Embed Size (px)
Citation preview

Giant Congenital Melanocytic NevusTreated With TrametinibAdnan Mir, MD, PhD,a Nnenna G. Agim, MD,a Alex A. Kane, MD,b Shellie C. Josephs, MD,c Jason Y. Park, MD, PhD,d
Kathleen Ludwig, MDe
abstractGiant congenital nevi are melanocytic proliferations of the skin that may becomplicated by melanoma, neurocutaneous melanocytosis, pain, pruritus, anddisfigurement. Current treatment options include surgical resection andmedical management of associated symptoms. There is limited efficacy inthese modalities. No effective pharmacologic treatments are available for thetreatment of these lesions. We present the case of a 7-year-old girl witha giant congenital melanocytic nevus that had an AKAP9-BRAF fusion and wastreated with trametinib, which resulted in rapid resolution of the patient’slifelong, intractable pain and pruritus as well as dramatic improvement in theextent of her nevus.
Congenital melanocytic nevi (CMNs)are melanocytic proliferations thattypically present in the skin at birthor shortly thereafter and are classifiedprimarily on the basis of size. Giantcongenital melanocytic nevi (GCMNs)are defined as those CMNs that arepredicted to be $40 cm in diameterby adulthood and that may becomplicated by melanoma,neurocutaneous melanocytosis,severe pain and pruritus,hypohidrosis, xerosis, cosmeticdisfigurement, and social isolation.There is an estimated incidence of ∼1in 20 000 to 500 000 live births.1,2
GCMNs are caused by somaticmosaicism in melanocytic precursors.NRAS mutations can be found in 80%to 95% of GCMNs and result in theactivation of the mitogen-activatedprotein kinase (MAPK) andphosphatidylinositol 3-kinase (PI3K)pathways, which ultimately increasesthe proliferation and survival ofmelanocytes.3 BRAF-activatingmutations (single-nucleotidevariants and fusions) that activatethe MAPK pathway have also beenreported.4,5
Traditional treatments of GCMNs haverelied on serial surgical resection withskin grafting or tissue expansion andadvancement. However, this is oflimited use in large lesions and in thosethat impinge on vital structures. Thepresence of activation of the MAPKpathway has led to the suggestion thattargeting MAP/ERK kinase (MEK),which is a downstream target of thispathway, may be a viable treatmentoption.6 No successful attempts at thistherapy have been reported thus far,and GCMNs continue to be difficult tomanage.
CASE REPORT
A 6-week-old African American girlpresented with a dark brown nevusthat covered the majority of the backand extended onto the flanks, rightabdomen, buttocks, thighs, andsuprapubic area. There were scatteredsatellite nevi on the scalp, face,extremities, and buttocks, with multiplehyperpigmented nail bands. Over thenext several years, she developedsignificant, disfiguring thickening of thenevus, predominantly over her back
Departments of aDermatology, bPlastic Surgery, cRadiology,and dPathology, Eugene McDermott Center for HumanGrowth and Development, and eDivision of PediatricHematology and Oncology, University of Texas SouthwesternMedical Center, Dallas, Texas
Dr Mir initiated the testing that led to the describedtreatment and drafted the manuscript; Drs Agim,Kane, and Josephs collected data and criticallyreviewed the manuscript; Dr Park performed genetictesting for the patient described in this study andcritically reviewed the manuscript; Dr Ludwiginitiated therapy, coinitiated the submission of thismanuscript, and performed the first critical reviewof the manuscript; and all authors approved the finalmanuscript as submitted and agree to beaccountable for all aspects of the work.
DOI: https://doi.org/10.1542/peds.2018-2469
Accepted for publication Oct 3, 2018
Address correspondence to Kathleen Ludwig, MD, UTSouthwestern Medical Center, 5323 Harry Hines Blvd,Dallas, TX 75390. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,1098-4275).
Copyright © 2019 by the American Academy ofPediatrics
FINANCIAL DISCLOSURE: The authors have indicatedthey have no financial relationships relevant to thisarticle to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors haveindicated they have no potential conflicts of interestto disclose.
