Embed Size (px)
Citation preview
Configuration of Arterial Grafts: In-situ vs composite arterial
conduits
Dr. Bakir Mostafa Bakir Associate Professor & Consultant of Cardiac Surgery
King Fahad Cardiac Center, KSUMC, KSA
• CABG continues to be an effective therapy for many patients with long-term durability and consistent outcomes despite the advancement in PCI.
• The unparalleled long-term patency and better clinical outcomes of the LIMA made it the conduit of first choice for anastomosis to the LAD in almost all patients.
Characteristics of the Internal Mammary Artery:
1. Remarkable resistance to the development of atherosclerosis
2. Thin medial layer with fewer smooth muscle cells and a lesser proliferative response
3. The endothelium has higher basal production of vasodilators
4. Non-fenestrated internal elastic lamina that inhibits cellular migration and prevents intimal hyperplasia.
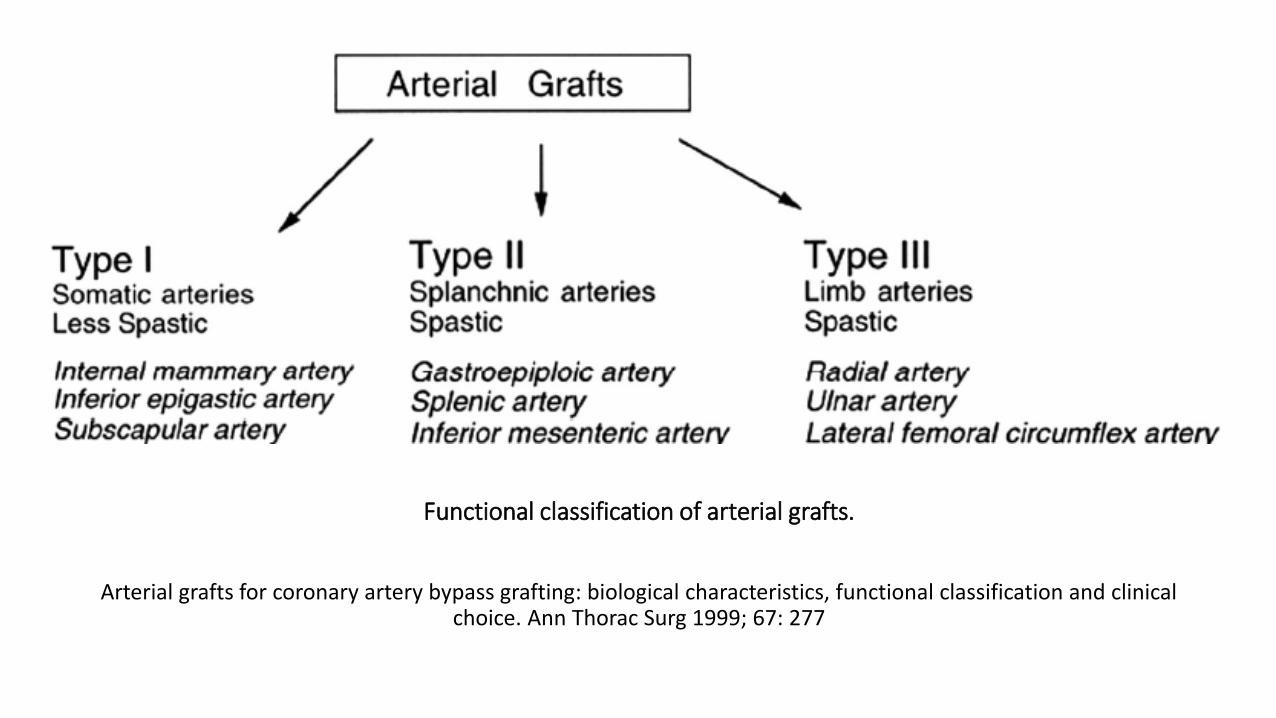
Functional classification of arterial grafts.
Arterial grafts for coronary artery bypass grafting: biological characteristics, functional classification and clinical choice. Ann Thorac Surg 1999; 67: 277
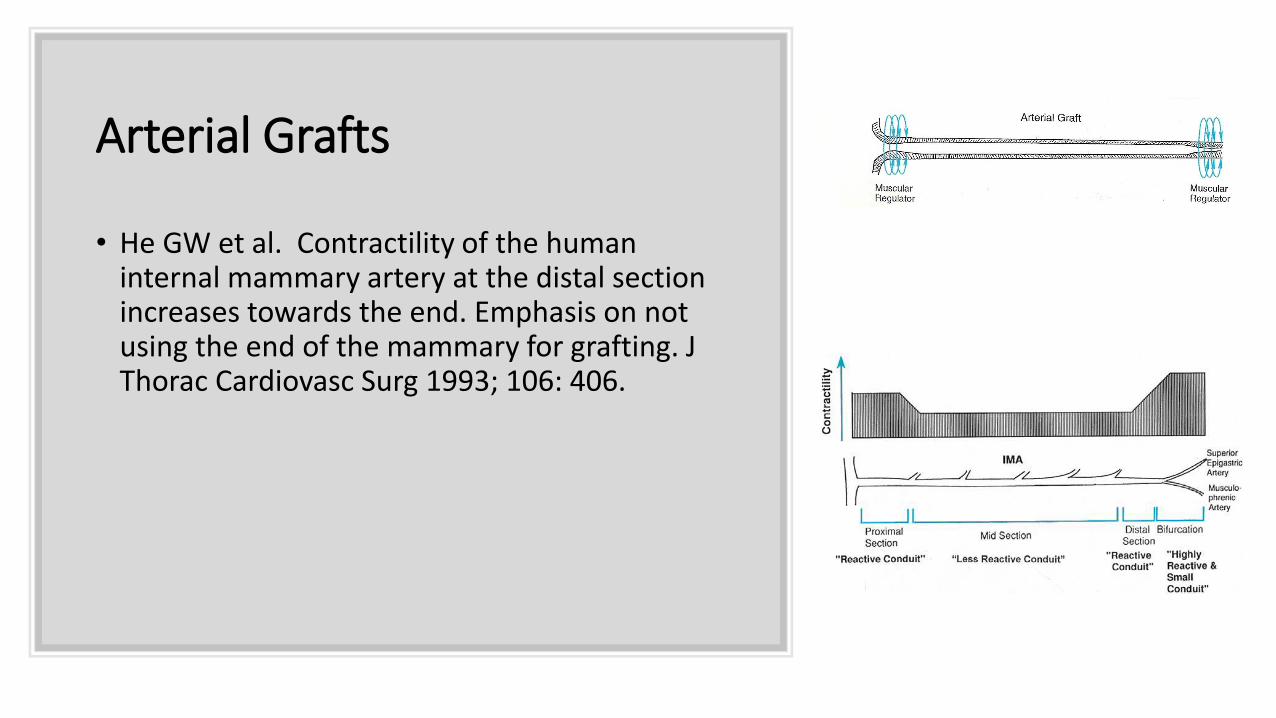
Arterial Grafts
• He GW et al. Contractility of the human internal mammary artery at the distal section increases towards the end. Emphasis on not using the end of the mammary for grafting. J Thorac Cardiovasc Surg 1993; 106: 406.
BIMA vs LIMA
• Evidence continues to accumulate that the use of BIMA in CABG positively affects long-term survival.
• Weiss et al (2013) conducted a meta-analysis demonstrating the definitive superiority of BIMA grafting when compared with LIMA grafting with additional SVGs. (Ann Cardiothorac Surg 2013; 2: 390).
Conclusion: there is increased long-term survival in patients receiving BIMA over those receiving a single IMA.
