Embed Size (px)
Citation preview

●
dpipsEimAi0nCw©
In
Am4a(Epowc
as
J
K
B
Sss
8
Endothelial Dysfunction and Increased Carotid Intima-MediaThickness in Patients With Autosomal Dominant
Polycystic Kidney Disease
Orhan Kocaman, MD, Huseyin Oflaz, MD, Ensar Yekeler, MD, Memduh Dursun, MD,Dogan Erdogan, MD, Seref Demirel, MD, Sabahat Alisir, MD, Faruk Turgut, MD,
Fehmi Mercanoglu, MD, and Tevfik Ecder, MD
Background: Cardiovascular problems are a major cause of morbidity and mortality in patients with autosomalominant polycystic kidney disease (ADPKD). Endothelial dysfunction (ED) and intima-media thickness (IMT) areredictors for the development and progression of atherosclerosis. In the present study, ED and IMT were
nvestigated in patients with ADPKD. Methods: Fifteen hypertensive and 16 normotensive patients with ADPKD withreserved renal function, 16 patients with essential hypertension, and 24 healthy subjects were included in thetudy. Endothelial function of the brachial artery was evaluated by means of high-resolution vascular ultrasound.ndothelial-dependent dilatation (EDD) was assessed by establishing reactive hyperemia, and endothelial-
ndependent dilatation was determined by using sublingual isosorbide dinitrate. Carotid IMT was measured byeans of high-resolution vascular ultrasound. Results: EDD was significantly worse in hypertensive patients withDPKD compared with patients with essential hypertension (9.1% � 4.1% versus 12.4% � 4.6%; P < 0.05) and even
n normotensive patients with ADPKD compared with healthy subjects (13.1% � 5.2% versus 18.1% � 8.1%; P <.01). Moreover, carotid IMT was significantly greater in both hypertensive (0.71 � 0.10 mm; P < 0.01) andormotensive (0.57 � 0.14 mm; P < 0.001) patients with ADPKD compared with healthy subjects (0.45 � 0.10 mm).onclusion: Both hypertensive and normotensive patients with ADPKD show significant ED and increased IMT,hich are predictors of atherosclerosis. Am J Kidney Dis 43:854-860.2004 by the National Kidney Foundation, Inc.
NDEX WORDS: Endothelial dysfunction (ED); endothelial-dependent dilatation (EDD); carotid intima-media thick-ess (IMT); autosomal dominant polycystic kidney disease (ADPKD).
li
rahhtdciiwpjta((m
ndtl
UTOSOMAL DOMINANT polycystic kid-ney disease (ADPKD) is the most com-
on hereditary renal disease, occurring in 1 of00 to 1,000 individuals.1 It is responsible forpproximately 4% of end-stage renal diseaseESRD) in the United States and 8% to 10% inurope.1 Hypertension, a common finding inatients with ADPKD, often occurs before thenset of renal insufficiency and is associatedith faster progression to ESRD and increased
ardiovascular mortality.2–4 Cardiovascular prob-
From the Departments of Internal Medicine, Cardiology,nd Radiology, Istanbul School of Medicine, Istanbul Univer-ity, Istanbul, Turkey.
Received October 6, 2003; accepted in revised formanuary 6, 2004.