To cite: Mir A, Agim NG, Kane AA, et al. GiantCongenital Melanocytic Nevus Treated WithTrametinib. Pediatrics. 2019;143(3):e20182469
PEDIATRICS Volume 143, number 3, March 2019:e20182469 CASE REPORT by guest on April 23, 2020www.aappublications.org/newsDownloaded from
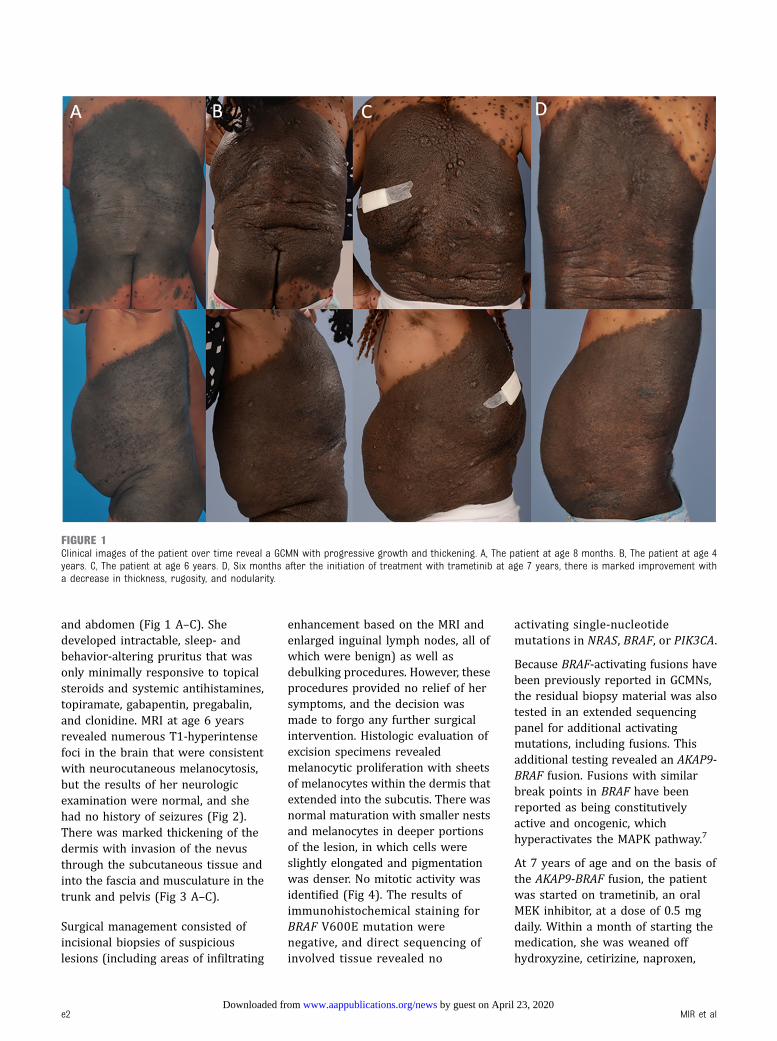
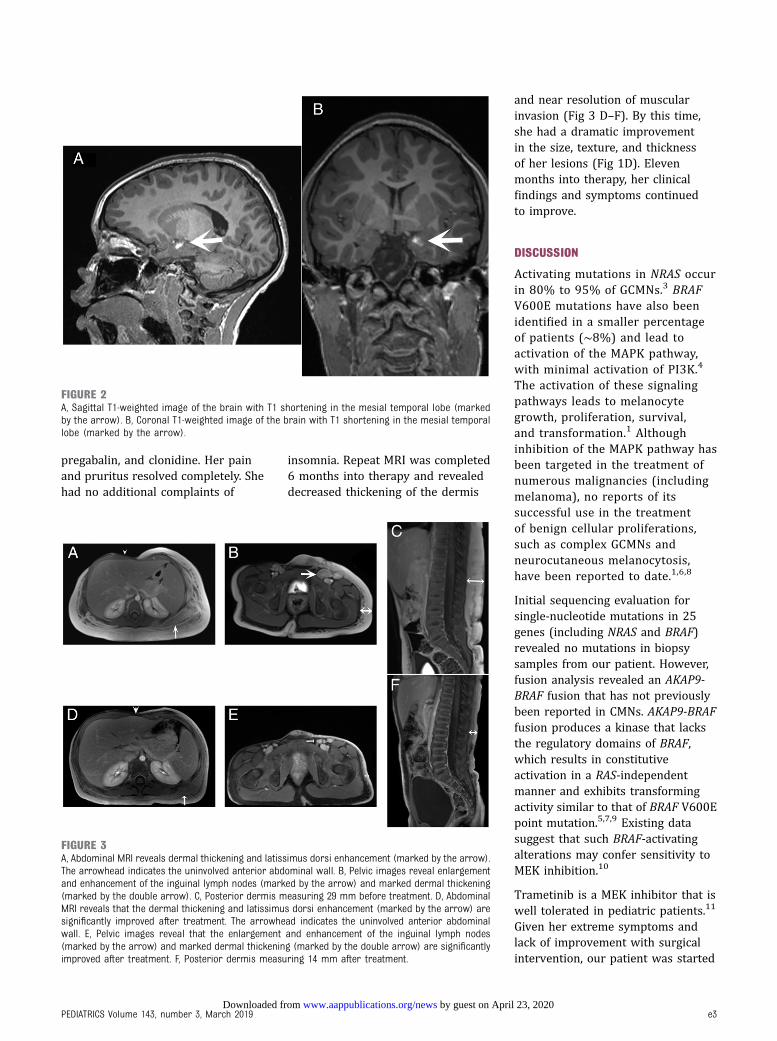
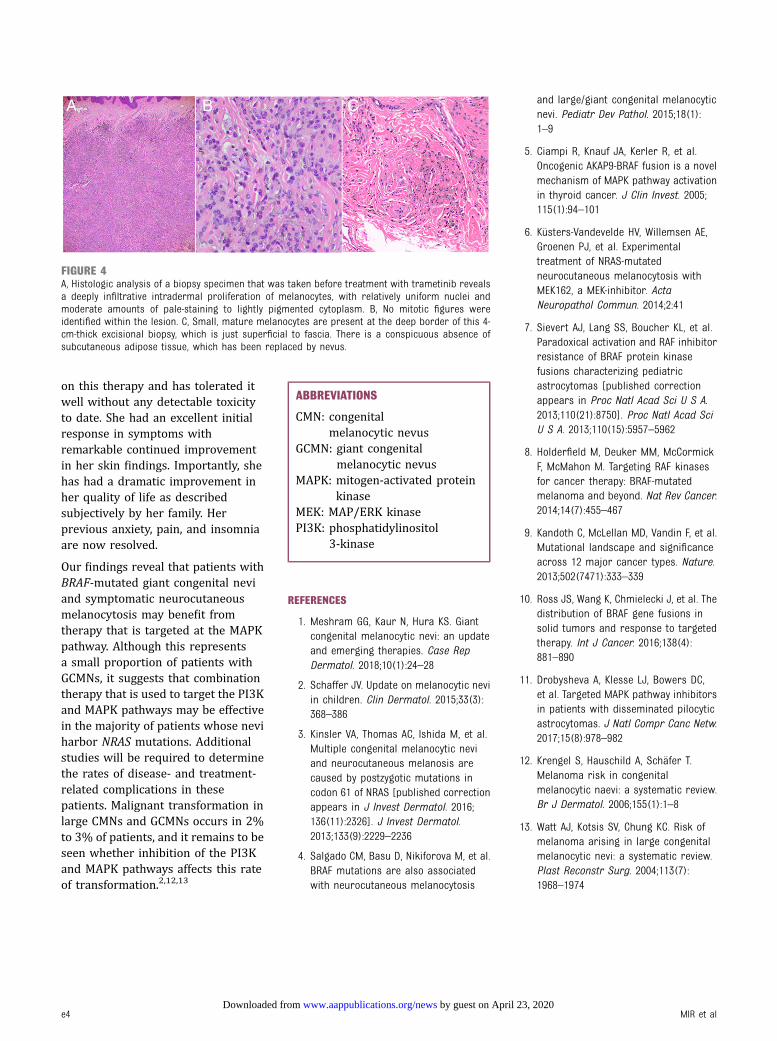
and abdomen (Fig 1 A–C). Shedeveloped intractable, sleep- andbehavior-altering pruritus that wasonly minimally responsive to topicalsteroids and systemic antihistamines,topiramate, gabapentin, pregabalin,and clonidine. MRI at age 6 yearsrevealed numerous T1-hyperintensefoci in the brain that were consistentwith neurocutaneous melanocytosis,but the results of her neurologicexamination were normal, and shehad no history of seizures (Fig 2).There was marked thickening of thedermis with invasion of the nevusthrough the subcutaneous tissue andinto the fascia and musculature in thetrunk and pelvis (Fig 3 A–C).
