Embed Size (px)
DESCRIPTION
Letný bioptický seminár SD-IAP Senec 21-22.6.2013. MUDr. Juraj Marcinek, PhD. Prípad SD-IAP 480. Ústav patologickej anatómie a Konzultačné centrum hematopatológie UNM a JLF UK. - PowerPoint PPT Presentation
Citation preview

Letný bioptický seminár SD-IAPLetný bioptický seminár SD-IAPSenec 21-22.6.2013Senec 21-22.6.2013
MUDr. Juraj Marcinek, PhD.MUDr. Juraj Marcinek, PhD.
Prípad SD-IAP 480Prípad SD-IAP 480
Ústav patologickej anatómie a Konzultačné centrum Ústav patologickej anatómie a Konzultačné centrum
hematopatológie UNM a JLF UK hematopatológie UNM a JLF UK

Letný bioptický seminár SD-IAP 9 - 10.11.2012. Prípad SD-IAP 480
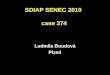
68 yer old man – Ca capitis pancreatis (cT3 N1 MX)68 yer old man – Ca capitis pancreatis (cT3 N1 MX)
makroskopic finding: vhite tumorous mas of 18mm rising aroud pancreatic duct in themakroskopic finding: vhite tumorous mas of 18mm rising aroud pancreatic duct in the
head of pancreashead of pancreas
under duodenal serosa visible tumorous mass corresponding to LNunder duodenal serosa visible tumorous mass corresponding to LN

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480
?

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480
PASPAS PASPAS
PASPAS PAS-KPAS-K

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480
CK20CK20CK7CK7
CK17CK17 CK19CK19

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480
CEApCEApCEAmCEAm
trypsinetrypsine chymotrypsinechymotrypsine

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480
HepPar1HepPar1
villinvillin AFPAFP
CD10CD10

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480
TTF1TTF1
ΒΒ-catenin-catenin glypican 3glypican 3
SchmorlSchmorl
?hepatoid carcinoma of pancreas with focal ductal differentiation

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480
hepatoid carcinomas – heterogenous neoplasms with morphologic and phenotypic hepatoid carcinomas – heterogenous neoplasms with morphologic and phenotypic
resemblance to hepatocellular carcinoma (HCC)resemblance to hepatocellular carcinoma (HCC)
- most common arise in stomach (since Ishikura et al. 1985)- most common arise in stomach (since Ishikura et al. 1985)
- less common in ovary, testis, esophagus, duodenum, pancreas, - less common in ovary, testis, esophagus, duodenum, pancreas,
colon, rectum, lung, gallblader, urinary tract, uterus, vaginacolon, rectum, lung, gallblader, urinary tract, uterus, vagina
- morphology: trabecular / pseudoacinar / solid growth pattern- morphology: trabecular / pseudoacinar / solid growth pattern
polygonal cells with abundant cytoplasm polygonal cells with abundant cytoplasm
central vesicular nuclei with prominent nucleolicentral vesicular nuclei with prominent nucleoli
pleomorphic cells, sinusoidal vascularisationpleomorphic cells, sinusoidal vascularisation
intracytoplasmic PAS+ hyalinne globulesintracytoplasmic PAS+ hyalinne globules
occasional bile productionoccasional bile production
- usually at least partial tubular/tubulopapilar - usually at least partial tubular/tubulopapilar
growth patterngrowth pattern
- immunohistochemistry: markers of hepatocellular differetiation:- immunohistochemistry: markers of hepatocellular differetiation:
AFP, HepPar1, polyklonal CEA, CD10, glypican 3, albumin mRNAAFP, HepPar1, polyklonal CEA, CD10, glypican 3, albumin mRNA
- usually not all markers are present- usually not all markers are present
- coexpression of cytokeratins atypical for HCC- coexpression of cytokeratins atypical for HCC

