Embed Size (px)
Citation preview

Management of disease recurrence after renal
transplantation
Patrick NiaudetNéphrologie Pédiatrique
Centre de référence des maladies rénales génétiques
Hôpital Necker-Enfants Malades, Paris
ESPN, September 2008

Recurrence of primary disease
Disease Recurrence frequency Graft loss
SRNS with FSGS 30% 40-50%
MPGN
Type I 20-30% 30-40%
Type II 80-100% 20%
Membranous nephropathy 10% 40%
IgA nephropathy 30% 15-30%
SHP nephritis <1% <1%
Systemic vasculitis 10-20% <5%
SLE < 2% rare
Anti-GBM disease < 5% 50%
D+HUS exceptionnal
Atypical HUS 30-50% >50%
Amyloidosis 25 % rare
Primary hyperoxaluria 100% 80%

Recurrence of nephrotic syndrome
after renal transplantation
• Occurs in about 30% of patients with SRNS and FSGS
• Extremely low rate of recurrence in genetic forms of the disease
• Proteinuria is most often of rapid onset

Recurrence of nephrotic syndrome
after renal transplantation• Risk factors for recurrence :
– duration of disease shorter than 3 years
– disease starting after the age of 6 years
– diffuse mesangial proliferation on initial biopsy
– recurrence on a previous graft
• Graft failure occurs in 60% of patients with
recurrence
• CsA does not prevent recurrence but improves graft
survival

Recurrence of nephrotic syndrome according to the age at onset of
disease
% with recurrence
age > 6 years 54
age < 6 years 22 (p < 0.01)
age < 3 years (n=41) 7
age < 1 year (n=15) 0
Enfants Malades

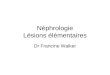
Removal of circulating factor lowers protein
excretion in recurrent NS
20
40
60
80
100 Plasma exchangeProtein absorption
Prett Tt Day 7 Day 15Dantal et al, NEJM 1994, 330: 7
Pu

Prophylactic plasma exchanges
• Recurrence in 4 of 6 pts in the non prophylactic group
• Recurrence in 5 of 15 pts in the prophylactic group
• 7 recurrent pts received PE with remission in 6
(Ohta et al, Transplantation, 2001)

Plasma exchanges plus cyclophosphamide
• Dall’Amico et al (AJKD, 1999)– Sucessfull in 9 of 11 children– Persistent remission in 7 with a follow-up of 32 months
• Cheong et al (NDT, 2000)– Complete remission in 3/6– Partial remission in 3/6

Rituximab failed to improve nephrotic syndrome in four adult renal transplant patients with early recurrent FSGS refractory or dependent on plasmapheresis
Yabu JM et al AJT 2008; 8: 222-7

Intravenous CsA for recurrent nephrotic syndrome
after RT
• Between March 1991 and July 2007, recurrence
has occurred in 22 grafts in 21 children
• CsA was immediately administered IV, at an
initial dose of 3 mg/kg/d and the dose was
adjusted in order to maintain whole blood
levels above 250 ng/ml
• Plasma exchanges, 2 to 10 sessions, in 9
patients
Enfants Malades

Intravenous CsA for recurrent nephrotic syndrome after RT
• One pt with delayed recurrence (day 18) did not respond to IV CsA + PE
• Among the 21 early recurrences (within the first week) :
–1 pt did not respond to IV CsA + PE
–3 pts showed partial remission (proteinuria without nephrotic syndrome) after IV CsA + ACEI
–17 pts (77%) entered into complete remission within 20 days (D12 to D40)
•with CsA alone in 11 cases
•with CsA + PE in 7 cases
–11 of the 17 pts are still in CR 1 to 14 years later

Recurrence of NS after RT
• Seems to be mediated by a circulating 50-kD plasma protein, which is bound to Ig
• Identification of the protein ?
• Clinical usefullness of the presence of the « permeability » factor ?
• Living donor or cadaveric donor ?
• Best therapy
– Plasma exchanges ± cyclophosphamide
– IV cyclosporine ± plasma exchanges
– Others ?

Atypical HUS
• Mutations in genes of the complement pathway (50%)
• Anti-CFH antibodies
• Von Willebrand factor cleaving protease deficiency (ADAMTS13 gene mutation)
• Defects of vitamine B12 metabolism
• Idiopathic autosomal recessive disease
• Idiopathic autosomal dominant disease

Atypical HUS : French Pediatric Registry
CFH IF MCP No
N (46) 10 (22%)
6 (13%)
7 (15%)
22 (48%)
Outcome
Death 2 1 0 1
ESRD 6 2 2 6
Mutation
(Sellier-Leclerc et al, JASN 2007)