Supported in part by grant no. 2004/3 from the Turkishidney Foundation.Presented in part at the World Congress of Nephrology,
erlin, Germany, June 8-12, 2003.Address reprint requests to Tevfik Ecder, MD, Istanbul
chool of Medicine, Department of Internal Medicine, Divi-ion of Nephrology, Capa, 34390, Istanbul, Turkey. E-mail:[email protected]
© 2004 by the National Kidney Foundation, Inc.0272-6386/04/4305-0011$30.00/0
odoi:10.1053/j.ajkd.2004.01.011
American Journal54
ems are a major cause of morbidity and mortal-ty in patients with ADPKD.4
Activation of the renin-angiotensin-aldoste-one system (RAAS) caused by cyst expansionnd local renal ischemia has been proposed toave an important role in the development ofypertension in patients with ADPKD.5 Stimula-ion of the RAAS starts at an early stage of theisease and precedes hypertension and the majorlinical manifestations of ADPKD.6,7 Increasedntrarenal activity of the RAAS has been shownn both hypertensive and normotensive patientsith ADPKD with normal renal function com-ared with age-matched healthy control sub-ects.6,7 The RAAS has a significant impact onhe development of target-organ damage, such astherosclerosis, left ventricular hypertrophyLVH), and ESRD.8–10 Endothelial dysfunctionED) is an early manifestation of vascular injury,ediated to some degree by angiotensin II.11
During the past decade, a noninvasive tech-ique has evolved to evaluate flow-mediatedilatation, an endothelial-dependent function, inhe brachial artery after occlusion.12–14 This stimu-us provokes the endothelium to release nitric
xide (NO), with subsequent vasodilation thatof Kidney Diseases, Vol 43, No 5 (May), 2004: pp 854-860

cvbwddcvem
swrv
Ets
s1ptsaA1
vepeaaac
tl(sap
d
ee2wEo
B
aamrscjrtttbAfi
wadmibSwtvinmslggo
bhia
C
ssTBbIcweiwtmca
ENDOTHELIAL DYSFUNCTION IN ADPKD 855
an be imaged and quantitated as an index ofasomotor function.15 Ultrasound imaging of therachial artery during reactive hyperemia is aidely used tool for quantifying endothelium-ependent vasomotion.16 Impaired endothelial-ependent vasomotion is a diffuse disease pro-ess resulting in abnormal regulation of bloodessel tone and loss of several atheroprotectiveffects of the normal endothelium and may be aarker of increased future cardiovascular risk.17
Carotid intima-media thickness (IMT), mea-ured noninvasively by ultrasonography, is aell-established index of atherosclerosis and di-
ectly associated with an increased risk for cardio-ascular disease.18–20
The aim of the present study is to investigateD and carotid IMT in normotensive and hyper-
ensive patients with ADPKD with well-pre-erved renal function.
METHODS
Thirty-one patients with ADPKD were included in thetudy. Fifteen patients had hypertension (blood pressure �40/90 mm Hg in the sitting position or administered antihy-ertensive drugs) and 16 patients were normotensive. Six-een patients with essential hypertension and 24 healthyubjects also were included in the study. Creatinine clear-nces were calculated using the Cockcroft-Gault formula.21
ll patients had creatinine clearances greater than 60 mL/min/.73 m2.
Subjects affected by diabetes mellitus, established cardio-ascular disease, other chronic diseases that could affectndothelial function, a family history of hyperlipidemia, andremature atherosclerosis were excluded. Biochemical mark-rs of thyroid and liver function were within normal range inll subjects. During the testing period, all subjects weresked to keep their normal diet and physical activity levelnd not perform intense physical activity. Written informedonsent was obtained from all subjects included in the study.
Systolic and diastolic blood pressures were measured onhe right arm of subjects in an upright sitting position after ateast 5 minutes of rest using an Erka sphygmomanometerPMS Instruments Ltd, Berkshire, UK) with appropriate cuffize. Two readings were recorded for each individual. Theverage of 2 readings was defined as the subject’s bloodressure.Venous blood samples for biochemical analyses were
rawn after an overnight fast between 8:00 PM and 8:00 AM.Echocardiographic examination was performed using an
chocardiographic system equipped with 2.5-MHz transduc-rs (Vingmed System Five, Oslo, Norway). M-Mode and-dimensional measurements were performed in accordanceith methods recommended by the American Society ofchocardiography.22,23 Cardiac mass was calculated by means
24
f the formula derived by Devereux and Reichek. wrachial Artery MeasurementsEndothelium-dependent dilatation (EDD) of the brachial
rtery after transient ischemia, a noninvasive method tossess endothelial function, was performed according toethods defined by Celermajer et al13 using a high-
esolution ultrasound machine (Vingmed System Five). Allubjects abstained from smoking and consuming caffeine-ontaining drinks for at least 12 hours before testing. Sub-ects were kept in a supine position for 10 minutes in a stableoom temperature between 20°C and 25°C. To best visualizehe brachial artery, the arm was immobilized comfortably inhe extended position, and the brachial artery was scanned inhe longitudinal section 3 to 5 cm above the antecubital fossay using a 10-MHz high-resolution linear-array transducer.fter optimal transducer positioning, the skin was marked
or reference for later measurements, and the arm was keptn the same position throughout the study.
