Embed Size (px)
Citation preview

Archives of Disease in Childhood, 1980, 55, 213-217
Fetal thyroid hyperplasia, rhesus isoimmunisation,and amniographyD M 0 BECROFT, W M I SMEETON, AND J H STEWART
Department of Pathology, and Department of Radiology, The National Women's Hospital, Auckland, NewZealand
SUMMARY Thyroid hyperplasia was identified at necropsy in 16 of 70 cases of haemolytic disease ofthe newborn due to rhesus isoimmunisation dying in the years 1959-76. No hyperplasia was foundin the thyroids from 140 nonrhesus-affected infants matched for date of birth, bodyweight andlength, and gestation, or in cases of haemolytic disease born before 1966. All 16 infants with thyroidhyperplasia had received intrauterine transfusions and the iodine-containing contrast media used forpreliminary amniography were the only goitrogenic factors identified. Lipiodol, first used in 1966, wasconsidered to have the greatest effect. The 16 infants with hyperplastic thyroids were less mature andsmaller than 22 infants with normal thyroids who had been similarly exposed to contrast media.The high incidence of hyperplasia may be due to immaturity of the adaptive mechanisms whichallow most normal individuals to escape the goitrogenic effects ofiodine compounds.
In a preliminary report in 1976 we described thefinding of hyperplasia of the thyroid glands in someinfants with haemolytic disease due to rhesusisoimmunisation.1 Thyroid hyperplasia had notpreviously been described in association with thisdisease. All infants had received intrauterinetransfusions, a procedure introduced by Liley at theNational Women's Hospital in 1963.2 We suggestedthat the use of iodine-containing contrast medium forpreliminary amniography (amniofetography) wasthe likely cause of the thyroid abnormality, althoughthere were many other similarly treated infants withnormal thyroids. We have made a more detailedstudy of infants with haemolytic disease dying at thesame hospital between 1959 and 1976.
Material and methods
We reviewed the histology of the thyroid glands of334 rhesus-affected infants examined at necropsy atthe National Women's Hospital between January1959 and April 1976. The majority were stillbirths inwhom tissues were autolysed, but histological
Princess Mary Hospital for Children, AucklandD M 0 BECROFT, pathologistDepartment of Pathology, School of Medicine, University ofAucklandW M I SMEETON, senior lecturerNational Women's Hospital, AucklandJ H STEWART, radiologist
interpretation was possible in glands from 70 cases.A control series of sections of thyroid glands from140 nonrhesus-affected infants was then obtained,2 from each of the 70, matched for gestation (± 1week) and crown to heel length (± 2 cm), these beingthe next 2 liveborn or stillborn infants with well-preserved glands, by name in alphabetical order, ofnecropsies for each year. The sections of all 210thyroid glands were coded and examined 'blind'.Clinical and radiological records and the remaininghistopathological material from the 70 rhesus-affected infants were then reviewed.
Results
Histology of 210 thyroid glands. 194 thyroids wereassessed as normal for gestation and these werefound to include all 140 glands from control infants.Thyroid follicles varied in size but most of them wereround, filled with pale-staining colloid, and lined bycuboidal or flattened cells with uniform nuclei andlittle cytoplasm (Fig. la). 16 glands, all from rhesus-affected infants, showed hyperplasia (Fig. lb and c).Follicles had variable sizes and irregular shapes, andthe lining cells were columnar, many had hyper-chromatic nuclei or were dividing. There were manyintrafollicular papillary projections. Colloid waseither absent or much diminished. The changewas diffuse and there was no nodule formationor inflammatory cell reaction. Some of the
213
on August 17, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.55.3.213 on 1 M
arch 1980. Dow
nloaded from

214 Becroft, Smeeton, and Stewart
S0
Os00
*.8,f
Normal histology S
With hyperplosio 0
0
* 0*0@ w
0
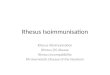
500 1000 1500 2000 2500 3000 > 3500Body weight (g )
Fig. 2 Weights of thyroid glands at necropsy, eachrelated to body weight, of 5 rhesus-affected inifants inwhich thyroid hyperplasia was identified and of 39randomly selected nonrhesus-affected infants with normalthyroid histology.
