Embed Size (px)
Citation preview
Clinical Study Protocol Egyptian Parkinson's Disease Study Group
1
Clinical Study Protocol
Determining the clinical profile of Parkinson’s disease among Egyptian
population; A National, Cross sectional, Collaborative Study
Egyptian Parkinson's Disease Study Group
EMRA student-led national research collaborative
Final protocol
Version no.1
Date of release 17/04/2017
Contact information
Website: www.emra-collaborative.org
FB group: https://www.facebook.com/groups/EMRA.Neuro1/
E-mail 1: [email protected]
E-mail 2: [email protected]
Tel 1: +20 1090032210
Tel 2: +20 1125549087

Clinical Study Protocol Egyptian Parkinson's Disease Study Group
2
Principal investigator Ahmed Negida Faculty of Medicine, Zagazig University Tel: +201125549087 Email: [email protected]
Co-Principal investigator Ahmed Elgebaly Faculty of Medicine, Al-Azhar University
Hussien Ahmed Faculty of Medicine, Zagazig University
Dr. Abdelrahman Ibrahim Abushouk, MBBCh Faculty of Medicine, Ain Shams University
Lead coordinators Mahmoud Atef Morsi Faculty of Medicine, Menoufia University Tel: +201090032210 Email: [email protected] Dr. Safwat Alnahrawy, MBBCh Faculty of Medicine, Tanta University Email: [email protected]
Electronic data managers Bilal Mansour Faculty of Medicine, Al-Azhar University Email: [email protected]
Dr. Mohamed Ahmed El-hendy, MBBCh Faculty of Medicine, Al-Azhar University, Cairo
Senior supervisors (alphabetically) Dr. Ali S Shalash, MD, PhD Movement Disorder Unit, Neurology department Faculty of Medicine, Ain Shams University
Prof. Hatem Samir, MD, PhD Movement Disorder Unit, Neurology department Kasr Al-ainy school of Medicine, Cairo University
Dr. Mohamed Abdel-Daim, PhD Pharmacology department, Faculty of veternary Medicine, Suez Canal University Member of the national ethics Committee – Academy of Scientific Research and Technology
Dr. Shaimaa Eljafary, MD, PhD Movement Disorder Unit, Neurology department Kasr Al-ainy school of Medicine, Cairo University
Dr. Wael Mohamed, MD, PhD Neuroscience research unit, Pharmacology department, Faculty of Medicine, Menoufia University
Clinical Study Protocol Egyptian Parkinson's Disease Study Group
3
Local Coordinators
Ain Shams University Doaa Alaa
Tel: +201115042512
Email: [email protected]
Alexandria University Mohamed Mamdouh Eissa
Tel: +201276590881
Email: [email protected]
Al-Azhar University (Cairo) Dr. Attia Mohamed Attia, MBBCh
Tel: +201098886071
Email: [email protected]
Al-Azhar University (Cairo) Females Asmaa Sameh Rashwan
Tel: +201019740159
Email: [email protected]
Al-Azhar University (Damietta) Doaa Emadeldin
Tel: +201028420048
Email: [email protected]
Al-Azhar University (Assiut) Aly Mogheeth
Tel: +201097002730
Email: [email protected]
Assiut University Muhammad Shawqi
Tel: +20 1100671067
Email: [email protected]
Beni Suef University Randa Nabil Abdelazeem
Tel: +201208538058
Email: [email protected]
Kasr Al-ainy School of Medicine Mariam Bakr
Tel: +201157890439
Email: [email protected]
Mansoura University Osama Abunar
Tel: +201121274792
Email: [email protected]
Menia University Hesham Mohamed Ali
Tel: +201116633496
Email: [email protected]
Menoufia University Mohamed El-Semany
Tel: +201065554243
Email: [email protected]

Clinical Study Protocol Egyptian Parkinson's Disease Study Group
4
Misr University of Science and Technology Ahmad Ali Hassanen
Tel: +201091716876
Email: [email protected]
October university Omar Mohamed El Zahar
Tel: +20 1090600068
Email: [email protected]
Suez Canal University Salma Fala
Tel: +201021040375
Email: [email protected]
Tanta University Dr. Shorouk El mesery, MBBCh
Tel: +201092365711
Email: [email protected]
Zagazig University Dr. Osama Mokhtar, MBBCh
Tel: +201143132442
Email: [email protected]

Clinical Study Protocol Egyptian Parkinson's Disease Study Group
5
1. Working Teams
This multicenter study will be delivered using a collaborative network model.
