Embed Size (px)
Citation preview

1
Motor Neuron Disease- Clinical Aspects -
Sanjay Kalra, MD, FRCPC Division of Neurology, Department of Medicine
Centre for Neuroscience Department of Biomedical Engineering
S Kalra, UofA
Case
A 53 year old man noticed progressive clumsiness in his right hand. He had difficulty writing and buttoning his shirt.
He was reassured by a physician that he probably had a pinched nerve in his neck.
S Kalra, UofA
Case (cont)
6 months later he was unsteady when walking and was liable to trip.
On examination he had wasting and weakness of hand muscles (right worse than left). The legs were spastic and reflexes were increased in the legs.
S Kalra, UofA
Case (cont)
MRI Cervical Spine – Normal
Electromyography – active lower motor neuron disease in the arms and legs
ALS was diagnosed – 9 months after his initial symptoms.
S Kalra, UofA
Case (cont)
3 months later his speech became slurred and he started coughing when eating or drinking. Eventually a feeding tube (PEG) was inserted.
Physiotherapy and analgesics were required to control shoulder pain.
2 years after his symptoms began, he was restricted to a wheelchair with no functional strength remaining in his arms.
S Kalra, UofA
Case (cont)
He slept poorly and fatigue worsened as respiratory muscle strength deteriorated. Non-invasive ventilation (NIV) alleviated this significantly. After several months he needed NIV and morphine during the day for shortness of breath.
Several episodes of pneumonia were treated successfully with antibiotics.
2
S Kalra, UofA
Case (cont)
He had dodged the discussion of personal directives throughout his illness, but eventually made it clear that he did not want invasive measures (tracheostomy with mechanical ventilation).
Death was peaceful at home 3 years after his first symptoms (no choking, suffocating).
S Kalra, UofA
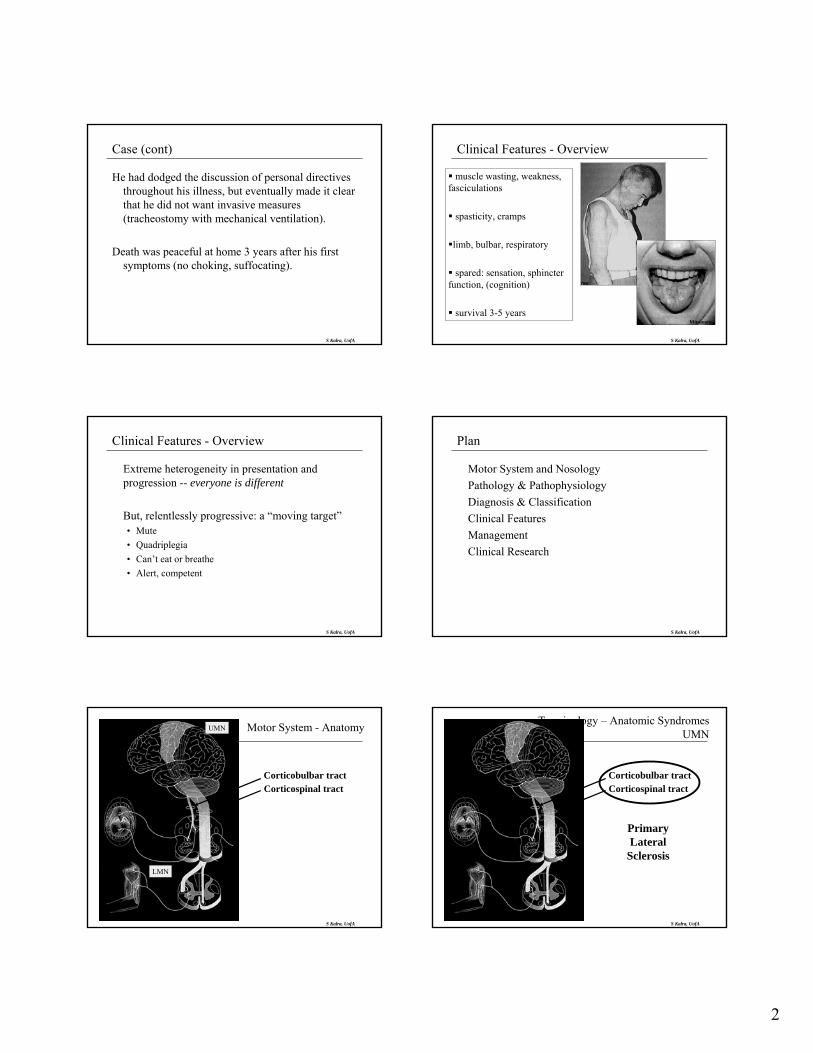
Clinical Features - Overview
muscle wasting, weakness, fasciculations
spasticity, cramps
limb, bulbar, respiratory
spared: sensation, sphincter function, (cognition)
survival 3-5 yearsMitsumoto
S Kalra, UofA
Clinical Features - Overview
Extreme heterogeneity in presentation and progression -- everyone is different
But, relentlessly progressive: a “moving target”• Mute• Quadriplegia• Can’t eat or breathe• Alert, competent
S Kalra, UofA
Plan
Motor System and Nosology Pathology & Pathophysiology Diagnosis & Classification Clinical Features Management Clinical Research
