. All rights reserved.
Peer review under responsibility of King Saud University.
URL: www.ksu.edu.sa
http://dx.doi.org/10.1016/j.jsha.2012.12.002Production and hosting by Elsevier
A.K.M. Monwarul Islam a,⇑, Lima Asrin Sayami a, Shahana Zaman a
a Department of Cardiology, National Institute of Cardiovascular Diseases, Dhaka
a Bangladesh
The Chiari network is mobile, net-like structures occasionally seen in right atrium near the opening of inferior venacava and coronary sinus. This is usually of no clinical significance and is often diagnosed incidentally. However,sometimes it may cause diagnostic confusion with right atrial pathologies, and may favour thromboembolism bycausing flow obstruction. It may be associated with infective endocarditis, arrhythmias, and migraine. Sometimes, itacts as a physical barrier during invasive procedures. The Chiari network has also been described to protect frompulmonary embolism by acting as an inferior vena cava filter due to its sieve-like effect at the cavo-atrial junction. Here,the Chiari network has been described in a case of Ebstein anomaly of tricuspid valve which produced diagnosticconfusion during echocardiography. A brief overview has also been presented.
� 2013 King Saud University. Production and hosting by Elsevier B.V. All rights reserved.
Keywords: Coronary sinus, Inferior vena cava, Ebstein anomaly
Introduction
The Chiari network, encountered infrequently inthe right atrium, is a fenestrated, net-like