The study teams are divided into three groups:
1.1. Steering committee
This team will be responsible for study concept and design, protocol writing,
study dissemination, Redcap system and monitoring the study, performing the
analysis and drafting the final manuscript.
1.2. Local Leaders
This team will be responsible for gaining ethical approval from their
anticipated institution, organize working teams to prevent overlapping and
monitoring the study on their level.
1.3. Data collectors
This team is composed of all collaborators who collect the data for the study;
they are the most vital part. Each team is composed of two students. Each
hospital has at least one neurologist as a supervisor to help working teams
access hospital data and ensure data accuracy.
2. Authorship
The final manuscript will be published in an international peer-reviewed
journal using the group name “Egyptian Parkinson’s disease group” as a single
author and all collaborators will gain PubMed citation under the group name
as “non-author contributors”. The contribution of all collaborators will be
described in the acknowledgment. Following publication of this project, the
identified patient data will be made available on a public portal to allow for
secondary analyses.

Clinical Study Protocol Egyptian Parkinson's Disease Study Group
6
3. Abstract
Introduction Parkinson's disease is the second most common
neurodegenerative disorder affecting about 1-3% of population above 50
years. The epidemiology of PD is variable from a population to another due to
the implication of multiple genetic, environmental, and dietary factors in the
pathogenesis and course of the disease. The aim of this study is to investigate
the epidemiological and clinical features of PD among Egyptian population.
Methods and analysis This is a multicenter, national, cross-sectional study.
Any hospital in Egypt performing routine follow up of PD, and any patient with
Parkinson's disease according to the UK brain bank diagnostic criteria is
eligible to enter the study. Investigators will collect observational data on PD
patients for a 3-week period during a 6-month window. The primary outcomes
of the study are pattern of early symptoms of the disease, Unified Parkinson's
disease rating scale (UPDRS) part III, and quality of life of PD patients. The
secondary outcomes include non-motor symptoms, drug sufficiency, and
caffeine consumption.
Ethics and dissemination Centers will process the required ethical approvals
from the corresponding ethics committee or institutional review board. An
oral informed consent will be taken from each patient in the presence of a
third party. During the study, patient IDs and will be kept secure. Following
the study, the deidentified IPD will be shared upon request with other
investigators to allow for secondary analyses.
Study registration The protocol of this study was registered on
www.clinicaltrials.gov (Registration number: NCT02785510).
Keywords Parkinson's disease, Clinical profile, Population, Egypt
Clinical Study Protocol Egyptian Parkinson's Disease Study Group
7
4. Introduction
Parkinson’s disease is the second most common neurodegenerative disorder,
affecting >1% of population above 60 years. The cardinal pathological features
of Parkinson’s disease are death of dopaminergic neurons and the formation
of Lewy bodies [1]. The diagnosis of PD depends on the presence of one or
more of the four most common motor symptoms including (rigidity, tremors,
postural instability, and bradykinesia) [2]. In addition, PD patients experience
a variety of non-motor symptoms such as anxiety, depression, mood swinging,
dementia, sleep disturbances, psychosis, hallucinations and orthostatic
hypotension [3, 4]. To date, there is no cure for PD and current
pharmaceutical therapies only target symptomatic relief.
Studying the epidemiology of PD plays a key role, not only in health care
planning, but also as a tool to investigate the cause and risk factors of the
disease. The incidence rate of PD (per 100,000 person-years) in the Unites
States is 12.3 persons and it increases to 44 persons among population over
50 years [5]. The prevalence of PD in Africa is 160 per 100,000 people and is
expected to increase by 200% within two decades after 2005 if the population
structure follows the current predictions [6].
The Egyptian population is demographically characterized by large family units
and high rates of birth and consanguinity marriage. Former studies on Arab
and North African populations showed that such demographic structure can
increase the risk of familial PD, both autosomal dominant and autosomal
recessive types. Moreover, as a developing country, the population is aging at
a faster rate than the developed countries, with an expected three-time
increase in the elderly population within the next 40 years. Therefore, the
burden of PD will increase, probably beyond the capabilities of the Egyptian
healthcare system.