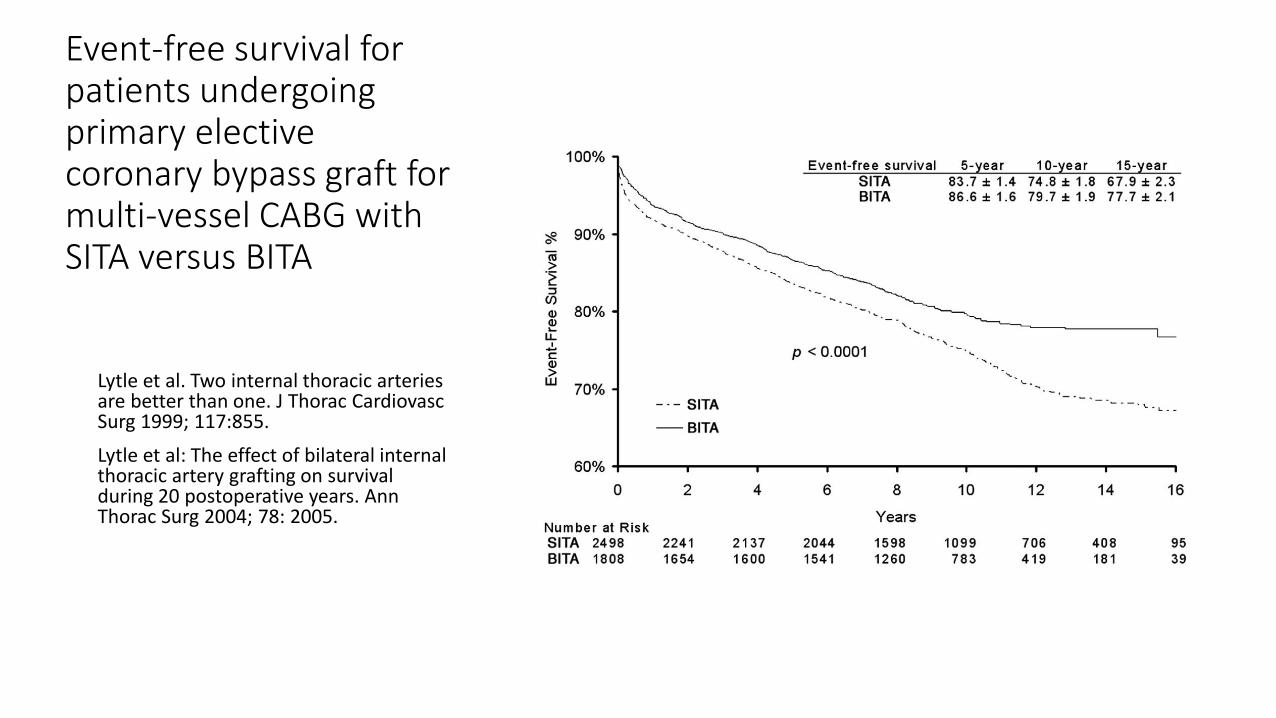
Event-free survival for patients undergoing primary elective coronary bypass graft for multi-vessel CABG with SITA versus BITA
Lytle et al. Two internal thoracic arteries are better than one. J Thorac Cardiovasc Surg 1999; 117:855.
Lytle et al: The effect of bilateral internal thoracic artery grafting on survival during 20 postoperative years. Ann Thorac Surg 2004; 78: 2005.
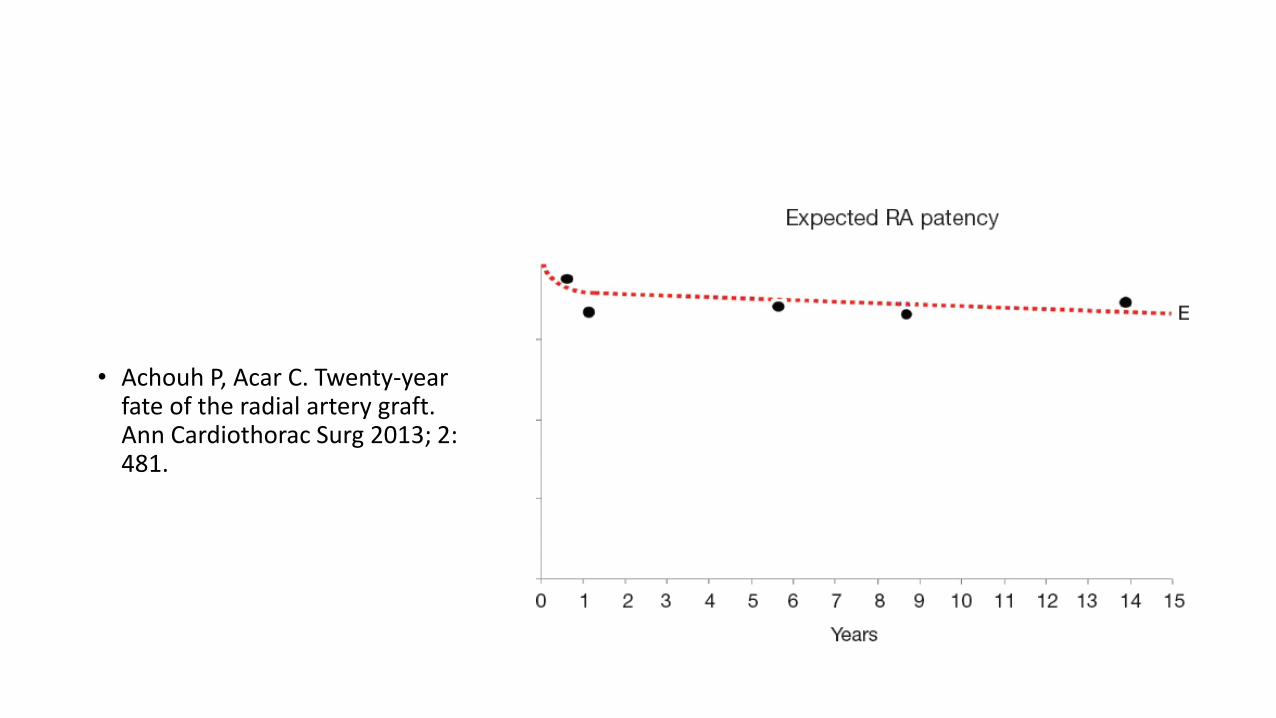
• Achouh P, Acar C. Twenty-year fate of the radial artery graft. Ann Cardiothorac Surg 2013; 2: 481.
• Logic suggests that using a second internal mammary artery would further improve long-term outcomes of revascularization.
Over 95% of all CABG in the USA, and over 90% in the United Kingdom and Australia, have only one arterial graft.
Tabata M, Grab JD, Khalpey Z, et al. Prevalence and variability of internal mammary artery graft use in contemporary multivessel coronary artery bypass graft surgery: analysis of the Society of Thoracic Surgeons National Cardiac Database. Circulation 2009;120:935-40.
The Society for Cardiothoracic Surgery in Great Britain and Ireland. Sixth National Adult Cardiac Surgical Database Report 2008. Bridgewater B, Keogh B, Kinsman R, et al. eds. Oxfordshire: Dendrite Clinical Systems Limited, 2009:125.
Configuration of Arterial Grafts
• Although there are many possible contributors to the underutilization of more arterial conduits, an important factor is the uncertainty about the optimal configuration of the arterial conduits.
• What is the best second arterial conduit of choice?
• How can the number of distal anastomoses /patient be increased
using arterial grafts?
• Outcome of composite grafts?
• Sternal complications?
Configuration of Arterial Grafts
• A number of techniques have been suggested to achieve total arterial revascularization as complete as possible using the RIMA &/or the Radial A. either as free or composite grafts to the in-situ LIMA as T or Y graft.
• The issue of which arterial conduit is the next best choice for surgical revascularization and how to use them to achieve total arterial revascularization has been studied and debated.
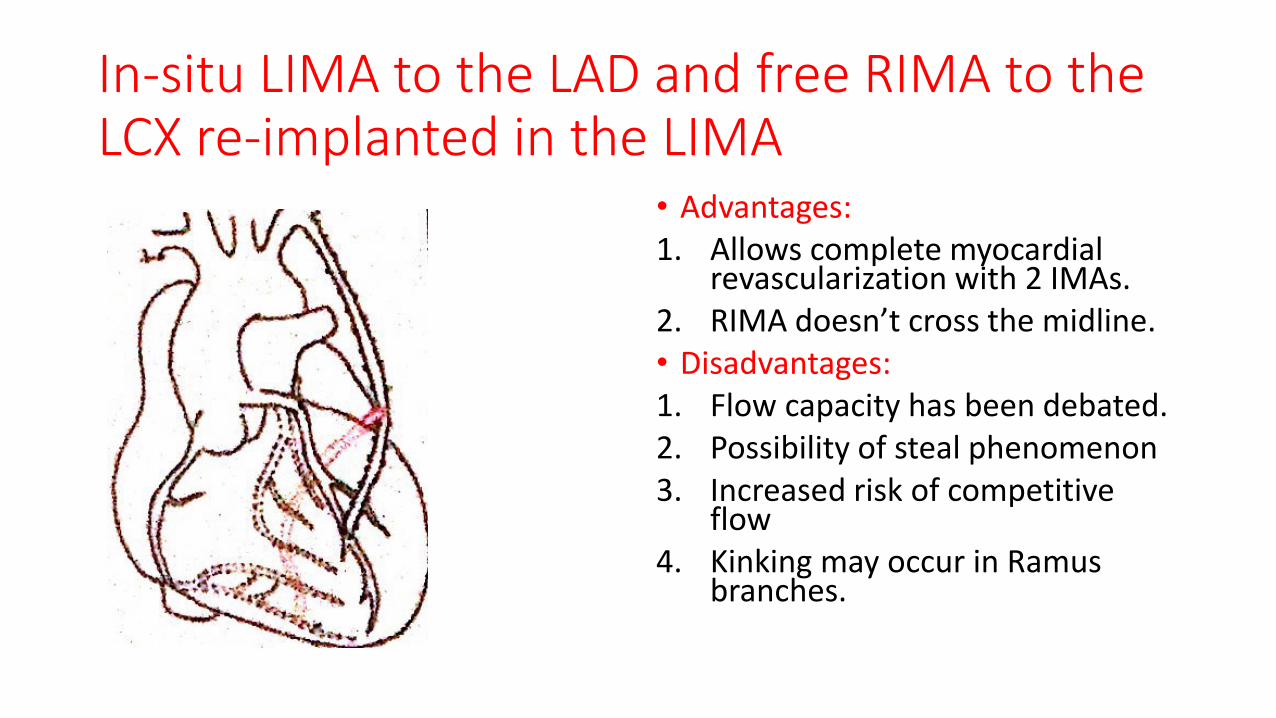
In-situ LIMA to the LAD and free RIMA to the LCX re-implanted in the LIMA
• Advantages: 1. Allows complete myocardial
revascularization with 2 IMAs. 2. RIMA doesn’t cross the midline. • Disadvantages: 1. Flow capacity has been debated. 2. Possibility of steal phenomenon 3. Increased risk of competitive
flow 4. Kinking may occur in Ramus
branches.
