Embed Size (px)
Citation preview
Fluid and Electrolyte Fluid and Electrolyte AbnormalitiesAbnormalities

Fluid & ElectrolytesAmount and Composition of Body Fluids-Approximately 60% of typical adult’s weight is fluid -Factors that influence amount of body fluid are:- ( age ,gender ,and body fat )-Body fluids located in two compartments :--Intracellular fluid (ICF) 2/3 of body fluid-Exteracellular fluid (ECF)
ECF divided into:- -Intravascular fluid (the blood within the vessels). About 3L of circulating blood is plasma ,the other 3L is made up of erythrocytes , leukocytes , and thrombocytes .-Interstitial Fluid
surrounds cellsabout 8L in adultslymph is an example of interstitial fluid
-Transcellular fluidabout 1L in total ,the smallest division of ECFcerebrospinal, pleural ,and digestive secretions .
♣ Body fluid moves between the two spaces to maintain equilibrium♣Loss of ECF into a space that doesn’t contribute to equilibrium status is referred as Third- space fluid shift. ♣ early clue of third space fluid shift is decrease in urine output despite fluid intake intravascular fluid -------- ►Third space ►↓Kidney input ►compensatory ↓urine output ►↑pulse ↓BP↑BW►I&O imbalance

1- Osmosis&OsmolalityOsmosis : movement of fluid from region of low solute concentration to the region of high solute concentration through semi-permeable membraneOsmolality: number of dissolved particles contained in a unit of fluid ( which influence the movement of fluid between fluid compartment)Tonicity: the ability of all solute to cause an osmatic deriving force that promotes water movement from one compartment to other Osmotic Pressure : amount of pressure needed to stop the flow of water by osmosis , and determine by concentration Oncotic Pressure : osmotic pressure exerted by protein (albumin) Osmotic Diuresis : occurs when the urine output increase due to the excretion of substances such as glucose ,and manitol.
2- Diffusion : natural tendency of a substance to move from an area of higher concentration to one of lower concentration , doesn’t need energy e.g. Exchange of o2 & co2 between capillaries & alveoli3- Filtration : movement of fluid and electrolytes with or against the concentration but from one compartment to another ( hydrostatic pressure is the deriving force ) 4- Sodium – Potassium Pump : (active Transport) movement of Na & K against the concentration , it implies that energy must be expended
Route of Gain & LossH2o & electrolytes are gained by drinking and eating ,or via intravenous ,subcutaneous, and enteral feeding tubes Loss by
1-Kidneys :Urine output is approximately 1000-2000 ml (1ml/kg/hr)
2-Skin: Sensible =visible , insensible = nonvisible
sweating vary from 0-1000 ml or more every hourfever & exercise evaporate approximately 600ml/day
3-Lungs : loss ↑ with high R.R & depth or both 300-400 ml/ day (insensible)4-G.I tract usual loss about 100 –200 ml/day
Laboratory Tests for Evaluating Fluid Status
Osmolality serum osmolality reflects the concentration of Na inionUrin osmolality reflects the concentratin of urea ,Cr ,& uric acidOsmolality reported as milli osmoles /kg of waterSerum osmolality is 280-300 mosm/kg
Osmolarity reflects the solute concentration per liter (mOsm/L)
SO osmolality is more common in clinical practice
Urine Specific Gravity
measure the kidneys ability to excrete or conserve waterNormal specific gravity is 1.010—1.025Specific gravity is inversely related with urine volume
Blood Urea Nitrogen (BUN)end products of protein metabolism from both muscle & dietary intakeNormal adults range is 10-20 mg/dlBUN increased with GI bleeding ,dehydration ,fever , sepsisBUN decrease with end stage liver diseases, & ↓protein intake ,& starvation

Creatinine The end products of muscle metabolism More specific indicator of renal functionNormal serum creatinine is 0.7-1.5 mg /dl
Hematocrit measure volume percentage of RBCs in whole blood 44%-52% for male39% -47% for female↑cases of dehydration &policy- themia↓ in cases of overhydration and anemia
Urine Sodiumchanges with sodium intakeaffected by circulating blood volumenormal range is 50-220 mEq/24hrs

Homeostatic Mechanism Organs involved in homeostatic mechanism include kidneys heart , adrenal gland, pituitary gland, & parathyroid gland .1-Kidney Function
Normally filter 170 liter of plasma every day to produce about 1.5 L of urine daily .Kidneys maintain normal fluid balance through :regulation of ESF volume by selective secretions or retention of body fluids .regulation of ESF electrolytes by selective retention of needed substance or secretion of unneeded substances regulation of blood PH by retention of H+ ionsexcretion of metabolic wastes & toxic substance.

