Embed Size (px)
Citation preview
850
Thorpe, who was chairman of the Section of GeneralPractice of the American Medical Association last year, reada paper on obesity at the 100th annual meeting of the A.M.A." The simplest to prepare and most easily obtainable high-protein, high-fat, low-carbohydrate diet " he said " and onethat will produce the most rapid loss of weight without hunger,weakness, lethargy, or constipation, is made up of meat, fat,and water. The total quantity eaten need not be noted."
This evidence and the evidence of history is veryconvincing, but what is needed to clinch the matter nowis a long-term prospective study of obese people treatedon these lines. This is a subject which might well engagethe attention of the College of General Practitioners.
RICHARD MACKARNESS.
1. Lancet, 1958, i, 1162.2. Pomeranze, J., Gadek, R. J. New Engl. J. Med. 1957, 257, 73.3. Rummel, W., Candon, B. H. Int. Rec. Med. 1956, 12, 783.4. Feldman, H. S., Rummel, W. Med. Times, 1956, 84, 1329.5. Dwyer, T. A. Clin. Med. 1957, 4, 457.6. Clancy, J. B., Aldrich, R. H., Rummel, W., Candon, B. H. Amer. Pract.
Digest Treat. 1957, 8, 1948.7. O’Brien, T. E., Onorato, R. R., Dwyer, T. A., Candon, B. H. West. J.
Surg. 1957, 65, 29.8. Wagner, H. Landarzt, 1955, 31, 496.9. Jorgensen, G. Arztl. Wschr. 1955, 10, 92.
10. Johnson, H. D. Lancet, 1957, ii, 518.11. Johnson, H. D. ibid. 1955, i, 266.12. Johnson, H. D. Surg. Gynec. Obstet. 1956, 102, 287.
IRON DEFICIENCY IN MAN
JULIUS POMERANZE.
SIR, Your leading article 1 on this subject was
extremely interesting and instructive. It is certain that a
large group of patients in need of intensive iron therapyare intolerant to the usual available preparations. In fact,the changes of the gastrointestinal mucosa in iron-
deficiency anxmia make it less -tolerant than during arepleted state. The new oral chelated-iron compoundsrepresent a distinct advance in the treatment of this verycommon condition.
I was somewhat disappointed that no mention was made ofthe most widely explored iron chelate/ferroglycine sulphatecomplex. Our own clinical experience was indicated in a recentpubltcation: " The therapeutic and performance indexes offerroglycine sulphate complex (’ Ferronord ’) are optimal inthe treatment of iron-deficiency anoemia."2 It was quite evidentthat this new oral iron chelate provided the best therapeuticresults with the least evidence of side-effects. This was
expressed as a therapeutic index which is a useful measurementof the value of any drug.Our results have been reproduced by a large group of investi-
gators. A long bibliography 3-9 attests to the unanimity con-cerning the therapeutic index of the oral iron chelate/ferro-sivcine sulphate complex.
COMBINED GASTRIC AND DUODENAL ULCER
H. DAINTREE JOHNSON.Royal Free Hospital,London, W.C.1.
SIR,-I am happy to read Dr. Billington’s analysis(Oct. 4) confirming the fact I recorded in your pages lastyear 10-that combined-ulcer patients genetically resemblesubjects with duodenal ulcers alone rather than those withgastric ulcers alone.
In earlier papers 11 12 I showed why this should be so, for ananalysis of 135 combined-ulcer cases demonstrated that theduodenal ulcer was probably always there first, the gastriculcer appearing later, usually as a complication of duodenalor pyloric stenosis with gastric retention. Combined-ulcerpatients were also shown to have gastric secretion patternssimilar to those of duodenal-ulcer patients, and, of course,different from those of the gastric-ulcer subjects. Gastric ulcerscomplicating duodenal ones appear to be a special varietywhich should probably be dealt with separately from othergastric ulcers in statistical analysis.My figures have differed from those of Dr. Billington, how-
ever, in that they have suggested that prepyloric ulcers, which
I have regarded as a third type of gastric ulcer, have more incommon with duodenal ulcers than with " ordinary " ortype-I gastric ulcers.
Incidentally, the three kinds of gastric ulcer have quitedifferent prognoses and call for different methods of treatment.Combined ulcers have a particularly bad record of intract-ability and haemorrhage.
THE FRONTIERS OF MEDICINE
O. A. TROWELL.M.R.C. Radiobiological Unit,
Harwell.
.
SIR,-Professor Stuart-Harris (Aug. 30) said that whenhe was a student (1930) " it was common to feel thatpatients were admitted to the medical wards to lie androt ", and Dr. Marshall (Sept. 20) has "
very deeplyresented " this statement. As one who felt with theProfessor and who felt further that many patients wereadmitted solely for teaching purposes and the exerciseof the higher diagnostic skills, may I quote a few figuresin support of this view.