There is a documented association in the literature between exposure to
pesticides and the risk of PD. Being an agricultural country, about 120,000
Egyptian citizens are annually involved in spraying 10 to 60 thousand tons of
pesticides in cotton fields, mainly in May, July, and September. These
individuals are employed by the Egyptian ministry of agriculture and they are
usually unequipped with the proper knowledge on safe handling of such
chemicals. Moreover, household use of insecticides and rodenticides
Clinical Study Protocol Egyptian Parkinson's Disease Study Group
8
increases the exposure to organophosphates and carbamates among Egyptian
citizens.
Despite these genetic and environmental risk factors, few former studies were
published about the prevalence of PD in some Egyptian governorates and
districts. Therefore, we designed this study to investigate the clinical profile of
PD among Egyptian patients on a nationwide scale.
5. Aims and objectives
The aim of this study is to determine the epidemiological and clinical features
of Parkinson’s disease among the Egyptian population.
The primary objectives of this study are:
▪ To determine early symptoms of Parkinson's disease onset in Egyptian
population
▪ To measure the quality of life in PD patients within Egypt
The secondary objectives of this study are:
▪ To estimate the prevalence and pattern of caffeine intake in Egyptian
population with PD
▪ To investigate the association between caffeine intake and age at
disease onset in Egyptian population with PD
▪ To investigate the association between quality in life and treatment
sufficiency in Egyptian population with PD
▪ To investigate the association between caffeine intake and quality of
life in Egyptian population with PD
6. Patient and Methods
This study is a national, collaborative, cross sectional study. This study is
delivered through social media and professional networks within Egypt. We
use the collaboration methodology to enroll potential centers to perform this
study.
6.1. Study setting
This study will be conducted in self-selected (registered) centers. Eligible
center is defined as a university hospital, teaching hospital, governmental or
Clinical Study Protocol Egyptian Parkinson's Disease Study Group
9
private clinic, where PD patients are attending for treatment and follow up.
Eligible centers should be registered on the study website before 1st, July 2017
(see appendix).
6.2. Study population
The target population is defined as patients with Parkinson's disease, those
who meet the Parkinson’s disease diagnostic criteria of UK Parkinson's Disease
Society Brain Bank [7]. Patients, who meet these criteria, within the registered
centers are included in this study.
6.3. Exclusion criteria
We will exclude patients with the following conditions:
▪ Patients with vascular Parkinsonism (history of stroke)
▪ Patients with treatment induced Parkinsonism
▪ Patients with a history of exposure to the dopaminergic neurotoxin
MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine)
6.4. Data entry
Data will be submitted to the Research Electronic Data Capture (RedCap)
system of Al Azhar University, Egypt (http://redcap.medicineazhar.edu.eg).
Each collaborating team will be assigned unique username and password to
access RedCap system. Data collection is designed to allow entry of individual
patient data electronically and uploading a scan of the data collection forms.
Data will be double-checked by the steering committee to avoid data entry
errors.
6.5. Study variables and outcome measures
We will collect the following data variables and measures from each eligible
patient:
▪ Age at disease onset
▪ Time to diagnosis
▪ Initial motor symptom
▪ Side of initial motor symptoms
▪ Clinical subtype of the disease
▪ Pattern of levodopa treatment
▪ Levodopa equivalent dose per day
Clinical Study Protocol Egyptian Parkinson's Disease Study Group
10
▪ Duration of levodopa treatment from disease onset
▪ Non-motor symptoms measured by the non-motor symptoms
questionnaire
▪ Quality of life including mobility, activities of daily living, emotional
well-being, stigma, social support, cognition, communication, and
bodily discomfort. The Parkinson's disease quality of life
questionnaire (PDQ-39) will be used.
▪ Caffeine consumption measured by the Caffeine use questionnaire
developed by Millar and colleagues.
▪ Motor functions measured by the Unified Parkinson's disease rating
scale – Part III will be included (if available)
6.6. Statistical analyses and power calculation
Assuming the recruitment of 15 patients within a 3-week period from 30
centers. This will give a total of 450 patients, which allows for detecting a
5(±3)% rate of early disease symptoms in the population with a confidence
level of 95% and 5% margin of error.