Surgical management consisted ofincisional biopsies of suspiciouslesions (including areas of infiltrating
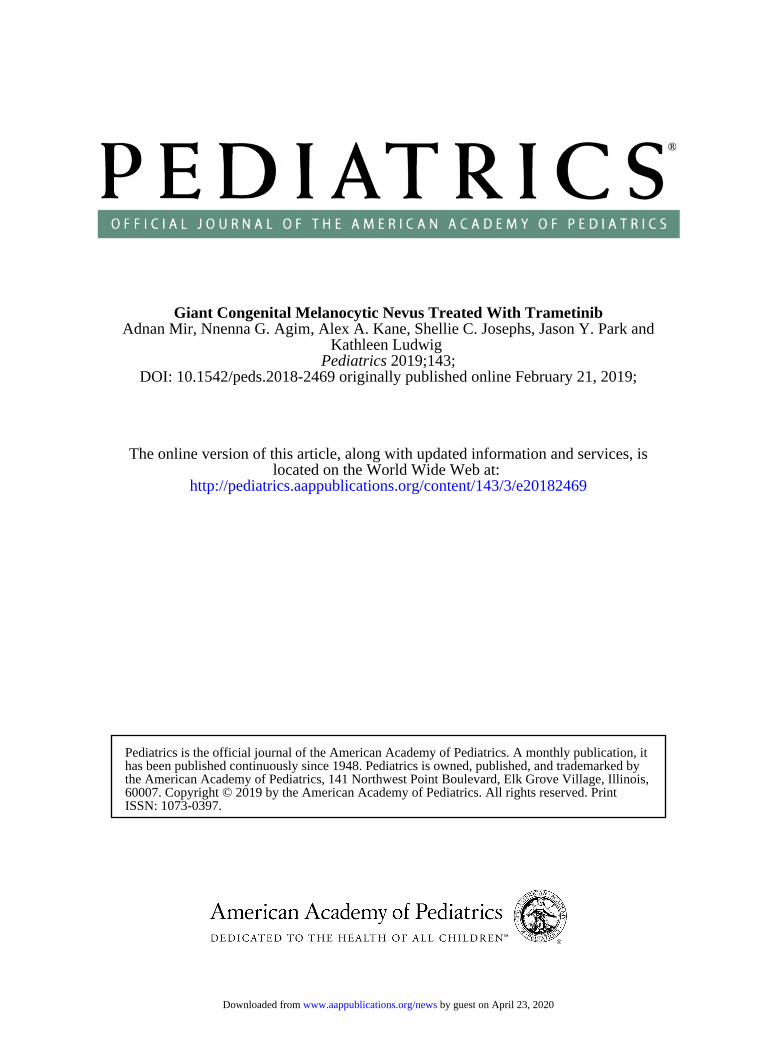
enhancement based on the MRI andenlarged inguinal lymph nodes, all ofwhich were benign) as well asdebulking procedures. However, theseprocedures provided no relief of hersymptoms, and the decision wasmade to forgo any further surgicalintervention. Histologic evaluation ofexcision specimens revealedmelanocytic proliferation with sheetsof melanocytes within the dermis thatextended into the subcutis. There wasnormal maturation with smaller nestsand melanocytes in deeper portionsof the lesion, in which cells wereslightly elongated and pigmentationwas denser. No mitotic activity wasidentified (Fig 4). The results ofimmunohistochemical staining forBRAF V600E mutation werenegative, and direct sequencing ofinvolved tissue revealed no
activating single-nucleotidemutations in NRAS, BRAF, or PIK3CA.
Because BRAF-activating fusions havebeen previously reported in GCMNs,the residual biopsy material was alsotested in an extended sequencingpanel for additional activatingmutations, including fusions. Thisadditional testing revealed an AKAP9-BRAF fusion. Fusions with similarbreak points in BRAF have beenreported as being constitutivelyactive and oncogenic, whichhyperactivates the MAPK pathway.7
At 7 years of age and on the basis ofthe AKAP9-BRAF fusion, the patientwas started on trametinib, an oralMEK inhibitor, at a dose of 0.5 mgdaily. Within a month of starting themedication, she was weaned offhydroxyzine, cetirizine, naproxen,
FIGURE 1Clinical images of the patient over time reveal a GCMN with progressive growth and thickening. A, The patient at age 8 months. B, The patient at age 4years. C, The patient at age 6 years. D, Six months after the initiation of treatment with trametinib at age 7 years, there is marked improvement witha decrease in thickness, rugosity, and nodularity.
e2 MIR et al by guest on April 23, 2020www.aappublications.org/newsDownloaded from
pregabalin, and clonidine. Her painand pruritus resolved completely. Shehad no additional complaints of
insomnia. Repeat MRI was completed6 months into therapy and revealeddecreased thickening of the dermis
and near resolution of muscularinvasion (Fig 3 D–F). By this time,she had a dramatic improvementin the size, texture, and thicknessof her lesions (Fig 1D). Elevenmonths into therapy, her clinicalfindings and symptoms continuedto improve.
