Embed Size (px)
Citation preview

Diphenylhydantoin in Cardiac Arrhythmias*
MICHAEL ROSEN, M.D., ROBERT LISAK, M.D. AND IRA L. KITBIN, M.D., F.A.C.C.
New York, New York
D IPHENYLHYDANTOIN, introduced over 25 years ago,’ has become a cornerstone of
seizure therapy, due to both its effectiveness and the infrequent occurrence of serious side effects.2 s3 Since 1950, studies concerning the efficacy of intravenously administered diphenyl- hydantoin in treating acute cardiac arrhyth- mias4-6 and of the orally administered prepara- tion in chronic arrhythmias7 have appeared. One study6 assessing the value of diphenylhy- dantoin in digitalis-induced arrhythmias in dogs showed a reduction in mortality from 60 per cent in controls to 5 per cent in animals treated with diphenylhydantoin.
Current studies have not fully evaluated the range of arrhythmias in which diphenylhy- dantoin may prove beneficial, nor has its con- sistency been ascertained.8 In this study, di- phenylhydantoin was administered as the initial drug in a series of patients with cardiac ar- rhythmias. The only patients excluded were those with ventricular rates less than bO/min. and those with second degree (or greater) atrioventricular block. Patients were classified as to type of arrhythmia, heart disease and cur- rent drug therapy.
METHODS
Fifty-seven patients, having 73 episodes of ar- rhythmias, received intravenous diphenylhydantoin, 5 mg./kg., not exceeding 350 mg. The drug was infused through a rubber sidearm of an infusion of 5% dextrose in water over 0.5 to 4 minutes. Blood pressure and electrocardiogram were monitored continuously. Metaraminol, 100 mg. in 500 cc. 5% dextrose in water, and atropine, 0.4 mg., were kept at the bedside to treat possible hypotension and bradycardia, respectively. When an arrhythmia responded favorably to diphenylhydantoin (con- version to sinus rhythm or significant slowing of ven- tricular rate), the patient was immediately given 100 mg. of the drug intramuscularly and then placed on o&a? or intramuscular maintenance, 300 to 400 mg./day in divided doses. Therapy was continued for an average of five days, after which the patient
was “weaned” off the drug and digitalis therapy re- instituted when indicated. If the initial intravenous dose of diphenylhydantoin failed to abort the ar- rhythmia within 10 minutes of administration, the drug was discontinued, and other methods of treat- ment were attempted. In 29 cases, infusion of 5% dextrose in water was given for five minutes prior to diphenylhydantoin, to evaluate any placebo effect.
RESULTS
All arrhythmias that responded did so within five minutes after completion of diphenylhy- dantoin infusion (Fig. l-5). There was no response to placebo therapy.
Supraventricular Arrhythmias: There were 7 instances of paroxysmal atria1 tachycardia (Table I). Three, including 1 patient with heart block, occurred in patients on digitalis therapy, 4 in nondigitalized patients. The former uniformly responded to diphenylhy- dantoin ; the latter did not. In 2 instances of wandering atria1 pacemaker in patients on digitalis therapy, diphenylhydantoin was in- effective. Of 15 cases of atria1 flutter 9 oc- curred in patients on digitalis; of these 9, 2 patients responded favorably to diphenylhy- dantoin and were maintained on this. The other 7 on digitalis and the 6 not on glycosides did not respond to diphenylhydantoin and were given digitalis with uniformly good results. Two episodes of paroxysmal atria1 fibrillation occurred in digitalized patients who responded favorably to diphenylhydantoin; 2 patients not on glycosides showed no response. Of the 7 remaining instances of atria1 fibrillation, 1 (the patient was on digitalis) was converted to wandering atria1 pacemaker after diphenylhy- dantoin administration. In the other 6 the patients failed to respond.
Ten additional instances of supraventricular tachycardia occurred in 8 patients. Seven were on digitalis, and all responded initially to diphenylhydantoin. However, in 2 cases, the
* From the Medical Division, Montefiore Hospital and Medical Center, 111 E. 210 St., Bronx, N.Y. 10467.
674 THE AMERICAN JOURNAL OF CARDIOLOGY

Dilantin in Cardiac Arrhythmias 675
arrhythmia recurred (in 1, maintenance di- phenylhydantoin was inadvertently not given) and proved refractory to further drug adminis- tration. One patient with supraventricular tachycardia not on glycosides failed to respond to diphenylhydantoin. Of 4 nodal tachycardias (all patient taking glycosides) 2 were reverted by diphenylhydantoin and 2 were not. In 2 instances of nodal premature contractions, the patients on glycoside therapy responded to diphenylhydantoin.