S Kalra, UofAAdapted from Belsh and Schiffman, 1996
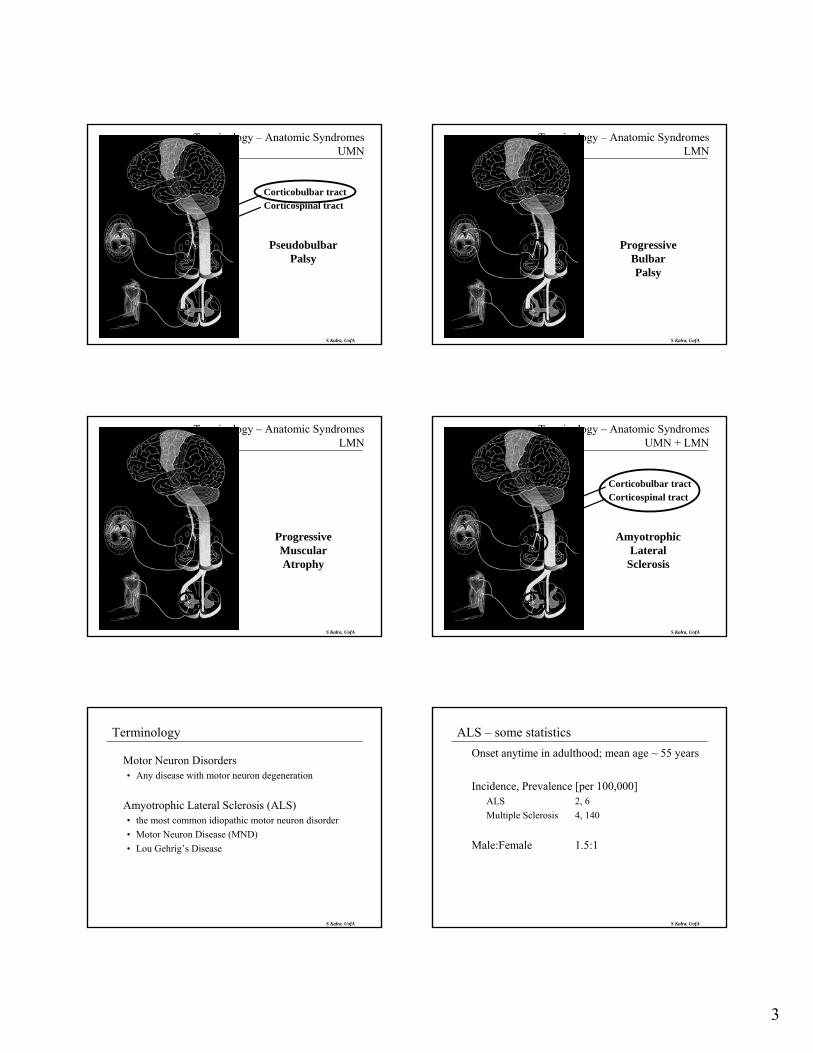
UMN
LMN
Corticobulbar tractCorticospinal tract
Motor System - Anatomy
S Kalra, UofA
Corticobulbar tractCorticospinal tract
Terminology – Anatomic SyndromesUMN
PrimaryLateral
Sclerosis
3
S Kalra, UofA
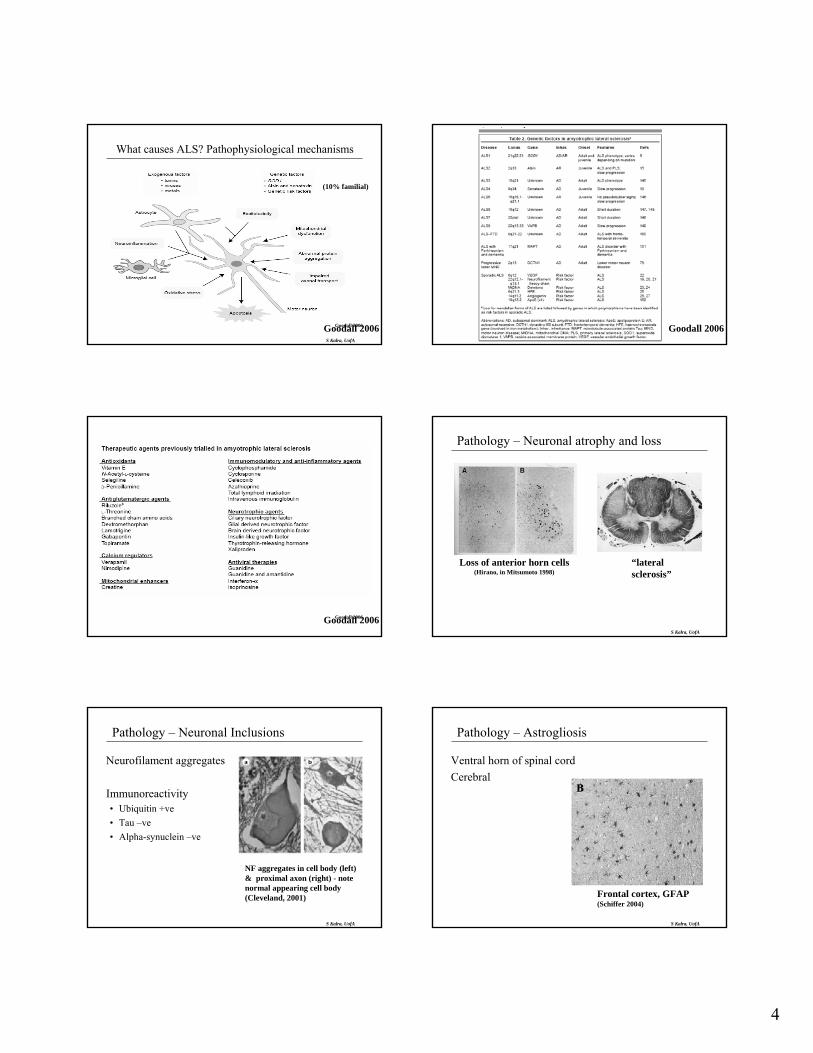
Corticobulbar tractCorticospinal tract
Terminology – Anatomic SyndromesUMN
PseudobulbarPalsy
S Kalra, UofA
Terminology – Anatomic SyndromesLMN
ProgressiveBulbarPalsy
S Kalra, UofA
Terminology – Anatomic SyndromesLMN
ProgressiveMuscularAtrophy
S Kalra, UofA
Corticobulbar tractCorticospinal tract
Terminology – Anatomic SyndromesUMN + LMN
AmyotrophicLateral
Sclerosis
S Kalra, UofA
Terminology
Motor Neuron Disorders• Any disease with motor neuron degeneration
Amyotrophic Lateral Sclerosis (ALS)• the most common idiopathic motor neuron disorder• Motor Neuron Disease (MND)• Lou Gehrig’s Disease
S Kalra, UofA
ALS – some statisticsOnset anytime in adulthood; mean age ~ 55 years
Incidence, Prevalence [per 100,000]ALS 2, 6Multiple Sclerosis 4, 140
Male:Female 1.5:1
4
S Kalra, UofA
Goodall 2006Goodall 2006
(10% familial)
What causes ALS? Pathophysiological mechanisms
Goodall 2006
Goodall 2006Goodall 2006