All measurements of brachial artery internal diameterere assessed at end-diastole (timed by the QRS complex)
nd calculated as the average of measurements obtaineduring 3 consecutive cardiac cycles. After baseline measure-ents of the brachial artery were recorded, the cuff was
nflated to 200 mm Hg (or 50 mm Hg higher than systoliclood pressure) for 5 minutes to create forearm ischemia.ubsequently, the cuff was deflated and arterial diameteras measured 60 seconds after deflation. In addition, endo-
helium-independent dilatation (EID), a surrogate marker forascular smooth muscle function, was assessed by measur-ng changes in brachial artery diameter after sublingualitrate administration in all subjects. Ten minutes after EDDeasurement, 5 mg of isosorbide dinitrate was administered
ublingually, and measurements were repeated 3 minutesater. All measurements were performed by a single investi-ator blinded to clinical and biochemical data of the studyroups and were recorded on VHS videotape for subsequentff-line analysis.EDD and EID are expressed as percentage of change in
rachial artery diameter from baseline to after reactiveyperemia and to after sublingual isosorbide dinitrate admin-stration, respectively. Intraobserver variability for brachialrtery measurements was 3%.
arotid IMT MeasurementsBilateral carotid ultrasound was performed on an ultra-
ound system with a high-resolution 10-MHz linear-arraycan head (attached to a standard Vingmed System Five).he common carotid arteries were scanned longitudinally.ulb dilation served as a landmark to indicate the borderetween the distal common carotid artery and carotid bulb.mages were obtained from the distal portion of the commonarotid artery, 1 to 2 cm proximal to the carotid bulb. Imagesere saved and stored on S-VHS videotape. The 2 bright
chogenic lines in the arterial wall were identified as thentima and media lines. Intimal plus medial thickness (IMT)as measured as the distance from the main edge of the first
o the main edge of the second echogenic line. Each measure-ent was repeated 3 times, and the mean of the left and right
ommon carotid arteries was obtained and used for furthernalysis. All scans were performed by the same observer,
ho was blinded to clinical and biochemical data. No
sni2
S
WaPv
gs(anpaAbppcceeN
LtNsstt3Cppcpgaht
03AhsstvsA
ASBSSDC
TTL
m
v
KOCAMAN ET AL856
ubject had atheromatous plaque, localized lesion of thick-ess greater than 2.0 mm, or stenosis in this region. Thentraobserver coefficient of variation for carotid IMT was.6%.
tatistical AnalysesComparison of groups was performed using Mann-hitney U and chi-square tests. Mann-Whitney U test was
pplied to the groups in pairs, for all possible combinations.less than 0.05 is considered statistically significant. All
alues are expressed as mean � SD.
RESULTS
There was no significant difference betweenroups regarding age, sex, body mass index,moking status, renal function, and lipid levelsTable 1). Hypertensive patients with ADPKDnd patients with essential hypertension had sig-ificantly greater systolic blood pressures com-ared with normotensive patients with ADPKDnd healthy subjects. Hypertensive patients withDPKD also had significantly greater diastoliclood pressures compared with normotensiveatients with ADPKD and healthy subjects. Hy-ertensive patients with ADPKD had a signifi-antly greater left ventricular mass index (LVMI)ompared with all other groups. Patients withssential hypertension also had a significantlylevated LVMI compared with healthy subjects.