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480
hepatoid carcinoma of pancreas – rare neoplasmhepatoid carcinoma of pancreas – rare neoplasm
- larges study contains 15 cases (Kai et al., Pathology - larges study contains 15 cases (Kai et al., Pathology
International 2012) International 2012)
- clinically unspecific symptoms- clinically unspecific symptoms
- can have elevated serum AFP (7/15) - can have elevated serum AFP (7/15)
- can differentiate form acinar/ductal/islet cells of - can differentiate form acinar/ductal/islet cells of
pancreaspancreas
- common associated with other cellular carcinoma - common associated with other cellular carcinoma
component (endocrine features 5/15, ductal component (endocrine features 5/15, ductal
carcinoma 3/15, acinar carcinoma 1/15) carcinoma 3/15, acinar carcinoma 1/15)
prognosis – hepatoid carcinomas have generally poor prognosis prognosis – hepatoid carcinomas have generally poor prognosis
- most tumors are aggressive with metastasis at time of diagnosis- most tumors are aggressive with metastasis at time of diagnosis
- mainly hematogenous metastases into liver, vascular permeation (veins)- mainly hematogenous metastases into liver, vascular permeation (veins)
- pancreatic hepatoid carcinomas – variable prognosis depending on stage at - pancreatic hepatoid carcinomas – variable prognosis depending on stage at
the time of diagnosis the time of diagnosis

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480
differential diagnosis of hepatoid carcinomas from: differential diagnosis of hepatoid carcinomas from:
1. hepatocellular carcinoma with extrahepatic spreading – problematic to impossible1. hepatocellular carcinoma with extrahepatic spreading – problematic to impossible
hepatoid carcinomas - morphologically similar, but often contain variabile amounth hepatoid carcinomas - morphologically similar, but often contain variabile amounth glandular or tubulopapilary adenocarcinomatous componentglandular or tubulopapilary adenocarcinomatous component - immunohistochemical pattern of HCC usually incomplete with - immunohistochemical pattern of HCC usually incomplete with strong coexpression of cytokeratins atypical fo HCC (CK19, strong coexpression of cytokeratins atypical fo HCC (CK19, CK17, CK20)CK17, CK20) - CEAm+ in adenocarcinomatous component- CEAm+ in adenocarcinomatous component - CEAp+ in both components (luminal/canalicular in hepatoid c.)- CEAp+ in both components (luminal/canalicular in hepatoid c.) - most important are clinical informations of liver finding- most important are clinical informations of liver finding - HCC spread into pancreas is a rare (2,7-5,6%) and late finding- HCC spread into pancreas is a rare (2,7-5,6%) and late finding - multiple liver nodules without chronic liver disease associated - multiple liver nodules without chronic liver disease associated with other large large gastrointestinal tumor are prone to be with other large large gastrointestinal tumor are prone to be metastasesmetastases

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480
differential diagnosis of hepatoid carcinoma of pancreasdifferential diagnosis of hepatoid carcinoma of pancreas
2. acinar cell carcinoma (solid variant)2. acinar cell carcinoma (solid variant)
– – morphologically similar cells, granular PAS+ cytoplasm, uniform, basal oriented nuclei morphologically similar cells, granular PAS+ cytoplasm, uniform, basal oriented nuclei
and „palisading“ of nuclei around vessels, distinct nucleoli and „palisading“ of nuclei around vessels, distinct nucleoli
- absence of dezmoplastic stroma- absence of dezmoplastic stroma
- immunohistochemically: lipase+, trypsin+, chymotripsin+- immunohistochemically: lipase+, trypsin+, chymotripsin+
CK19-, CK7-, CK20-, AFP (10% positive)CK19-, CK7-, CK20-, AFP (10% positive)

Letný bioptický seminár SD-IAP 21 – 22.6.2013. Prípad SD-IAP 480
differential diagnosis of hepatoid carcinoma of pancreasdifferential diagnosis of hepatoid carcinoma of pancreas
3. pancreatoblastoma3. pancreatoblastoma
- mainly in children (1st. decade of live)- mainly in children (1st. decade of live)
- trabecular and solid growth pattern with/without other pancreatic structures- trabecular and solid growth pattern with/without other pancreatic structures
(acinar, ductal, endocrine, stromal)(acinar, ductal, endocrine, stromal)
- presence of atypical squamoid corpusles- presence of atypical squamoid corpusles
- a mesenchymal component with stromal hyalinisation may be present - a mesenchymal component with stromal hyalinisation may be present
- immunohistochemically: lipase+, trypsin+, chymotripsin+, AFP+, HMW-CK+- immunohistochemically: lipase+, trypsin+, chymotripsin+, AFP+, HMW-CK+

Tlstá, Veľká Fatra, 2.7.2008 pohľad na Ostredok a Ostrú
Ďakujem za pozornosť