Data will be presented as mean and standard deviation for continuous
variables and frequencies and percentages for categorical variables. Data
normality will be examined using the Kolmogorov-Smirnov test. Chi-square
test and student t-test will be employed the test the significance of
differences in categorical and continuous variables, respectively. Multivariate
analysis will be conducted to compare caffeine consumption and quality of life
in PD patient groups (classified according to early disease symptoms). An
alpha level below 0.05 will be considered for statistical significance. Statistical
analysis will be conducted using Stata statistical package (version 14) for
windows.
7. Discussion
In this protocol, we have presented the detailed design and objectives of our
cross-sectional study, targeted at nationwide assessment of the clinical profile
of PD among the Egyptian population. The definition of study population, the
ethical soundness of the protocol, and the means for data collection were
given attention in the design process. Moreover, we reported the exact
methods of data entry and provided prospective solutions for possible
challenges in our statistical analysis.
Clinical Study Protocol Egyptian Parkinson's Disease Study Group
11
In a systematic review by Benamer et al. (2008) on the clinical profile of PD
among Arabs, the authors found only three epidemiological studies,
conducted in Tunisia, Libya, and Saudi Arabia. The review reported that PD
has an incidence of 4.5 per 100,000 person-years, with a prevalence that
ranges from 27 to 43 per 100,000 persons. It concluded that the clinical
features of PD in Arabs are not different from those reported in other
populations and highlighted the need for further epidemiological studies on
PD clinical profile within Arab populations.
After surveying the literature, we identified four epidemiological studies,
recently published from Egypt, on the epidemiology of PD. In 2012, Khedr and
colleagues conducted a community-based survey in Assiut governorate, Egypt
to identify the prevalence and clinical profile of PD within the Egyptian
population. The authors estimated a crude prevalence of 659/100,000
inhabitants, which increases with age, living in rural areas, and illiteracy.
Moreover, the study showed that compared to other populations, these
patients showed a high prevalence of mood/cognition dysfunction (84.4%)
and gastrointestinal symptoms (90.9%).
Another two cross sectional studies by El-Tallawy et al. (2013) and Khedr et al.
(2015) were conducted on the Egyptian population in the New Valley and
Qena governorates, respectively. These studies have reported crude
prevalence rates, ranging from 213.15 to 2748 per 100,000 individuals. These
figures are relatively high, compared to those, reported in other Arab
countries. Khedr et al. explained their findings by the presence of several
sugar refining, paper making, and manganese production factories in Qena
governorate, which partly drain their sewage into the Nile or its water canals.
