Embed Size (px)
Citation preview

Eur Reaplr J 1991, 4, 1135-1139
Increased coagulation activity of the pleura after tube drainage and quinacrine Instillation in malignant pleural effusion
V. Agrenius*, J. Chmielewska*"1, 0. Widstrom*, M. Blomback**
Increased coagulation activity of the pleura after tube drainage and quinacrine instillation in malignant pleural effusion. V. Agrenius, J. Chmielewska, 0. Widstrom, M. Blomblic/c.
• Depts of Thoracic Medicine and • • Clinical Chemistry and Blood Coagulation, Karolinska Institute, Karolinska Hospital, Stockholm, Sweden. t Kabi, Stockholm, Sweden. ABSTRACf: Chronic malignant pleural effusions are usually treated with
an intrapleunlly administered irritant that creates an Inflammatory reaction. The Induced lnOammatlon results in fibrin deposition and termination of Ouid exudation.
Couespondence: V. Agrenius, Dept of Thoracic Medicine, Karolinska Hospital, S-104 01 Stockholm, Sweden.
In the present study several factors In the coagulation system In the pleural Ould were followed during treatment with tube drainage and quinacrine Instillation Into the pleural space. In the chronic exudative phase before treatment, both thrombin activity and fibrinopeptide A (FP A), were present at low levels. During treatment the levels Increased markedly. Betathrombog)obulln, a platelet marker, showed a simlJar pattern. Prothrombin, antithrombin m, prekallikreio and kallikrein Inhibiting activity showed DO
such variations In activity.
Keywords: Beta·thromboglobulin; fibrinopeptide A; malignant pleurisy; pleurodesis; thrombin activity.
Received: January 25, 1991; accepted after revision July 1, 1991.
This study has been supported by The Swedish Heart-Lung Foundation, Swedish Medical Research Council (No. 520) and The Karo.linska Institute. The high tbrombln activity and FPA level Induced by treatment reflect an
active process or fibrin formation wblcb seems to play an important role In arresting chronic pleural exudation. Eur Respir J., 1991, 4, 1135-1139.
Malignant disease in serous membranes may cause chronic effusion. This is often seen in the pleura and the peritoneum, but less often in the pericardium. Malignant pleural effusion causes great discomfort and anxiety and the treatment is painful and time-consuming. A better understanding of the pathogenic mechanism is needed in order to find better methods of treatment. The presence of exudate gives a much greater possibility to analyse biologically active substances from the malignant cells and tumour environment than is possible from studies on solid tumours.
The pleurodesis method routinely used in our clinic includes thoracoscopy and chest tube drainage. Insertion of a drainage tube in itself causes inflammation which might be compared with the inflammation of a wound trauma. Pleurodesis also involves the application of an irritant substance (in our department quinacrine) which induces a still stronger inflammatory reaction, with destruction of the pleural surface [1]. The reaction is similar to that seen with other substances used for pleurodesis, such as talcum, Corynebacterium parvum and tetracycline [2-6]. The macroscopic picture is typical, with fibrin formation later followed by swelling of the pleura, and of vessels and collagen forming fibrotic tissue [7]. Fibrin is evidently the matrix substance for the formation of fibrotic tissue. For unknown reasons, this inflammatory process with formation of fibrotic tissue, leads to the cessation of fluid production despite the persistence of malignant tissue.
In a previous study, fibrinolytic activity was shown to be high in the exudative stage before treatment [8]. The activity decreased markedly after the trauma of inserting a chest tube for drainage. A moderate but significant further decrease in fibrinolysis was seen after quinacrine instillation into the pleural space. The aim of this study was to determine whether the phenomena of fibrin deposition and adhesion also reflect a change in coagulation activity.
Material and methods
Patients
Eleven patients, consecutively admitted to the Department of Thoracic Medicine, Karolinska Hospital, from February to December 1986, were investigated. There were six males and five females, aged 36-79 yrs, mean age 62 yrs. The following malignant tumours were diagnosed: breast carcinoma ( 4), adenocarcinomas of uncertain origin (3), mesotheliomas (2) ovarian carcinoma (1) and kidney carcinoma (1). All patients suffered from unilateral chronic malignant pleural effusion and were considered to benefit from pleurodesis treatment. In seven of the eleven cases the pleural fluid was macroscopically sanguinolent.
This study was approved by the Human Research Ethical Committee of the Karolinska Hospital and informed consent was obtained from each subject.

