Embed Size (px)
DESCRIPTION
rtstdluyf;uy;iu
Citation preview

GASTROINTESTINAL PHYSIOLOGY
DEPARTMENT OF PHYSIOLOGY
FACULTY OF MEDICINE HASANUDDIN UNIVERSITY
MAKASSAR

STRUCTURE
Structure of gastrointestinal system– Gastrointestinal tract; oral cavity,
pharynx, esophagus, stomach, small intestine, large intestine, rectum, and anal canal
– Accessory organs; tounge, teeth, salivary glands, liver, and gall bladder

FUNCTION
Breaking down food and supplying the body with the water, electrolytes, and nutrients to sustain life.
Before can be used, food must be:– ingested– digested– absorbed
All of these processes involve coordinated movement of muscle and secretion of various substances

INGESTION
Placing food into the mouthChewing the food into smaller
pieces (mastication)Moistening the food with salivary
secretionsSwallowing the food (deglutition)

DIGESTION
Food is broken down into small particle by grinding action
Food is degraded by digestive enzymes into usable nutrient– Starches are degraded by amylase into
monosaccharides
– Proteins are degraded by variety of enzymes (pepsin, trypsin) into dipeptides and amino acids
– Fats are degraded by lipases and esterases into monoglyserides and free fatty acids

LEARNING CONCEPT
STRUCTURE
GI TRACT
ORAL CAVITYPHARYNXESOPHAGUSSTOMACHSMALL INTESTINELARGE INTESTINERECTUMANAL CANAL
ACCESSORYORGANS
TONGUETEETHSALIVARY GLANDSPANCREASLIVERGALL BLADDER
FUNCTION
INGESTION
DIGESTION
ABSORPTION
SECRETION
MOVEMENT




MOTILITY OF GI TRACT
The basic mechanisms of GI movement is peristaltis. Peristaltis is a coordinated pattern of smooth muscle contraction and relaxation
Peristaltis helps move food through the pharynx and esophagus and within the stomach. Peristaltis plays a minor role in propelling food through the intestine
During peristaltis, contraction of small section of proximal muscle is followed immediately by relaxation of the muscle just distal to it. The resulting wavelike motion.


Electrical Activity and Regulation of Motility
The smooth muscle of GI tract has spontaneous rhytmic fluctuations (basic electrical rhytm; BER) which is initiated by the interstitial cells of Cajal
The rate of BER is 4/min in the stomach, 12/min in duodenum and fall to about 8/min in distal ileum
Spike potensials playing important role in BER Ionic basis of spike potentials is due to Ca2+ influx,
and K+ effluxMany neurotransmitter and hormone affect the
BER. Acetylcholine increases BER and Epinephrine decrease BER

Basic Electrical Activity (BER) of Gastrointestinal Sooth Muscle

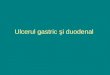
Migrating Motor Complex
Modification of motor activity during fasting between periods of digestion
Each cycle of this activity starts with quiescent period (phase I), continues with period of irregular activity (phase II), and ends with a burst of regular activity (phase III)
MMCs migrate at a rate of about 5 cm/min, with interval of 90 minutes
The function of MMC is to clear the stomach and small intestine luminal contents in preparation of the next meal
MMC immediately stopped by ingestion

Migrating Motor Complexes
Meal
90 minute
III
IIIStomach
DistalIleum
Propagatianrate 5cm/min

MASTICATIONFunction of Mastication
Breaks food into smaller pieces, which:– Makes it easier for the food to be
swallowed– Breaks off the undigestible cellulose
coatings of fruits and vegetables– Making easier for food to be digested
by digestive enzymes

MASTICATIONFunction of Mastication
Mixes the food with salivary gland secretions, which:– Initiates the process of starch digestion
by salivary amylase– Initiates the process of lipid digestion
by lingual lipase– Lubricates and softens the bolus of
food, making it easier to swallow

MASTICATIONFunction of Mastication
Brings food into contact with taste receptors and release odors that stimulate the olfactory receptors
The sensations generated by these receptors increase the pleasure of eating and initiate gastric secretions

MASTICATIONMastication Reflex
Although mastication is a voluntary act, it is coordinated by reflex centers in he brain stem that facilitate the opening and closing of the jaw– When the mouth opens, stretch receptors in the jaw
muscle initiate a refkex contraction of the masseter, medial pterygoid, and temporal muscle, causing mouth to close
– When the mouth closes, food comes into contact with buccal receptors eliciting a reflex contraction of digastric and lateral pterygoid muscles, causing the mouth to open
– When the jaw drops, the stretch reflex causes the entire cycle to be repeated

DEGLUTITION (SWALLOWING)
Deglutition or swallowing consists of three phase:– Oral (voluntary) phase. During this phase, the
tongue forms a bolus of food and forces it into the oropharynx by pushing up and back against the hard palate
– Pharyngeal phase. This phase coordinated by a swallowing center in the medulla and lower pons
– Esophageal phase. After reaching the esophagus, food is propelled into stomach by peristaltis

Pharyngeal PhaseThis phase begins when the food reaches
the oropharynx and progresses as follows:– The nasopharynx is closed by the soft palate,
preventing regurgitation of food in to nasal cavities
– The palatopharyngeal folds are pulled medially, forming a passageway for the food to move into the pharynx
– The glottis and vocal cords are closed and the epiglottis swing down over the larynx, guiding the food toward the esophagus
Respiration is inhibited for the duration of the pharyngeal phase (1-2 seconds)

Esophageal PhaseSphincters involved in esophageal peristaltis:
– The upper esophageal sphincter (striated muscle)
– The lower esophageal sphincter (smooth muscle)
Types of esophageal peristaltis:– Primary esophageal peristaltis is initiated by
swallowing
– Secondary peristaltis is initiated by the presence of food within the esophagus
Coordination of esophageal peristaltis:– Primary esophageal peristaltis is coordinated by
vagal fibers
– Secondary esophageal peristaltis is coordinated by the intrinsic nervous system