Table 1. Pati
Hypertensive PatientsWith ADPKD (n � 15)
ge (y) 39.6 � 7.2ex (M/F) 4/11ody mass index (kg/m2) 25.5 � 3.5mokers (n) 2ystolic blood pressure (mm Hg) 138 � 18*iastolic blood pressure (mm Hg) 85 � 11†reatinine clearance (mL/min/1.73 m2)
91 � 29
otal cholesterol (mg/dL) 195 � 23riglycerides (mg/dL) 121 � 37VMI (g/m2) 132 � 23‡
NOTE. To convert creatinine clearance in mL/min to mL/sultiply by 0.02586; serum triglycerides in mg/dL to mmol/L*P � 0.01 versus normotensive patients with ADPKD and†P � 0.005 versus normotensive patients with ADPKD a‡P � 0.02 versus normotensive patients with ADPKD, P
ersus healthy subjects.§P � 0.005 versus healthy subjects.
ormotensive patients with ADPKD had a greater h
VMI compared with healthy subjects. Althoughhis was not statistically significant, P was 0.06.o patient in the groups had been administered
tatins. Five patients were administered angioten-in-converting enzyme (ACE) inhibitors; 4 pa-ients, calcium channel blockers (CCBs); 3 pa-ients, angiotensin-receptor blockers (ARBs); and
patients, a combination of ACE inhibitors andCBs in the hypertensive ADPKD group. Sixatients were administered ACE inhibitors; 3atients, CCBs; 4 patients, ARBs; 3 patients, aombination of ACE inhibitors and CCBs; and 1atient, a �-blocker in the essential hypertensiveroup. No statistically significant difference inntihypertensive use was present between theypertensive ADPKD group and essential hyper-ensive group.
Basal diameter of the brachial artery was 3.4 �.6 mm in hypertensive patients with ADPKD,.1 � 0.5 mm in normotensive patients withDPKD, 3.6 � 0.4 mm in patients with essentialypertension, and 3.5 � 0.6 mm in healthyubjects. It was significantly less in normoten-ive patients with ADPKD compared with pa-ients with essential hypertension (3.1 � 0.5ersus 3.6 � 0.4 mm; P � 0.05). EDD wasignificantly worse in hypertensive patients withDPKD compared with patients with essential
aracteristics
tensive PatientsADPKD (n � 16)
Patients With EssentialHypertension (n � 16)
Healthy Subjects(n � 24)
5.8 � 8.8 40.8 � 4.8 38.1 � 8.87/9 7/9 8/16
3.4 � 4.1 26.0 � 3.2 24.7 � 3.53 4 3
120 � 18 134 � 14* 119 � 1474 � 8 77 � 13 75 � 9
106 � 17 112 � 14 105 � 12
181 � 30 179 � 29 180 � 3099 � 39 115 � 35 114 � 37
108 � 24 111 � 16§ 95 � 17
ly by 0.01667; serum total cholesterol in mg/dL to mmol/L,ply by 0.01129.y subjects.lthy subjects.2 versus patients with essential hypertension, P � 0.0001
ent Ch
NormoWith
3
2
, multip, multihealth
nd hea� 0.0
ypertension (9.1% � 4.1% versus 12.4% �

4APvstj0Aap
tPsn0Fip0
esibicc
taimatabd
aEvttthv
ENDOTHELIAL DYSFUNCTION IN ADPKD 857
.6%; P � 0.05), normotensive patients withDPKD (9.1% � 4.1% versus 13.1% � 5.2%;� 0.05), and healthy subjects (9.1% � 4.1%
ersus 18.1% � 8.1%; P � 0.01). EDD wasignificantly worse even in normotensive pa-ients with ADPKD compared with healthy sub-ects (13.1% � 5.2% versus 18.1% � 8.1%; P �.01). EID was significantly less in patients withDPKD (both hypertensive and normotensive)
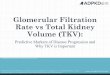
nd patients with essential hypertension com-ared with healthy subjects (Fig 1).Carotid IMT was significantly greater in hyper-
ensive patients with ADPKD (0.71 � 0.10 mm;� 0.01) and patients with essential hyperten-
ion (0.71 � 0.10 mm; P � 0.01) compared withormotensive patients with ADPKD (0.57 �.14 mm) and healthy subjects (0.45 � 0.10 mm;ig 2). Carotid IMT also was significantly greater
n normotensive patients with ADPKD com-ared with healthy subjects (0.57 � 0.14 versus
Fig 1. Results of brachialrtery measurements: (A)DD and (B) EID. *P < 0.05ersus normotensive pa-ients with ADPKD and pa-ients with essential hyper-ension; P < 0.01 versusealthy subjects. **P < 0.01ersus healthy subjects.