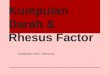
Fig. 1 Photomicrographs of histological sections of(a) a normal neonatal thyroid gland and, (b) and (c)hyperplastic glands from rhesus-affected infants afteramniography x 100.
hyperplastic glands had been visibly enlarged.Latterly, glands were weighed and in Fig. 2 theweights of 5 hyperplastic glands are compared withthose from 40 nonrhesus-affected infants.
Because thyroid hyperplasia had been found onlyin cases of rhesus isoimmunisation, further study wasrestricted to the latter disease.
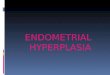
Analysis of 70 rhesus-affected infants. The hyper-plastic glands were from 16 (400%) of 40 infants bornafter 1965 and no hyperplasia was found in 30infants born earlier (Fig. 3). All infants examined in1974-76 had hyperplastic glands.Other data on the infants with and without
thyroid hyperplasia are presented in the Table.Infants with hyperplastic glands were of lessermedian gestation and body size; there was anunexplained male predominance among those withnormal glands; other differences were insignificant.
12
11 -
10-
9'
8.
in 7'
° 6-
Z 5-
Z 4-
3'
With thyroid hyperplasia
With rormol thyroids E
Year
Fig. 3 Incidence of thyroid hyperplasia in 70 infantswith haemolytic disease of the newborn dying between1959 and 1976.
Three possible reasons for thyroid hyperplasiawere investigated.
Maternal factors unrelated to rhesus isoimmunisationThere was no history of thyroid disease or treatmentfor thyroid disease in mothers of infants both withand without thyroid hyperplasia. No drugs withknown effects on thyroid function had been given tomothers in either group. Several drugs had beengiven more often to the mothers of the infants withthyroid hyperplasia but none was common to all.The most common was ampicillin, given pro-phylactically after amniocentesis to I I mothers.
a
0
6-
5-
4-
-3-
or.9a)
2-
0
1-
0 0
I
on August 17, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.55.3.213 on 1 M
arch 1980. Dow
nloaded from

Fetal thyroid hyperplasia, rhesus isoimmatnisation, and amniography 215
Severity ofhaemolytic diseaseAll 16 infants with hyperplastic thyroids hadreceived intrauterine transfusions because theirhaemolytic disease was severe. In comparison 15 ofthe 40 infants without thyroid hyperplasia receivedintrauterine transfusions. 16 others had cord bloodHb <8 0 g/dl and therefore were severely affected,although for various reasons they did not haveintrauterine transfusions.The pathological findings in other organs of the
16 infants with hyperplastic thyroids were thoseexpected in severe haemolytic disease which had beenmodified by intrauterine transfusions-that is, a
variable severity of subcutaneous oedema, effusionsinto serous cavities, visceral and intravascularerythroblastosis, hepatic and splenic haemosiderosis,lipid accumulation in the fetal adrenal cortex, andplacental oedema. However, equally severe changeswere found in a larger number of infants who hadnormal thyroids. Eight infants with thyroid hyper-plasia had hyperplastic islets of Langerhans, but thischange was also found in 12 infants with normalthyroids. Sections of pituitary glands were availablefrom 5 infants with hyperplastic thyroids and no
differences were detected between these and pituita-ries fromrhesus-affectedinfantswith normal thyroids.
Management ofhaemolytic diseaseAll infants with hyperplastic thyroids had receivedat least one intrauterine transfusion. The bloodtransfused is unlikely to have affected thyroidfunction in all cases, whereas the associated radio-logical procedures provide a very likely explanation.The practice at the National Women's Hospital3 is toperform amniography at the first diagnosticamniocentesis with, according to the size of thefetus, 3 to 6 ml of iodised oil (Lipiodol Ultra-fluid,containing 37 to 39% by weight of combined* May and Baker Ltd.
iodine) mixed with 12 to 20 ml of water-solublecontrast medium (76% Urografin,t containing 37%iodine by weight). At the later intrauterine trans-fusion at least 2 ml Urografin was injected into thefetal peritoneal cavity to help in the localisation ofthe catheter. Urografin alone was used for thepreliminary amniography before 1966. Furtherintraperitoneal Urografin was given at subsequenttransfusions, but additional intra-amniotic contrastmedium rarely was required.