Heart & Blood Vessels FunctionsHeart & Blood Vessels FunctionsAffect kidney functions ↓cardiac output Affect kidney functions ↓cardiac output
→↓renal perfusion→↓renal perfusionLung FunctionsLung FunctionsRemove approximately 300 ml of water Remove approximately 300 ml of water (↑hyperpnea, and contentious coughing , (↑hyperpnea, and contentious coughing ,
play major role in acid base balance )play major role in acid base balance )Pituitary Functions Pituitary Functions Hypothalamus manufacture ADH and stored Hypothalamus manufacture ADH and stored
in the posterior pituitary gland and in the posterior pituitary gland and released as needed .released as needed .

-Adrenal Function
Aldesteron which secreted from Zona Granulosa ( outer Zona) of the adrenal cortex .It cause Na and H2O retention and ↑K+ losses Cortison secreted from the Zona reticulates of the adrenal cortexProduce water & Na retention but lesser effectiveness
-Para thyroid Functions :Regulate Ca & phosphate balance Parathyroid Hormones influence bone resorption of calciumAbsorption from intestine & re absorption from renal tubules

Other Mechanism : There are another mechanism that contribute to the homeostatic status
Baroreceptors :small nerve receptors detect change in blood pressure ,and transmitted this information to CNScategorized as low pressure and high pressure receptors low pressure located in the cardiac atria (left atrium) High pressure located in the aortic arch & cardiac sinus When atreal BP decreased the low pressure baroreceptor transmit impulses , ↓in impulses will stimulate the sympathetic nervous system includes ↑of heart rate , contractility , ↑Co2 , vasoconstriction & thus ↑ BP

B-Renin-Angiotensine – Aldesteron System :-B-Renin-Angiotensine – Aldesteron System :- Renin is an enzyme released from the kidney under the Renin is an enzyme released from the kidney under the
stimulation of decreased renal blood flow .stimulation of decreased renal blood flow . Renin converts angiotensinogen to more active angiotensin 1Renin converts angiotensinogen to more active angiotensin 1
Angiotensin – converting enzyme is released whithen the lung Angiotensin – converting enzyme is released whithen the lung capillaries , this enzyme converts angiotenssin 1 to the capillaries , this enzyme converts angiotenssin 1 to the final active form Angiotensin Пfinal active form Angiotensin П
C-Thirst C-Thirst
Oral intake is controlled by thirst center in the Oral intake is controlled by thirst center in the hypothalamushypothalamus
Thirst center stimulated by ↓blood volume ,↑serum Thirst center stimulated by ↓blood volume ,↑serum osmolality ,& intracellular dehydrationosmolality ,& intracellular dehydration
Stimulation of thirst center encourage to ↑fluid intakeStimulation of thirst center encourage to ↑fluid intake
D- ADH released from hypothalamus stimulated by ↓blood volume & ↑serum osmolalitycontrol water retention & excretion
E- Atrial Natriuritic Piptide (slide 13-3 0Released from cardiac atria as a responsse to the ↑arterial pressureIt acts in the opposite direction of the Rennin- Angiotensin -Aldesteron System The end results are to ↓BP by vasodilation ↑ urine excretion, &↓ serum osmolality
Fluid Volume Disturbances
1- (Fluid volume Deficit) Hypovolemia-Hypovolemia : is result when water & electrolytes are lost in the same proportion as they exist in the normal body fluids-Dehydration : refer to loss of water alone with increased serum Na+ level
♣ ♣ Clinical Manifestations :Clinical Manifestations : Acute weight lossAcute weight loss Decrease skin turgor , and cold skin Decrease skin turgor , and cold skin Oligurea & concentrated urineOligurea & concentrated urine Postural hyopotension, Weak & rapid pulsePostural hyopotension, Weak & rapid pulse Increased temperatureIncreased temperature Thirst , Nausea , Muscle weakness & crampsThirst , Nausea , Muscle weakness & cramps