Excessive deposition of manganese within the brain tissue leads to
manganism, a condition that shares multiple features with PD such as
hypokinesia, rigidity, and psychotic symptoms. Table 1 shows a list of the
cross-sectional studies, conducted within the Arab populations, on the
epidemiology or clinical profile of PD.
Clinical Study Protocol Egyptian Parkinson's Disease Study Group
12
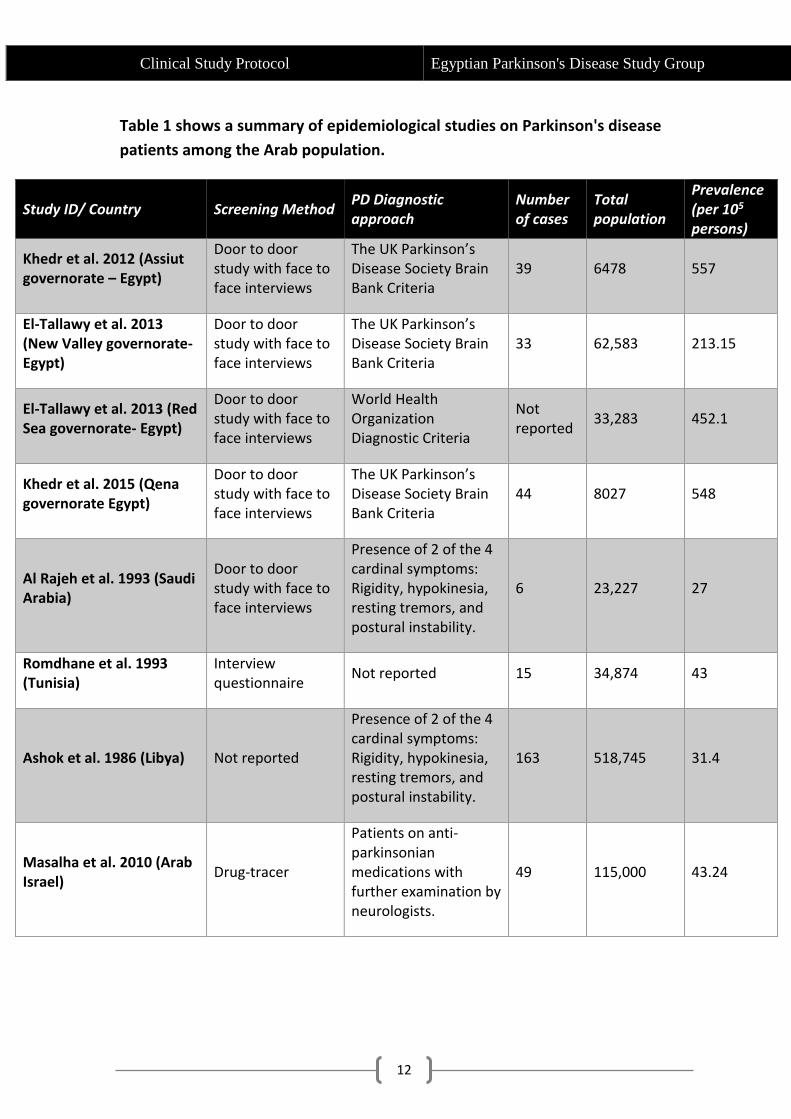
Table 1 shows a summary of epidemiological studies on Parkinson's disease
patients among the Arab population.
Study ID/ Country Screening Method PD Diagnostic approach
Number of cases
Total population
Prevalence (per 105 persons)
Khedr et al. 2012 (Assiut governorate – Egypt)
Door to door study with face to face interviews
The UK Parkinson’s Disease Society Brain Bank Criteria
39 6478 557
El-Tallawy et al. 2013 (New Valley governorate- Egypt)
Door to door study with face to face interviews
The UK Parkinson’s Disease Society Brain Bank Criteria
33 62,583 213.15
El-Tallawy et al. 2013 (Red Sea governorate- Egypt)
Door to door study with face to face interviews
World Health Organization Diagnostic Criteria
Not reported
33,283 452.1
Khedr et al. 2015 (Qena governorate Egypt)
Door to door study with face to face interviews
The UK Parkinson’s Disease Society Brain Bank Criteria
44 8027 548
Al Rajeh et al. 1993 (Saudi Arabia)
Door to door study with face to face interviews
Presence of 2 of the 4 cardinal symptoms: Rigidity, hypokinesia, resting tremors, and postural instability.
6 23,227 27
Romdhane et al. 1993 (Tunisia)
Interview questionnaire
Not reported 15 34,874 43
Ashok et al. 1986 (Libya) Not reported
Presence of 2 of the 4 cardinal symptoms: Rigidity, hypokinesia, resting tremors, and postural instability.
163 518,745 31.4
Masalha et al. 2010 (Arab Israel)
Drug-tracer
Patients on anti-parkinsonian medications with further examination by neurologists.
49 115,000 43.24
Clinical Study Protocol Egyptian Parkinson's Disease Study Group
13
Another focus of our study is the assessment of non-motor symptoms (NMS)
among the Egyptian PD patients, including cognitive impairment, sleep
disturbances, neuropsychiatric disorders, sexual dysfunction, and
gastrointestinal and cardiovascular symptoms. These symptoms can limit the
effective treatment of motor manifestations; therefore, early management of
NMS can supplement motor treatment, limit the financial impact of PD, and
improve the quality of life for the patient and the caregiver. In our study, we are
planning to use the Non-Motor Symptoms Scale (NMSS), which was designed to
quantify the overall prevalence of NMS.
Other important characteristics of PD that were not comprehensively
investigated in Egyptian patients include the mean age at disease onset, time to
PD diagnosis from the onset of symptoms, drug responsiveness, and quality of
life. Therefore, in our study, we planned to identify these variables by using
validated questionnaires such as the Parkinson's disease quality of life
questionnaire (PDQ-39) and calculating the duration of Levodopa treatment and
its current dosages.
