Embed Size (px)
Citation preview

Intense pulsed light devices:Are claimed outputparameters valid?
Poster Authors:
Dr. Mario Trelles,Instituto Médico Vilafortuny, Cambrils, Spain
Godfrey Town,Laser Protection Adviser, Haywards Heath, UK
C. Ash,Optoelectronics engineer, University of Wales Swansea, School of Physical Sciences, Swansea, UK
Correspondence to: Mario A Trelles MD PhD, Instituto Médico Vilafortuny /ANTONI DE GIMBERNAT FOUNDATION
Av. Vilafortuny 31, E-43850 Cambrils, Spain. Tel: +34 977 361320 Fax: +34 977 791024 E-mail: [email protected]
Presented at the 16th European Academy of Dermatology and Venerology (EADV) in Vienna, 16th – 20th May 2007

AbstractBackground:High quality IPLs can offer simple, safe and effective treatments for long-term hair removal, removal of benign vascular andpigmented skin abnormalities, skin rejuvenation and acne treatments. However, significant differences in clinical outcomehave been recorded among different IPLs despite apparently identical settings. This study investigates the differences inoptical outputs of eighteen IPLs in daily clinical use in the UK and proposes a correlation between light-tissue interactionand spectral output as measured by time-resolved photo-spectrometry.
Methods:Seven key parameters were identified as having an important role to play in the way light interacts with the skin, andtherefore have an important function in patient safety and effective treatment. Simple methods were devised to measureenergy density, pulse duration, pulse profile, homogeneity of treatment spot, averaged spectral output, time resolvedspectral data outputs and physical dimensions of transmission block. These evaluations were made on site in workingclinics between patient appointments.
Results:Using the assessment methods in this study, fluence values in some IPLs were found to be outside of the tolerancesallowed for Class IV medical lasers. Several IPLs, which claimed matching of pulse durations to the thermal relaxation timesof specific follicular or vascular targets were measured to have pulse durations that were significantly shorter or longer thanclaimed. Some IPLs claiming ‘square pulse’ characteristics failed to show constant spectral output across the duration ofthe pulse or sub-pulses. Poor spot homogeneity was noted in some systems which could lead to significant side effects at higher output levels.
Conclusions:This study provides a method to determine accurately all relevant parameters of the emitted light pulses from IPLs. In particular, the ‘spectral footprints’ measured using time-resolved spectroscopy may have important clinical consequencesin terms of anticipating different light-tissue interactions and hence clinical efficacy and safety and identify potential for side effects.
IntroductionMost IPL systems have a number of parameters, which the operator can modify to match the patient’s Fitzpatrick skin type and treatment selected. These parameters may include: exposure time of intense light (pulse duration or total durationof sub-pulses) in ms, energy density (fluence) in J/cm2 and choice of cut-off filters to eliminate unwanted wavelengths. Each of these parameters is important to produce the most desirable thermal profile in the melanin of the hair follicle orepidermal pigmented lesions, or in the haemoglobins in the blood vessel, whichever is the major chromophore beingtargeted. Positive clinical outcomes are widely documented in the literature using a number of well-established IPL devices.The recent increase in the number of IPLs produced worldwide without thorough clinical data to support manufacturer’sclaims of efficacy, safety and reliability raises the question of the suitability of these devices for their intended purpose.
IPLs can be categorised into two main types by the method which they use to generate and deliver the energy required for light-based treatments, they are:
1. Free discharge
2. Constant current
A free discharge system applies a large electrical charge to a capacitor or a number of capacitors in parallel thendischarges the entire stored energy directly though the flashlamp, this discharge profile is characterised by a rising/fallingslope (Figure 1). As the current through a xenon flashlamp starts with a low initial value, the light spectrum is shiftedpredominantly towards the infrared end of the spectrum. As the current increases exponentially, the spectrum shifts towardsthe blue part of the electromagnetic spectrum, then as the current falls away, the optical spectrum moves back to the redend of the spectrum [1,2,3]. This effect of ‘spectral jitter’ during the pulse means that the optical output not only variesduring the pulse but may also differ significantly from one energy setting to another.
32
Most free discharge systems are unable to generate true long pulse durations to match the thermal relaxation time (TRT) of the target structure (eg hair follicle or blood vessel). The TRT of a typical hair follicle is in the order of 25 – 55 ms andtherefore, for optimum thermal destruction of the hair, the light energy should be delivered in the same time regimen [4,5,6].Most conventional free discharge IPLs therefore deliver a train of shorter, high energy sub-pulses with variable on and offtimes to generate an overall duration and average energy density in the range of the TRT of the target chromophore.