♣ ♣ Assessment Diagnostic evaluationAssessment Diagnostic evaluation Health History & Physical examinationHealth History & Physical examination Serum BUN & CreatininSerum BUN & Creatinin Hematocrit level “great than normal”Hematocrit level “great than normal” Urine specific gravity Urine specific gravity Serum electrolytes level Serum electrolytes level
Hypokalemia in case of GI & renal lossHypokalemia in case of GI & renal loss
Hyperkalemia in case of adrenal insufficiencyHyperkalemia in case of adrenal insufficiency
Hypernatremia in case of ↑insensible losses & Hypernatremia in case of ↑insensible losses & diabetic insepedusdiabetic insepedus
♣ Managementtreatment of the causes of FVD should be go with treatment of FVD itselffactors influence the pt fluid needs should be taken in consideration In case of sever or acute FVD IV replacement should be started Isotonic solutions used to treat hypotension resulted from FVDRenal function & hemodynamic status should be evaluated
♣Nursing ManagementMonitor I&O as needed “urine”Monitor V/S, skin turgor , mental status & daily weightExtensive Hemodynamic CVP, arterial pressureMouth care & ↓ irritating fluids
2-Fluid Volume Excess♣ Hypervolemia :Is an isotonic expansion of ECF caused by abnormal retention of water & Na in approximately the same proportion as normal ♣Clinical Manifestations
Edema Distended neck VeinsIncreased BP,CVP ,pulse rateCrackles over the lungs, shortness of breath,& wheezingIncreased body weight & urine output
♣Assessment & Diagnostic Evaluation
Decreased BUN , Creatinin , Serum osmolality & hematocrete because of plasma dilution, &↓protein intakeUrine sodium is increased if kidneys excrete excess fluid CXR may disclosed pulmonary congestion

♣Management Direct cause should be treatedSymptomatic treatment consist of :
Diureticsrestrict fluid & Na intakeMaintained electrolytes balance
Hemodialysis in case of renal impairmentK+ supplement & specific nutrition
♣Nursing Management:Assess breathing , weight ,degree of edema regularlyI & O measurement regularlySmifowler position in case of shortness of breathPatient education
HyponatremiaHyponatremia
FormsForms HypotonicHypotonic
Hypovolemic with loss of isotonic fluid and hypotonic Hypovolemic with loss of isotonic fluid and hypotonic replacementreplacementHypervolemic due to retention statesHypervolemic due to retention statesIsovolemic due to free water overload, SIADH, renal dx, Isovolemic due to free water overload, SIADH, renal dx, hypokalemia (ADH sensitization)hypokalemia (ADH sensitization)
Isotonic or “pseudohyponatremia”Isotonic or “pseudohyponatremia”Occurs with hypertriglyceridemia or hyperproteinemiaOccurs with hypertriglyceridemia or hyperproteinemia
HypertonicHypertonicNon sodium osmotics induce redistribution (glucose, Non sodium osmotics induce redistribution (glucose, mannitol) for each 100mg/dl of glucose over 100 Na is mannitol) for each 100mg/dl of glucose over 100 Na is decreased by 3 mEq/Ldecreased by 3 mEq/L
Hyponatremia, continuedHyponatremia, continued
S/Sx: S/Sx: Neurologic: muscle twitching, hyperreflexia, seizures Neurologic: muscle twitching, hyperreflexia, seizures
and HTNand HTN Salivation, lacrimation, diarrheaSalivation, lacrimation, diarrhea Often asymptomatic if slow until below 120 mEq/L. Often asymptomatic if slow until below 120 mEq/L.
(130 mEq/L if acute) (130 mEq/L if acute)
Treatment: correct underlying disorderTreatment: correct underlying disorder Fluid restrict, Fluid restrict, ++ diuretics diuretics Hypertonic saline to increase level 2-3 mEq/L/hr and Hypertonic saline to increase level 2-3 mEq/L/hr and
max rate 100cc of 5% saline/hrmax rate 100cc of 5% saline/hr
HypernatremiaHypernatremia
Free water deficit or water loss greater Free water deficit or water loss greater than salt loss. Always assoc with hyper than salt loss. Always assoc with hyper osmolar state.osmolar state.Forms:Forms: Hypervolemic: loss of hypotonic fluids with Hypervolemic: loss of hypotonic fluids with
inadequate replacement with hypertonic fluidsinadequate replacement with hypertonic fluids Isovolemic is subclinical hypovolemia seen in Isovolemic is subclinical hypovolemia seen in
diabetes insipidusdiabetes insipidus Hypervolemic usually iatrogenic, also Hypervolemic usually iatrogenic, also
Cushing’s, Conn’s, CAHCushing’s, Conn’s, CAH