S Kalra, UofA
Pathology – Neuronal atrophy and loss
“lateralsclerosis”
Loss of anterior horn cells(Hirano, in Mitsumoto 1998)
S Kalra, UofA
Pathology – Neuronal Inclusions
Neurofilament aggregates
Immunoreactivity• Ubiquitin +ve• Tau –ve• Alpha-synuclein –ve
NF aggregates in cell body (left) & proximal axon (right) - note normal appearing cell body (Cleveland, 2001)
S Kalra, UofA
Pathology – Astrogliosis
Ventral horn of spinal cord Cerebral
Frontal cortex, GFAP(Schiffer 2004)

5
S Kalra, UofA
Pathology – Activated Microglia
Lipid-laden microgliawithin degeneratingcorticospinal tract
Ramified activatedmicroglia adjacentto spinal motor neuronsin spinal cord
Strong 2003
S Kalra, UofA
Pathology – Cognitively impaired ALS
Superficial spongiform degeneration in layers II/III of frontal lobe
Higher density and distribution of dystrophic neurites and Tau+veinclusions (Yang, 2003)
Wilson 2001
S Kalra, UofA
MR Volumetry: Motor and Extramotor Atrophy
Chang 2005
S Kalra, UofA
Positron Emission Tomography (PET)
Lloyd 2000
GABAA receptor ligand: [C11]-Flumazenil
Motor and extra motor involvement also indicated by:-11CR-PK11195 (activated microglia)
S Kalra, UofA
Spectrum: ALS FTD
Clinical Pathology / Imaging