Whilst this method may produce a clinically measurable result, it is by no means the most efficient way of achieving longterm stable hair reduction or long term vessel clearance with the minimal number of treatments and low incidence ofadverse effects.
A constant current (‘square pulse’) system generates energy in the same way as a free discharge system by charging alarge capacitor or a number of capacitors in parallel, the difference between the two systems is the way in which the energyis delivered to the flashlamp. Constant current systems create a square pulse discharge profile through the xenon flashlamp(Figure 2) at an optimum energy level and this is repeated without variation. As a result, little energy is wasted and theconstant current system can operate efficiently and effectively at lower energy levels producing true long single pulses orgroups of square sub-pulses.
The duration of the discharged pulse or sub pulses of intense light may be measured using a reversed biased photodiode,acting as a light dependant switch (Figure 3). This method records total xenon lamp output pulse duration recorded by thephotodiode including all of the optical energy in the decay slope.
Most manufacturers represent the spectral output of their IPL as an average spectral measurement taken across the entirepulse duration as measured above. It is useful to note the approximate distribution of energy across the differentwavelengths from a xenon lamp characterised by the bulk of the energy in the range 530 nm – 800 nm with several specificatomic lines between 820 nm and 920 nm (Figure 4).
Figure 3—Measurement of pulse duration using a reversed biasedphotodiode acting as a light dependent switch.
Figure 4—Standardised Spectral Output Measurement showing IPL ‘E’ with a sharp cut-off at 530 nm and typical xenon lamp spectral profile:
intensity is irrelevant.
Figure 1—Oscilloscope trace of a rising-falling xenon lamp discharge slope,typical of a free discharge IPL (IPL ‘B’).
Figure 2—Oscilloscope trace of a ‘square pulse’ xenon lamp dischargeprofile of a constant current IPL (IPL ‘E’).

MethodsSeven key parameters were identified as having an important role to play in the way light interacts with the skin, andtherefore having an important role in patient safety and effective treatment. The authors used previously published methods[7 – 9] for standardised measurements to quantify the following parameters:
energy density (fluence) for various typical pulse patterns over the claimed lifetime of the lamp, to establish whether there is any significant deterioration compared with accepted standards for lasers (which might result in under-treatment);
pulse duration, to establish whether TRT for specific chromophores could be matched accurately to the pulse duration;
pulse profile, i.e. electrical discharge (oscilloscope trace) to the flashlamp vs. manufacturers’ claims to determine whether the discharge to the xenon lamp is constant (‘square’) or variable (‘free discharge’);
the homogeneity of the treatment spot produced by the IPL glass transmission block, to determine whether any ‘hot spots’ or low energy areas are produced (that may lead to over- or under-treatment);
dimensions of the crystal transmission block contacting the skin surface, to allow accurate calculation of energy density values;
averaged spectral output across the entire pulse, to identify cut-off filter accuracy and any unwanted or potentially hazardous (UV) wavelengths;
the time-resolved ‘spectral footprint’ of the intense pulsed light (IPL) across the entire pulse duration to allow detailed examination of the spectral structure of individual IPL pulses and consider potential treatment implications.
Time-Resolved SpectrumFew studies have attempted to document methods for measuring IPL pulse durations, and it appears that no previouslypublished study has examined the time-resolved spectral output of IPLs i.e. across each millisecond of the pulse duration[9,10]. Time-resolved spectroscopy is intended to demonstrate the light energy distribution and stability during a light pulse.These measurements on free discharge vs. constant current systems may be helpful in determining whether there is apotential impact on efficacy of absorption of light by the primary skin chromophore targets of interest.
Conventional spectrometers need relatively long sample times, rather like the exposure time on a camera and it is thisaveraging effect that dampens or eliminates the variations in spectral peaks during the pulse. Time-resolved spectralmeasurements make it possible to assess variations in spectral composition during the light pulse and hence considerpotential treatment implications.