embryonic remnants of valves of sinus venosus, ly-ing closely in relation to the inferior vena cava andcoronary sinus, sometimes connecting these withother right atrial structures [1]. It is usually of noclinical significance. However, it may at times pro-duce diagnostic confusion, cause thromboembo-lism, infective endocarditis, arrhythmias, or causephysical barrier to invasive procedures [1]. Here,the Chiari network has been described in a case ofEbstein anomaly of tricuspid valve which produceddiagnostic confusion during echocardiography.
Case presentation
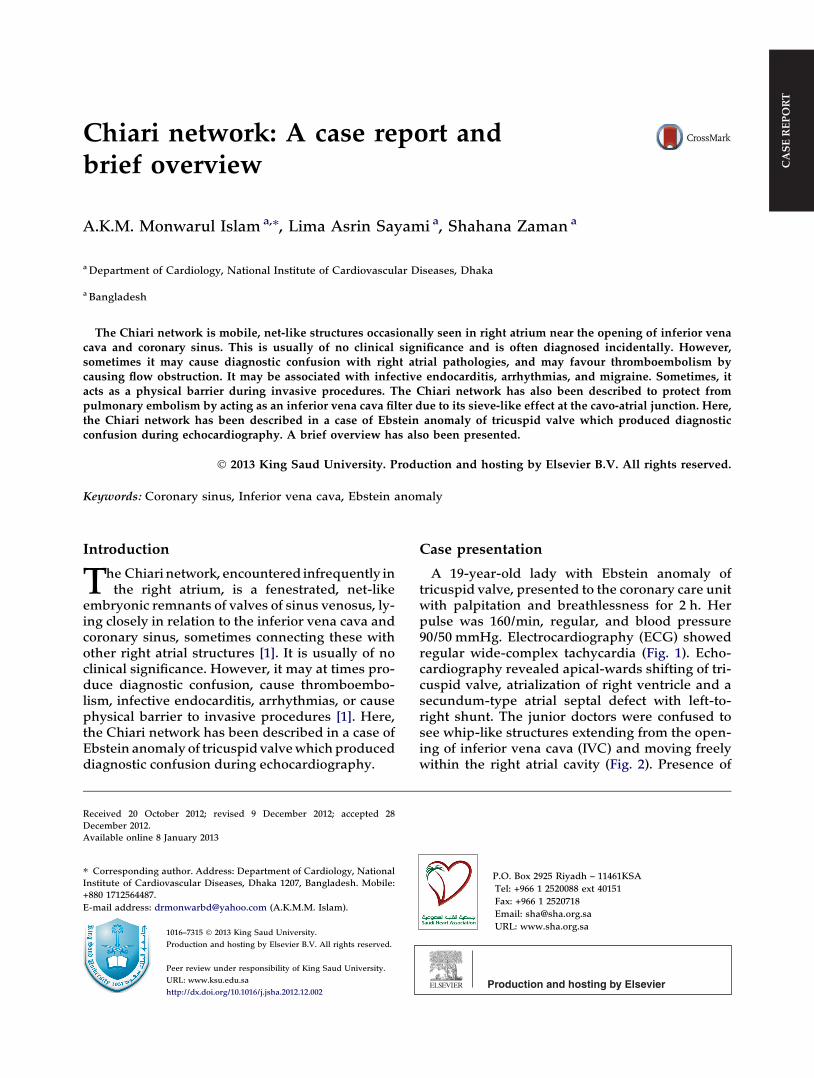
A 19-year-old lady with Ebstein anomaly oftricuspid valve, presented to the coronary care unitwith palpitation and breathlessness for 2 h. Herpulse was 160/min, regular, and blood pressure90/50 mmHg. Electrocardiography (ECG) showedregular wide-complex tachycardia (Fig. 1). Echo-cardiography revealed apical-wards shifting of tri-cuspid valve, atrialization of right ventricle and asecundum-type atrial septal defect with left-to-right shunt. The junior doctors were confused tosee whip-like structures extending from the open-ing of inferior vena cava (IVC) and moving freelywithin the right atrial cavity (Fig. 2). Presence of
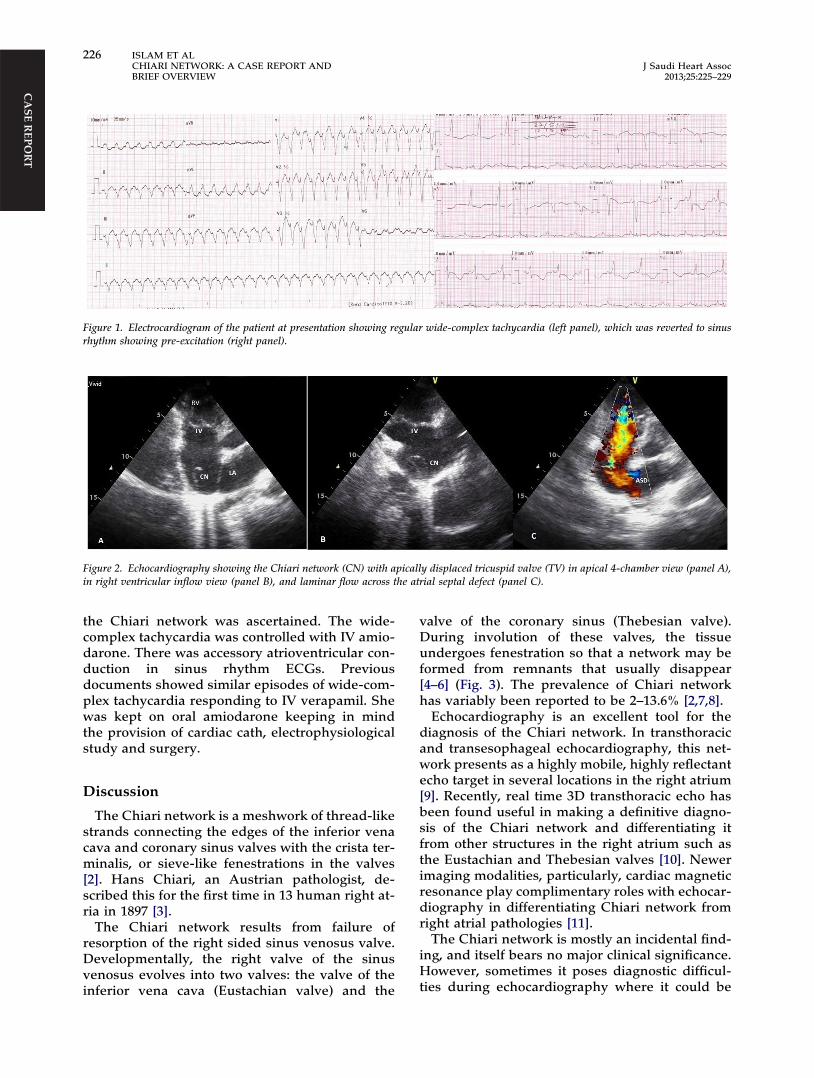
Figure 2. Echocardiography showing the Chiari network (CN) with apically displaced tricuspid valve (TV) in apical 4-chamber view (panel A),in right ventricular inflow view (panel B), and laminar flow across the atrial septal defect (panel C).