Hypernatremia, continuedHypernatremia, continued
S/Sx:S/Sx: Neurologic: restless, seizure, coma, delirium and Neurologic: restless, seizure, coma, delirium and
maniamania Sticky mucus membranes, poor Sticky mucus membranes, poor
salivation/lacrimation, hyperpyrexia, Red swollen salivation/lacrimation, hyperpyrexia, Red swollen tonguetongue
THIRST, weaknessTHIRST, weaknessTreatment: correct underlying disorderTreatment: correct underlying disorder Free water replacement: (0.6 * kg BW) * ((Na/140) Free water replacement: (0.6 * kg BW) * ((Na/140)
– 1). Slow infusion of D5W give ½ over first 8 hrs – 1). Slow infusion of D5W give ½ over first 8 hrs then rest over next 16-24 hrs to avoid cerebral then rest over next 16-24 hrs to avoid cerebral edema. edema.
HypokalemiaHypokalemia
Etiology:Etiology: Intracellular uptake with redistribution seen in acute Intracellular uptake with redistribution seen in acute
alkalosis, inmsulin therapy, and anabolismalkalosis, inmsulin therapy, and anabolism Depletion due to GI losses, renal/diuretics, steroids, Depletion due to GI losses, renal/diuretics, steroids,
and renal tubular acidosisand renal tubular acidosis
S/Sx:S/Sx: Clinical: muscle weakness/fatigue, decreased DTR’s, Clinical: muscle weakness/fatigue, decreased DTR’s,
ileus. Insulin resistance in DMileus. Insulin resistance in DM EKG: low, flat T-waves, ST depression, and U wavesEKG: low, flat T-waves, ST depression, and U waves

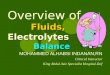
Hypokalemia, continuedHypokalemia, continued
ECG changes in hypokalemiaECG changes in hypokalemia

Hypokalemia, continuedHypokalemia, continued
Treatment:Treatment: Check renal functionCheck renal function Treat alkalosis, decrease sodium intakeTreat alkalosis, decrease sodium intake PO with 20-40 mEq dosesPO with 20-40 mEq doses IV: peripheral 7.5 mEq/hr, central 20 mEq/hr IV: peripheral 7.5 mEq/hr, central 20 mEq/hr
and increase Kand increase K++ in maintenance fluids. in maintenance fluids.