DISCUSSION
Activating mutations in NRAS occurin 80% to 95% of GCMNs.3 BRAFV600E mutations have also beenidentified in a smaller percentageof patients (∼8%) and lead toactivation of the MAPK pathway,with minimal activation of PI3K.4
The activation of these signalingpathways leads to melanocytegrowth, proliferation, survival,and transformation.1 Althoughinhibition of the MAPK pathway hasbeen targeted in the treatment ofnumerous malignancies (includingmelanoma), no reports of itssuccessful use in the treatmentof benign cellular proliferations,such as complex GCMNs andneurocutaneous melanocytosis,have been reported to date.1,6,8
Initial sequencing evaluation forsingle-nucleotide mutations in 25genes (including NRAS and BRAF)revealed no mutations in biopsysamples from our patient. However,fusion analysis revealed an AKAP9-BRAF fusion that has not previouslybeen reported in CMNs. AKAP9-BRAFfusion produces a kinase that lacksthe regulatory domains of BRAF,which results in constitutiveactivation in a RAS-independentmanner and exhibits transformingactivity similar to that of BRAF V600Epoint mutation.5,7,9 Existing datasuggest that such BRAF-activatingalterations may confer sensitivity toMEK inhibition.10
Trametinib is a MEK inhibitor that iswell tolerated in pediatric patients.11
Given her extreme symptoms andlack of improvement with surgicalintervention, our patient was started
FIGURE 2A, Sagittal T1-weighted image of the brain with T1 shortening in the mesial temporal lobe (markedby the arrow). B, Coronal T1-weighted image of the brain with T1 shortening in the mesial temporallobe (marked by the arrow).
FIGURE 3A, Abdominal MRI reveals dermal thickening and latissimus dorsi enhancement (marked by the arrow).The arrowhead indicates the uninvolved anterior abdominal wall. B, Pelvic images reveal enlargementand enhancement of the inguinal lymph nodes (marked by the arrow) and marked dermal thickening(marked by the double arrow). C, Posterior dermis measuring 29 mm before treatment. D, AbdominalMRI reveals that the dermal thickening and latissimus dorsi enhancement (marked by the arrow) aresignificantly improved after treatment. The arrowhead indicates the uninvolved anterior abdominalwall. E, Pelvic images reveal that the enlargement and enhancement of the inguinal lymph nodes(marked by the arrow) and marked dermal thickening (marked by the double arrow) are significantlyimproved after treatment. F, Posterior dermis measuring 14 mm after treatment.
PEDIATRICS Volume 143, number 3, March 2019 e3 by guest on April 23, 2020www.aappublications.org/newsDownloaded from
on this therapy and has tolerated itwell without any detectable toxicityto date. She had an excellent initialresponse in symptoms withremarkable continued improvementin her skin findings. Importantly, shehas had a dramatic improvement inher quality of life as describedsubjectively by her family. Herprevious anxiety, pain, and insomniaare now resolved.
Our findings reveal that patients withBRAF-mutated giant congenital neviand symptomatic neurocutaneousmelanocytosis may benefit fromtherapy that is targeted at the MAPKpathway. Although this representsa small proportion of patients withGCMNs, it suggests that combinationtherapy that is used to target the PI3Kand MAPK pathways may be effectivein the majority of patients whose neviharbor NRAS mutations. Additionalstudies will be required to determinethe rates of disease- and treatment-related complications in thesepatients. Malignant transformation inlarge CMNs and GCMNs occurs in 2%to 3% of patients, and it remains to beseen whether inhibition of the PI3Kand MAPK pathways affects this rateof transformation.2,12,13
ABBREVIATIONS
CMN: congenitalmelanocytic nevus
GCMN: giant congenitalmelanocytic nevus
MAPK: mitogen-activated proteinkinase
MEK: MAP/ERK kinasePI3K: phosphatidylinositol
3-kinase
REFERENCES
1. Meshram GG, Kaur N, Hura KS. Giantcongenital melanocytic nevi: an updateand emerging therapies. Case RepDermatol. 2018;10(1):24–28
2. Schaffer JV. Update on melanocytic neviin children. Clin Dermatol. 2015;33(3):368–386