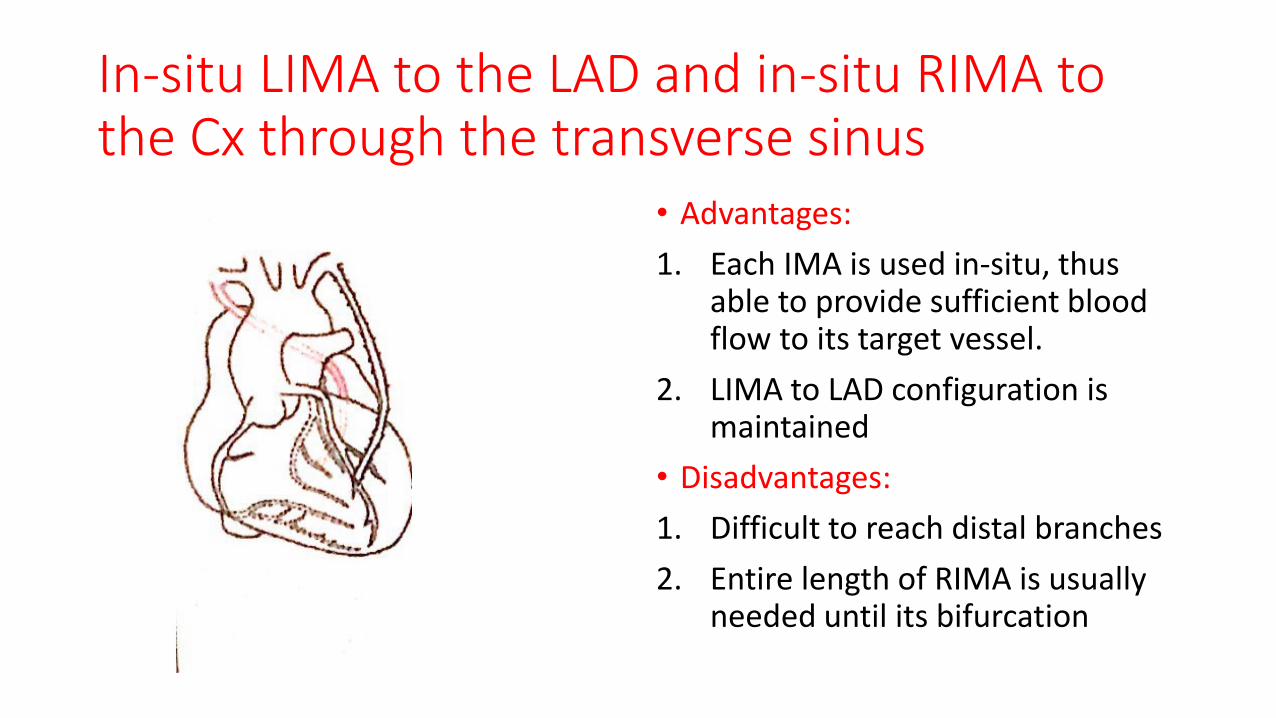
In-situ LIMA to the LAD and in-situ RIMA to the Cx through the transverse sinus
• Advantages:
1. Each IMA is used in-situ, thus able to provide sufficient blood flow to its target vessel.
2. LIMA to LAD configuration is maintained
• Disadvantages:
1. Difficult to reach distal branches
2. Entire length of RIMA is usually needed until its bifurcation
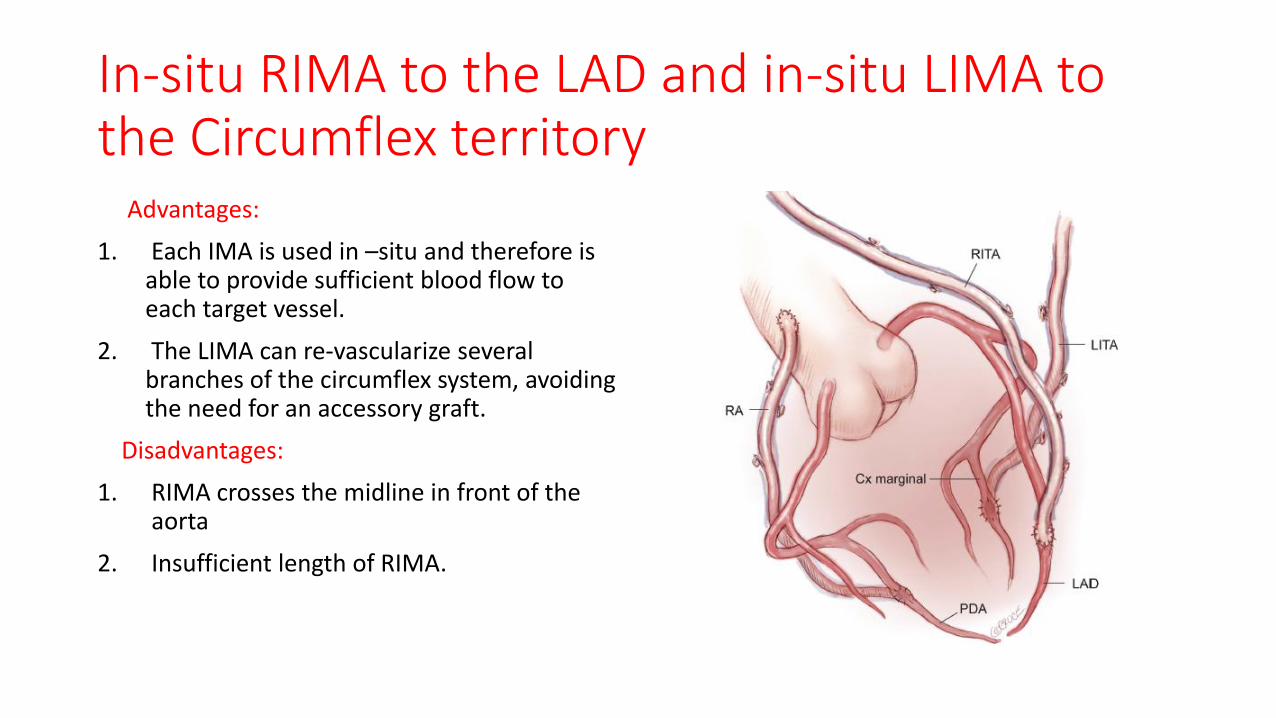
In-situ RIMA to the LAD and in-situ LIMA to the Circumflex territory Advantages:
1. Each IMA is used in –situ and therefore is able to provide sufficient blood flow to each target vessel.
2. The LIMA can re-vascularize several branches of the circumflex system, avoiding the need for an accessory graft.
Disadvantages:
1. RIMA crosses the midline in front of the aorta
2. Insufficient length of RIMA.
In-situ LIMA to the LAD and free RIMA implanted in the aorta: Advantages:
1. allows multiple anastomoses on the lateral wall of the heart using the RIMA.
2. two in-flows ensure that all territories re-vascularized by BIMA receive sufficient blood flow
3. risk of flow competition is decreased.
Disadvantages:
1. patency of RIMA when re-implanted on the aorta is questionable.