.45 � 0.10 mm; P � 0.001). d
DISCUSSION
The RAAS has a detrimental role in the pathogen-sis of target-organ damage, such as atherosclero-is, LVH, heart failure, and ESRD.8–11 The RAASs stimulated at an early stage of ADPKD, evenefore the onset of hypertension and clinical find-ngs.6,7 Thus, increased activity of the RAAS mayontribute to the increased incidence of cardiovas-ular complications in patients with ADPKD.
ED is considered to have an important role inhe pathogenesis of vascular disease.11 An imbal-nce characterized by reduced NO production orncreased reactive oxygen species productionay promote ED.25,26 It has been shown that
ngiotensin II contributes to ED by stimulatinghe production of reactive oxygen species, suchs superoxide, through the activation of mem-rane-bound reduced nicotinamide adenineinucleotide/reduced nicotinamide adenine
27
inucleotide phosphate oxidase.
aislrnnuIsdbdvwomifiIp
hPnshcistlhmn
Ahchht
ApiwalA
htcphAtlhE
tttt(tawp
KOCAMAN ET AL858
Wang et al28 reported that both normotensivend hypertensive patients with ADPKD havempaired endothelial-dependent relaxation ofmall resistance vessels. In that study, acetylcho-ine-induced relaxation rate was decreased inesistance vessels obtained by biopsy of subcuta-eous fat from the gluteal region. In our study, aoninvasive method of high-resolution vascularltrasound was used to determine ED and carotidMT in patients with ADPKD during the earlytages of their disease. Evaluation of endothelium-ependent flow-mediated vasodilatation of therachial artery is a method widely used for theetermination of early atherosclerosis and cardio-ascular risks.13–15 Likewise, carotid IMT is aell-established index of atherosclerosis and thenly noninvasive imaging test currently recom-ended by the American Heart Association for
nclusion in the evaluation of risk.18,29 This is therst study showing ED and increased carotidMT by using these noninvasive methods inatients with ADPKD.In the present study, patients with essential
ypertension and hypertensive patients with AD-KD had significantly less EDD compared withormotensive patients with ADPKD and healthyubjects. This is an expected finding because itas been shown that endothelial function be-omes progressively impaired as blood pressurencreases, and degree of dysfunction is related toeverity of hypertension.30,31 Importantly, hyper-ensive patients with ADPKD had significantlyess EDD compared with patients with essentialypertension with similar blood pressures. Thisay occur because the RAAS is stimulated sig-
ificantly more in hypertensive patients with s
DPKD than in similar patients with essentialypertension.5 Another factor that could haveontributed to the difference in EDD may be thatypertensive patients with ADPKD likely couldave elevated blood pressures for a longer periodhan patients with essential hypertension.