HyperkalemiaHyperkalemia
Etiology:Etiology: Psuedohyperkalemia in leukocytosis, Psuedohyperkalemia in leukocytosis,
hemolysis and thrombocytosishemolysis and thrombocytosis Redistribution in acidosis, hypoinsulinism, Redistribution in acidosis, hypoinsulinism,
tissue necrosis, digoxin poisoningtissue necrosis, digoxin poisoning Renal insufficiency, mineralocorticoid Renal insufficiency, mineralocorticoid
deficiency, DM, spironolactone usedeficiency, DM, spironolactone use
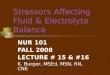
Hyperkalemia, continuedHyperkalemia, continued
S/Sx: S/Sx: Clinical: nausea/vomiting, colic, weakness Clinical: nausea/vomiting, colic, weakness
diarrheadiarrhea EKG: early – peaked T waves then flat P EKG: early – peaked T waves then flat P
waves, depressed ST segment, widened QRS waves, depressed ST segment, widened QRS progressing to sine wave and V fib.progressing to sine wave and V fib.
Cardiac arrest occurs in diastoleCardiac arrest occurs in diastole
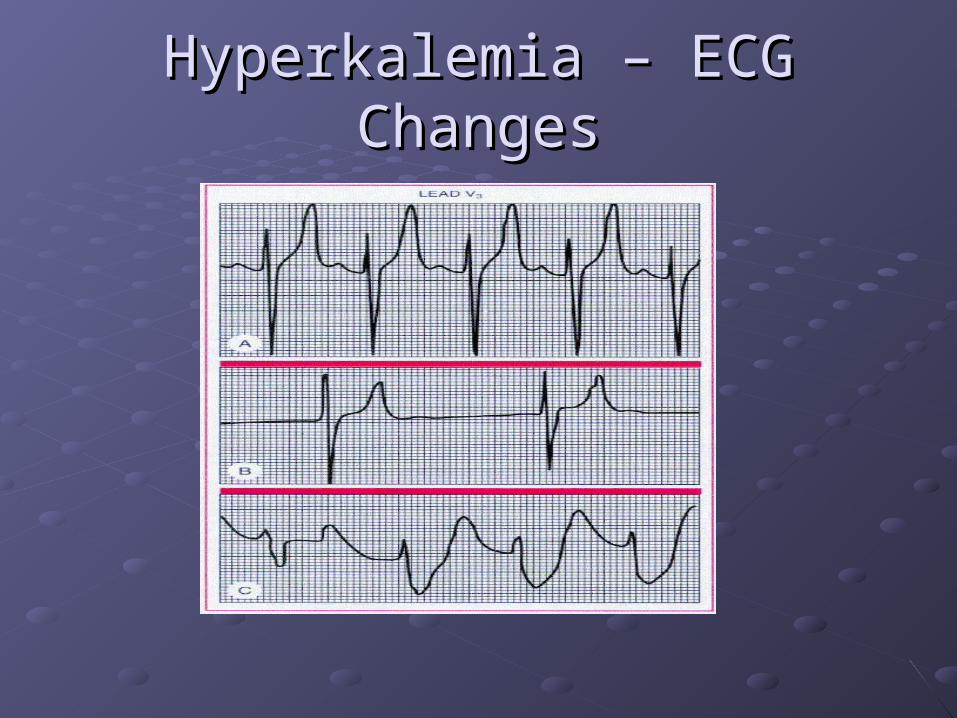
Hyperkalemia – ECG ChangesHyperkalemia – ECG Changes

Hyperkalemia, continuedHyperkalemia, continued
Treatment:Treatment: Remove iatrogenic causesRemove iatrogenic causes Acute: if > 7.5 mEq/L or EKG changesAcute: if > 7.5 mEq/L or EKG changes
Ca-gluconate – 1 gm over 2 min IVCa-gluconate – 1 gm over 2 min IV
Sodium bicarbonate – 1 amp, may repeat in 15minSodium bicarbonate – 1 amp, may repeat in 15min
D50W (1 ampule = 50 gm) and 10U regular insulinD50W (1 ampule = 50 gm) and 10U regular insulin
Emergent dialysisEmergent dialysis Hydration and diuresis, kayexalate 20-50 g, in Hydration and diuresis, kayexalate 20-50 g, in
100-200cc of 20% sorbitol q 4hrs or enema100-200cc of 20% sorbitol q 4hrs or enema