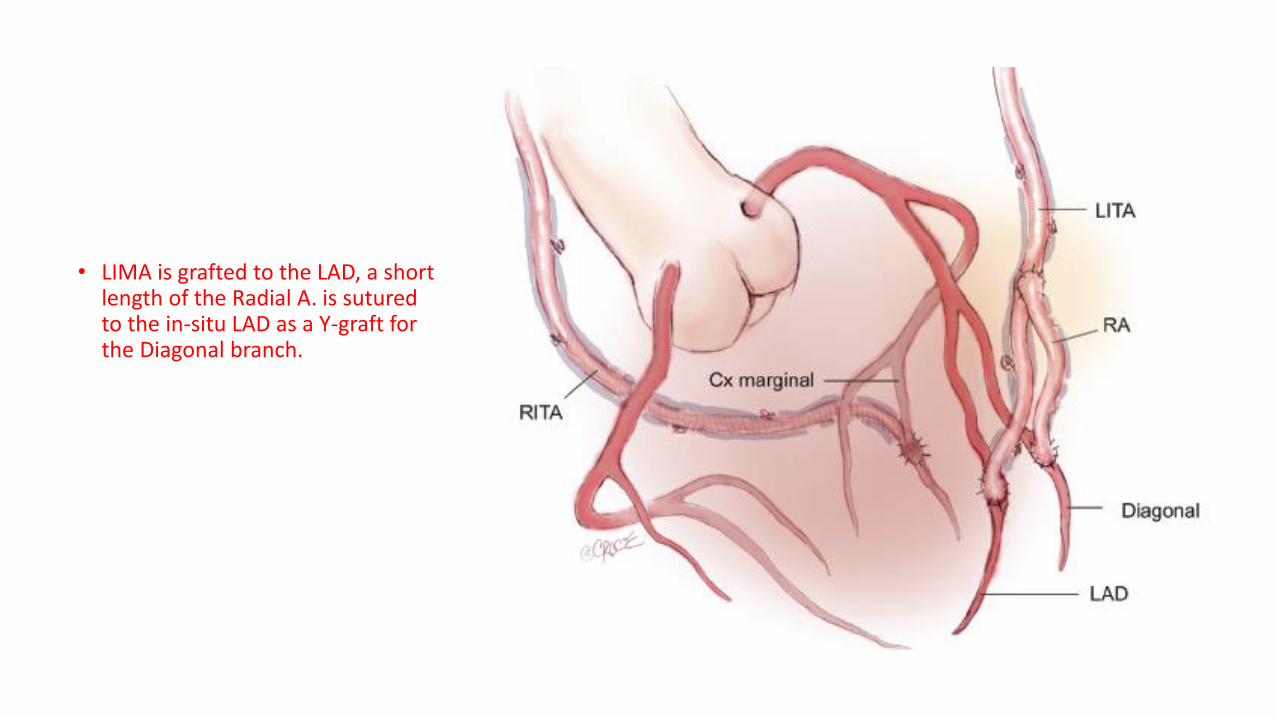
• LIMA is grafted to the LAD, a short length of the Radial A. is sutured to the in-situ LAD as a Y-graft for the Diagonal branch.
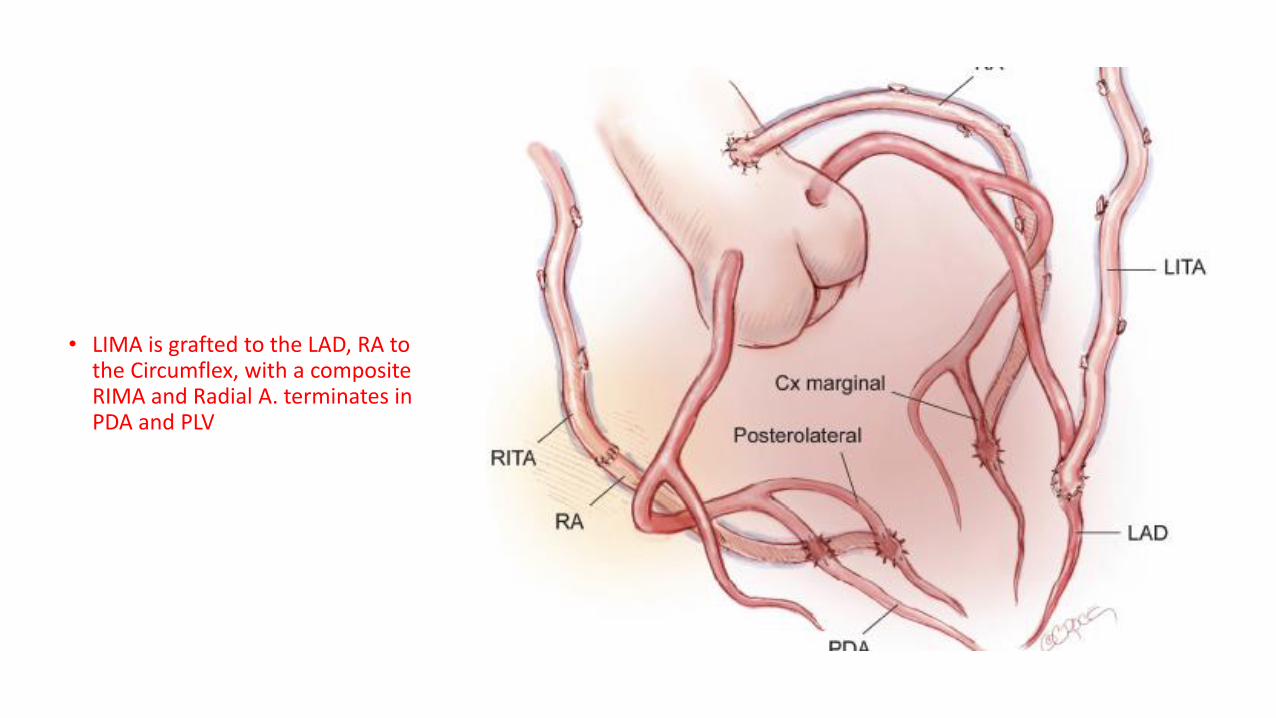
• LIMA is grafted to the LAD, RA to the Circumflex, with a composite RIMA and Radial A. terminates in PDA and PLV
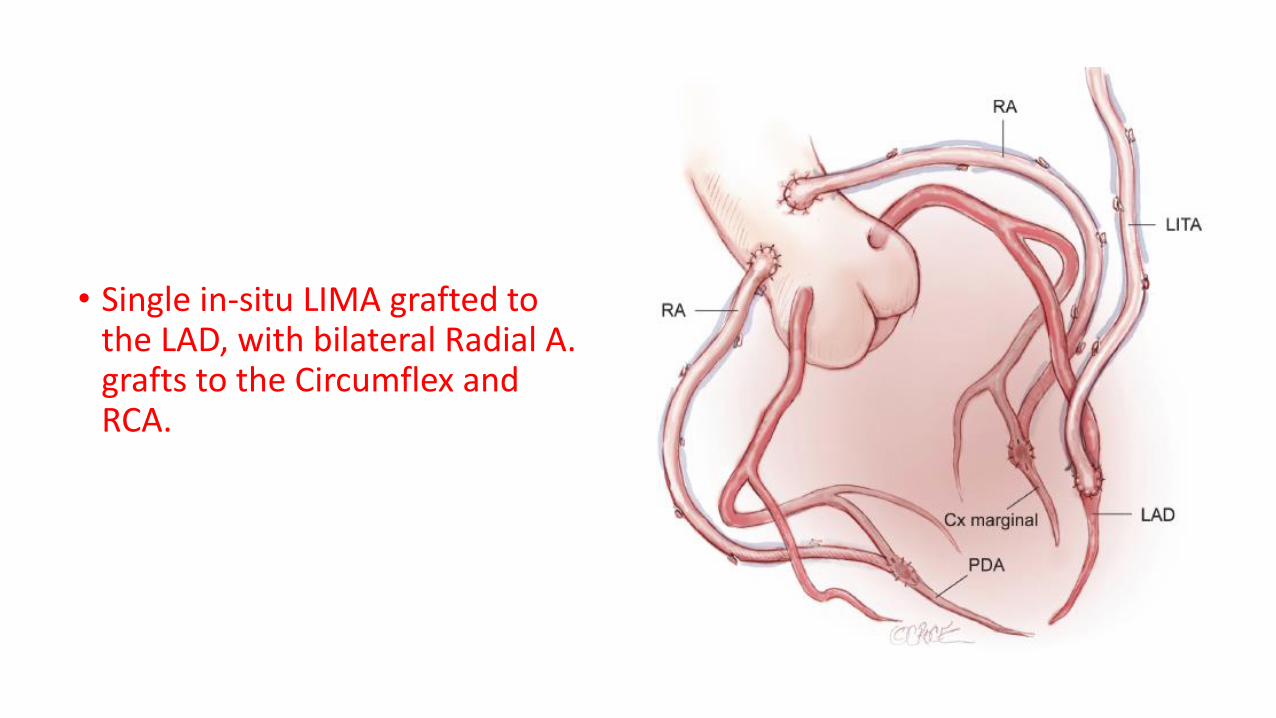
• Single in-situ LIMA grafted to the LAD, with bilateral Radial A. grafts to the Circumflex and RCA.