In the present study, hypertensive patients withDPKD had a significantly greater LVMI com-ared with subjects in all other groups. The highncidence of LVH has been reported in patientsith ADPKD.32 Findings of both ED and LVH
re consistent with the high rate of cardiovascu-ar morbidity and mortality in patients withDPKD.All hypertensive patients were receiving anti-
ypertensive therapy. Thus, the direct effect ofhese drugs on vascular function cannot be ex-luded in the present study. Furthermore, bloodressure was lower in patients with essentialypertension than in hypertensive patients withDPKD (134/77 versus 138/85 mm Hg, respec-
ively), although not significant. Therefore, theower blood pressure of patients with essentialypertension may have masked the full extent ofD in this group.An important finding in the present study is
he observation of significant ED, even in normo-ensive patients with ADPKD. Although not sta-istically significant, LVMI also was greater inhese patients compared with healthy subjectsP � 0.06). Previous studies showed signs ofarget-organ damage, such as microalbuminuriand LVH, in normotensive patients with ADPKDith normal renal function.33,34 It also was re-orted that the nocturnal decrease in blood pres-
Fig 2. Measurements ofcarotid IMT. *P < 0.01 versusnormotensive patients withADPKD and healthy subjects.**P < 0.001 versus healthysubjects.
ure is attenuated in normotensive patients with

Aifi
bsfpsAmgp
mamrdaldneeiemhmEsatap
trftdtcAte
inp
rBcAbsttcb
kaW
du
ct
Cd
Td1
cwI
Dtcn
al
ro1
s1
i2
ct
Nd1
ENDOTHELIAL DYSFUNCTION IN ADPKD 859
DPKD.35 Stimulation of the RAAS very earlyn the course of ADPKD may contribute to thesendings.6,7
Wang et al28 found an inverse relationshipetween degree of EDD and mean arterial pres-ure and suggested that impaired endothelialunction may contribute to hypertension in theseatients. Similarly, in our study, the finding ofignificant ED in normotensive patients withDPKD compared with healthy subjects andore severe ED in hypertensive patients sug-
ests that ED may predispose to hypertension inatients with ADPKD.Nitroglycerin is used to determine the maxi-um obtainable vasodilator response and serve
s a measure of EID reflecting vascular smoothuscle function.36 Thus, decreased vasodilatory
esponse to exogenous administration of NOonor suggests smooth muscle dysfunction in therterial wall. Wang et al28 reported that endothe-ium-independent relaxation response to an NO-onor (SIN-1) was similar in hypertensive andormotensive patients with ADPKD, patients withssential hypertension, and control subjects. How-ver, in the present study, vasodilator response tososorbide dinitrate was impaired in patients withssential hypertension and hypertensive and nor-otensive patients with ADPKD compared with
ealthy subjects. This finding suggests smoothuscle dysfunction in these patients. ImpairedID has been reported even in asymptomaticubjects with reduced EDD who are at risk fortherosclerosis.37 Although increased activity ofhe RAAS might have an effect on this finding,dditional studies are needed to understand theathogenesis.Multiple studies have shown that carotid ar-
ery IMT, measured noninvasively by ultrasonog-aphy, is associated directly with increased riskor cardiovascular disease, and it has been showno be an independent predictor of cardiovascularisease after adjustment for traditional risk fac-ors.18 The presence of a significant increase inarotid IMT in normotensive patients withDPKD compared with healthy subjects reflects
he increased cardiovascular risk, even in thearly stages of the disease.
In conclusion, findings of significant ED andncreased carotid IMT in both hypertensive andormotensive patients with ADPKD with well-
reserved renal function suggest that atheroscle-osis starts at a very early stage of the disease.ecause cardiovascular problems are a majorause of morbidity and mortality in patients withDPKD, risk factors for atherosclerosis shoulde treated aggressively. Prospective randomizedtudies are needed to determine the benefits ofhis approach in these patients. Interventionalrials using drugs that block the RAAS or statinsould be of particular importance owing to theireneficial effects on endothelial function.