Information on the use of contrast media was
available for 68 of the 70 cases. All 16 infants withhyperplastic thyroids had been exposed to contrastmedia in utero compared with 22 infants exposedamong 52 with normal thyroids, a difference unlikelyto have occurred by chance (P<0'025). All infantswith hyperplastic thyroids had been exposed toUrografin, but with one exception there was a
record that this had been in combination withLipiodol. Thus, only one of 10 infants apparentlyexposed to Urografin alone showed thyroid hyper-plasia, compared with 15 cases with hyperplasiafrom 28 infants ex-posed to both Lipiodol andUrografin, a highly s-ignificant-difference (P<0 003)which indicates that the addition of Lipiodol had a
major effect.The reason why only some infants exposed to
contrast media were affected was then considered.
Analysis of 38 infants exposed to contrast media. The16 infants with hyperplastic thyroids were comparedwith the 22 with normal thyroids who had also beenexposed to contrast media in utero (Table).
Severity of diseaseAs expected in cases requiring treatment by intra-uterine transfusions, all had the pathologicalt Schering Chemicals Ltd.
Table Data on 70 infants with haemnolytic disease due to rhesus isoimmunisation
With thyroid hyperplasia With normal thyroids(n= 16)
All infants (n =54*) Infants exposed to contrastmedia (n 22)
Sex: male : female 7:9 38:16 13:9Stillborn 2 7t 4tLiveborn 14 41t 17t
Median Range No.t Median Range No.t Median Range No.t
Maternal age (years) 26 21-36 15 27 20-39 53 27 21-40 22Previous pregnancies 3 1-10 14 3 1-10 53 3 1-8 22Gestation (weeks) 30 28-33 16 35 26-40 50 33 27-37 21Birthweight (kg) 1.60 1-38-2-48 15 2.22 0-814-15 53 2.17 0-81-3-67 21Crown to heel length (cm) 39 34-5-46 16 45 34-53 42 45 34-51 21Age at death (liveborn) (hours) 11 15-6t 14 9-5 0-5-70 t 41 23 0-5-70t 16
*Includes one set of twins, t number with reliable information, $upper limit in days.
on August 17, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.55.3.213 on 1 M
arch 1980. Dow
nloaded from

216 Becroft, Smeeton, and Stewart
features of severe disease and there were nodifferences between the two groups.
Maturity and size of infantsThe infants with hyperplastic thyroids were bornat significantly shorter gestations than those withnormal thyroids (P<0 05) and had correspondinglylower weights and crown to heel lengths.
Number of transfusionsThe number of intrauterine transfusions rangedfrom 1 to 5. A mean of 18 transfusions had beengiven to the 13 cases with hyperplastic thyroids inwhich this information was reliably recorded,compared with a mean of 2 5 transfusions given to15 infants who had normal thyroids.
Dose of contrast mediaAlthough intra-amniotic and intraperitoneal doseswere within the ranges previously quoted, the exactamounts were often not stated and total doses in thetwo groups could not be compared. In the singleexample of hyperplasia believed to follow the use ofUrografin only, the dose of 42 ml was the largestrecorded.
Absorption and dispersal ofmediaThere was insufficient radiologicaJ data to allowcomparison of fetal swallowing and other dispersalofmedia in the two groups.
Duration of exposureIn 12 infants who had thyroid hyperplasia afterLipiodol and Urografin had been used in combina-tion, the median interval between the first amniogramand delivery was 19 days (range 4-70), little differentfrom the median of 20 days (range 3-96) for 12infants with normal thyroids. Delivery was 20 daysafter the first amniogram in the single case withhyperplasia after Urografin alone, compared with amedian of 16 days (range 2-30) in 9 infants withouthyperplasia after Urografin alone.
