-
8/12/2019 Inf Nosocomiale Bgn 2002
1/7
1600 CID 2002:34 (15 June) Blot et al.
M A J O R A R T I C L E
Nosocomial Bacteremia Caused by Antibiotic-Resistant
Gram-Negative Bacteria in CriticallyIll Patients: Clinical Outcome
and Lengthof Hospitalization
Stijn Blot,1 Koenraad Vandewoude,1 Dirk De Bacquer,2 and Francis
Colardyn1
1Department of Intensive Care, Ghent University Hospital, and
2Department of Public Health, Ghent University, Ghent, Belgium
Population characteristics and outcomes were retrospectively
compared for critically ill patients with noso-
comial bacteremia caused by antibiotic-susceptible (AB-S; ) or
antibiotic-resistant (AB-R; )np 208 np 120
gram-negative bacteria. No significant differences in severity
of illness and comorbidity factors were seen
between groups. Patients with bacteremia caused by AB-R strains
had a longer hospitalization before the onset
of the bacteremia. The in-hospital mortality for patients with
bacteremia caused by AB-S strains was 41.8%;
for patients infected with AB-R strains, it was 45.0% ( ). A
multivariate survival analysis demonstratedPp .576
that older age ( ), a high-risk source of bacteremia (abdominal
and lower respiratory tract;Pp .009 Pp
), and a high acute physiology and chronic health evaluation
IIrelated expected mortality ( ) were.031 Pp .032
independently associated with in-hospital mortality ( ).
Antibiotic resistance in nosocomial bacteremiaP! .05
caused by gram-negative bacteria does not adversely affect the
outcome for critically ill patients.
The widespread use of broad-spectrum antibiotics is
the principal factor in the emergence of antibiotic re-
sistance. Consequently, in intensive care units (ICUs),
where the use of antibiotics is considerably greater than
in general wards [1], dealing with antibiotic-resistant
microorganisms is an almost daily challenge. This must
be considered a major problem, because the develop-
ment of newer and more-potent antibiotics cannotkeep
up with the increase in antibiotic resistance.
In ICUs, gram-negative bacteria are responsible for a
Received 3 December 2001; revised 1 February 2002;
electronically published
23 May 2002.
Presented in part: 14th Annual Congress of the European Society
of Intensive
Care Medicine, Geneva, 30 September3 October 2001.
Financial support: Fund for Scientific Research, Flanders,
Belgium (special
doctoral grant 1.9.205.02N00 to S.B.).
Reprints or correspondence: Dr. Stijn Blot, Dept. of Intensive
Care, Ghent
University Hospital, De Pintelaan 185, B-9000 Ghent, Belgium
(stijn.blot@rug
.ac.be).
Clinical Infectious Diseases 2002;34:16006
2002 by the Infectious Diseases Society of America. All rights
reserved.
1058-4838/2002/3412-0009$03.00
considerable percentage of all bloodstream infections [2].
In ICUs in the United States and Europe, patterns of
reduced susceptibility to antibiotics were found among
gram-negative bacteria [3, 4]. Despite the high prevalence
of antibiotic resistance among gram-negative bacteria
causing bacteremia, the clinical consequences of resis-
tance remain unclear. The main objective of our study
was to evaluate the relationship between antibiotic re-
sistance in gram-negative bacteria causing bacteremia
and the clinical outcomes for critically ill patients. Sec-
ondary objectives were to compare the length of the ICU
stay and hospitalization for patients with bacteremia
caused by antibiotic-susceptible (AB-S) or antibiotic-
resistant (AB-R) gram-negative strains.
METHODS
Setting. This study was performed in the ICU of the
1060-bed Ghent University Hospital in Ghent,Belgium.
The ICU has 54 beds and includes a medical and sur-
gical ICU, an ICU for cardiac surgery, and an ICU for
-
8/12/2019 Inf Nosocomiale Bgn 2002
2/7
Bacteremia Caused by Resistant Microorganisms CID 2002:34 (15
June) 1601
severely burned patients. No significant changes in mean age
of patients, length of the ICU stay, or acute physiology and
chronic health evaluation (APACHE) II score [5] were
observed
during the study period.