REFERENCES1. Fick-Brosnahan GM, Ecder T, Schrier R: Polycystic
idney disease, in Schrier RW (ed): Diseases of the Kidneynd Urinary Tract. (ed 7). Philadelphia, PA, Lippincottilliams & Wilkins, 2001, pp 547-5882. Ecder T, Schrier RW: Hypertension in autosomal-
ominant polycystic kidney disease: Early occurrence andnique aspects. J Am Soc Nephrol 12:194-200, 20013. Schrier RW, McFann KK, Johnson AM: Epidemiologi-
al study of kidney survival in autosomal dominant polycys-ic kidney disease. Kidney Int 63:678-685, 2003
4. Fick GM, Johnson AM, Hammond WS, Gabow PA:auses of death in autosomal dominant polycystic kidneyisease. J Am Soc Nephrol 5:2048-2056, 19955. Chapman AB, Johnson A, Gabow PA, Schrier RW:
he renin-angiotensin-aldosterone system and autosomalominant polycystic kidney disease. N Engl J Med 323:1091-096, 19906. Harrap SB, Davies DL, Macnicol AM, et al: Renal,
ardiovascular and hormonal characteristics of young adultsith autosomal dominant polycystic kidney disease. Kidney
nt 40:501-508, 19917. Barrett BJ, Foley R, Morgan J, Hefferton D, Parfrey P:
ifferences in hormonal and renal vascular responses be-ween normotensive patients with autosomal dominant poly-ystic kidney disease and unaffected family members. Kid-ey Int 46:118-1123, 19948. Brunner HR: Experimental and clinical evidence that
ngiotensin II is an independent risk factor for cardiovascu-ar disease. Am J Cardiol 87:3C-9C, 2001
9. Hirsch AT, Pinto YM, Schunkert H, Dzau VJ: Potentialole of the tissue renin-angiotensin system in the pathophysi-logy of congestive heart failure. Am J Cardiol 66:22D-30D,99010. Wolf G: Angiotensin II: A pivotal factor in the progres-
ion of renal diseases. Nephrol Dial Transplant 14:S42-S44,999 (suppl 1)11. Luscher TF: Endothelial dysfunction: The role and
mpact of the renin-angiotensin system. Heart 84:Si20-Si22,000 (suppl 1)12. Anderson EA, Mark AL: Flow-mediated and reflex
hanges in large peripheral artery tone in humans. Circula-ion 79:93-100, 1989
13. Celermajer DS, Sorensen KE, Gooch VM, et al:on-invasive detection of endothelial dysfunction in chil-ren and adults at risk of atherosclerosis. Lancet 340:1111-115, 1992
14. Sorensen KE, Celermajer DS, Spiegelhalter DJ, et al:

NdH
lflC
Cn
t
tC
AmC
Bts
c
tNd
mrm
mt
h
Tod
Io
aJ
taK
nRl
tE1
Ree
GaN
Rfn9
cd3
tsd
Jgv1
mt
KOCAMAN ET AL860
on-invasive measurement of human endothelium depen-ent arterial responses: Accuracy and reproducibility. Breart J 74:247-253, 199515. Corretti MC, Anderson TJ, Benjamin EJ, et al: Guide-
ines for the ultrasound assessment of endothelial-dependentow-mediated vasodilation of the brachial artery. J Am Collardiol 39:257-265, 200216. Barth JD: Which tools are in your cardiac workshop?