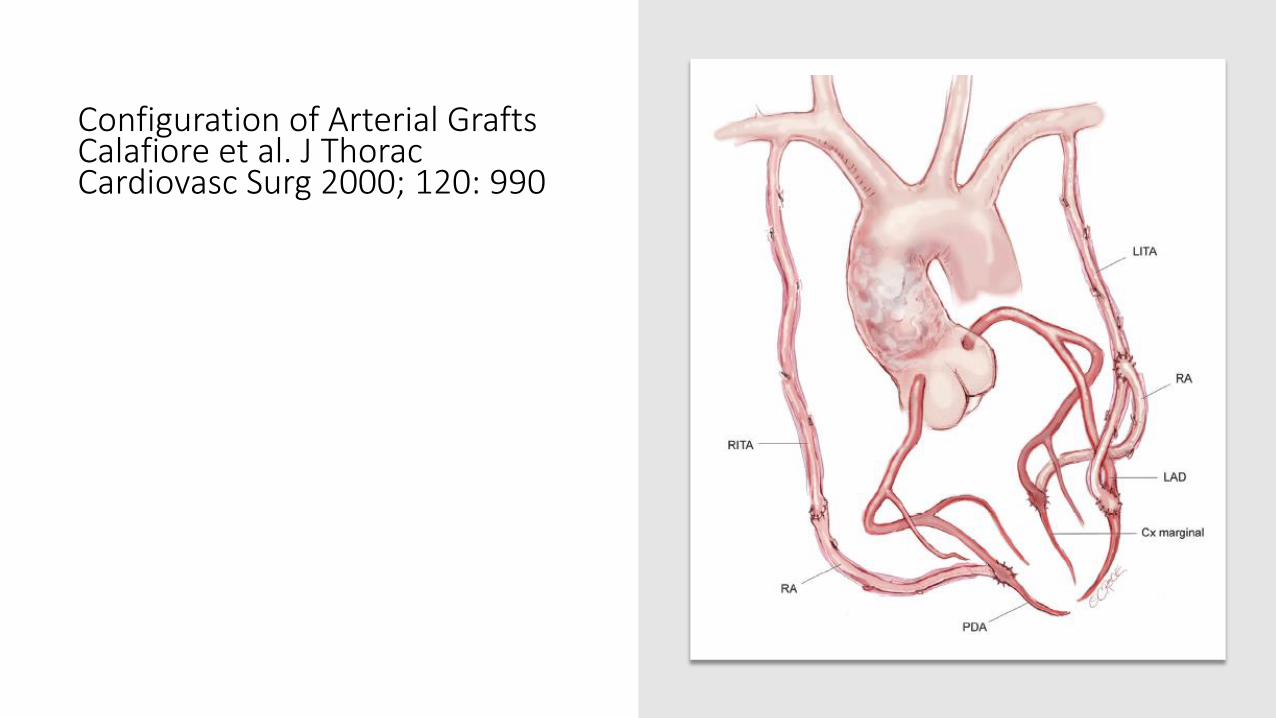
Configuration of Arterial Grafts Calafiore et al. J Thorac Cardiovasc Surg 2000; 120: 990
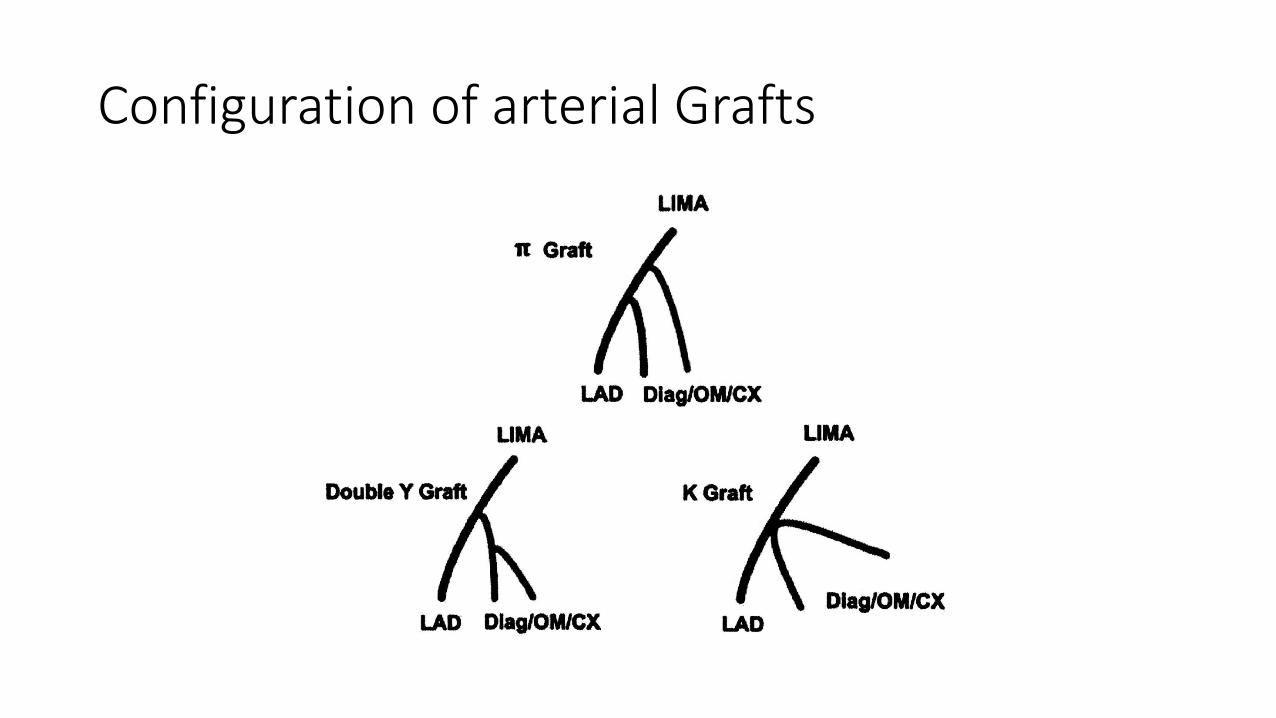
Configuration of arterial Grafts
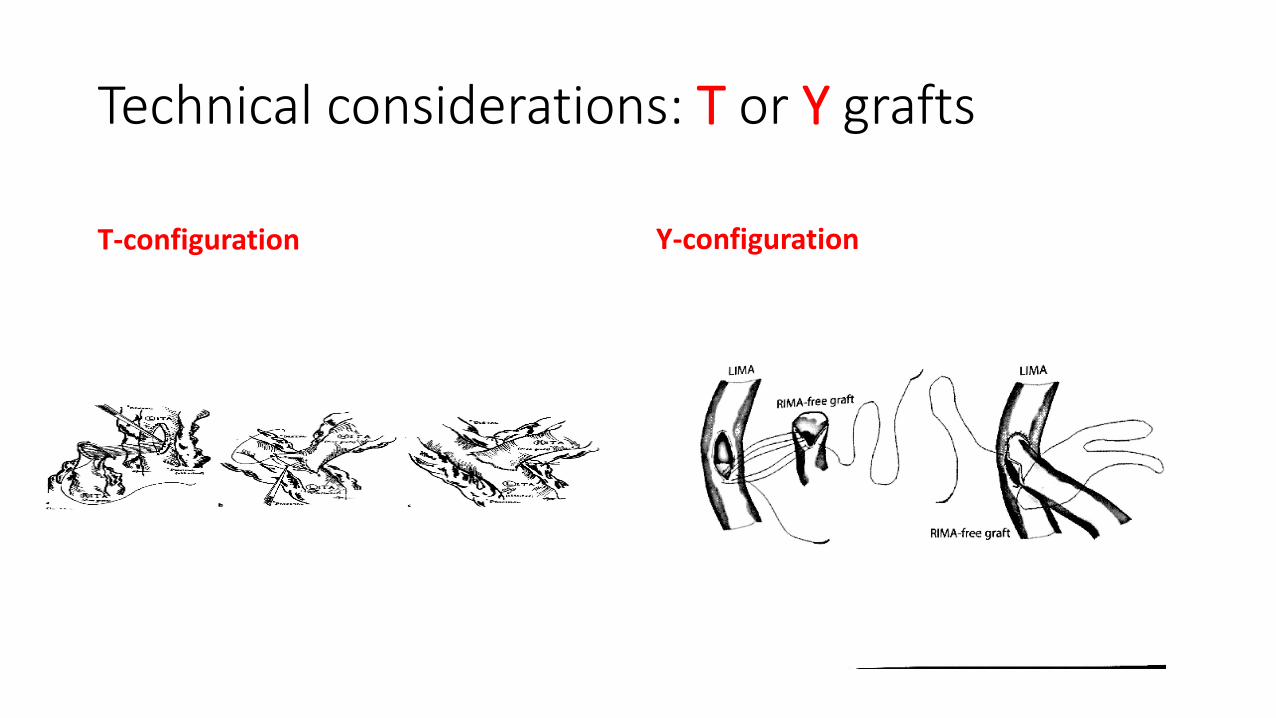
Technical considerations: T or Y grafts
T-configuration Y-configuration
Technical considerations: T or Y grafts
Construction of the T/Y anastomosis:
1. The T/Y graft can be constructed before placing the patient on CPB to reduce the pump time and to allow for measurement of the flow in the limbs of the grafts.