Study design and data collection. We conducted a retro-
spective, observational cohort study that included ICU
patients
with nosocomial, microbiologically documented bacteremia
caused by gram-negative bacteria. We compared data from
pa-tients with bacteremia caused by AB-S gram-negative bacteria
with data from patients with bacteremia caused by AB-R gram-
negative bacteria. In-hospital mortality (mortality rate for
3
evaluation points) was the principal outcome variable evalu-
ated. We also assessed secondary outcomes, including length
of stay in the ICU and in the hospital and prevalence of
acute
organ failure.
The study included critically ill adult patients who were
ad-
mitted to the ICU during a 9-year period (January 1992
December 2000). All microbiologically documented nosoco-
mial bloodstream infections are prospectively screened by
the
center for infection control. This hospital-wide case-based
sur-
veillance program was used to perform a retrospective search
for ICU patients with bacteremia caused by gram-negative
bac-
teria. Every patient whose ICU stay was complicated by this
bloodstream infection was assessed in our analysis. For ICU
patients who developed 11 case of bacteremia caused by gram-
negative bacteria, only the first episode was considered.
Patients
with hemocultures that yielded 11 type of gram-negative bac-
teria of which at least 1 strain was AB-R were included in
the
AB-R group.
Definitions. Bacteremia was considered to be nosocomial
when it was diagnosed at least 48 h after hospital
admission.Gram-negative bacteremia was defined as the presence
of
gram-negative bacteria in the blood, documented by at least
1
positive hemoculture. Hemocultures were routinely performed
when the patients temperature was 138.4C or when infection
was suspected on clinical grounds; blood samples were pro-
cessed following the BacT/Alert (Organon Teknika) procedure.
A 10-mL blood culture inoculum was standard. Antibiotic
resistance was defined as in vitro resistance to ceftazidime.
In
our hospital, ceftazidime resistance is considered to be an
in-
dicator of epidemic extended-spectrum b-lactamaseproducing
strains or hyperproducers ofb-lactamases, and, therefore, it
is
a sign of infection with organisms that are resistant to
multipledrugs [6, 7]. Because susceptibility patterns for
Pseudomonas
aeruginosavary, such isolates were considered to be AB-R
when
resistance to one of the following antipseudomonal
antibiotics
was seen: piperacillin, ciprofloxacin, ceftazidime, and
imipen-
em [8].
Antibiotic resistance was determined according to methods
for disk-diffusion testing recommended by the National Com-
mittee for Clinical Laboratory Standards [9]. For the sake
of
convenience, cases of bacteremia were designated AB-S bac-
teremia or AB-R bacteremia, depending on the antibiotic-
resistance status of the isolated organisms. During the
study
period, no changes in microbiologic laboratory techniques
were
seen. The source of the bacteremia was determined by
intensive
care physicians and microbiologists, on the basis of the
isolation
of gram-negative bacteria from the presumed portal of entry
and clinical evaluation. For the purpose of analysis, sources
ofbacteremia were divided into 3 categories: low risk
(associated
mortality, 30%), which were sinus, urinary tract,
intravenous
catheter, and soft-tissue sources; intermediate risk
(associated
mortality, 31%50%), which were primary sources of bacte-
remia; and high risk (associated mortality, 150%), which
were
lower respiratory tract and abdominal sources. Patients with
11 possible source of bacteremia (e.g., 1 low-risk and 1
high-
risk source) were considered to have a high-risk source.
Antibiotic therapy was considered to be appropriate if the
drugs used had in vitro activity against the isolated strain.
We
considered antibiotic therapy to be inadequate if the drugs
used did not have in vitro activity against the isolated
strainor if the patient did not receive antibiotic treatment. The
delay
in the initiation of appropriate antibiotic treatment was
cal-
culated from the day of onset of bacteremia. Acute
respiratory
failure was defined as ventilator dependence; acute renal
fail-
ure, as the need for renal replacement therapy; and hemo-
dynamic instability, as the need for vasopressive or
inotropic
support during the ICU stay. For the comparison of outcomes,
survival status was evaluated at 14 and 28 days after the
onset
of bacteremia and at the end of the hospital stay (all 3
evaluation
points are included in in-hospital mortality).