1136 V. AGRENIUS ET AL.
We followed our normal routine for pleurodesis treatment. Initially, a thoracocentesis with collection of samples for routine analyses was performed. Subsequently, 500 ml of air was instilled to improve X-ray conditions and the safety of the thoracoscopy. On the following day, thoracoscopy was performed providing a clear view of the pleural surface and permitting good pleural biopsies. A drainage tube was inserted and connected for suction, which was started at -5 cmHp and continued at -15 cmHp. When the lung had expanded, as determined by X-ray, which was usually on the following day, 600 mg of quinacrine, dissolved in 20 ml of saline, was instilled into the pleural space.
Within one day after treatment all the patients developed a fever reaction. The drainage tube was removed when the fluid production fell below 50 ml·day·1
•
Sampling
The samples of fluid were taken at the initial thoracocentesis, just before the injection of quinacrine, and 6, 24 and 48 h after instillation. On each occasion the total volume of fluid produced was measured. To prevent any further coagulation reaction, one part of the anticoagulant was added to six parts of pleural fluid. The anticoagulants employed were 10% sodium edetic acid (EDTA) for betathromboglobulin analysis; physiological saline containing 1,000 KIU·ml·1 Trasylol~ and 1,000 IU·ml·1 heparin for fibrinopeptide A (FPA) measurements and 0.13 mol·/"1
trisodium citrate for other assays. All samples were centrifuged at 2,500 g for 20 rnin and supematants were aliquoted and stored at -70°C until assay.
Materials
Quinacrine hydrochloride was purchased from Boots Limited, Nottingham, UK. Trasylol was purchased from Bayer, Leverkusen, FRG and heparin from Kabi, Stockholm, Sweden. The chromogenic substrate for thrombin H-D-Phe-Pip-Arg-pNA (S-2238) was supplied by Kabi Diagnostica, Molndal, Sweden. The radioimmunoassay (RIA) kit for beta-thromboglobulin was purchased from Amersham Co., Amersham, UK. Thrombin came from Hoffman-LaRoche, Basel, Switzerland and Cephotest from Nycomed NS, Oslo, Norway. The kit for FPA was obtained from IMCO, Stockholm, Sweden and 1251 used for its labelling was from Amersham. All other chemicals were of analytical grade.
Laboratory methods
FPA-levels were measured with Nossel's radioimmunoassay, as modified by KocKUm and FREBEIJUS [9]. The beta-thromboglobulin radioimmunoassay was performed according to the instructions of the manufacturer. The chromogenic substrate S-2238 was used for the assays of thrombin, prothrombin and antithrombin Ill. The latter was assayed by the method of ABILDGAARD et al. [10]
modified for the Cobas-Bio centrifugal enzyme analyser. Prothrombin was determined by the method of BERGSTROM and BLOMBACK [11]. Prekallikrein and kallikrein inhibiting activity were measured using the chromogenic substrate S-2302 by the methods of GALLIMORE and FRIBERGER [12]. The levels of prothrombin, antithrombin Ill, prekallikrein and kallikrein inhibiting activity are expressed in U-ml-1 where 1 U is defined as the activity present in 1 ml of pooled human plasma. The amidolytic activity of pleural fluid on the thrombin-sensitive chromogenic substrate S-2238 was measured as described previously [13]. The activity is expressed as delta absorbance per unit of time (min). The activity measured is mainly that of the alpha -macroglobulin-thrombin complex, which is active on the substrates but inactive on the macromolecular fibrinogen. Thus, both FPA- levels and the thrombin activity reflect recent thrombin activity [13].
Statistical analysis
Mean and standard deviations were used. The Friedman non-parametric two-way analysis of variance and multiple comparison on ranks of several related samples was performed as described by THEODORSSON-NORHEIM (14].
Results
In all11 patients the drainage tube was removed when fluid production fell below 50 ml·day h·1
, which mostly occurred within 2-4 days (mean 3.6 days) after the injection of quinacrine into the pleural space. All of the patients developed a fever, of about 38°C within 24 h. The treatment was sucessful in all of the patients, since no further thoracocentesis was needed. Indeed, these 11 patients all showed full expansion of the lung on X-ray with no further signs of pleural effusion.
Before treatment, the levels of FPA and betathromboglobulin in the pleural fluid at the time of thoracocentesis were higher than normal plasma. Furthermore, thrombin activity, not normally present in plasma, was demonstrated in pleural fluid. Thrombin and FP A levels increased in parallel in all cases during the entire treatment, including the insertion of drainage tube and during quinacrine instillation (figs. 1 and 2). The FP A levels reached their maximum in fluid collected 6 h after quinacrine treatment, while thrombin activity and beta-thromboglobulin reached maximal levels in pleural fluid collected at 24 h. See table 1 for a summary of the results.