The time-resolved spectrum in this study was produced using a fast spectrometer and its counterpart Spectra Suitesoftware (OceanOptics Inc, Dunedin, Florida, USA). This spectrometer and software has the capability of sampling thespectrum of light with a minimum integration time of 1 ms by generating 1000 full spectral scans per second across theentire pulse. Time-resolved spectral data of IPL outputs was captured and stored with an optical resolution of amonochromatic source measured as Full Width Half Maximum (FWHM) resolution of 0.035 nm. This fast spectrometer usesa 2048-element linear silicon CCD-array detector (Sony ILX511, Sony Corp, Tokyo, Japan) to capture data into memoryevery millisecond interfaced to a standard PC via a USB 2.0 port for later analysis.
The spectrometer is externally triggered using a breakout box and because of the relatively fast pulse duration of an IPLsystem the sampling was taken over an extended time period to ensure capture of the data.
The source of the intense white light from the IPL system and the spectrometer optical fibre was separated by a distance of150 cm to 180 cm to prevent saturation of exposed light upon the CCD array within the spectrometer. During testingsuitable Shade 3 IPL protective eyewear was worn by the investigators.
IPL spectral outputs were calculated and graphically modeled using MathCAD™ software. For optimal, uniform visualrepresentation of the three-dimensional images, several specific visual aspects were chosen to show the results including,front view of spectral wavelength, time-resolved spectrum view, 3D ‘flying view’ of all the dimensions in proportion and aview of the plasma discharge.
54
Results & DiscussionCalibrationThe key optical component requiring calibration in an intense pulsed light device is the applicator head containing the xenonflash lamp assembly. This flash lamp has a finite operating life during which output values deteriorate following decay ofparts (deposition of material from the plasma on the inside wall of the lamp envelope, decay of coloured glass cut-off filters,erosion of the optical surfaces of dichroic filters and reflectors, etc.). Therefore, the more shots that are fired, the weaker thelamp becomes and the more variable the output spectrum of light produced.
Some more expensive devices include rudimentary built-in energy meters and through software programming allowcalibration adjustments to be made automatically to compensate for lamp energy density deterioration.
Many devices have i-button control over total available shots in each applicator hand set and upon expiry require the userto either return the entire applicator and umbilical to the supplier for refurbishing / exchange or call out a service technicianto change lamps, filters, etc., on site.
Several manufacturers have user-replaceable lamp cartridges with a pre-programmed number of shots requiring exchangeupon expiry.
Some devices had ‘unlimited’ lamps with only a recommendation when to change the lamp. These systems depend uponpreventive maintenance by a factory-trained service engineer routinely checking that the output values remain withinmanufacturer’s tolerances. In this study, these IPLs were shown to have the least reliable parameters.
Energy DensityStated device fluence is assumed by users to be the energy density delivered evenly per cm2 from the whole of the crystalblock contact surface to the skin and the fluence values displayed by screen software are believed by operators to beaccurate (at least to the nearest whole number). For treatments utilizing ‘selective photothermolysis’ the light energy isabsorbed by chromophores in the skin, such as melanin and oxyhaemoglobin and converted into heat energy. As energy isabsorbed, the temperature of the chromophore increases and tissue goes through biological changes. The ideal fluence willraise the temperature of the chromophore to a level that causes damage to the target but does not lead to adverse sideeffects such as burns or blisters. Even the most simple IPL devices at least allow the user some control over energydensity, which makes reproducible measurement very important to ensure consistent output and prevent under or over treatment.
Measurements in this study were taken for the most popularly used and the highest IPL settings. Maximum fluencemeasurements are recorded in Table 1 and fluence results were plotted on graphs for the example eighteen devices againstthe system displayed fluence (or manufacturers’ claimed fluence in the user manual if not displayed on the IPL screen)(Figures 5 & 6). By measuring devices in routine daily use, measurements were effectively taken at different stages in the
Figure 5—Standardised Energy Density Measurement showing IPL ‘E’ whose energy output is well within the accepted tolerance of ±20% for Class 4 medical lasers (EN 60825).

76
Figure 6—Standardised Energy Density Measurement showing IPL ‘F’ whose output energy is only ca. 25% of the stated energy on the device screen displayand which is well outside the accepted tolerance of ±20% for Class 4 medical lasers (EN 60825).
Figure 7—30 IPL applicators were measured at maximum fluence of which 11 were more than 20% below and 8 were more than 10% above fluence levelsgiven on the device display or claimed in user manuals, even where brand-new lamps were tested.
FIgure 8—9 IPL devices out of 18 had applicators that were outside of the standard for medical Class 4 lasers (> ±20%)
manufacturers’ claimed warranty lifetime of the applicator or lamp/filter assembly, which allowed observation of the degreeof deterioration in fluence against claimed values.