2. The composite anastomosis can also be performed while the patient is on CPB after constructing all distal anastomoses. This may be safer to precisely determine the location of the composite anastomosis without compromising the LIMA flow to the LAD.
Raja et al. Skeletonized bilateral internal mammary arteries for total arterial myocardial revascularization. Heart Lung Circ 2004; 13: 35.
Technical considerations: T or Y grafts
• Y vs T anastomosis:
The site and orientation of the composite anastomosis depends on the presence of an intermediate branch to bypass.
If there is one, a T anastomosis is performed or a Y anastomosis more proximal on the LIMA in order to avoid kinking. Otherwise, a Y anastomosis is performed.
Glineur et al. Bilateral internal thoracic artery graft configuration and coronary artery bypass grafting conduits. Curr Opin Cardiol 2016; 31:625.
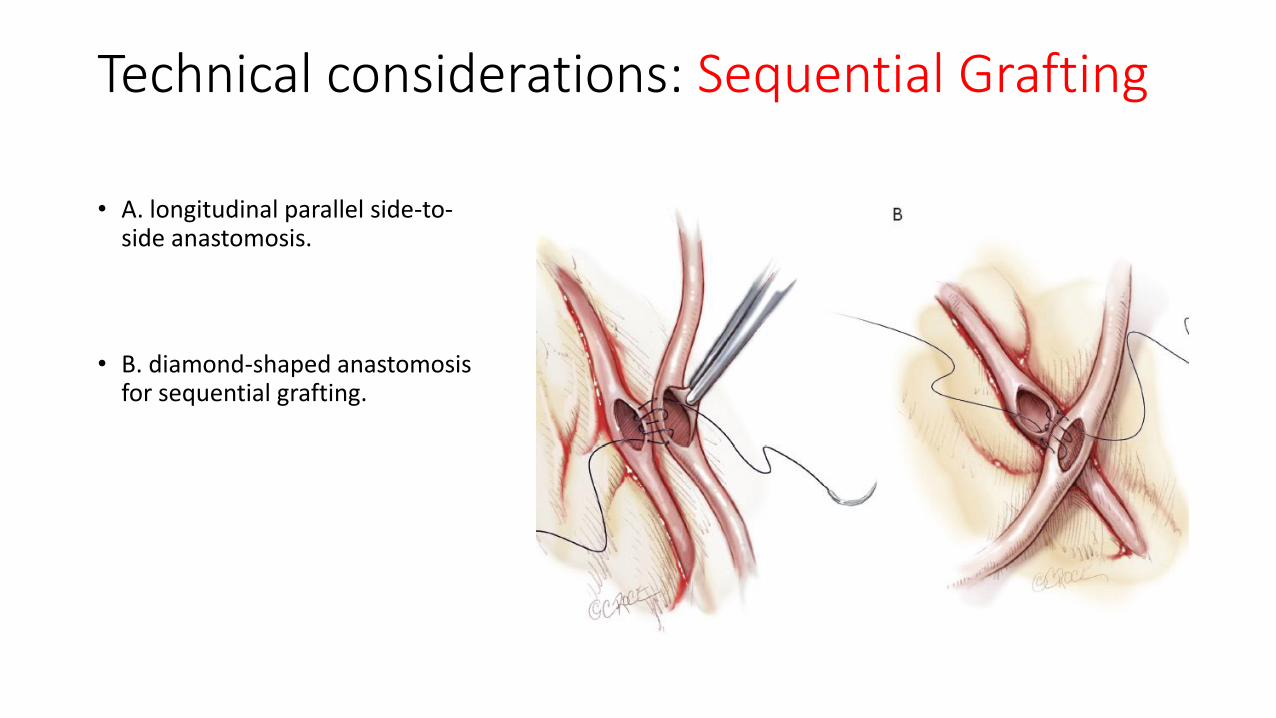
Technical considerations: Sequential Grafting • A. longitudinal parallel side-to-
side anastomosis.
• B. diamond-shaped anastomosis for sequential grafting.

Technical considerations
• Oblique end-to-end anastomosis to minimize stricture and provide extra length.
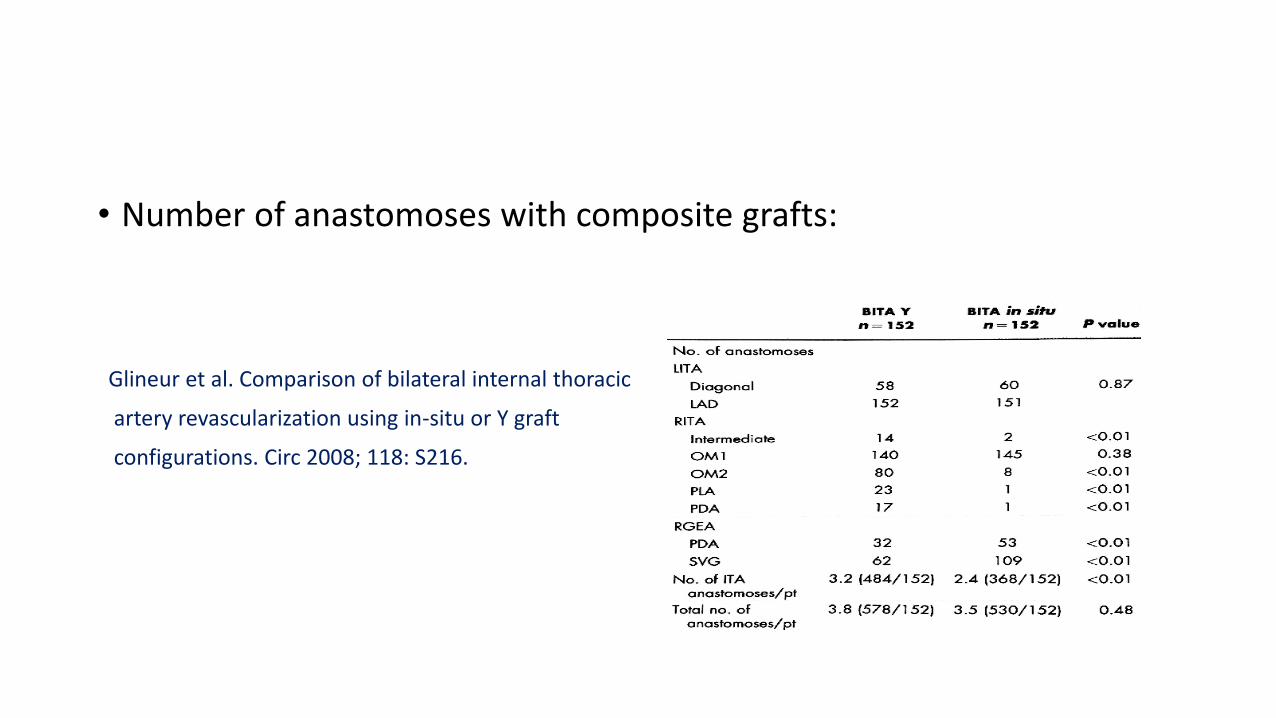
• Number of anastomoses with composite grafts:
Glineur et al. Comparison of bilateral internal thoracic
artery revascularization using in-situ or Y graft
configurations. Circ 2008; 118: S216.
Configuration of Arterial Grafts: Concerns
1
Learning curve
2
Prolonging the operation.
3
Sternal problems
4
Uncertainty as to how best to deploy the second conduit:
Sternal complications: Pedicled vs skeletonized IMA
• Pedicled harvesting of both IMA grafts may impair sternal wound healing by decreasing sternal blood flow, resulting in an increased risk of sternal wound infection and dehiscence.