Atypical HUS : posttransplant course
• 24 grafts in 15 patients
• 12 graft failures during the first year (50%)– 8 from thrombosis– 3 from recurrence– 1 from CMV
• 4 graft failures later (recurrence in 2, rejection in 2)
• 2 functioning grafts at 2yr despite recurrence• 6 grafts with good outcome 5 to 15 yr later
(Sellier-Leclerc, JASN 2007)

Atypical HUS : recurrence after RT
CFH IF MCP No
Nb pts 34 8 10 20
Recurrence 76% 88% 20% 30%
Graft loss (from recurrence at 1yr)
81% 100% 1/2 83%
Richards 2003 ; Fremeaux-Bacchi 2004, 2006, 2007 ; Kavanagh 2005 ; Bresin 2005 ;
Caprioli 2006 ; Heinen 2006 ; Venables 2006 ; Nilsson 2007 ; Geelen 2007 ; Sellier-Leclerc 2007
Mutation

Possible therapy
• FFP ± PE• Eculizumab (monoclonal antibody)
– Binds to C5, inhibiting its clivage to C5a and C5b
– Prevents the release of C5a and the formation of C5b-C9
– Reduces transfusion requirements in paroxysmal noctural hemoglobinuria (lack of GPI-linked-proteins that protect cells from complement-mediated attack)

Atypical HUS with CFH mutation : results of liver
transplantation
• Initial experience with combined L+K (2) or L (1) but no plasma therapy : 2 deaths and 1 with neurological sequellae (Remuzzi, Cheong)
• Combined L+K with extensive plasma therapy : 4 children with excellent outcome and no recurrence (Saland, Jalanko)– PE with FFP before surgery– FFP ± PE during surgery– Anticoagulation after surgery

Consensus Conference (Bergame, Dec 2007)
Indications for combined liver-renal or isolated liver transplantation
• CFH mutation– First graft lost from recurrence– Another family member with the same mutation and who lost a graft from recurrence
– Patient with a mutation reported to be associated with graft loss from recurrence
• Not enough data for HUS associated with other complement mutations

Conservative treatment of primary hyperoxaluria
• High fluid intake over 24h : 3l/m2
• Solubilization of calcium oxalate : potassium citrate
• AGT coenzyme : Pyridoxine [G170R]
• Avoid surgical removal of calculs
• Low oxalate diet
• Oxalobacter formigenes (OxabactTM : 2 x 107 UFC/d) : ongoing trial

0
20
40
60
80
100
120
140
160
180
200
0 24 48 72 96 120 144 168 192 216 240
time (months)
GFR (Schwartz formula) mL/mn/1.73m2
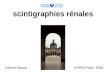
Evolution of GFR in children with PH1 under conservative
treatment
GFR at initiation : 92 ml/mnAt last examination• Stable GFR 19/27pts• Decreased GFR 8/27pts• ESRF 4/27pts
(Société de Néphrologie Pédiatrique)

Extra renal complications in PH1
• bone disease
• retinal deposits with amblyopia
• conduction system abnormalities
• cardiomyopathy
• artery calcifications and ischemia
• livedo reticularis , gangrene
• polyneuritis
Oxalate accumulates in tissues when plasma oxalate reaches 50mol/l
4 to 8 mmol of oxalate are produced every day

Liver + kidney
Liver then kidney
Kidney Liver
Infantile (ESRF<2yr)
Second choice
First choice X X
GFR 40 to 60 mL/min
X X X ?
GFR 20 to 40 mL/min
First choice X
? If Vit B is active and G170R mutation
X
GFR<20 mL/min Second
choiceFirst choice X X
Transplantation strategy (P. Cochat)

Management of primary hyperoxaluria
• The best treatment of oxalosis is conservative and
preventive when possible
• A careful protocol must be applied and maintained
for preventing recurrence on the graft
• The most important point is to maintain high urine
output after renal transplantation (low oxalate
concentration)
• Dialysis is indicated only in case of oliguria

24 h Oxaluria in 3 children after liver/ kidney transplantation
2000200015001500100010005005000000
250250
500500
750750
10001000
12501250
15001500
17501750
20002000
Days post Days post graftinggrafting
µmol/ dayµmol/ day

Evolution of extra renal complications after liver-
kidney transplantation
• Bone disease improves very slowly but complete healing was reported after several years
Toussaint et al Am J Kidney Dis 1993 21 54
• Conduction system abnormalities and cardiomyopathy may rapidly be reversed after some weeks
Rodby et al. Am J Med 1991 90 498
Fyfe et al. Am J Cardiol 1995 75 210

Conclusion
• Recurrent disease in a renal transplant remains an important cause of chronic allograft dysfunction and graft failure
• Patients and their families should be informed of the recurrence risk, potential therapeutic options and prognosis
• The indication of retransplantation when a primary graft has been lost to recurrence is a difficult issue