Here is an analysis, which I made when a student,of the treatment and outcome of 30 consecutive admissionsto two medical wards of a general hospital in 1932.
Treatment received was:
Only 2 cases showed any improvement as a result of the" special " treatment available only in hospital. This is avery small series, but I think it is a fair random sample ofconditions prevailing at that time. As regards impact onthe student mind, some of us were diverted to the lesslucrative but, as we felt, more honest pursuit of funda-mental research.
FLICKERING LARYNGOSCOPES
J. D. M. BARTON.
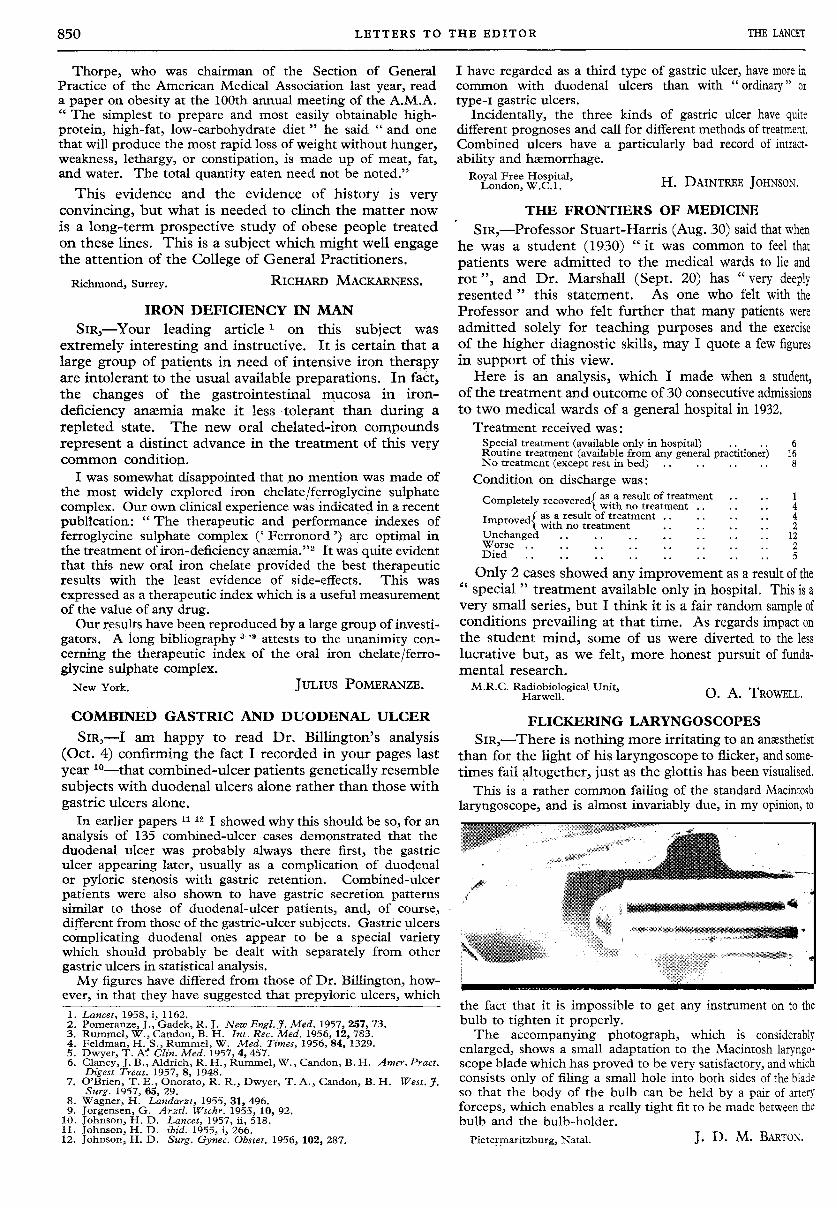
SIR,-There is nothing more irritating to an anxsthedstthan for the light of his laryngoscope to flicker, and some-times fail altogether, just as the glottis has been visualised.
This is a rather common failing of the standard Macintoshlaryngoscope, and is almost invariably due, in my opinion, to
the fact that it is impossible to get any instrument on to thebulb to tighten it properly.The accompanying photograph, which is considerably
enlarged, shows a small adaptation to the Macintosh laryngo-scope blade which has proved to be very satisfactory, and whichconsists only of filing a small hole into both sides of the bladeso that the body of the bulb can be held by a pair of arteryforceps, which enables a really tight fit to be made between thebulb and the bulb-holder.