Figure 1. Electrocardiogram of the patient at presentation showing regular wide-complex tachycardia (left panel), which was reverted to sinusrhythm showing pre-excitation (right panel).
CA
SE REPO
RT
226 ISLAM ET ALCHIARI NETWORK: A CASE REPORT ANDBRIEF OVERVIEW
J Saudi Heart Assoc2013;25:225–229
the Chiari network was ascertained. The wide-complex tachycardia was controlled with IV amio-darone. There was accessory atrioventricular con-duction in sinus rhythm ECGs. Previousdocuments showed similar episodes of wide-com-plex tachycardia responding to IV verapamil. Shewas kept on oral amiodarone keeping in mindthe provision of cardiac cath, electrophysiologicalstudy and surgery.
Discussion
The Chiari network is a meshwork of thread-likestrands connecting the edges of the inferior venacava and coronary sinus valves with the crista ter-minalis, or sieve-like fenestrations in the valves[2]. Hans Chiari, an Austrian pathologist, de-scribed this for the first time in 13 human right at-ria in 1897 [3].
The Chiari network results from failure ofresorption of the right sided sinus venosus valve.Developmentally, the right valve of the sinusvenosus evolves into two valves: the valve of theinferior vena cava (Eustachian valve) and the
valve of the coronary sinus (Thebesian valve).During involution of these valves, the tissueundergoes fenestration so that a network may beformed from remnants that usually disappear[4–6] (Fig. 3). The prevalence of Chiari networkhas variably been reported to be 2–13.6% [2,7,8].
Echocardiography is an excellent tool for thediagnosis of the Chiari network. In transthoracicand transesophageal echocardiography, this net-work presents as a highly mobile, highly reflectantecho target in several locations in the right atrium[9]. Recently, real time 3D transthoracic echo hasbeen found useful in making a definitive diagno-sis of the Chiari network and differentiating itfrom other structures in the right atrium such asthe Eustachian and Thebesian valves [10]. Newerimaging modalities, particularly, cardiac magneticresonance play complimentary roles with echocar-diography in differentiating Chiari network fromright atrial pathologies [11].
The Chiari network is mostly an incidental find-ing, and itself bears no major clinical significance.However, sometimes it poses diagnostic difficul-ties during echocardiography where it could be
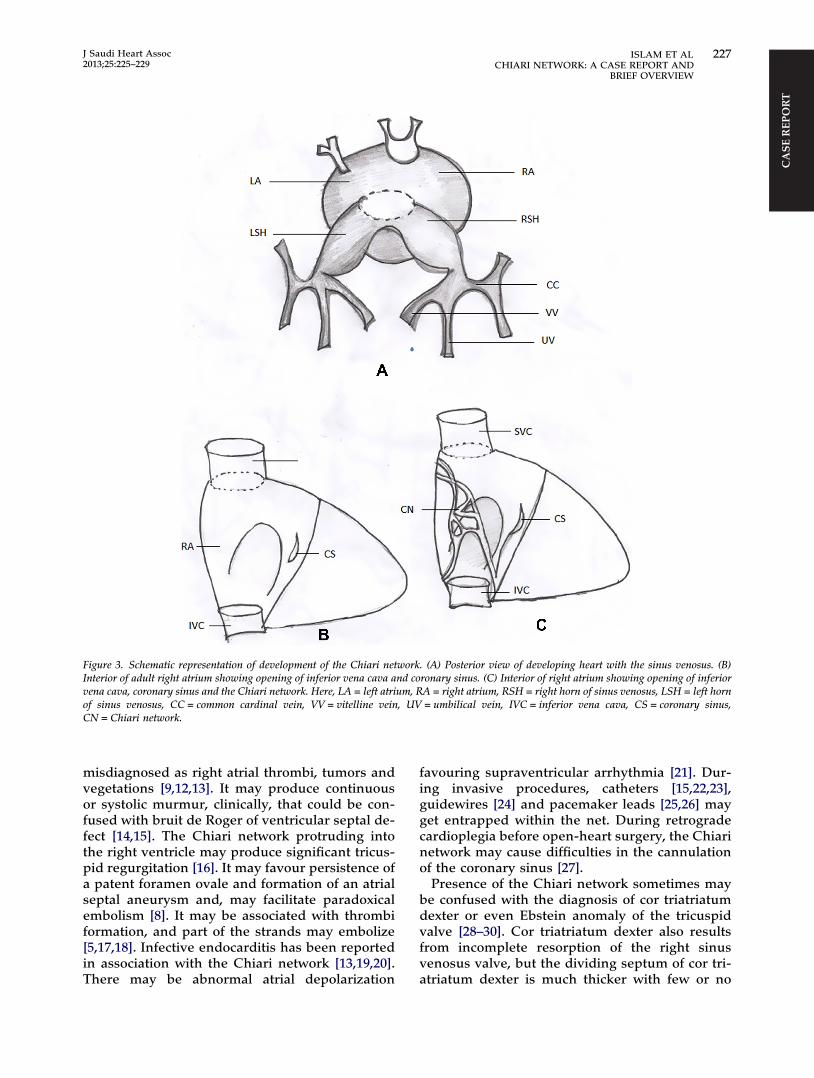
Figure 3. Schematic representation of development of the Chiari network. (A) Posterior view of developing heart with the sinus venosus. (B)Interior of adult right atrium showing opening of inferior vena cava and coronary sinus. (C) Interior of right atrium showing opening of inferiorvena cava, coronary sinus and the Chiari network. Here, LA = left atrium, RA = right atrium, RSH = right horn of sinus venosus, LSH = left hornof sinus venosus, CC = common cardinal vein, VV = vitelline vein, UV = umbilical vein, IVC = inferior vena cava, CS = coronary sinus,CN = Chiari network.