Ubiquinated inclusions in FTD and ALS• both contain fragmented protein TDP-43 (Lee, Science,
2006)
S Kalra, UofA
ALS is a multisystem disease
Neuronal and non-neuronal elements Motor cortex and extra-motor cortex
6
S Kalra, UofA
Diagnosis
El Escorial Criteria• combined upper AND
lower motor neuron signs • progression
UMN
• Spasticity, hyperreflexia, Babinski sign
LMN
• Atrophy, fasciculations, hypotonia, hyporeflexia
• EMG
UMN
LMN
S Kalra, UofA
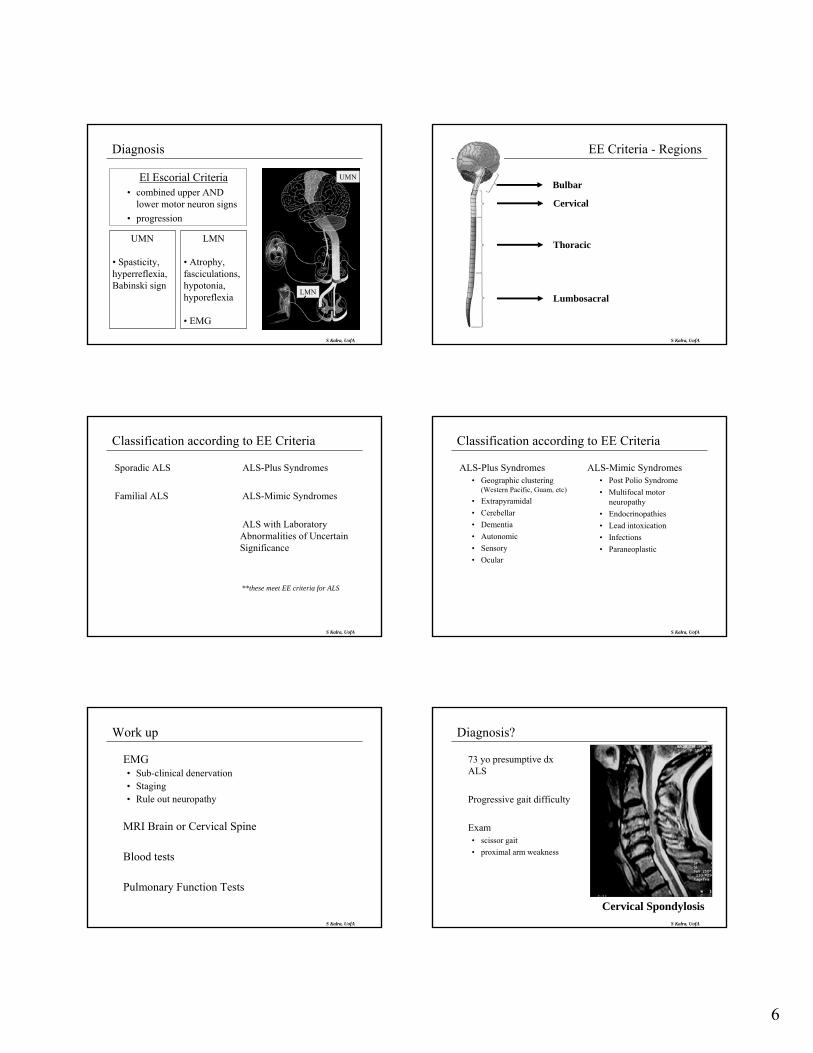
EE Criteria - Regions
Bulbar
Cervical
Thoracic
Lumbosacral
S Kalra, UofA
Classification according to EE Criteria
Sporadic ALS
Familial ALS
ALS-Plus Syndromes
ALS-Mimic Syndromes
ALS with Laboratory Abnormalities of Uncertain Significance
**these meet EE criteria for ALS
S Kalra, UofA
Classification according to EE Criteria
ALS-Plus Syndromes• Geographic clustering
(Western Pacific, Guam, etc)• Extrapyramidal• Cerebellar• Dementia• Autonomic• Sensory• Ocular
ALS-Mimic Syndromes• Post Polio Syndrome• Multifocal motor
neuropathy• Endocrinopathies• Lead intoxication• Infections• Paraneoplastic
S Kalra, UofA
Work up
EMG• Sub-clinical denervation• Staging• Rule out neuropathy
MRI Brain or Cervical Spine
Blood tests
Pulmonary Function Tests
S Kalra, UofA
Diagnosis?