Ventricular Arrhythmias: Four cases of ven- tricular bigeminy occurred in digitalized pa- tients; all responded to diphenylhydantoin.
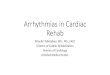
FIG. 1. Ventricular bigeminy and nzultifocal wntricular and nodal extrasystoles developed in a 73 year old woman on digitalis therapy. Diphenylhydantoin, 250 mg.. was administered for 120 seconds. Ninety seconds after the end of the infusion, normal sinus rhythm was restored.
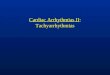
FIG. 2. Paroxysmal atria1 tachycardia with varying block developed in a 67 year old man on digitalis therapy. Di- phenylhydantoin was administered intravenously for four minutes. Fifty seconds after the end of infusion, normal sinus rhythm resumed.
The fifth, in a patient not on glycosides, was re- fractory. Of 13 instances of multifocal ven- tricular premature contractions, 9 occurred in digitalized patients; in 8 of these the patients responded to diphenylhydantoin. In the ninth that was refractory the patient subsequently re- sponded to further digitalis. Of the 4 patients not on glycosides, 1 responded to diphenyl- hydantoin ; the others did not. There were 3 cases of ventricular tachycardia, all in patients not taking digitalis; none responded to di- phenylhydantoin.
A final case was not supervised by our group but was brought to our attention after death. A patient terminally ill after abdominal surgery was placed on intravenous isoproterenol be- cause of complete atrioventricular dissociation and a slow idioventricular rhythm. Diphenyl- hydantoin was infused, and within 60 seconds ventricular standstill developed and the patient died.
Summary of Results: Of 73 arrhythmias, 49 occurred in patients on digitalis. Thirty-one of these responded to diphenylhydantoin (63.2%). There were 36 episodes of supraven- tricular arrhythmia in patients on digitalis; 19 were converted by diphenylhydantoin (52.9%). If the cases of atria1 flutter and
VOLUME 20, NOVEMBER 1967
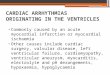
FIG. 3. Supraventricular tachycardia developed in a 68 year old woman on digitalis and quinidine therapy. Di- phenylhydantoin, 250 mg., was administered for 34 sec- onds. Twenty-seven seconds after onset of infusion the arrhythmia reverted to sinus tachycardia.
FIG. 4. Paroxysmal atrialjbrillation developed in a 76 year old woman on digitalis therapy. Diphenylhydantoin, 250 mg., was administered for three minutes. Sixty sec- onds after the end of infusion, the ventricular response decreased markedly. The patient was restored to normal sinus rhythm in 12 hours.

676 Rosen, Lisak and Rubin
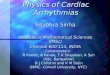
FIG. 5. A, bidirectional nodal tachycardia developed in an 84 year ok1 woman on digitalis therapy. Diphenylhydantoin, 200 mg., was administered for 30 seconds. Twenty-four seconds after the end of infusion, the patient was converted to a slower nodal rhythm. B, atrial@ter with a ventricular rate of 1 SO devrloped in a 76 year old man on digitalis therapy. Diphenylhydantoin, 250 mg., was ad- ministered for 30 seconds. Fourteen seconds after onset of infusion the ventri- cular response slowed transiently and then was converted to nodal rhythm at a rate of 93/min.
chronic atria1 fibrillation are subtracted from the series, then of the 35 total arrhythmias in digitalized patients, diphenylhydantoin was effective in 28 (8Oyc); and of the 22 supraven- tricular arrhythmias, effective in 16 (72.7%). Thirteen ventricular arrhythmias occurred in digitalized patients; in 12 there was favor- able response to diphenylhydantoin (92.3%). Twenty-four supraventricular and ventricular arrhythmias occurred in patients not on digitalis; in only 1 was diphenylhydantoin (4.1%) effec- til-e.
Side Effects and Complications: Side effects in- cluded light-headedness (13 cases) and transient pain at infusion site (19 cases). There was transient but marked hypotension in 3 cases, an incidence of 5.2 per cent. In 2, metaraminol infusion was required for less than 15 minutes to maintain blood pressure; in the other, pressure returned to normal within 90 seconds. In all 3 cases, the blood pressure fell within two min- utes of diphenylhydantoin infusion. Transient hypotension of a lesser degree (a fall of less than 15 mm. Hg systolic pressure) was an invariable accompaniment of drug infusion. There was 1 case of sinus arrest lasting six seconds in which the patient responded favorably to a single blow on the chest. There were no unfavorable se- quelae to any of the aforementioned toxic mani- festations. The sole mortality in the series may be traced directly to improper use of diphenyl- hydantoin for the treatment of complete heart block with an idioventricular rhythm.