CalciumCalcium
Hypocalcemia:Hypocalcemia: Seen in hypoalbuminemia. Check ionized CaSeen in hypoalbuminemia. Check ionized Ca Often symptomatic below 8 mEq/dLOften symptomatic below 8 mEq/dL Check PTH: Check PTH:
low may be Mg deficiencylow may be Mg deficiencyHigh think pancreatitis, hyperPO4, low Vitamin D, High think pancreatitis, hyperPO4, low Vitamin D, pseudohypoparathyroidism, massive blood transfusion, pseudohypoparathyroidism, massive blood transfusion, drugs (e.g. gentamicin) renal insufficiencydrugs (e.g. gentamicin) renal insufficiency
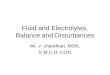
S/Sx: numbness, tingling, circumoral paresthesia, S/Sx: numbness, tingling, circumoral paresthesia, cramps tetany, increased DTR’s, Chvostek’s sign, cramps tetany, increased DTR’s, Chvostek’s sign, Trousseau’s signTrousseau’s sign
EKG has prolonged QT intervalEKG has prolonged QT interval
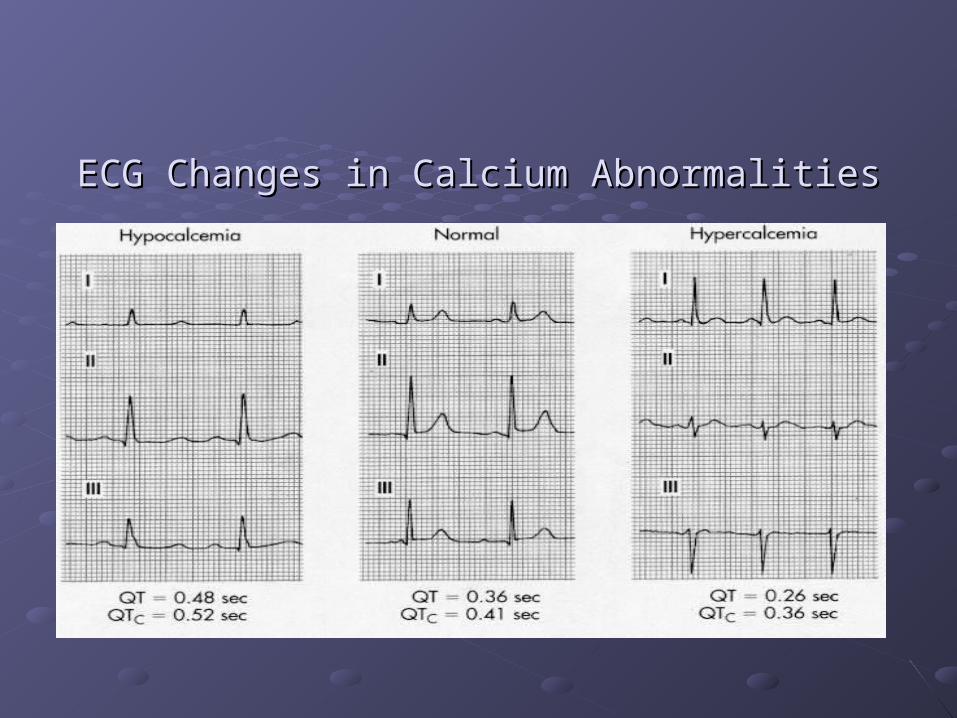
ECG Changes in Calcium AbnormalitiesECG Changes in Calcium Abnormalities

Calcium, continuedCalcium, continued
Hypocalcemia cont.Hypocalcemia cont. Treatment:Treatment:
Acute: (IV) CaCl 10 cc of 10% solution = 6.5 Acute: (IV) CaCl 10 cc of 10% solution = 6.5 mmole Ca or CaGluconate 10cc of 10% solution = mmole Ca or CaGluconate 10cc of 10% solution = 2.2 mmole Ca2.2 mmole Ca
Chronic: (PO) 0.5-1.25 gm CaCOChronic: (PO) 0.5-1.25 gm CaCO33 = 200-500 mg = 200-500 mg
Ca. Ca. Phosphate binding antacids improve GI absorption of CaPhosphate binding antacids improve GI absorption of Ca
Vit D (calciferol) must have normal serum PO4. Vit D (calciferol) must have normal serum PO4. Start 50,000 – 200,000 units/dayStart 50,000 – 200,000 units/day

Calcium, continuedCalcium, continued
HypercalcemiaHypercalcemia Usually secondary to hyperparathyroidism or Usually secondary to hyperparathyroidism or
malignancy. Other causes are thiazides, milk-alkali malignancy. Other causes are thiazides, milk-alkali syndrome, granulomatous disease, acute adrenal syndrome, granulomatous disease, acute adrenal insufficiencyinsufficiency
Acute crisis is serum Ca> 12mg/dL. Critical at 16-Acute crisis is serum Ca> 12mg/dL. Critical at 16-20mg/dL20mg/dL
S/Sx: N/V, anorexia, abdominal pain, confusion, S/Sx: N/V, anorexia, abdominal pain, confusion, lethargy MS changes= “Bones, stone, abdominal lethargy MS changes= “Bones, stone, abdominal groans and psychic overtones.”groans and psychic overtones.”