Discussion
The only constant association found on review ofthese cases of thyroid hyperplasia and rhesusisoimmunisation was that their severe haemolyticdisease required treatment by intrauterine trans-fusions. The thyroid hyperplasia is unlikely to be afurther manifestation of the endocrine abnormalitiesfound in severe haemolytic disease because it wasabsent in an even larger number of severely affectedinfants, and it was not observed in affected infantsbefore 1966. A relationship to a change in medicalmanagement occurring about 1966 appears more
likely. The only change identified was the introduc-tion of Lipiodol Ultra-fluid into amniography, andthe coincidence reinforces the likelihood that thehyperplasia was caused by the goitrogenic effect ofiodine released from the contrast medium andabsorbed either from the fetal gut or perhaps fromthe skin.4
There have been many reports of the induction ofcongenital goitre by iodine-containing compounds,and hypothyroidism has been identified in somesurviving infants. Wolff5 reviewed 25 cases ofcongenital goitre due to maternal ingestion ofinorganic or organic iodine compounds and otherreports of substantial numbers of similar cases havecontinued.6-7 Wolff5 noted the high incidence ofhistological hyperplasia in iodine-induced goitresin the newborn, but his suggestion that this mightoccur frequently at this age from other causes is notborne out by the control series of the study, or byour experience of neonatal thyroid histology ingeneral. Iodides, above a critical dose, inhibithormone formation in the thyroid glands ofman andanimals, the Wolff-Chaikoff effect, the mechanism ofwhich remains uncertain.8 If the effect is prolonged,thyroid enlargement develops because of stimulationby pituitary thyroid-stimulating hormone (TSH).The effect appears to be rapid because the leastdegree of histological abnormality detected in oursurvey was in an infant dying only 4 days afteramniography.Other studies of thyroid function in newborn
infants after amniography support our observationthat Lipiodol has a much greater effect than water-soluble contrast media. RodeEch et al.9 who used12 ml Lipiodol and 30 ml meglumine diatrizoate(Angiografin) found that 6 of 7 infants exhibited apronounced increase in serum TSH levels on the5th day of life, and in 2 cases hypothyroidism ofshort duration was confirmed by the association ofincreased TSH levels with decreased T4 levels. Incontrast Morrison et al.10 found no abnormality ofthe levels of serum T4 and T3-resin-uptake in thecord bloods of 25 infants born after amniographywith Urografin alone. Ranke et al.11 describedgoitre and hypothyroidism in an infant born 3 weeksafter amniography with Lipiodol and a water-soluble contrast medium. Two other cases ofneonatal hypothyroidism were reported afteraccidental injection of contrast media, includingLipiodol, into the fetal subcutaneous tissues duringamniography.12 The greater effect of Lipiodol ismost likely due to its persistence in the amnioticcavity and on the fetal skin until birth, providingcontinuous exposure to iodide, whereas water-soluble media are cleared rapidly. Other factorswhich might be contributory are greater instability
on August 17, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.55.3.213 on 1 M
arch 1980. Dow
nloaded from

Fetal thyroid hyperplasia, rhesus isoimmunisation, and amniography 217
leading to release of more free iodine, greaterabsorption, with or without degradation in the fetalintestine, and differing rates of clearance from thefetal circulation by the placenta.The absence of thyroid hyperplasia in other