DISCUSSION
Our data suggest that diphenylhydantoin is of significant value in treating digitalis- induced supraventricular and ventricular ar- rhythmias; however, we do not believe a suc-
cessful result with this drug should be considered diagnostic of digitalis toxicity. The favorable result obtained in 1 patient not on glycosides, coupled with the unresponsiveness of several ar- rhythmias we considered to be digitalis-in- duced (2 instances of nodal tachycardia), sup- port this interpretation.
In instances where diphenylhydantoin ther- apy successfully abolished supraventricular ar- rhythmias, three patterns of conversion were noted: (1) an abrupt shift of rhythm and rate from tachycardia to a slower rate or sinus rhythm; (2) a variable period of slowed ven- tricular response, never more than two minutes in duration, occurring prior to conversion; and (3) a brief sinus arrest (6 sec. in 1 patient, other- wise no longer than 3 sec.) followed by sinus rhythm. No significant change in duration of QRS complexes was noted.
The action of diphenylhydantoin at the atrio- ventricular node appears to be that of increasing block. This was demonstrated transiently even in some arrhythniias that did not convert, no- tably the atria1 flutters. The possibility that this effect may be vagally mediated has not been explored.
Little is known concerning the relation of diphenylhydantoin action to ion transport. One suggestion, that diphenylhydantoin may deplete intracellular sodium,8 is contradicted by Woodbury’s studies,g which failed to demon- strate sodium or potassium gradients in cardiac tissues of normal rats (although in rats rnade acutely hyponatremic, diphenylhydantoin did bring about intracellular sodium depletion). In our patients, serum electrolyte determinations for the most part revealed no aberrations. However, in 1 patient on digitalis and in hepatic coma (Case 47) with serum potassium 2.7
‘I-HE AMERICAN JOURNAI. OF CARDIOLOGY

Dilantin in Cardiac 4rrhythmias 677
? ABLE 1 Summary of Treated Cases
r-----On Digitalis---- No
Response Response
,--Not on Digitalis-- ~. No
Response Response
Paroxysmal atria1 tach. Paroxysmal atria1 tach. with block Wandering atria1 pacemaker Atria1 flutter Paroxysmal atria1 fibrillatron Chronic atria1 fibrillation Nodal tachycardia Nodal premature contractions Unclassified supraventricular tach.
Subtotal
2* - - 4 1 -
2 2 7 6 2 - 2 1 4 - 2 2 2 --
2 - -
7i 2 - --
19 17 0 15
B. Vmtl-icular Arrhythmias
--.
Bigeminy Multifocal ventricular premature con. Ventricular tach. Atrioventricular dissociation
Subtotal Totals
41 - - 1 SC - - 3 II
37 - 1”
12 1 1 8 31 18 1 23
* One of these patients was on potassium chloride, 4 gm./day, and hydrochlorothiazide, 50 mg./day as well as digitalis. Two hours prior to administration of diphenylhydantoin, his arrhythmia was found to be unresponsive to 40 mEq. of potassium chloride intravenously administered.
t Two of these patients were on quinidine, 1.6 gm./day, as well as digitalis. t One of these patients was on potassium chloride, 4 gm./day and hydrochlorothiazide, 50 mg./day as well as
digitalis. 5 One of these patients was on procainamide, 2 gm./day, and potassium chloride, 4 gm./day, as well as digitalis. II Two of these patients were on procainamide, 2 gm./day. li One of these patients was on quinidine, 1.6 gm./day. f This patient was on an isoproterenol intravenous infusion prior to administration of diphenylhydantoin. Tach. = tachycardia; con. = contractions.
mEq.,‘L., the arrhythmia responded to di- phenylhydantoin prior to any potassium ad- ministration. This is consistent with either a direct effect of diphenylhydantoin upon the potassium gradient, or an effect on another ion (sodium, calcium, magnesium) compensating for potassium depletion. Although this is speculation, it may be that an alteration in intra- or extracellular sodium or potassium, or both, induced by overdigitalization can lay the groundwork for a diphenylhydantoin- induced ionic gradientlO This may explain why diphenylhydantoin converted predom- inantly digitalis-induced arrhythmias.