Using this test method, 30 IPL applicators were measured at maximum fluence of which 11 were more than 20% belowand 8 were more than 10% above fluence levels given on the device display or claimed in user manuals, even where brandnew lamps were tested (Figure 7). Altogether 9 IPL devices out of 18 had applicators that were outside of the standard formedical Class 4 lasers (> ±20%) (Figure 8). The authors considered the accuracy of higher fluence values to be of greatestimportance owing to the risk of under- or over-treatment.
This study measured several device (IPLs ‘F’ and ‘P’) where the maximum fluence value displayed was vastly lower than theamount of energy actually delivered to skin and measured fluences were frequently outside the generous tolerance rangefor lasers (±20%) set out in BS EN Standard 60825. The shape of long cylindrical Xenon lamps in many intense pulsed lightdevices and the presence of a simmer circuit not running along the entire length of the visible discharge tube in theapplicator head may suggest an uneven output from the crystal glass transmission block with the greatest concentration ofenergy produced at the centre.
For assurance of continuing reliability of the lamp and filter it is useful if these measurements can be repeated throughoutthe lamp lifetime. If output drifts significantly from the results recorded with a new lamp then procedures should be in placeto replace the lamp or treatment head.
Pulse DurationMeasured pulse and sub-pulse durations using a reversedbiased photodiode were recorded as an oscilloscope traceto permit measurement of pulse and sub-pulse durationsand intra-pulse delay times (Figure 9). This test also servedto validate the number of sub-pulses in a pulse train. Usingthis method, there was generally a poor correlationbetween manufacturers’ claims or system-displayed valuesand the pulse durations measured. The data measured forsix of the eight medical CE-marked IPLs was consistentwith displayed values (where given).
Only fourteen of 31 pulse duration measurements werewithin ±20% of the manufacturers stated or system-displayed values. E.g. IPL ‘B’ claimed single pulsedurations of 5 ms, which were measured at 15 – 17 msacross all programs and settings.
In one example IPL program for IPL ‘F’, one sub-pulse wasfound to be entirely missing which correlated with the lowfluence measured for that program compared with otherson the same device. Such discrepancies are clearly unacceptable as they may lead to selecting incorrect fluence valuesand under- or over-treatment of the patient leading to either ineffective treatment or unwanted side effects (Figure 10).
Study Ref Stated Pulse Duration (ms) Measured Pulse Duration (ms)
A 3 x 10 ms = 30 3 x 6 ms = 18
A1 14 14.52 x 2.5 ms = 15 2 x 3 ms = 15.5
B 5 15–17
C 5 15–17
D 50 5110–15 no data
E 10–50 10–51 ms
F 20–150 missing pulses20–151 missing pulses
G 10 620 6.620 8.7
H 5.5/5.5/5.5 5.4 6.4 7.0
I short:5.5/5.5 (2) 5.5/5.5 (2)med:3.6/3.6/3.6 (3) 4.0/4.0/4.0 (3)long:3.6/3.6/3.6 (3) 4.5/4.5/4.5 (3)
J 40 40
K 34.8 37123 121
L 15 black 2.215 blonde 5
M 3 35 5
N 35 13235 13210 24
O 40 42
Q 30/40/50 30/40/50
Figure 9—Only 14 of 29 pulse duration measurements were within ±20% of the manufacturers stated or system-displayed values.

98
Lamp Discharge Current: Pulse ProfileMany IPL manufacturers promote a ‘square’ or ‘controlled’pulse shape (meaning the pulse of electrical energydischarged across the xenon lamp) and colourful artist’sillustrations are often used rather than shown as an actualoscilloscope trace. It was apparent that almost all claimsrecorded in this study made in manufacturers’ literature fora ‘square pulse’ were not reflected in our exampleoscilloscope measurements as the pulses were usually thetypical xenon discharge slope (increasing/decreasing) of afree discharge system.
Only IPLs ‘E’ and ‘G’ exhibited a true single square pulseshape confirming that they used partial discharge capacitortechnology although close pulse-stacking in devices ‘A’and ‘O’ effectively achieved the same pulse shape and device ‘D’ showed a nearly square pulse shape. Only a comparisonof time-resolved spectral output will demonstrate whether there is any spectral deterioration across the entire pulse durationwhen comparing these devices (Figure 11).