• Absence of surrounding tissues (muscle, fascia, veins) allows the IMA to increase in both dimensions.
• Skeletonization of IMA allows the preparation of longer conduits with a superior free flow, and can reduce the incidence of postoperative pulmonary and sternal complications.
Composite Arterial Grafts: Single blood source
It has been questioned whether a single IMA can always be a sufficient blood source especially in a composite T or Y graft to 3 territories and about possible steal phenomenon occurring during periods of maximal myocardial blood flow demand.
Royse and colleagues reported that construction of a composite Y graft led to 75% increase of the free flow through a single IMA pedicle and that the composite graft had a considerable potential of flow reserve.
Royse AG, Royse CF, Groves KL, Bus B, Yu G. Blood flow in composite arterial grafts and effect of native coronary flow. Ann. Thorac. Surg 1999; 68(5): 1619.
• Glineur (2005) studied the steal phenomenon by measuring the FFR and the pressure drops in both branches of the composite configuration at rest and during maximal hyperemia.
(Glineur et al. Resistance to flow of arterial Y-grafts 6 moths after coronary artery bypass surgery. Circ 2005; 112(S9): 1281.)
Conclusion: Y-graft allows adequate revascularization of the whole left coronary system with an even distribution of perfusion pressure in both distal branches& minimal resistance to maximal blood flow.
• Mannacio et al (2015) studied complex composite configurations (K, double-Y) and found that multiple composite grafts while adequate at rest, were unable to meet flow requirements during maximal hyperaemia (interact Cardiovasc Thorac Surg 2015; 20: 60).
• Pevni et al (2007) concluded that composite T-grafting or Y-grafting with two IMAs should be reserved for patients with severe stenoses in the LAD and Circumflex arteries.
Composite Arterial Grafts: competitive flow
• In the composite graft, the mechanism of competitive flow is more complex than that in the individual graft as it is not caused only by the association between the graft and its target coronary branch where competitive flow occurs, but also by the interactions of all anastomosed branches within the composite graft.
• It is probably wise to avoid using composite arterial grafts on moderately stenotic coronaries.
Nakajima H et al. 10-year angiographic follow-up of competitive flow in sequential and composite arterial grafts. Eur J Cardiothorac Surg 2011; 40: 399.
Composite Arterial Grafts: Hypo-perfusion syndrome • Spasm of the proximal IMA in composite grafts may result in hypo-
perfusion of the whole left coronary system (1-2%), further, the RA being a muscular artery with high propensity to spasm if not treated properly.
• The hypo-perfusion syndrome is attributed to injury to the conduit during harvest, technical errors in the anastomosis, tension on the conduit, angulation at the anastomotic site and unresolved harvest spasm.
• Strategies: Meticulous attention to conduit harvesting, construction of the anastomosis in addition to flow measurement using TTFM.
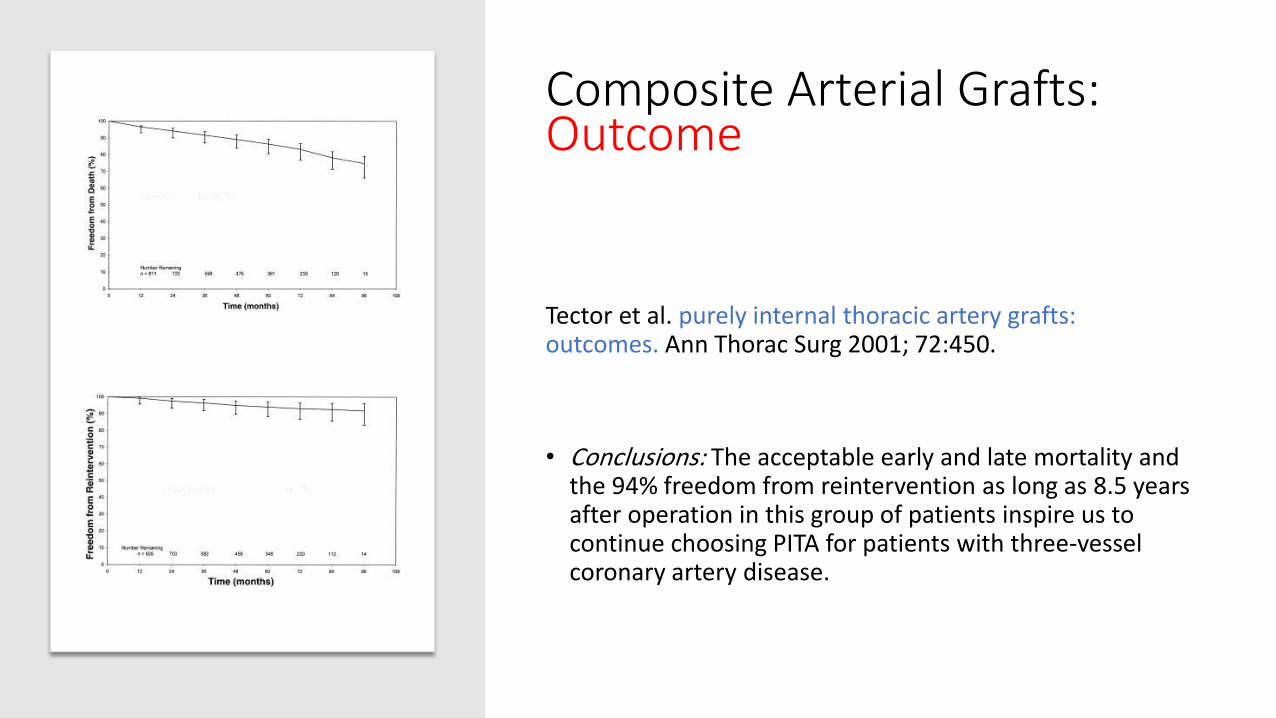
Composite Arterial Grafts: Outcome
Tector et al. purely internal thoracic artery grafts: outcomes. Ann Thorac Surg 2001; 72:450.
• Conclusions: The acceptable early and late mortality and the 94% freedom from reintervention as long as 8.5 years after operation in this group of patients inspire us to continue choosing PITA for patients with three-vessel coronary artery disease.
RIMA In-situ vs Composite grafts: Outcome
• Calafiore studied a total of 2072 patients (1308 with in-situ grafts vs 764 with Y grafts)with no significant difference between both groups.
Conclusion: the Y group gave the same early & late clinical & angiographic results as BIMA in-situ, but the Y graft can provide a higher number of anastomoses.
RIMA In-situ vs Composite grafts: Outcome
• Glineur et al (Circ Cardiovasc Interv 2016): Bilateral Internal Thoracic Artery configuration for Coronary Artery Bypass Surgery. A prospective randomized trial.
• They compared the 2 most commonly used configurations for the RIMA.
Conclusions: 3-year angiographic follow-up revealed no significant difference in graft patency between the 2 BITA configurations. However, compared with in-situ configuration, the use of BITA in a Y configuration results in lower rates of major adverse cardiovascular and cerebrovascular events.
RIMA In-situ vs Composite grafts: Outcome
• Shi et al. Are all forms of total arterial revascularization equal? A comparison of single versus bilateral internal thoracic artery grafting strategies. (J Thorac Cardiovasc Surg 2015; 150: 1526).
• Conclusion: The use of bilateral IMAs as an in-situ or free conduit is associated with greater survival and offers a prognostic advantage over the use of only a single IMA supplemented by RAs.
Composite Arterial Grafts: Outcome
• Bilateral internal thoracic artery grafting: Does graft configuration affect outcome?
• Magreuder et al . J Thorac Cardiovasc Surg 2016; 152: 120.
• 4 groups were studied:
1. In-situ-LIMA (LAD) with in-situ RIMA (LCX).
2. In-situ LIMA (LAD) with in-situ RIMA (RCA).
3. In-situ RIMA (LAD) with in-situ LIMA (LCX).
4. In-situ LIMA (LAD) with free RIMA
Conclusion: BIMA graft configuration has no independent effect on need for repeat revascularization or long-term survival.
IMA-RA Composite Grafts: Outcome
• Muneretto et al evaluated the potential advantages of the use of left internal thoracic artery-radial artery composite grafts compared with conventional coronary artery bypass grafts in elderly patients.
• Conclusion: Left internal thoracic artery-radial artery composite grafts proved to be a safe procedure in elderly patients. It improved the clinical outcome, providing a significantly higher graft patency rate and a lower incidence of late cardiac events.
• Muneretto et al. Left internal thoracic artery-radial artery composite grafts as the technique of choice for myocardial revascularization in elderly patients: a prospective randomized evaluation. J. Thorac. Cardiovasc Surg 2004; 127(1): 179–184.