CA
SE R
EPO
RT
J Saudi Heart Assoc2013;25:225–229
ISLAM ET AL 227CHIARI NETWORK: A CASE REPORT AND
BRIEF OVERVIEW
misdiagnosed as right atrial thrombi, tumors andvegetations [9,12,13]. It may produce continuousor systolic murmur, clinically, that could be con-fused with bruit de Roger of ventricular septal de-fect [14,15]. The Chiari network protruding intothe right ventricle may produce significant tricus-pid regurgitation [16]. It may favour persistence ofa patent foramen ovale and formation of an atrialseptal aneurysm and, may facilitate paradoxicalembolism [8]. It may be associated with thrombiformation, and part of the strands may embolize[5,17,18]. Infective endocarditis has been reportedin association with the Chiari network [13,19,20].There may be abnormal atrial depolarization
favouring supraventricular arrhythmia [21]. Dur-ing invasive procedures, catheters [15,22,23],guidewires [24] and pacemaker leads [25,26] mayget entrapped within the net. During retrogradecardioplegia before open-heart surgery, the Chiarinetwork may cause difficulties in the cannulationof the coronary sinus [27].
Presence of the Chiari network sometimes maybe confused with the diagnosis of cor triatriatumdexter or even Ebstein anomaly of the tricuspidvalve [28–30]. Cor triatriatum dexter also resultsfrom incomplete resorption of the right sinusvenosus valve, but the dividing septum of cor tri-atriatum dexter is much thicker with few or no

CA
SE REPO
RT
228 ISLAM ET ALCHIARI NETWORK: A CASE REPORT ANDBRIEF OVERVIEW
J Saudi Heart Assoc2013;25:225–229
fenestrations. Unlike the Chiari network, it maycause obstruction to blood flow and is usuallyassociated with other congenital abnormalitiessuch as atrial septal defect and tricuspid atresia[28–30].
Interestingly, the Chiari network has been de-scribed to play a protective role in special situa-tions, such as an inferior vena cava filter inpatients with thrombophilia [31], and holdingthrombus in the network preventing embolization[32,33]. This network has also been described inassociation with neurofibromatosis [34], Behçetsyndrome [35], platypnea–orthodeoxia [36] andmigraine [37].
In the case presented here, the Chiari networkin probably an incidental finding. However, itspresence might facilitate the occurrence of acces-sory pathway of atrioventricular conductionresulting in Wolf–Parkinson–White syndrome;otherwise, the accessory pathway might be awell-recognized association of Ebstein anomalyof tricuspid valve.