A constant current through the xenon flashlamp may be critically important in the treatment of certain skin conditions toachieve the desired photo therapeutic effect. Potentially, much of the discharged energy may be wasted due to unevenwavelength distribution of the light energy across the pulse duration.
Figure 10—Standardised Lamp Discharge Duration Measurements showingIPL system ‘F’ which is a triple pulse system with one pulse missing, thus
one third of the energy is lost. System display values: T1 3 ms, T2 20 ms, T34.5 ms, T4 30 ms, T5 4.5 ms (T3 4.5 ms sub-pulse missing). It is assumed
that this is due to an error when writing the system software or whencalibrating the microprocessor control system.
Figure 11—Only IPLs ‘E’ and ‘G’ exhibited a true single square pulse shape confirming that they used partial discharge capacitor technology although closepulse-stacking in devices ‘A’ and ‘O’ effectively achieved the same pulse shape and device ‘D’ showed a nearly square pulse shape.
IPL ‘E’
IPL ‘C’
IPL ‘Q’
IPL ‘G’
IPL ‘A’
IPL ‘B’
Spot Homogeneity MeasurementThe homogeneity of the distribution of output energy at the surface of the quartz or sapphire transmission block isimportant as uneven distribution of energy to the patient’s skin during discharge of the flashlamp will create over- or under-treated areas. This difference in energy distribution usually occurs where energy is focused into the centre of thetransmission block and thus the perimeter has a lower energy density. In this case, the skin only receives adequate energyin circular or elliptical “hot spots” within the glass transmission block surface area, resulting in the operator having to overlap the treatment areas to achieve effective treatment.
Uneven energy distribution may also occur if the side walls of the transmission block are highly polished whereby theenergy may be focused around the perimeter of the block’s skin contact surface creating an “picture framing” effect with anarea of ineffective energy located in the centre leading to potential blotchiness on the patient’s skin where dischromia or hair regrowth appears in discreet patches.
The homogeneity of the energy distribution is measured in this study by capturing the intense pulsed light discharge 100times per second using a digital video camera (Logitech Webcam, Fremont CA, USA) and storing the individual frames on a laptop computer for selection and subsequent analysis. The best quality compression ratio of the software used bymodern digital cameras is utilized to reduce the amount of data stored, which results in the frame rate being dramaticallydecreased. As this study measured a flash of intense light with pulse durations in the order of tens of milliseconds, the test apparatus had to have the capability to save as many frames-per-second as possible to provide sufficient images tocapture the development of the plasma phase in the Xenon lamp. To generate as many frames-per-second as possible,in this study a screen recorder with MJPEG compression at 100 frames-per-second at its highest quality setting was used,which acted as a secondary data recorder and allowed a high frames-per-second capture without compromising quality of the images.
To prevent saturation of the diode array detectors at the rear of the digital camera, a sheet of white, 1.5 mm thick PTFEwas used to heavily filter the amount of light being exposed to the camera.
From a general assessment of the homogeneity profiles produced by the camera system by the authors, it was onlypossible to grade profiles as poor, moderate or good. This approximation was capable of exposing major discrepancies(Figure 12) and give a general overview of light distribution but did not quantify results.
Explanation of Spectral GraphsThe spectrum analysis of light emitted from flashlamps contains both discrete line structure and continuum radiation. The continuum radiation is blackbody radiation, characteristic of the temperature of the plasma in the discharge. The sharppeaks in the distribution of the wavelength spectrum are due to specific energy transitions of electrons interacting with thexenon plasma. Figure 13 shows a spectral graph of a typical IPL system, with 60% of the total energy found between 550 – 700 nm (the key wavelengths for hair depilation and vascular abnormalities) and illustrates the proportionaldistribution of the wavelengths.
The line spectra in the infrared region of the graph are more dominant, where bound transitions between energy levels ofatoms and ions dominate and these lines are known as the “Paschen Series”. The xenon plasma results in the emission of photons with a continuous range of energies; thus, the spectrum from the xenon ions causes a continuous spectrum. This is known as a bound-free transition and was discovered in 1939 by Rupert Wildt [11].