Measurements from the drainage tube performed prior to the injection of quinacrine, were intended as baseline values. However, even at this early stage the levels were considerably increased. The finding that the drainage tube itself was mainly responsible for the increase in values encouraged us to design some experiments. Thus, in three patients pleural fluid was collected from the drainage tube during three days (fig. 3). On the second and third days of treatment, all of the patients showed a decrease in the three parameters. However, following the injection of quinacrine, the' levels rose again.

\ 10
~ '?
0 ... f Cll c:: l5
~ ~
COAGULATION ACllVITY IN PLEURAL INFLAMMATION
1000 ...
L E
t ~ 100
~2~~~!i
Pre Post tube drainage
8h 24h 48h after quinacrine
1000
100
1137
... ' ~ a c:: .E B 0
I ~ i
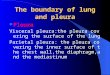
Fig. 1. - Levels of thrombin activity (...-.-.); fibrinopeptide A (FP A) (o-o); and beta-thromboglobulin (beta-TO) (Q--0) before (pre-tube drainage) and during (post-tube drainage, 6, 24 and 48 h after) quinacrine instillation in the pleural space. Mean values are indicated. For comparison, the normal plasma levels are 0.29-2.0 pmol·ml·1 for FPA and 11-34 ng·mi·• for beta-TO. Thrombin is not present in normal plasma. 11A: A absorbance.
100 1000 1000
~ 'i:.. E
~ 10 100 ~ 100
~ ~ .!: • ~
f t t I ~
I <::
25 10 ~ 10 • ~ ~
~
• T .. T
Pre Post 24h Pre Post 8h Pre Post 24h tube after tube after tube after
drainage quinacrine drainage quinacrine drainage quinacrine
Fig. 2. - Individual levels are given to demonstrate the variation of thrombin activity, fibrinopeptide A (FP A) and beta-thromboglubulin levels before, and after insertion of drainage tube, and the maximum level after quinacrine instillation, at 24 h for thrombin activity and beta-thromboglobulin and at 6 h for FP A 11A: A absorbance.
Table 1. - Summary of results and statistical analyses
Pleural fluid Before After After quinacrine instillation tube tube
drainage drainage 6h 24 h 48 h
Thrombin activity xl0·3 1.10:t0.9 ll.l:t9.3• 16.1:t7.4• 18.0:t10.S•t 12.1:t9.4* A·min·1
FPA pmol·mP 120:t140 1250:t990* 1990:t11SO•t 1120:t560* 1230:t780• Beta-thromboglobulin 58:t60 184:t123• 152:t108* 274:t159• 225:t128* ng·m1·1
Prothrombin U·ml·1 0.3l:t0.10 0.23:t0.10 0.26:t0.11 0.22:t0.09 0.18:t0.11 Kallikrein inhibiting 0.43:t0.17 0.42:t0.15 0.35:t0.11 0.47:t0.16 0.47:t0.18 activity U·ml·1
Antithrombin Ill 0.43:t0.10 0.44:t0.12 0.41:t0.13 0.49:t0.15 0.50:t0.16 U·ml·1
Prekallikrein 0.41:t0.12 0.40:t0.13 0.37:t0.13 0.45:t0.16 0.45:t0.15 U·mi·1
Values are mean:tsD, 11 analyses on each occasion. •: levels before and after quinacrine instillation in the pleural space were significantly higher (p<O.OOl) than those at the time of the first thoracococentesis; t: levels after quinacrine instillation were significantly higher (p<O.Ol) than those before quinacrine instillation; FPA: fibrinopeptide A. A: absorbance.

1138 V. AGRENIUS ET AL.
-._ ~ 10
't -
T Pre 24 h 48 h
tube drainage
l Quinacrine
72h 24h 48h after quinacrine
Fig. 3. - Thrombin activity in three patients with a prolonged period of tube drainage just before quinacrine instillation. A slight decrease in levels is seen on the second and third day. After quinacrine instillation a further increase is observed. M: 11 absorbance.
During treatment there were small alterations in concentrations of other factors and inhibitors and the variation observed revealed no obvious pattern (table 1).