Conclusion
The Chiari network is an uncommon diagnosis.It has to be recognized appropriately, otherwiseit may lead to misdiagnosis. This apparently ‘nor-mal variant’ may not be always so. Respective cli-nicians should keep its presence in mind whiledoing echocardiography to avoid diagnostic di-lemma, while performing cardiovascular interven-tions to overcome difficulties, and while dealingwith patients to make the appropriate diagnosis.
Conflict of Interest
Authors have no conflict of interest to declare.
References
[1] Loukas M, Sullivan A, Tubbs RS, Weinhaus AJ, DerDerianT, Hanna M. Chiari’s network: review of the literature.Surg Radiol Anat 2010;32(10):895–901.
[2] Bhatnagar KP, Nettleton GS, Campbell FR, Wagner CE,Kuwabara N, Muresian H. Chiari anomalies in the humanright atrium. Clin Anat 2006;19:510–6.
[3] Chiari H. Ueber Netzbildungen im rechten VorhofedesHerzens. Beitr Pathol Anat 1897;22:1–10.
[4] Gresham GA. Networks in the right side of the heart. BrHeart J 1957;19:381–6.
[5] Yater WM. Variations and anomalies of the venous valvesof the right atrium of the human heart. Arch Pathol1929;7:418–41.
[6] Powell EDV, Mullaney JM. The Chiari network and thevalve of the inferior vena cava. Br Heart J 1960;22:570–84.
[7] Yater WM. The paradox of Chiari’s network. Review andreport of a case of Chiari’s network ensnaring a largeembolus. Am Heart J 1936;11:542–52.
[8] Schneider B, Hofmann T, Justen MH, et al.. Chiari’snetwork: normal anatomic variant or risk factor forarterial embolic events. J Am Coll Cardiol 1995;26:203–10.
[9] Werner JA, Cheitlin MD, Gross BW, et al..Echocardiographic appearance of the Chiari network:differentiation from right heart pathology. Circulation1981;5:1104–9.
[10] Pothineni KP, Nanda NC, Burri MV, Singh A, Panwar SR,Gandhari S. Live/real time three-dimensionaltransthoracic echocardiographic visualization of Chiarinetwork. Echocardiography 2007;24(9):995–7.
[11] Altbach MI, Squire SW, Kudithipudi V, Castellano L,Sorrell VL. Cardiac MRI is complementary toechocardiography in the assessment of cardiac masses.Echocardiography 2007;24(3):286–300.
[12] Wiegers S, Plappert T, Sutton MSJ. Echocardiography inpractice, a case oriented approach. [cited 2012 Oct 15].Available from: <http://www.echo-web.com/asp/CaseStudiyChiari.asp>.
[13] Payne DM, Baskett RJF, Hirsch GM. Infectiousendocarditis of a Chiari network. Ann Thorac Surg2003;76:1303–5.
[14] Friedberg CK. Diseases of the heart. 3rded. Philadelphia: Saunders; 1966. p. 1298.
[15] Goldschlager A, Goldschlager N, Brewster H, Kaplan J.Catheter entrapment in a Chiari network involving anatrial septal defect. Chest 1972;62:345–6.
[16] Jen-Ping Chang JP. Tricuspid regurgitation as a result ofChiari network attachment. J Thorac Cardiovasc Surg2012;143:235.
[17] Yater WM. The paradox of Chiari’s network. Am Heart J1936;1936(11):542–53.
[18] Powell EDU, Mullaney JM. The Chiari network and thevalve of the inferior vena cava. Br Heart J 1960;22:579–84.
[19] Mousavi N, Bhagirath K, Ariyarajah V, Fang T, Ahmadie R,Lytwyn M, et al.. Chiari network endocarditis: not just aninnocent bystander. Echocardiography 2008;25(6):642–5.
[20] Lejko-Zupanc T, Kozelj M, Pikelj F. Right sidedendocarditis: clinical and echocardiographiccharacteristics. J Clin Basic Cardiol 1999;2:81–4.
[21] Prajapat L, Ariyarajah V, Spodick DH. Abnormal atrialdepolarization associated with Chiari network? Cardiology2007;108(3):214–6.