arotid ultrasound, endothelial function, and magnetic reso-ance imaging. Am J Cardiol 87:8A-14A, 200117. Celermajer DS: Endothelial dysfunction: Does it mat-
er? Is it reversible? J Am Coll Cardiol 30:325-333, 199718. O’Leary DH, Polak JF: Intima-media thickness: A
ool for atherosclerosis imaging and event prediction. Am Jardiol 90:18L-21L, 200219. Crouse JR III, Craven TE, Hagaman AP, Bond MG:
ssociation of coronary disease with segment-specific inti-al-medial thickening of the extracranial carotid artery.irculation 92:1141-1147, 199520. O’Leary DH, Polak JF, Kronmal RA, Manolio TA,
urke GL, Wolfson SK Jr: Carotid-artery intima and mediahickness as a risk factor for myocardial infarction andtroke in older adults. N Engl J Med 340:14-22, 1999
21. Cockcroft DW, Gault MH: Prediction of creatininelearance from serum creatinine. Nephron 16:31-41, 1976
22. Henry WL, DeMaria A, Gramiak R, et al: Report ofhe American Society of Echocardiography Committee onomenclature and Standards in Two Dimensional Echocar-iography. Circulation 62:212-217, 198023. Sahn DJ, DeMaria A, Kisslo J, Weyman A: Recom-endations regarding quantitation in M-mode echocardiog-
aphy: Results of a survey of echocardiographic measure-ents. Circulation 58:1072-1083, 197824. Devereux RB, Reichek N: Echocardiographic deter-ination of left ventricular mass in man. Anatomic valida-
ion of the method. Circulation 55:613-618, 197725. Drexler H, Hornig B: Endothelial dysfunction in
uman disease. J Mol Cell Cardiol 31:51-60, 199926. Dijkhorst-Oei LT, Stroes ES, Koomans HA, Rabelink
J: Acute simultaneous stimulation of nitric oxide andxygen radicals by angiotensin II in humans in vivo. J Car-iovasc Pharmacol 33:420-424, 199927. Rajagopalan S, Kurz S, Munzel T, et al: Angiotensin
I-mediated hypertension in the rat increases vascular super-
xide production via membrane NADH/NADPH oxidase sctivation. Contribution to alterations of vasomotor tone.Clin Invest 97:1916-1923, 199628. Wang D, Iversen J, Wilcox CS, Strandgaard S: Endo-
helial dysfunction and reduced nitric oxide in resistancerteries in autosomal-dominant polycystic kidney disease.idney Int 64:1381-1388, 200329. Greenland P, Smith SC, Grundy SM: Improving coro-
ary heart disease risk assessment in asymptomatic people.ole of traditional risk factors and noninvasive cardiovascu-
ar tests. Circulation 104:1863-1867, 200130. Dohi Y, Thiel MA, Buhler FR, Luscher TF: Activa-
ion of endothelial L-arginine pathway in resistance arteries:ffect of age and hypertension. Hypertension 16:170-179,99031. Panza JA, Casino PR, Kilcoyne CM, Quyyumi AA:
ole of endothelium-derived nitric oxide in the abnormalndothelium-dependent vascular relaxation of patients withssential hypertension. Circulation 87:1468-1474, 1993
32. Chapman AB, Johnson AM, Rainguet S, Hossack K,abow P, Schrier RW: Left ventricular hypertrophy in
utosomal dominant polycystic kidney disease. J Am Socephrol 8:1292-1297, 199733. Bardaji A, Martinez-Vea A, Gutierrez C, Ridao C,
ichart C, Oliver JA: Left ventricular mass and diastolicunction in normotensive young adults with autosomal domi-ant polycystic kidney disease. Am J Kidney Dis 32:970-75, 199834. Martinez-Vea A, Gutierrez C, Bardaji A, et al: Mi-
roalbuminuria in normotensive patients with autosomalominant polycystic kidney disease. Scand J Urol Nephrol2:356-359, 199835. Valero FA, Martinez-Vea A, Bardaji A, et al: Ambula-
ory blood pressure and left ventricular mass in normoten-ive patients with autosomal dominant polycystic kidneyisease. J Am Soc Nephrol 10:1020-1026, 199936. Ducharme A, Dupuis J, McNicoll S, Harel F, Tardif
C: Comparison of nitroglycerin lingual spray and sublin-ual tablet on time of onset and duration of brachial arteryasodilation in normal subjects. Am J Cardiol 84:952-954,99937. Adams MR, Robinson J, McCredie R, et al: Smoothuscle dysfunction occurs independently of impaired endo-
helium-dependent dilation in adults at risk of atherosclero-
is. J Am Coll Cardiol 32:123-127, 1998