Calcium, continuedCalcium, continued
Treatment: Hydration with NS then loop Treatment: Hydration with NS then loop diuretic. Steroids for lymphoma, multiple diuretic. Steroids for lymphoma, multiple myeloma, adrenal insufficiency, bone mets, myeloma, adrenal insufficiency, bone mets, Vit D intoxication. May need Hemodialysis.Vit D intoxication. May need Hemodialysis.
Mithramycin for malignancy induced hyperCa Mithramycin for malignancy induced hyperCa refractory to other treatment. Give 15-25 mcg/kg refractory to other treatment. Give 15-25 mcg/kg IVPIVP
Calcitonin in malignant PTH syndromesCalcitonin in malignant PTH syndromes

MagnesiumMagnesium
HypomagnesemiaHypomagnesemia Malnutrition, burns, pancreatitis, SIADH, Malnutrition, burns, pancreatitis, SIADH,
parathyroidectomy, primary parathyroidectomy, primary hyperaldosteronismhyperaldosteronism
S/Sx: weakness, fatigue, MS changes, S/Sx: weakness, fatigue, MS changes, hyperreflexia, seizure, arrhythmiahyperreflexia, seizure, arrhythmia
Treatment: IV replacement of 2-4 gm of Treatment: IV replacement of 2-4 gm of MgSO4 per day or oral replacement MgSO4 per day or oral replacement
Magnesium, continuedMagnesium, continued
HypermagnesemiaHypermagnesemia Renal insufficiency, antacid abuse, adrenal Renal insufficiency, antacid abuse, adrenal
insufficiency, hypothyroidism, iatrogenicinsufficiency, hypothyroidism, iatrogenic S/Sx: N/V, weakness, MS changes, S/Sx: N/V, weakness, MS changes,
hyporeflexia, paralysis of voluntary muscles, hyporeflexia, paralysis of voluntary muscles, EKG has AV block and prolonged QT interval.EKG has AV block and prolonged QT interval.
Treatment: Discontinue source, IV Treatment: Discontinue source, IV CaGluconate for acute Rx, DialysisCaGluconate for acute Rx, Dialysis
PhosphatePhosphate
HypophosphatemiaHypophosphatemia Seen in hyperalimentation, after starvation, Seen in hyperalimentation, after starvation,
DKA, malabsorption, phosphate binding DKA, malabsorption, phosphate binding antacids, alkalosis, hemodialysis, antacids, alkalosis, hemodialysis, hyperparathyroidismhyperparathyroidism
S/Sx: myocardial depression due to low ATP, S/Sx: myocardial depression due to low ATP, shift of oxyhemoglobin curve to left due to low shift of oxyhemoglobin curve to left due to low 2,3 DPG, anorexia, bone pain, hemolysis, 2,3 DPG, anorexia, bone pain, hemolysis, cardiac arrestcardiac arrest

PhosphatePhosphate
Treatment: PO replacement (Neutraphos) or Treatment: PO replacement (Neutraphos) or IV KPhos or NaPhos 0.08-0.20 mM/kg over 6 IV KPhos or NaPhos 0.08-0.20 mM/kg over 6 hrshrs
HyperphosphatemiaHyperphosphatemia Renal insufficiency, hypoparathyroidism, may Renal insufficiency, hypoparathyroidism, may
produce metastatic calcificationproduce metastatic calcification Treat with restriction and phosphate-binding Treat with restriction and phosphate-binding
antacid (Amphogel)antacid (Amphogel)

ZincZinc
1-2 gm in body (brain, pancreas, liver, kidney, 1-2 gm in body (brain, pancreas, liver, kidney, prostate and testis)prostate and testis)Enzyme activator and cofactorEnzyme activator and cofactorDeficiency in malabsorption, trauma, IBD, Deficiency in malabsorption, trauma, IBD, refeeding syndrome, cancer or diarrhea refeeding syndrome, cancer or diarrhea Absorbed in terminal ileumAbsorbed in terminal ileumS/Sx: “4 D’s” – diarrhea, depression, dermatitis, S/Sx: “4 D’s” – diarrhea, depression, dermatitis, dementiadementia Also alopecia, nyctalopia, tremor, loss of tasteAlso alopecia, nyctalopia, tremor, loss of taste
Treat with zinc sulfate 3-6mg/day if with (normal Treat with zinc sulfate 3-6mg/day if with (normal number of stools)number of stools)