Statistical analysis. Continuous variables are given as
or as median (lowerupper quartile), dependingmean SD
on the distribution. Comparative analyses were done with the
Mann-WhitneyUtest or the x2 test, as appropriate. Survival
curves were prepared by means of the Kaplan-Meier method,
and univariate survival distributions were compared by the
log-
rank test. To assess the relationship between in-hospital
mor-
tality and a set of independent variables, a multivariate
survival
analysis was used (Cox proportional hazard model); hazard
ratios and 95% CIs are reported. In this multivariate
analysis,
continuous variables were handled continuously. Variables
en-
tered in the Cox regression model were required to have a
plausible relationship with mortality, to avoid spurious
asso-
ciations. Statistical analyses were performed using
Statistica,
version 4.5 (StatSoft), and SPSS, version 9.0. All tests were
2
tailed; was considered to be statistically significant.P!
.05
RESULTS
During the study period, 29,727 patients were admitted to
the
ICU. Among these, 328 patients were identified as
havinggram-
-
8/12/2019 Inf Nosocomiale Bgn 2002
3/7
1602 CID 2002:34 (15 June) Blot et al.
Table 1. Characteristics of hospitalized, critically ill
patients who had nosocomial bacteremia caused by gram-negative
bacteria.
Characteristic
Outcome of hospital stay Type of bacteremia
Death
(n p 141)
Survival
(n p 187) P
AB-S
(n p 208)
AB-R
(n p 120) P
Age, mean years SD 59 14.3 49 18.1 !.001 54 17.4 52 16.9
.303
APACHE II score, mean SD 26 9.4 22 8.0 !.001 23 9.0 23 8.6
.814
APACHE IIrelated expected mortality, mean %
SD 50 29.0 36 25.1 !.001 41 28.2 44 27.3 .305
Acute renal failure, % of patients 38.3 16.0 !.001 25.0 26.7
.431
Hemodynamic instability, % of patients 86.5 75.9 .017 77.9 85.0
.117
Acute respiratory failure, % of patients 95.7 92.0 .021 92.4
95.8 .227
Ventilator dependence, median days (lowerupper
quartile) 17 (628) 21 (834) .165 16 (527) 23 (1238) !.001
Length of ICU stay, median days
(lowerupper quartile)
Before onset of bacteremia 10 (318) 13 (624) .009 8 (3.517) 18
(933) !.001
After onset of bacteremia 8 (317) 12 (525) .002 10 (319) 11
(520) .321
Total 18 (934) 28 (1446) !.001 21 (940) 28.5 (1648) !.001
Length of hospitalization, median days
(lowerupper quartile)Before onset of bacteremia 13 (527) 16
(727) .428 11 (522) 23 (1141) !.001
After onset of bacteremia 10 (321) 59 (28117) !.001 27 (963.5)
35 (1077) .333
Total 29 (1554) 76 (44144) !.001 47 (2285) 60 (30130) .007
Mortality at 14 days, % of patients 61.0 0 26.0 26.7 .550
Mortality at 28 days, % of patients 81.0 0 34.1 35.8 .756
In-hospital mortality, % of patients 100 0 41.8 45.0 .576
NOTE. AB-R, antibiotic resistant; AB-S, antibiotic susceptible;
APACHE, acute physiology and chronic health evaluation; ICU,
intensive care unit.
negative bacteremia and were included in the study cohort (a
prevalence of 11.0 cases of gram-negative bacteremia per
1000
ICU admissions). The mean age of the patients was 54years. The
mean APACHE II score was , and the17.2 23 8.9
mean APACHE IIrelated expected mortality was 42%
. Fifty-four percent of the patients were admitted to
the27.8%
ICU after a surgical procedure; 75% of these patients had
non-
elective surgery. Twenty percent of the patients were
admitted
after experiencing trauma.