[22] Cooke JC, Gelman JS, Harper RW. Chiari networkentanglement and herniation into the left atrium by anatrial septal defect occluder device. J Am Soc Echocardiogr1999;12:601–3.
[23] Aydın A, Gürol T, Yılmazer MS, Dagdeviren B. Catheterentrapment around the Chiari network duringpercutaneous atrial septal defect closure. [cited 2012 Oct15]. Anadolu Kardiyoloji Dergisi. doi: http://dx.doi.org/10.5152/akd.2011.047.
[24] Shimoike E, Ueda N, Maruyama T, Kaji Y, Niho Y.Entrapment of a guide wire by the Chiari network in apatient with ablated idiopathic ventricular tachycardia. JInterv Card Electrophysiol 2001;5(2):219–22.
[25] Dissmann R, Schröder J, Völler H, Behrens S. Entrapmentof pacemaker lead by a large netlike Eustachian valvewithin the right atrium. Clin Res Cardiol 2006;95(4):241–3.
[26] Maruyama T, Kurogouchi F. Entrapment of a tined lead bythe chiari network with preserved atrial sensing ability in apatient with atrioventricular block: a case report. J Cardiol2004;44(6):251–4.
[27] Teo EYL, Ittleman F, Hamlin MP. A Chiari network anddifficult cannulation of the coronary sinus for retrogradeperfusion. Anesth Analg 2010;111(1):79–81.
[28] Hansing CE, Young WP, Rowe GG. Cor triatriatum dexter.Am J Cardiol 1972;30:559–64.
[29] Lanzarini L, Lucca E. Persistence of the right valve of thesinus venosus resulting in an unusually prominent Chiarinetwork remnant mimicking cor triatriatum dexter.Pediatr Cardiol 2002;23:103–5.
[30] Salama S, Gallachera D, Uzuna O. Cor triatriatum dextermasquerading as Ebstein’s anomaly. Cardiol Young2011;21:354–6.
[31] Obaji SG, Cooper R, Somauroo J. Chiari network: aprotective filter against pulmonary embolism in a case of

CA
SE R
EPO
RT
J Saudi Heart Assoc2013;25:225–229
ISLAM ET AL 229CHIARI NETWORK: A CASE REPORT AND
BRIEF OVERVIEW
polycythaemia. BMJ Case Rep 2012. http://dx.doi.org/10.1136/bcr.05.2011.4289.
[32] Motovska Z, Widimsky P, Bilkova D, Penicka M,Linkova H, Kautznerova D, et al.. An embolus in theright atrium caught in the Chiari network and resistantto thrombolysis. J Thromb Thrombolysis 2010;30(1):114–8.
[33] Goedde TA, Conetta D, Rumisek JD. Chiari networkentrapment of thromboemboli: congenital inferior venacava filter. Ann Thorac Surg 1990;49(2):317–8.
[34] Koz C, Yokusoglu M, Baysan O, Uzun M. Giant Chiarinetwork mimics intracardiac tumor in a case ofneurofibromatosis. Int J Cardiol 2008;130(3):488–9.
[35] Alonso G, Santos E, Fuertes A, Jiménez A, Gutiérrez JA.Behçet’s disease and Chiari’s network. Clin Rheumatol2007;26(12):2189–90.
[36] Shakur R, Ryding A, Timperley J, Becher H, Leeson P. Lateemergence of platypnea orthodeoxia: Chiari network andatrial septal hypertrophy demonstrated withtransoesophageal echocardiography. Eur J Echocardiogr2008;9(5):694–6.
[37] Rigatelli G, Dell’avvocata F, Cardaioli P, Giordan M,Braggion G, Aggio S, et al.. Migraine-patent foramenovale connection: role of prominent eustachian valve andlarge Chiari network in migrainous patients. Am J Med Sci2008;336(6):458–61.






![Rx161 Arnold-Chiari Malformationfinalcopy0048502.netsolhost.com/.../pdfs/RXforms/Arnold_Chiari_Malformation.pdfArnold-Chiari malformation [Chiari malformation (CM)] is a congenital](https://img.pdfslide.net/doc/110x75/5ab9a8f17f8b9ac60e8e5491/rx161-arnold-chiari-malforma-malformation-chiari-malformation-cm-is-a-congenital.jpg)






