Configuration of Arterial Grafts: Outcome
• In a recent study by Navia et al comparing patients receiving BITA to patients with LIMA in addition to RA, they found that BIMA experienced better outcomes in terms of recurrent angina, recurrent MI, and mortality. ( J Thorac Cardiovasc Surg 2014; 147:632).
• Rutman et al compared 2 groups: BIMA-SVG and the LIMA-RA-SVG group. They found that the incidence of perioperative major adverse cardiovascular events was significantly lower in the RIMA compared to the RA group (Circulation 2011).
Configuration of Arterial Grafts: Outcome
• Benedetto et al. Right internal thoracic artery versus radial artery as the second best arterial conduit: Insights from a meta-analysis of propensity-matched data on long-term survival. (J Thorac Cardiovasc Surg 2016; 152: 1083).
• Conclusion: The present PSM data meta-analysis suggests that the use of RITA compared with RA was associated with superior long-term survival and freedom from repeat revascularization, with similar operative mortality and incidence of sternal wound complication when the skeletonized harvesting technique was used.
Configuration of Arterial Grafts: Outcome
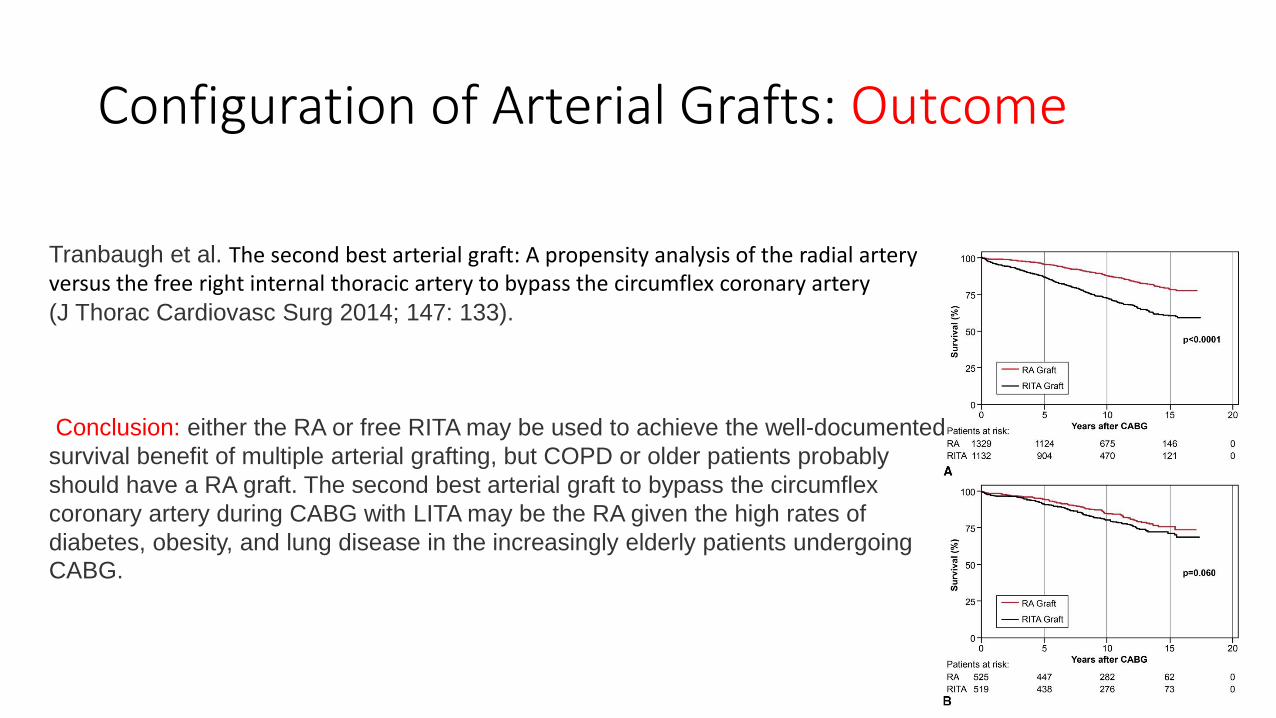
Tranbaugh et al. The second best arterial graft: A propensity analysis of the radial artery versus the free right internal thoracic artery to bypass the circumflex coronary artery (J Thorac Cardiovasc Surg 2014; 147: 133).
Conclusion: either the RA or free RITA may be used to achieve the well-documented
survival benefit of multiple arterial grafting, but COPD or older patients probably
should have a RA graft. The second best arterial graft to bypass the circumflex
coronary artery during CABG with LITA may be the RA given the high rates of
diabetes, obesity, and lung disease in the increasingly elderly patients undergoing
CABG.
Configuration of Arterial Grafts: Outcome
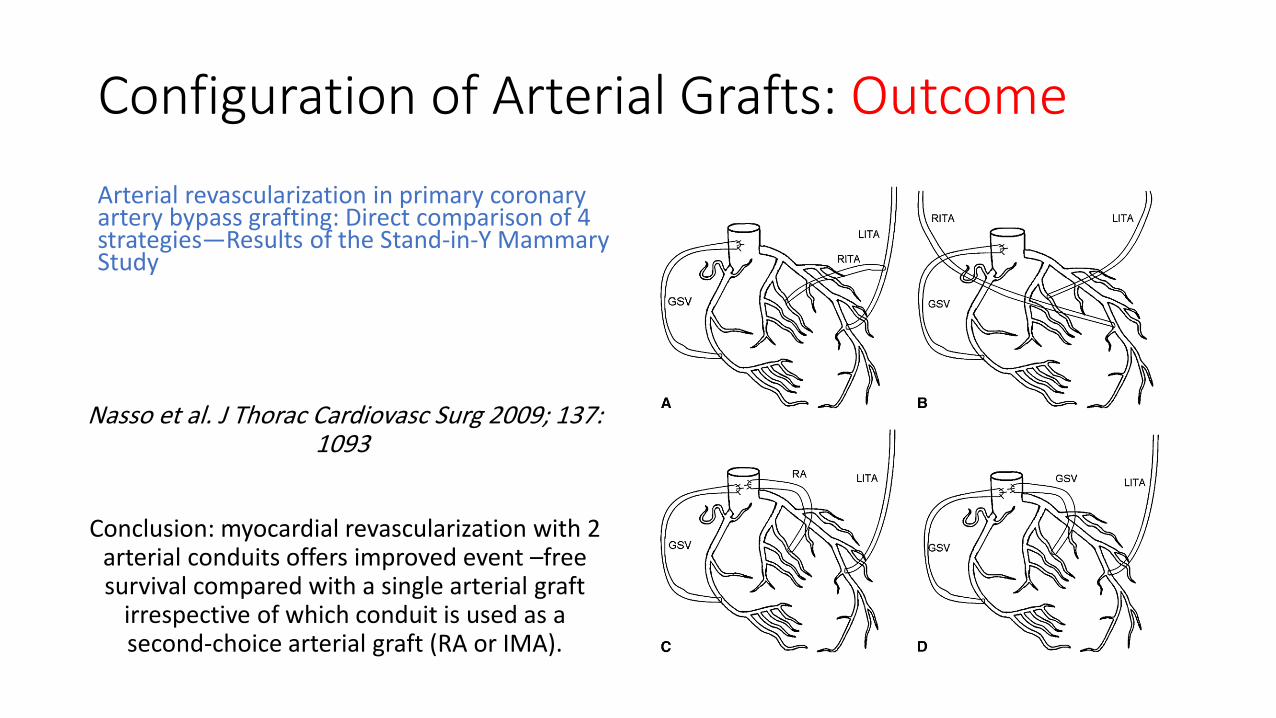
Arterial revascularization in primary coronary artery bypass grafting: Direct comparison of 4 strategies—Results of the Stand-in-Y Mammary Study
Nasso et al. J Thorac Cardiovasc Surg 2009; 137: 1093
Conclusion: myocardial revascularization with 2 arterial conduits offers improved event –free survival compared with a single arterial graft
irrespective of which conduit is used as a second-choice arterial graft (RA or IMA).
Configuration of Arterial Grafts: Summary
1. There is no single approach for utilization of arterial grafts but instead a variety of configurations.
2. Comparative studies between the 2 conduits suggest that the RA contends to the RIMA the role of the second arterial conduit.
3. However, the data suggest that the use of 2 or more arterial conduits (RIMA / RA) is associated with further clinical benefits.
4. Proper patient selection, accurate evaluation of the severity of the coronary lesion is essential before utilizing arterial grafts (FFR may be performed).
Thank You





