Among the 328 cases of bacteremia included in the analysis,
369 gram-negative isolates were identified. The most
frequently
detected gram-negative microorganisms were Escherichia coli
( ), Enterobacter species ( ), P. aeruginosa (np 71 np 68 np
),Klebsiellaspecies ( ),Acinetobacterspecies ( ),62 np 52 np
51
and Serratia species ( ). In 36.6% (120 of 328) of thenp 27
cases of bacteremia, the strain involved was AB-R. During
the
study period, the yearly rate of AB-R bacteremia remained
stable ( ) (data not shown).Pp .495
Outcome of hospital stay. Mortality rates at 14 days, at
28 days, and at the end of the hospital stay were,
respectively,
26%, 35%, and 43%. The characteristics of the patients who
died in the hospital and the characteristics of those who
sur-
vived are compared in table 1. Patients who died in the
hospital
generally were older and had higher APACHE II scores and
APACHE IIrelated expected mortality, and the prevalence oforgan
failure was also higher in this group. These patients had
a shorter ICU stay and a shorter hospitalization. Of all
bac-
teremia-associated factors, only infection with P.
aeruginosa
and high-risk sources of bacteremia were more prevalentamong
nonsurvivors (table 2).
Patients with AB-S bacteremia versus those with AB-R bac-
teremia. The population characteristics of patients with AB-
S gram-negative bacteremia and those with AB-R gram-neg-
ative bacteremia are listed in tables 1 and 2. Polymicrobial
bloodstream infections were more likely to occur in the AB-
R group. Furthermore, no important differences in severity
of illness were found, but patients with AB-R bacteremia had
a longer stay in the ICU, as well as in the hospital. This
seems
to be the consequence of a longer hospitalization before the
onset of the bacteremia; length of stay (both in ICU and
hospital) after the onset of the bacteremia was not
different.
Antibiotic resistance was not associated with higher mor-
tality rates (table 1). Figure 1 shows the survival curves
for
both groups from the onset of bacteremia to the end of hos-
-
8/12/2019 Inf Nosocomiale Bgn 2002
4/7
Bacteremia Caused by Resistant Microorganisms CID 2002:34 (15
June) 1603
Table 2. Factors associated with bacteremia in a study of
hospitalized, critically ill patients with nosocomial
bacteremia caused by gram-negative bacteria.
Factor
Outcome of hospital stay Type of bacteremia
Death
(n p 141)
Survival
(n p 187) P
AB-S
(n p 208)
AB-R
(n p 120) P
AB-R bacteremia 38.3 35.3 .576
Isolated microorganism
Escherichia coli 21.3 21.9 .888 30.8 5.8 !.001
Enterobacterspecies 17.0 23.5 .150 14.4 31.7 !.001
Pseudomonas aeruginosa 27.0 12.8 .001 18.8 19.2 .926
Klebsiellaspecies 12.7 18.2 .184 15.9 15.8 .994
Acinetobacterspecies 12.1 17.6 .163 4.8 33.3 !.001
Serratiaspecies 9.2 7.5 .572 9.6 5.8 .230
Polymicrobial bloodstream infection 33.3 26.2 .160 24.5 37.5
.013
Source of the bacteremia
Low risk 17.0 41.2 !.001 33.7 27.5 .247
Intermediate risk 22.7 25.1 .609 20.7 30.0 .060
High risk 60.3 32.6 !.001 45.7 42.5 .578
More than 1 possible source 9.2 10.0 .901 7.7 12.5 .152
Appropriate antibiotic therapy 89.3 94.6 .108 93.1 91.1 .547
Delay in antibiotic therapy, mean days SD 0.5 0.9 0.7 1.6 .296
0.5 0.8 0.8 2.0 .556
NOTE. Data are percentage of patients, unless otherwise
indicated. AB-R, antibiotic resistant; AB-S, antibiotic
susceptible.
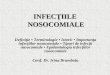
Figure 1. Survival curves for patients in the intensive care
unit who had bacteremia caused by antibiotic-susceptible(dashed
line)or antibiotic-
resistant (solid line)gram-negative bacteria ( ; log-rank
test).Pp .319
pitalization. The mortality rates for the 2 groups were very
similar ( ). At the end of the hospitalization period,Pp
.319
mortality rates for patients with AB-S bacteremia and those
with AB-R bacteremia were, respectively, 41.8% and 45.0%
( ). To adjust for differences in clinical virulence, out-Pp
.576
come comparisons for the 2 groups of patients were per-
formed, according to the different types of gram-negative
mi-
croorganisms involved. When patients were stratified by
most-prevalent bacteria, no statistically significant
difference
in mortality was seen between the 2 groups ( ; table
3).P1.05
Multivariate survival analysis. A multivariate survival
analysis demonstrated that older age, a high-risk source of
bacteremia, and a high APACHE IIrelated expected mortality
were independently associated with in-hospital mortality
(ta-
-
8/12/2019 Inf Nosocomiale Bgn 2002
5/7
1604 CID 2002:34 (15 June) Blot et al.
Table 3. Mortality rates among hospitalized, critically ill
pa-
tients with bacteremia caused by gram-negative bacteria,
strat-
ified by most frequently detected microorganism and
distributed
by antibiotic-resistance status of the isolate.