A sharp cut off point usually around 500 to 600 nm can be seen on the graphs. This is due to a dichroic coated filterformed on the rear surface of the treatment transmission glass block or a separately located dichroic or coloured glassabsorption filter to remove any wavelengths below the chosen cut-off. Shorter wavelengths in the blue and ultraviolet regionof the spectrum are heavily absorbed in melanin may burn the patient’s skin and are therefore removed. In addition, most
Figure 12—Example Standardised Spectral Output Measurement showing (left) IPL ‘F’ with applicators with cut-off filters at 560 nm and 690 nmdemonstrating poor (shallow slope) cut-off profiles and inaccurate cut-off (620 nm red rather than 690 nm as stated in the manufacturer’s user manual) and
(right) IPL ‘I’ with cut-off filters at 645 nm, 695 nm and 755 nm showing good but inaccurate (steep slope) cut-off profiles compared with manufacturer’soperators manual: intensity is irrelevant.

1110
flashlamp cylindrical envelope walls containing the inert xenon or krypton gas are of cerium- or titanium-doped quartz orsilica and have the property of filtering out the most harmful of these wavelengths in the ultra violet region i.e. below 400 nm.Measurements in this study included both an average value for the complete pulse or pulse train and time-resolved spectralmeasurements produced by the tested IPL applicators. The spectrum graphs of the entire output are useful as they give anindication of accuracy of cut-off filter wavelengths and the presence of unwanted ultraviolet or infrared wavelengths. Of the30 applicators tested, 7 IPLs measured more than 1% and two measured more than 2% of unwanted UV output below400 nm when cut-off filters were set significantly higher (Table 2 and Figure 14).
Measurements of 29 applicators showed nineteen (65.5%)with cut-off filters that were inaccurate by more than 20 nmversus the claimed cut-off value given by the manufacturer.Only 10 applicators (34.5%) were within 20 nm of thestated cut-off. (Figure 15)
A few systems also use filters to cut off infraredwavelengths as these are absorbed predominantly in tissuewater and therefore do not contribute to specific heating ofeither melanin or haemoglobin. The results show clearlythat for free discharge systems, despite pulse durationsquoted by the manufacturer, the optical energy is often onlyconcentrated in a narrow time domain of the pulse. Thisdifference between specified pulse duration and effectiveoptical output may explain unwanted side effects or sub-optimal treatments.
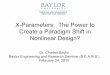
Figure 16 shows both the schematic and thecorresponding time-resolved ‘spectral footprint’ for both IPL‘C’ (free discharge) and IPL ‘E’ (square pulse). The pulseduration of IPL ‘C’ was measured at 15 – 17 ms andshows an analogous rising and falling optical output. The‘useful’ energy, however, is concentrated into only a fewmilliseconds. IPL ‘E’ shows almost perfectly stable spectralemission across the entire 50 ms pulse. Both the atomicpeak (825 nm) in the background and the bulk of theenergy in the foreground spread almost evenly across theentire pulse duration (peak at 555 nm) with only slightattenuation of optical output towards the end of the pulsecan be clearly identified.
0.12
%
0.10
%
0.17
%
0.38
%
0.52
%
0.7%
4.62
%
10.0
5%
10.1
1%
9.42
%
8.87
%
7.71
%
6.7%
5.98
%
5.26
%
4.33
%
3.58
%
2.92
%
2.43
%
1.71
%
1.47
%
4.31
%
0.86
%
1.0%
2.63
%
1.68
%
0.74
%
0.54
%
0.45
%
0.42
%
0.17
%
0.07
%
Figure 13—Averaged spectral distribution graph for a typical xenon lampspectral profile measuring less than 10% of total light energy above 790 nmand less than 0.5% above 950 nm. The bulk of the energy (90%) is in the
range of 530 – 790 nm.
14 filters(47% of tested filters)
10 filters(33% of tested filters)
4 filters(13% oftested filters)
2 filters(7% oftested filters)
0% UV<1% UV1-2% UV>2% UV
Figure 14—Shorter wavelengths in the ultraviolet region of the spectrum mayburn the patient’s skin or may be hazardous to the operator’s eyes and are
therefore removed. Of the 30 applicators tested, 6 IPLs measured more than1% and two measured more than 2% of unwanted UV output below 400 nm
when cut-off filters were set significantly higher.
560nm Handpiece690nm Handpiece
695nm Handpiece645nm Handpiece755nm Handpiece
Figure 15—Standardised Spectral Output Measurement showing (left) IPL‘F’ with applicators with cut-off filters at 560 nm and 690 nm demonstrating
poor (shallow slope) cut-off profiles and inaccurate cut-off (620 nm redrather than 690 nm as stated in the manufacturer’s user manual) and (right)IPL ‘I’ with cut-off filters at 645 nm, 695 nm and 755 nm showing good but
inaccurate (steep slope) cut-off profiles compared with manufacturer’soperators manual: intensity is irrelevant.