Esophageal Muscle

Swallowing Mechanism and Regulation

Disorders of SwallowingEsophageal reflux, may occur if the
intragastric pressure rise high enough to force the lower esophageal sphincter open– During pregnancy
– Reflux of stomach acid causes esophageal painBelching (eructation), following a heavy meal
or ingestion of large amount of gas (e.g., from carbonated beverages)
Achalasia, is a neuromuscular disorder of the lower two-thirds of the esophageal that leads to absence of peristaltis and failure of the lower esophageal sphincter to relax

MOTILITY OF STOMACH
The three functional parts of the stomach are the fundus, corpus, and antrum
Gastric contents are isolated from other parts of the GI tract by the lower esophageal sphincter proximally and by the pylorus distally
The antrum and pylorus are anatomically continous and respond to nervous control as a unit
Functional components


MOTILITY OF STOMACH
Each muscle layer forms a functional syncytium and therefore acts as a unit
In the fundus, where the layers are relatively thin, strength of contraction is weak; in the antrum, where the muscle layers are thick, strength of contraction is strong
The stomach and duodenum are divided by a thickened muscle layer called the pyloric sphincter
Musculature

MOTILITY OF STOMACH
Intrinsic innervation directly responsible for peristaltis– The myenteric plexus (Auerbach’s) is located
between the layers of the circular and longitudinal muscles of the stomach
– The submucosal plexus (Meissner’s) is located between the layers of the circular muscle and mucosa on the luminal surface of the stomach
Extrinsic through autonomic nervous system:– Sympathetic, via the celiac plexus (inhibits motility)– Parasympathetic, via the vagus nerve (stimulates
motility)
Innervation

Function of Motility
Storage. When food enters the stomach, the upper region - primarily fundus - enlarges to accommodate the food by receptive relaxation
Mixing. Combination of peristaltis and retropulsion mixes the food with acid and enzymes. When the food is mixed into pasty consistency, it is called chyme
Emptying. When the chyme is broken down into small enough particles, it is propelled through the pyloric sphincter into intestine
Gastric motility serves three basic function

Function of Motility
Initiated as apart of the peristaltic process causing swallowing and esophageal motility or in response to food entering the stomach
Strecth receptors in the upper portion of stomach detect the presence of food and initiate a vago-vagal reflex producing relaxation
This process regulate by postganglionic fibers within the enteric nervous system release a noncholinergic nonadrenergic transmitter, may be ATP or VIP
Receptive relaxation

Function of Motility
Produced by periodic change in BER originate in a pace maker within longitudinal muscle
BER or slow wave occur at a rate of approximately 3-4/min and velocity is 1 cm/sec at the corpus and increase to 3-4 cm/sec in the antrum
Ca2+ play an important role in BER, and the force of peristaltis contractions is regulated by gastrin and acetylcholine
Peristaltis

Function of Motility
Is the back and forth movement of the chyme caused by the forceful propulsion of food against the closed pyloric sphincter
The forward and backward movement of the chyme (caused by peristaltis and retropulsion) breaks the chyme into smaller and smaller pieces and mixes it with the gastric secretions present within stomach
Retropulsion

Function of Motility
Each time the chime pushed against the pyloric sphincter, a small amount (2-7 ml) may escape into duodenum
The amount of chyme passing the pylorus depends on the size of the particles
Liquids empty much faster than solids. The rate of liquids emptying is proportional to pressure within the upper portion of stomach, which increase slowly during the digestive period
Gastric emptying

Functional Disorder of Motility
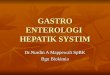
Initiation– The vomiting center. Directly activated by afferent
fibers or by irritation due to injury or increases in intracranial pressure
– Chemoreceptor trigger zone. Activated by afferent nerves originating within the GI tract or by circulating emetic agents
Mechanical sequence of vomiting– Begins with deep inspirasion followed by the closing
of the glottis
– Intestine propels chyme into upper region of stomach
– Increase in abdominal pressure forces the chyme into esophagus and out of the mouth
Vomiting or emesis

Vomiting Reflex

INTESTINAL MOTILITY
Contractile activity of the smooth muscle lining the small intestine serve two functions:– Mixing the chyme with digestive enzymes and
bile to facilitate digestion and absorption
– Propelling the chyme from the duodenum to the colon
It usually takes about 2-4 hours for the chyme to move from one end of the small intestine to the other
Contractile activity

INTESTINAL MOTILITY
Segmentation is the most common type of intestinal contraction
Peristaltic contractions is not considered to be an important component of intestinal transit
MMC spreads over the intestine during interdigestive period
Types of movements

INTESTINAL MOTILITY
During segmentation, about 2 cm of the intestinal wall contracts, forcing the chyme throughout the digestive period
When the muscle relaxes, the chyme returns to the area from which it was displaced
This back-and-forth movement enables the chyme to become mixes with digestive enzymes and to make contact with the absorptive surface of the intestinal mucosa
Segmentation occur about 12 times/min in the duodenum and 8 times/min in the ileum. The contraction last for 5-6 seconds
Segmentation contractions

INTESTINAL MOTILITY
Segmentation occur only if the slow waves produce spikes potentials which is controlled by pacemaker cells within the wall of the intestine and is not infuenced by neural activity or circulating hormones
The frequency of segmentation is directly related to the frequency of the slow wave
The strength of segmentation is proportional to the frequency of the spike potentials generated by slow wave
Slow wave amplitude is increased by gastrin, CCK, motilin, and insulin; and decreased by secretin and glucagon
Regulation of intestinal motility