Discussion
Coagulation activity, as evidenced by thrombin activity and FPA-levels, was found in the pleural exudates before treatment. The levels showed considerable variation, some being higher than those seen after treatment (fig. 2). It is impossible to judge whether spontaneous cessation of fluid production would have occurred in some patients with high levels without treatment. During pleurodesis a marked increase in levels occurred. Most of this increase was achieved at the time of the insertion of the chest tube before quinacrine instillation. The increase in thrombin activity seen after the tube drainage accords with the fmding that, in a certain proportion of cases, fluid production stops when no irritant is used [15).
The presence of fibrin is monitored by the interaction between the coagulation and the fibrinolytic systems (16-18). The authors have demonstrated [8] that fibrinolysis is very active during the chronic exudative phase of malignant pleurisy. However, during treatment, it is significantly inhibited. Thus, pleurodesis treatment affects both the fibrinolytic and the coagulation systems and leads to fibrin deposition.
The increase in the concentrations of the platelet marker beta-thromboglobulin makes evident the activation of the platelets. The role of platelets in the mediation of immunological and inflammatory processes may be more important than is generally believed since they produce or release a great number of substances, such as thrombin, fibrinogen, platelet-derived growth factor (PDGF), and serotonin [19]. In this study we can only confirm the presence of platelet activation and
thereby the potential of this broad range of possible activities.
In formation of distant metastases the cancer cells must form vessels and connective tissue to survive in the new enviroment. In experimental research on the mechanism of cancer cell formation it has been demonstrated that cancer cells produce a strongly vasoactive substance, known as, vascular permeability factor (VPF) (20]. This factor is produced mainly in the growth zone of cancer tissue and causes the neighbouring vessels to leak. The leaking plasma forms a fibrin gel because of the action of procoagulant factors from the cancer cells [21-23]. The stroma needed for support and nutrition of the cancer nodules is formed by proliferation of fibroblasts and endothelial cells in this gel. The process seems to be monitored by coagulation and fibrinolytic activity present and by cytokinins and growth factors. The formation of fluid in malignant pleural effusion may depend on VPF which causes the vessels to form the exudate. The high fibrinolytic activity may maintain this leakage. By changing the balance between the fibrinolytic and coagulation activity towards coagulation, one may stop the leakage. The permanent effect of pleurodesis treatment may reflect the destruction of a cellular source of fibrinolytic activity, such as the mesothelial cells, which are known to disappear after severe inflammation, as in cases of tuberculosis [24).
Acknowledgement The authors thank the staff at the lung clinic, and at the blood coagulation laboratory for their devoted collaboration, and E-M. Karlsson for preparing the manuscript.
References
1. Stiksa G, Korsgaard R, Simonsson BG. - Treatment of recurrent pleural effusion by pleurodesis with quinacrine. Scand J Respir Dis, 1979, 60, 197-205. 2. Adler RH, Sayek I. - Treatment of malignant pleural effusion: a method using tube thoracostomy and talc. Ann Thorac Surg, 1976, 22, 8-14. 3. Sherman S, Grady KJ, Seidman JC. - Clinical experience with tetracycline pleurodesis of malignant pleural effusions. South Med J, 1987, 8, 716-719. 4. Felletti R, Ravazzoni C. - Intrapleural Corynebacterium parvum for malignant pleural effusions. Thorax, 1983, 38, 22-24. 5. Austin EH, Flye MW. - The treatment of recurrent malignant pleural effusion. Ann Thorac Surg, 1979, 28, 190-203. 6. Fentima IS, Millis R, Sexton S, Hayward JL. - Pleural effusion in breast cancer: a review of 105 cases. Cancer, 1981, 47, 2087-2092. 7. Dvorak HF, Harvey VS, Estrella P, Brown LF, McDonagh J, Dvorak AM. - Fibrin containing gels induce angiogenesis. Implication for tumour stroma generation and wound healing. Lab Invest, 1987, 57, 673-686. 8. Agrenius V, Chmielewska J, Widstrom 0, Blomback M. - Pleural fibrinolytic activity is decreased in inflammation as demonstrated in quinacrine pleurodesis treatment in malignant pleural effusion. Am Rev Respir Dis, 1989, 140, 1381-1385.