Microorganism,
resistance status
No. of
isolates
Mortality, no. (%) of patients
At 14 days At 28 days Total
Escherichia coli
AB-S 64 14 (21.9) 20 (31.3) 25 (39.1)
AB-R 7 4 (57.1) 4 (57.1) 5 (71.4)
Enterobacterspecies
AB-S 31 7 (22.6) 9 (29.0) 11 (35.5)
AB-R 37 7 (18.9) 9 (24.3) 13 (35.1)
Pseudomonas
aeruginosa
AB-S 39 12 (30.8) 17 (43.6) 25 (64.1)
AB-R 23 9 (39.1) 11 (47.8) 13 (56.5)
Klebsiellaspecies
AB-S 34 6 (17.6) 9 (26.5) 9 (26.5)
AB-R 18 5 (27.8) 8 (44.4) 9 (50.0)
Acinetobacterspecies
AB-S 10 0 1 (10.0) 1 (10.0)
AB-R 41 8 (19.5) 14 (34.1) 17 (41.5)
Serratiaspecies
AB-S 21 7 (33.3) 10 (47.6) 10 (47.6)
AB-R 6 3 (50.0) 3 (50.0) 3 (50.0)
NOTE. Differences in mortality for patients
withantibiotic-susceptible(AB-
S) and patients with antibiotic-resistant (AB-R) bacteremia did
not reach sta-
tistical significance at any time point ( ).P! .05
Table 4. Factors associated with in-hospital mortality among
hospitalized, critically ill patients with bacteremia caused
by
gram-negative bacteria.
Variable Hazard ratio (95% CI) P
Age 1.01 (1.001.02) .009
High-r isk source of bacteremia 1.33 (1.031.72) .031
APACHE IIrelated expected
mortality 1.71 (1.052.79) .032
Acute renal failure 1.32 (0.981.76) .065
Pseudomonas aeruginosa
bacteremia 1.33 (0.961.85) .085
NOTE. Associations were assessed using multivariate survival
analysis
(Cox proportional-hazard model). APACHE, acutephysiology and
chronic health
evaluation.
ble 4). Acute renal failure and bacteremia caused byP. aeru-
ginosahad an association with in-hospital mortality that wasof
borderline significance ( ).P!.1
DISCUSSION
It is presumed that infections caused by AB-R bacteria
result
in higher mortality, longer hospitalizations, and greater
costs
than do infections caused by AB-S bacteria, although few
data
support this intuitive concept [10]. The assumption that in-
fections caused by AB-R bacteria are associated with a
higher
mortality rate may be based on the possibility that
appropriate
antibiotic therapy will be initiated later for such infections
than
for infections caused by AB-S bacteria. Although some
studies
have described very high mortality rates in association with
infections caused by AB-RP. aeruginosaand Acinetobacter bau-
mannii[8, 11], the causal link between antibiotic resistance
and
fatal bacteremia remains unclear.
Comparisons of the outcomes for patients with AB-R bac-
teremia and for patients with AB-S bacteremia can be
difficult
to perform: important differences in demographic character-
istics between the populations are repeatedly observed in
stud-
ies of bacteremia caused by AB-R gram-positive bacteria
[1214]. In the present study, no important differences in
severity of illness (as measured by the APACHE II score) or
prevalence of acute organ failure hampered the outcome com-
parison. Polymicrobial bloodstream infections were seen more
frequently among patients with AB-R bacteremia. Although
this is considered to be an ominous sign [15, 16], it has
been
demonstrated elsewhere that the mortality associated
withpolymicrobial bacteremia in ICU patients is not necessarily
higher than that associated with monomicrobial bacteremia
[17]. In our study, polymicrobial bacteremia was not asso-
ciated with higher in-hospital mortality on either
univariate
or multivariate analysis.