Wavelength (nm)
180
1100
510
15
T ime (ms)
Inte
nsi
ty
Inte
nsi
ty
Wavelength (nm)
T ime (ms)
60
40
20180
1100
More red/IR More red/IR
More blue
Constant current
Partial dischargeFree discharge
Wastedenergy
Rel
ativ
ein
ten
sity
Pulse duration (ms)
Figure 16—(above) Schematic illustration of the difference in the spatial and temporal characteristics of a free discharge and partial discharge pulse to an IPLxenon lamp and (below) time-resolved spectral measurements of example IPL devices: free discharge (IPL ‘C’) and partial discharge (IPL ‘E’).
ConclusionsMeasurement of IPL devices is becoming an important issue but is still at a very early stage after being neglected for yearsbecause of commercial pressures and a lack of regulation. However the popularity of IPL as a treatment is growing andthere is now a definite need for measurement to help improve both safety and efficacy.
The measurements in this paper will give technicians working with IPLs a useful tool for checking output consistency anddiagnosing performance issues. Discrepancies can be seen between measured parameters and manufacturer claims butcaution must be exercised with this comparison because the techniques described in the paper are subject to on-goingdevelopment. In particular, traceability to national standards is a pre-requisite to accurate, absolute, as opposed to relative,measurements. On the other hand, comparing different devices is useful as discrepancies highlight the need for legislationto produce standard measurement procedures.
This study has determined easily reproducible test methods for key parameters of IPL devices and tested their validity oneighteen IPL systems in daily use. As mentioned, further work is required if measurement results are to be made traceableto national standards. It is also hoped that an improved homogeneity test can be developed to provide objectivemeasurable values to ensure even distribution of energy across skin contact areas.
Time-resolved optical spectroscopy is useful for service engineers to evaluate the performance of IPL systems in the fieldand for manufacturers to construct improved systems for future clinical treatments. Expert clinicians may use graphicalrepresentations of pulse parameters including time-resolved spectroscopy as a tool to evaluate likely treatment efficacy andidentify potential for side effects.
Based upon the limited number of different units and applicators measured in this study, the variability of output data versusmanufacturers’ claims indicates a need for wider studies of device parameters and the introduction of internationalstandards for intense pulsed light devices.

References
1. Trelles M A. The efficacy of a low energy constant spectrum emission device for hair epilation Poster at European Academy of Dermatology and Venereology12 – 16th October 2005.
2. Clement M, Daniel G, Trelles M. Optimising the design of a broad-band light source for the treatment of skin J Cosmetic Laser Ther 2005; 7:177 – 189
3. Clement M, Kiernan M, Ross Martin GD, Town, G. Preliminary Clinical Outcomes Using iPulse™ Intense Flash Lamp Technology and the Relevance of Constant Spectral Output with Large Spot Size on Tissue Australasian Journal of Cosmetic Surgery 2006; 1:54 – 59.
4. Clement M, Omi T. The use of a constant spectrum, uniform temporal profile intense pulsed light source for long term hair removal J Cosmetic Laser Ther 2006; 8:138 – 145.
5. Anderson R.R, Parish J.A Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science 1983; 220(4596):524 – 7
6. Altshuler GB, Anderson RR, Mainstein D Zenzie HH, Smirnov MZ. Extended Theory of selective photothermolysis Laser Surg Med 2001; 29:416 – 32
7. Town, G. Output Data & Claims made for Intense Pulsed Light Devices: A Comparative Evaluation. Abstract No: 122, Lasers Surg Med, 26th Annual Meeting, Boston, April 5th – 9th, 2006.
8. Town G, Ash C. Evaluation of Intense Pulsed Light Devices Using Standized Methodology. Abstract No: 41, Lasers Surg Med, 27th Annual Meeting, Grapevine, USA. April 11th – 15th, 2007
9. Town G, Ash C, Eadie E, Mosley H. Measuring key parameters of intense pulsed light (IPL) devices. J Cosmetic Laser Ther 2007; In Press.
10. Clarkson DM. The role of measurement of pulse duration and pulse profile for lasers and intense pulsed light sources. J Med Eng Technol 2004; 28:132 – 6.
11. Wildt, R., ”Electron affinity in Astrophysics,” Astrophysical Journal 1939; 89:295.