COAGUlATION ACTIVITY IN PLEURAL INFlAMMATION 1139
9. Kockum C, Frebelius S. - Rapid radio-immunoassay of fibrinopeptide A - removal of cross-reacting fibrinogen with bentonite. Thromb Res, 1980, 19, 589-598. 10. Abildgaard U, Lie M, Odegaard OR. - Antithrombin (heparin co-factor) assay with "new" chromogenic substrates (S-2238 and Chromozym TH). Thromb Res, 1977, 11, 549-553. 11. Bergstrom K, Blomback M. - Determination of plasma prothrombin with a reaction rate analyzer using a synthetic substrate. Thromb Res, 1974, 4, 719-729. 12. Gallimore MJ, Friberger P. Simple chromogenic peptide substrate assays for determining prekallikrein; kallikrein inhibitor and kallikrein "like" activity in human plasma. Thromb Res, 1982, 2, 293-298. 13. Widstrom 0, Chmielewska J, Blomback M. Measurements of enzymatic activities in pleural exudates with chromogenic substrates. Thromb Res, 1986, 42, 859-864. 14. Theodorsson-Norheim E. Friedman and Quade tests basic computer program to perform non-parametric twoway analysis of variance and multiple comparison on ranks of several related samples. Comput Bioi Med, 1987, 17, 85-99. 15. Izbicki R, Weyhing BT 3rd, Baker L, Caoili EM, Vaitkevicius VK. - Pleural effusion in cancer patients. A prospective study of pleural drainage with the addition of radioactive phosphorous to the pleural space as pleural drainage alone. Cancer, 1975, 36, 1511-1518. 16. Glauser Fl, Otis PT, Levine RI, Smith WR. - Coagulation factors and fibrinogen in pleural effusions. Respiration, 1976, 33, 396-402. 17. Glauser Fl, Otis PT, Levine RI, Smith WR. - In vitro pleural fluid clottability and fibrinogen content. Chest, 1975, 68, 205-208. 18. Good JT Jr, Targle DA, Hyers TM, Sahn SA. - Clotting and fibrinolytic activity of pleural fluid in a model of pleural adhesions. Am Rev Respir Dis, 1978, 118, 903-908. 19. Holmsen H. - Platelet secretion. In: Hemostasis and Thrombosis: Basic Principles and Clinical Practice. Colman et al. eds, J.B. Lippincoft Co., Philadelphia and Toronto, 1982, pp. 390-403. 20. Senger DR, Galli SJ, Dvorak AM, Perruzzi CA, Harvey VS, Dvorak HF. - Tumour cells secrete a vascular permeability factor that promotes accumulation of ascites fluid. Science, 1983, 219, 983-985.
21. Dvorak HF, Form DM, Manseau EJ, Smith BD. -Pathogenesis of desmoplasia. I. Immunofluorescence identification and localization of some structural proteins of Line 1 and Line 10 guinea-pig tumours and of healing wounds. JNCL, 1984, 73, 1195-1205. 22. Dvorak HF, Horvey VS, McDonagh J. - Quantitation of fibrinogen influx and fibrin deposition and turnover in Line 1 and Line 10 guinea-pig carcinomas. Cancer Res, 1984, 44, 3348-3354. 23. Van De Water L, Tracy PB, Aronson D, Mann KG, Dvorak HF. - Tumour cell generation of thrombin via functional prothrombinase assembly. Cancer Res, 1985, 45, 5521-5525. 24. Spriggs AI, Boddington MM. - Absence of mesothelial cells from tuberculous pleural effusions. Thorax, 1960, 15, 169-171.
Activite accrue de coagulation de la ptevre apres drainage et instillation de quinacrine dans les epachements pleuraux matins. V. Agrenius, J. Chmielewska, 0. Widstrom, M. Blombiick. RESUME: Les epanchements pleurax malins chroniques sont habituellement traites par administration intra-pleurale d'irritants provocateurs d'une reaction inflammatoire. L'inflammation induite entaine des depots de fibrine et la fin de l'exsudation de liquide.
Dans la presente etude, differents facteurs du systeme de coagulation du liquide pleural ont ete suivis au cours d'un traitement par drainage et instillation de quinacrine dans l'espace pleural. Dans la phase exsudative chronique avant traitement, l'on trouve de faibles niveaux, i\ la fois de l'activite de la thrombine et du fibrinopeptide A (FP A). Au cours du traitement, ces niveaux augmentent de fac;on marquee. La betathromboglobuline, un marqueur plaquettaire, se comporte de fac;on similaire. La prothrombine, l'antithrombine III, la prekallikreine et l'activite inhibitrice de la kallikreine, ne montrent pas de pareilles variations d'activite.
Les niveau eleves d'activite de thrombine et de FP A au cours du traitement sont le reflet d'un processus actif de fibrinogenese qui semble jouer un role important dans !'arret de l'exsudation pleurale chronique. Eur Respir J., 1991, 4, 1135-1139.