infants who were exposed to Lipiodol and Urografinfor a similar time may be due to the well-knownindividual variability in responsiveness to iodine.The mechanism of the usual rapid 'escape oradaption' of hormone secretion from the inhibitoryeffects of excess iodide is poorly understood,8 but it isassociated with a decrease in iodide transport intothe gland. The failure of a minority of individuals toshow such adaption is in part genetically-determined,13 but genetic factors alone are unlikelyto have determined the hyperplastic response foundin 40% of the infants born between 1966 and 1975.Glands stimulated by TSH are more sensitive to theWolff-Chaikoff effect, and blood TSH levels are highduring the latter half of pregnancy.14 Immaturity ofthe adaptive response is another possible explanationwhich is supported by the lesser gestations of thoseinfants who did have a hyperplastic response. Thealternative explanation, that the smaller size of theseinfants was a reflection of a greater dose of contrastmedium relative to body weight, could not beexamined in detail because of lack of data on thequantities of contrast media used. Since, on average,the infants with normal thyroids received moretransfusions than those with hyperplasia a dose-related effect is unlikely, but the number oftransfusions is irrelevant if Lipiodol is the majorfactor and is given only at the first transfusion. Allthyroid glands studied in the years 1974-76 werehyperplastic, causing suspicion of a high free-iodinecontent of batches of media in use at that time, butno further information could be obtained.Although histological changes were impressive,
the enlargement of the thyroid glands of our caseswas slight in comparison with the massive goitreswhich have developed after prolonged maternalingestion of iodides, and there was none of theanatomical consequences of such enlargement. Theconsequences of hypothyroidism, however transient,are more difficult to assess. The deaths of all infantswere adequately accounted for by the severity oftheir haemolytic disease or the effects of prematurity.Nevertheless, hypothyroidism would suppress
bilirubin conjugation in surviving infants and theeffects on the nervous system and other develop-mental processes are unpredictable. Amniofeto-graphy with Lipiodol provides valuable informationfor the management of severe haemolytic disease andin other clinical situations, but a further assessmentof the consequences on thyroid function is necessarybefore the procedure can be regarded as withoutharmful effects on the fetus.
References
Becroft D M 0, Stewart J H, Smeeton W M I. Letter:Rhesus sensitisation, amniography, and thyroid hyper-plasia. Lancet 1976; 2: 1191-2.
2 LileyA W. Intrauterine transfusion offoetus in haemolyticdisease. Br MedJ 1963; fl: 1107-9.
3 Stewart J H. Further observations on the radiology ofintrauterine foetal blood transfusions. Australas Radiol1969; 13: 205-10.
4 Chabrolle J P, Rossier A. Goitre and hypothyroidism inthe newborn after cutaneous absorption of iodine.Arch Dis Child 1978; 53: 495-8.
5 Wolff J. Iodide goiter and the pharmacologic effects ofexcess iodide. AmJMed 1969; 47: 101-24.
6 Carswell F, Kerr M M, Hutchison J H. Congenital goitreand hypothyroidism produced by maternal ingestion ofiodides. Lancet 1970; 1: 1241-3.
7 Job J C, Bocquentin F, Canlorbe P. Les goitres dunouveau-n6. Arch Fr Pediatr 1974; 31: 127-36.
8 Vagenakis A G, Braverman L E. Adverse effects ofiodides on thyroid function. Med Clin North Am 1975; 59:1075-88.
9 Rodesch F, Camus M, Ermans A M, Dodion J, Delange F.Adverse effect of amniofetography on fetal thyroidfunction. Am J Obstet Gynecol 1976; 126: 723-6.
10 Morrison J C, Boyd M, Friedman B I, et al. Effects ofRenografin-60 on the fetal thyroid. Obstet Gynecol 1973;42: 99-103.Ranke M, Nothjunge J, Mentzel H. Kongenitale Strumabei einem Fruhgeborenen nach Amniographie. MonatsschrKinderheilkdI 977; 125: 941-3.
12 Denavit M-F, Lecointre Cl, Mallet E, de Menibus Cl,Rossier A. Un accident de l'amniofoetographie: I'hypo-thyroidie. Arch FrPediatr 1977; 34: 543-51.
13 Croughs W, Visser H K A. Familial iodide-inducedgoitre. Evidence for an abnormality in the pituitary-thyroid homeostatic control. JPediatr 1965; 67: 353-62.
14 Fisher D A, Hobel C J, Garza R, Pierce C A. Thyroidfunction in the pre-term fetus. Pediatrics 1970; 46: 208-16.
Correspondence to Dr D M 0 Becroft, PrincessMary Laboratory, Auckland Hospital, Park Road,Grafton, Auckland 1, New Zealand.
Received 5 December 1978
on August 17, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.55.3.213 on 1 M
arch 1980. Dow
nloaded from