3. Kinsler VA, Thomas AC, Ishida M, et al.Multiple congenital melanocytic neviand neurocutaneous melanosis arecaused by postzygotic mutations incodon 61 of NRAS [published correctionappears in J Invest Dermatol. 2016;136(11):2326]. J Invest Dermatol.2013;133(9):2229–2236
4. Salgado CM, Basu D, Nikiforova M, et al.BRAF mutations are also associatedwith neurocutaneous melanocytosis
and large/giant congenital melanocyticnevi. Pediatr Dev Pathol. 2015;18(1):1–9
5. Ciampi R, Knauf JA, Kerler R, et al.Oncogenic AKAP9-BRAF fusion is a novelmechanism of MAPK pathway activationin thyroid cancer. J Clin Invest. 2005;115(1):94–101
6. Küsters-Vandevelde HV, Willemsen AE,Groenen PJ, et al. Experimentaltreatment of NRAS-mutatedneurocutaneous melanocytosis withMEK162, a MEK-inhibitor. ActaNeuropathol Commun. 2014;2:41
7. Sievert AJ, Lang SS, Boucher KL, et al.Paradoxical activation and RAF inhibitorresistance of BRAF protein kinasefusions characterizing pediatricastrocytomas [published correctionappears in Proc Natl Acad Sci U S A.2013;110(21):8750]. Proc Natl Acad SciU S A. 2013;110(15):5957–5962
8. Holderfield M, Deuker MM, McCormickF, McMahon M. Targeting RAF kinasesfor cancer therapy: BRAF-mutatedmelanoma and beyond. Nat Rev Cancer.2014;14(7):455–467
9. Kandoth C, McLellan MD, Vandin F, et al.Mutational landscape and significanceacross 12 major cancer types. Nature.2013;502(7471):333–339
10. Ross JS, Wang K, Chmielecki J, et al. Thedistribution of BRAF gene fusions insolid tumors and response to targetedtherapy. Int J Cancer. 2016;138(4):881–890
11. Drobysheva A, Klesse LJ, Bowers DC,et al. Targeted MAPK pathway inhibitorsin patients with disseminated pilocyticastrocytomas. J Natl Compr Canc Netw.2017;15(8):978–982
12. Krengel S, Hauschild A, Schäfer T.Melanoma risk in congenitalmelanocytic naevi: a systematic review.Br J Dermatol. 2006;155(1):1–8
13. Watt AJ, Kotsis SV, Chung KC. Risk ofmelanoma arising in large congenitalmelanocytic nevi: a systematic review.Plast Reconstr Surg. 2004;113(7):1968–1974
FIGURE 4A, Histologic analysis of a biopsy specimen that was taken before treatment with trametinib revealsa deeply infiltrative intradermal proliferation of melanocytes, with relatively uniform nuclei andmoderate amounts of pale-staining to lightly pigmented cytoplasm. B, No mitotic figures wereidentified within the lesion. C, Small, mature melanocytes are present at the deep border of this 4-cm-thick excisional biopsy, which is just superficial to fascia. There is a conspicuous absence ofsubcutaneous adipose tissue, which has been replaced by nevus.
e4 MIR et al by guest on April 23, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2018-2469 originally published online February 21, 2019; 2019;143;Pediatrics
Kathleen LudwigAdnan Mir, Nnenna G. Agim, Alex A. Kane, Shellie C. Josephs, Jason Y. Park and
Giant Congenital Melanocytic Nevus Treated With Trametinib
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/143/3/e20182469including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/143/3/e20182469#BIBLThis article cites 13 articles, 2 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/cancer:neoplastic_subCancer/Neoplastic_subhttp://www.aappublications.org/cgi/collection/hematology:oncologyHematology/Oncologyhttp://www.aappublications.org/cgi/collection/dermatology_subDermatologyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on April 23, 2020www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2018-2469 originally published online February 21, 2019; 2019;143;Pediatrics
Kathleen LudwigAdnan Mir, Nnenna G. Agim, Alex A. Kane, Shellie C. Josephs, Jason Y. Park and
Giant Congenital Melanocytic Nevus Treated With Trametinib
http://pediatrics.aappublications.org/content/143/3/e20182469located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2019 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on April 23, 2020www.aappublications.org/newsDownloaded from








![RESEARCH AND REVIEWS: JOURNAL OF MEDICAL AND … · Giant congenital nevus (Bathing trunk nevus / Garment nevus / Giant hairy nevus / Nevus pigmentosus et pilosus) – [6]have one](https://img.pdfslide.net/doc/110x75/5c8b90c109d3f21b168c6625/research-and-reviews-journal-of-medical-and-giant-congenital-nevus-bathing.jpg)




