Our data revealed that the mortality associated with AB-R
gram-negative bacteremia is not higher than that associated
with AB-S bacteremia. Although mortality is high in both
groups of patients, the observed mortality rates are in line
with
the APACHE IIrelated expected mortality. In a retrospective
study, Menashe et al. [18] also found no significant increase
in
mortality among patients with bacteremia caused by
extended-spectrumb-lactamaseproducing Enterobacteriaceae (50%,
vs.
38% among patients with bacteremia caused by nonextended-
spectrumb-lactamaseproducing isolates; ), but theirPp .367
study cohort was small ( ). Harbarth et al. [16], in anp 55
large retrospective study, also failed to demonstrate that
anti-
biotic resistance had a major clinical effect on outcome for
patients with gram-negative bacteremia. However, the
hospital-
wide setting and large proportion of cases of community-
acquired bacteremia (61%) in that study hampers comparison
with the results we obtained.
Previous studies have identified important associations be-
tween antibiotic resistance and negative outcome for
patients
with gram-negative bacteremia [1921]. However, causality re-
mains unclear, and differences in study populations impede
comparison with the present study.
It is a possible weakness in our study that the outcome
comparison between the 2 groups of patients might be con-
-
8/12/2019 Inf Nosocomiale Bgn 2002
6/7
Bacteremia Caused by Resistant Microorganisms CID 2002:34 (15
June) 1605
founded by differences in the clinical virulence of the types
of
gram-negative bacteria involved [16]. For example, 80%
ofAci-
netobacter species, which are considered to be low-virulence
pathogens, were AB-R, whereas 37% ofPseudomonasisolates,
which are known to be extremely virulent, were AB-R. Re-
gardless, in the multivariate survival analysis, no
individual
microorganism was recognized as being an independent pre-
dictor of mortality. Therefore, we assume that the
confoundingeffect of differences in clinical virulence of the
different types
of bacteria seen in our study is of minor importance.
However,
outcome evaluation after stratification for different bacteria
can
be interesting.
In a prospective cohort study involving patients with bac-
teremia caused exclusively byEnterobacterspecies, Chow et
al.
[21] describe greater morbidity and mortality among patients
with bacteremia caused by AB-REnterobacterspecies. Our study
included 68 ICU patients with bacteremia caused byEntero-
bacter, 37 of whom were infected with AB-R strains. Although
these numbers are small and, therefore, are difficult to
interpret,
the mortality rates in these subgroups were nearly equal
(35.5%
and 35.1%, respectively), raising doubts about whether a
worse
prognosis was associated with bacteremia caused by AB-REn-
terobacterspecies in our population. Also, when data were
strat-
ified by other frequently detected gram-negative microorgan-
isms, no statistically significant differences in the mortality
rates
were found for the AB-S group and the AB-R group (table 3).
Nonetheless, the differences in the mortality rates for
patients
with bacteremia caused by AB-S or AB-R strains ofKlebsiella
species, E. coli, and, in particular, Acinetobacterspecies,
which
reached borderline significance ( ), are noteworthy. TheseP!
.1
results, however, must be interpreted cautiously because of
thesmall numbers of patients included.
It can be presumed that bacteremia caused by AB-R bacteria
may have a worse prognosis because of the delay in
initiation
of appropriate antibiotic therapy [22, 23]. Especially when
high-
virulence microorganisms such as P. aeruginosa are involved,
early initiation of appropriate therapy is crucial to the
survival
of the patient [24, 25]. In our study, patients with AB-R
bac-
teremia were treated appropriately at a rate similar to that
for
patients with AB-S bacteremia. The delay in the initiation
of
appropriate treatment was longer in the AB-R group, but the
difference we found was of no significance, either
statistically
or clinically (table 2).The high rate of administration of
appropriate therapy that
was achieved in our ICU population can be explained by 3
factors: (1) consideration of previous colonization, as
assessed
by regular site-specific surveillance cultures (3 times
weekly),
(2) initial administration of broad-spectrum antibiotic
therapy,
and (3) close interaction between the physician, clinical
mi-
crobiologists, and clinical infectious diseases consultants.