Although toxicity secondary to diphenylhy- dantoin infusion was for the most part minor, significant hypotension did occur in 3 of our patients. The work of Mixter et al.” suggests
VOLUME 20, NOVEMBER 1967
that diphenylhydantoin is both a myocardial depressant and a vasodilator, thereby explain- ing the mechanism of its action. The only avail- able study comparing diphenylhydantoin to the commonly employed myocardial depres- sants, quinidine and procainamide, states that all three are equally efficacious in abolishing ouabain-induced ventricular tachycardias in dogs, with diphenylhydantoin being the least toxic.12 Although additional studies are needed comparing efficacy and toxicity of the three drugs in man, this is further evidence for the relative safety of diphenylhydantoin in the treatment of digitalis-induced ventricular and supraventricular arrhythmias.
Previously reported clinical studies do not entirely support our own. Conn’s5 successes included a number of patients who were not on

678 Rosen, Lisak and Rubin
digitalis when their arrhythmia developed. The observations of Bernstein et al.,? that re- current arrhythmias unrelated to digitalis ther- apy responded to chronic oral use of diphenyl- hydantoin, also are not in agreement with ours. Although selection of patients and route of drug administration could account in part for this variance, the differences among the series cannot be entirely reconciled.
SUMMARY
1. Diphenylhydantoin was administered in- travenously to 57 patients in whom 73 cardiac arrhythmias occurred. Thirty-one of 49 ar- rhythmias in patients on digitalis preparations were converted by diphenylhydantoin. Of 24 arrhythmias in patients not on digitalis, di- phenylhydantoin was effective in 1. All re- sponses occurred within five minutes after drug infusion.
2. In digitalized patients, conversion of an arrhythmia to regular sinus rhythm or signif- icant slowing of ventricular response following diphenylhydantoin may be considered suppor- tive evidence that the arrhythmia was digitalis- induced. However, unresponsiveness to di- phenylhydantoin in a digitalized patient should not necessarily mean that the patient is inade- quately digitalized.
3. Minor side effects included transient pain at the infusion site and light-headedness. Three patients experienced profound hypotension of brief duration (2 required metaraminol), and 1 experienced sinus arrest and asystole of six seconds’ duration prior to conversion of his arrhythmia. None of these episodes was as- sociated with serious sequelae. The occurrence of hypotension indicates the need for slow drug administration.
4. Diphenylhydantoin should not be used in
patients who have a high degree of heart block or marked bradycardia.
REFERENCES
1. MERRITT, H. H. and PUTNAM, T. J. Sodium di- phenylhydantoin in treatment of convulsive dis- orders. J.A.M.A., 111: 1068, 1938.
2. TORMAN, J. E. In: GOODMAN, L. S. and GILMAN, A. The Pharmacological Basis of Therapeutics, ed. 3, chap. 13, p. 222. New York, 1965. Macmillan.
3. UNNA, K. R. W. Drugs used in epilepsy and hyper- kinetic states. In: Pharmacology in Medicine, ed. 3, p. 184. Edited by DRILL, V. A. New York, 1958. McGraw-Hill, Blakiston Division.
4. HARRIS, A. S. and KOKERNOT, R. M. Effects of diphenylhydantoin sodium and phenobarbital so- dium upon ectopic ventricular tacbycardia in acute myocardial infarction. Am. J. Physiol., 163: 505, 1950.
5. CONN, R. D. Diphenylhydantoin sodium in cardiac arrhythmias. New Engkmd J. Med., 272: 277, 1965.
6. LANG, T. et al. Digitalis toxicity; treatment with diphenylhydantoin. Arch. Znt. Med., 116: 573, 1965.
7. BERNSTEIN, M., et al. Sodium diphenylhydantoin in the treatment of recurrent cardiac arrhythmias. J.A.M.A., 191: 695, 1965.
8. RUTHEN, G. C. Antiarrhythmic drugs. Diphenyl- hydantoin in cardiac arrhythmias. Am. Heart J., 70: 275, 1965.
9. WOODBURY, D. H. Effect of diphenylhydantoin on electrolyte and radiosodium turnover in brain and other tissues of normal, hyponatremic, and postic- tal rats. J. Pharmacol. & Exper. Therap., 74: 115, 1955.
10. HELFANT, R. Personal communication. 11. MIXTER, C. G., MORAN, J. M. and AUSTIN, W. G.
Cardiac and peripheral vascular effects of di- phenylhydantoin sodium. Am. J. Cardiol., 17: 332, 1966.
12. MOSEY, L. and TYLER, M. D. The effect of di- phenylhydantoin sodium, procaine hydrochloride, procainamide hydrochloride, and quinidine hydrochloride upon ouabain-induced ventricular tachycardia in unanesthetized dogs. Circulation, 10: 65, 1954.
THE AMERICAN JOURNAL OF CARDIOLOGY