7.1. Expected challenges and solutions
The presence of cognitive impairment in some parkinsonian patients may
increase the risk of recall bias; therefore, during the interviews, caregivers will
be allowed to help their patients to ensure accurate data collection. To increase
the participation of clinical neurologists in data collection, all practicing
neurologists who contribute to data collection will be listed as collaborators in
our published study. All used questionnaires or scales of assessment will be
prospectively reviewed by expert neurologists and all open-ended questions will
be coded and entered in a simple spread sheet. We excluded patients with
vascular or treatment-related Parkinsonism due to the temporary nature of the
condition.
In summary, there are no sufficient data about the clinical profile of PD in Egypt.
Therefore, we designed this nation-wide, cross sectional study to provide these
data, which would provide better therapeutic management for PD patients and
guide future planning of healthcare services in Egypt.
Clinical Study Protocol Egyptian Parkinson's Disease Study Group
14
8. Ethical Considerations
8.1. Risk, benefit, and participant confidentiality
The Study does not have any physical, psychological, social, legal, economic, or
any other anticipated risks to study participants. In addition, participants will not
receive a direct benefit from the study. Investigators will keep the privacy of
patient data. Data submitted to the RedCap will not include patient name or
national ID; instead, patient ticket number will be used as a unique number to
avoid duplicate reporting of the patient data. We confirm that patient data will
not be used outside this study.
8.2. Informed Consent Process
We will comply with institutional guidelines of each registered center. The
informed consent form, provided by the anticipated IRB or ethics committee,
will be used by study collaborators. All eligible patients who agree to participate
in the study will be asked to sign the informed consent.
8.3. Institutional Review Board
Before starting data collection, collaborators of the registered centers should
gain ethical approval from the anticipated local IRB or ethics committee of their
institution. Investigators are advised to comply with institutional guidelines. In
case of any changes to the study protocol, the ethics committee will be
informed.
9. Publication and dissemination
This project will be published using a collaborative publishing model. The final
manuscript will be published in an international peer-reviewed journal using the
group name “Egyptian Parkinson’s disease group” as a single author and all
collaborators will gain PubMed citation under the group name as “non-author
contributors”. The contribution of all collaborators will be described in the
acknowledgment. Following publication of this project, the identified patient
data will be made available on a public portal to allow for secondary analyses.
Clinical Study Protocol Egyptian Parkinson's Disease Study Group
15
10. Centers registration
This study follows a collaborative model. Collaborators are required to register
their centers and submit the institutional ethical approval before starting data
collection.
This study will be published using the collaborative published model. The
manuscript(s) are published under a single group name as an author (Egyptian
Parkinson’s Disease Study Group). and all collaborators (see the working teams
in the next section) will be listed with their institution in the acknowledgment
section.
11. References
1. Obeso JA, Rodríguez-Oroz MC, Benitez-Temino B, et al (2008) Functional organization of the basal ganglia: Therapeutic implications for Parkinson’s disease. Mov Disord 23:548–559. doi: 10.1002/mds.22062
2. Jankovic J (2008) Parkinson’s disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry 79:368–376. doi: 10.1136/jnnp.2007.131045
3. Zindo FT, Barber QR, Joubert J, et al (2013) Steady progress on parkinson’s disease. Eur J Med Chem 54:883–891. doi: 10.1016/j.bmcl.2010.07.013
4. Ceravolo R, Frosini D, Rossi C, Bonuccelli U (2010) Impulse control disorders in Parkinson’s disease: definition, epidemiology, risk factors, neurobiology and management. Park Relat Disord 15:S111–S115. doi: 10.1016/S1353-8020(09)70847-8
5. Van Den Eeden SK (2003) Incidence of Parkinson’s Disease: Variation by Age, Gender, and Race/Ethnicity. Am J Epidemiol 157:1015–1022. doi: 10.1093/aje/kwg068
6. Dotchin C, Msuya O, Kissima J, et al (2008) The prevalence of Parkinson’s disease in rural Tanzania. Mov Disord 23:1567–672. doi: 10.1002/mds.21898
7. Hughes AJ, Daniel SE, Kilford L, Lees AJ (1992) Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry 55:181–184.