This
strategy appeared to contribute to a delay in administration
of
appropriate antibiotic treatment that was short (!1 day)
overall
in our study. Surveillance sampling was found to have a high
specific and negative predictive value, because colonization
pre-
ceded infection in almost all patients who had P. aeruginosa
infection in the ICU [26, 27]. On the other hand, performing
surveillance cultures routinely is expensive. Furthermore,
whether this policy has greater clinical benefits than does
ini-
tiation of blind therapy with broad-spectrum antibiotics is
stillcontroversial. It is well understood that blind therapy is
re-
stricted to a smaller spectrum, once microbiologic
identification
is completed, yet it might be assumed that this promotes the
emergence of AB-R microorganisms, because there is more
exposure to broad-spectrum antibiotics. Our strategy is to
re-
serve these agents for patients with sepsis whose condition
is
deteriorating and for whom no isolate has been obtained from
the presumed septic focus and for patients who have micro-
biologically proved superinfection.
Patients with AB-R bacteremia had a significantly longer
stay
in the ICU, as well as in the hospital. However, when length
of ICU stay and length of hospitalization (from the day of
theonset of bacteremia to discharge or death) were compared, no
difference was found. We conclude from this that the excess
length of stay, both in the ICU and the hospital, is a result
of
a longer ICU and hospital stay before the onset of the
bacte-
remia. Consequently, it appears that cases of AB-R
bacteremia
are not responsible for the increased need for hospital
resources
among these patients but that risk factors for the
acquisition
of AB-R infections are the major triggers of this problem.
In conclusion, we found that AB-R gram-negative bacteremia
is not associated with higher mortality than is AB-S gram-
negative bacteremia in critically ill patients. AB-R
bacteremia
is associated with a longer stay in the ICU, as well as in
the
hospital. This, however, is the consequence of a longer stay
before the onset of the bacteremia, whereas length of stay
in
the ICU and length of stay in the hospital after onset of
the
bacteremia in the 2 group of patients were not different.
References
1. Roder BL, Nielson SL, Magnussen P, et al. Antibiotic usage in
an
intensive care unit in a Danish university hospital. J
Antimicrob
Chemother1993; 32:63342.
2. Vincent J-L, Bihari DJ, Suter PM, et al. The prevalence of
nosocomial
infection in intensive care units in Europe: results of the
EuropeanPrevalence of Infection in Intensive Care (EPIC) study.
JAMA 1995;
274:63944.
3. Burwen DR, Banerjee SN, Gaynes RP. Ceftazidime resistance
among
selected nosocomial gram-negative bacilli in the United States.
National
Nosocomial Infections Surveillance System. J Infect Dis
1994;170:
16225.
4. Hanberger H, Garcia-Rodriguez J, Gobernado M, et al.
Antibiotic sus-
ceptibility among aerobic gram-negative bacilli in intensive
care units
in 5 European countries. JAMA 1999; 281:6771.
5. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II:
a
severity of disease classification system. Crit Care Med 1985;
13:81829.
-
8/12/2019 Inf Nosocomiale Bgn 2002
7/7
1606 CID 2002:34 (15 June) Blot et al.
6. Sirot D. Extended-spectrum plasmid-mediated beta-lactamases.
J An-
timicrob Chemother 1995; 36(Suppl A):1934.
7. Colardyn F, Decruyenaere J, Verschraegen G, et al. Failure of
selective
digestive decontamination (SDD) to control an epidemic of
coloni-
zation by extended spectrum b-lactamaseproducingKlebsiella
pneu-
moniae(CAZ) [abstract IM-9]. In: Program and abstracts of the
37th
Interscience Conference on Antimicrobial Agents and
Chemotherapy
(Toronto). Washington, DC: American Society for
Microbiology,1997:
365.
8. Carmeli Y, Troillet N, Karchmer AW, Samore MH. Health and
eco-
nomic outcomes of antibiotic resistance in Pseudomonas
aeruginosa.
Arch Intern Med 1999; 159:112732.
9. National Committee for Clinical Laboratory Standards (NCCLS).
Per-
formance standards for antimicrobial disk susceptibility tests.
NCCLS
document M2A5. Villanova, PA: NCCLS, 1993.
10. Mehta RM, Niederman MS. Antibiotic resistance in the
intensive care
unit. In: Vincent J-L, ed. Yearbook of intensive care 2001.
Berlin:
Springer-Verlag, 2001:15161.
11. Rello J, Rue M, Jubert P, et al. Survival in patients with
nosocomial
pneumonia: impact of the severity of illness and the etiologic
agent.
Crit Care Med 1997; 25:18627.
12. Blot S, Vandewoude K, Colardyn F. Staphylococcus
aureusinfections
[letter]. N Engl J Med 1998; 339:20256.
13. Soriano A, Martinez J, Mensa J, et al. Pathogenic
significance of meth-
icillin resistance for patients with Staphylococcus
aureusbacteremia.
Clin Infect Dis 2000; 30:36873.14. Bhavnani SM, Drake JA,
Forrest A, et al. A nationwide multicenter,
case-control study comparing risk factors, treatment, and
outcome for
vancomycin-resistant and -susceptible enterococcal bacteremia.
Diagn
Microbiol Infect Dis 2000; 36:14558.
15. Reuben AG, Musher DM, Hamill RJ, Brouke I. Polymicrobial
bacte-
remia: clinical and microbiologic patterns. Rev Infect Dis
1989;11:
16183.
16. Harbarth S, Rohner P, Auckenthaler R, Safran E, Sudre P,
Pittet D.
Impact and pattern of gram-negative bacteraemia during 6 y at a
large
university hospital. Scand J Infect Dis 1999; 31:1638.
17. Rello J, Quintana E, Mirelis B, Gurgui M, Net A, Prats G.
Polymicrobial
bacteremia in critically ill patients. Intensive Care Med1993;
19:225.
18. Menashe G, Borer A, Peled N, et al. Clinical significance
and impact
on mortality of ESBL-producing gram-negative isolates in
nosocomial
bacteremia [abstract 1425]. In: Program and abstracts of the
39th In-
terscience Conference on Antimicrobial Agents and
Chemotherapy
(San Francisco). Washington, DC: American Society for
Microbiology,
1999:616.
19. Krcmery V Jr, Spanik S, Krupova I, et al. Bacteremia due to
multi-
resistant gram-negative bacilli in neutropenic cancer patients:
a case
controlled study. J Chemother 1998; 10:3205.
20. Mehlhaff DL, Briceland L, Tobin E, et al. Comparison of
survival in
patients having bacteremia with and without extended-spectrum
beta-
lactamase producing Enterobacteriaceae (ESBLPE) [abstract J98].
In:
Program and abstracts of the 36th Interscience Conference on
Anti-
microbial Agents and Chemotherapy (New Orleans). Washington,
DC:
American Society for Microbiology,1996:237.
21. Chow JW, Fine MJ, Shlaes DM, et al. Enterobacterbacteremia:
clinical
features and emergence of antibiotic resistance during therapy.
Ann
Intern Med 1991; 115:58590.
22. Kollef MH, Sherman G, Ward S, Fraser VJ. Inadequate
antimicrobial
treatment of infections: a risk factor for hospital mortality
among
critically ill patients. Chest 1999; 115:46274.
23. Ibrahim EH, Sherman G, Ward S, Fraser VJ, Kollef MH. The
influence
of inadequate antimicrobial treatment of blood stream infections
on
patient outcomes in the ICU setting. Chest 2000; 118:14655.24.
Bodey G, Jadeja L, Elting L. Pseudomonasbacteremia:
retrospective
analysis of 410 episodes. Arch Intern Med 1985; 145:16219.
25. Vidal F, Mensa J, Almela M, et al. Epidemiology and outcome
of
Pseudomonas aeruginosabacteremia, with special emphasis on the
in-
fluence of antibiotic treatment. Arch Intern Med 1996;
156:21216.
26. Bertrand X, Thouverez M, Talon D, et al. Endemicity,
molecular di-
versity and colonisation routes ofPseudomonas aeruginosain
intensive
care units. Intensive Care Med 2001; 27:12638.
27. Langer M, Carretto E, Haeusler EA. Infection control in ICU:
back
(forward) to surveillance samples. Intensive Care Med 2001;
27:15613.