73 yo presumptive dxALS
Progressive gait difficulty
Exam• scissor gait• proximal arm weakness
Cervical Spondylosis

7
Mitsumoto, 1998 S Kalra, UofA
Clinical Features
Limb Bulbar Respiratory Cognitive Indirect
S Kalra, UofA
Clinical Features
Limb• Weakness• Cramps• Fasciculations• Fatigue• Stiffness
Bulbar• Dyasarthria• Dysphagia• Drooling• Laryngospasm• Labile affect
S Kalra, UofA
Clinical Features - Respiratory
Dyspnea Orthopnea Sleep disordered breathing
• Frequent awakenings• Unrefreshing sleep• Fatigue• Poor concentration• Morning headache• Anxiety, depression• Anorexia, weight loss
S Kalra, UofA
Clinical Features - Cognitive Impairment
Frontotemporal Lobar Degeneration (FTLD)• Executive dysfunction• Behavioural changes
Prevalence: upwards of 50% Frank dementia rare
impacts decision making capacity reduced survival
S Kalra, UofA
Cognitive Impairment -Features and proposed criteria
ALS
ALS withoutFrontotemporal
Involvement
FrontotemporalInvolvement
Cognitive ImpairmentALSci
(attention, cognitive flexibility, word generation
spared visuospatial and memory)
Behavioural ImpairmentALSbi
(interpersonal skills, socialComportment
esp. apathy, irritability)
FrontotemporalDementia FTD
8
S Kalra, UofAAdapted from Belsh and Schiffman, 1996
UMN
LMN
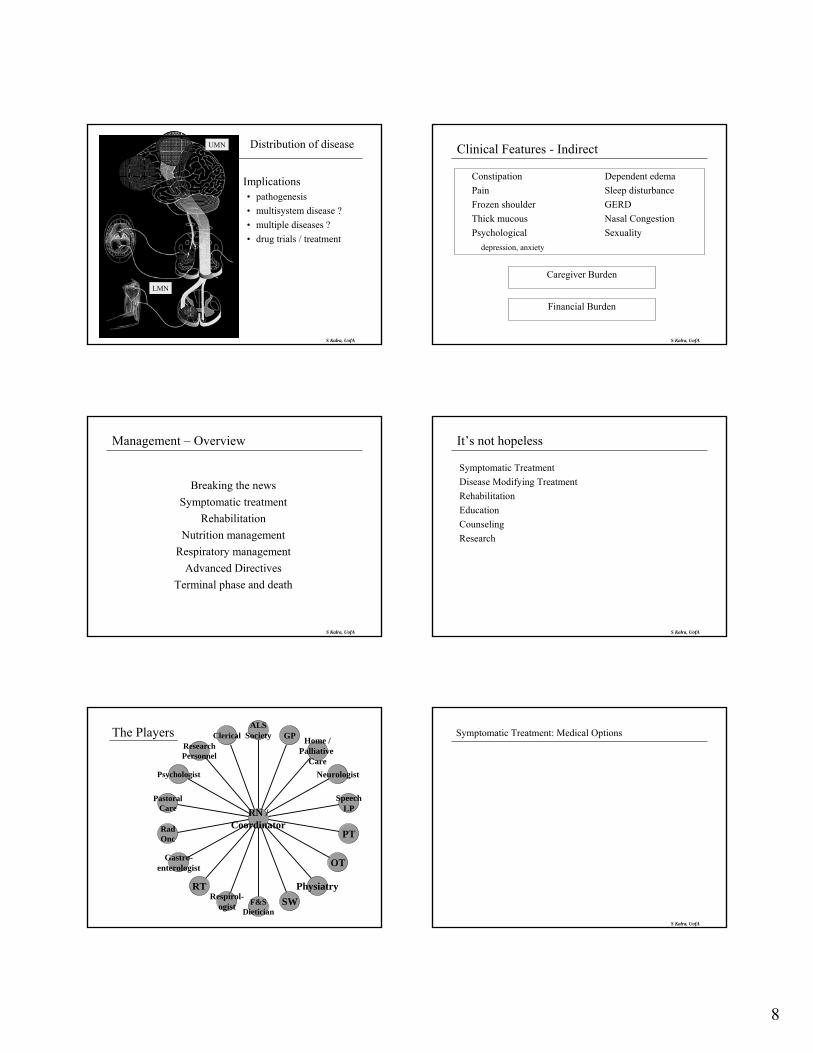
Distribution of disease
Implications• pathogenesis• multisystem disease ?• multiple diseases ?• drug trials / treatment
S Kalra, UofA
Clinical Features - Indirect
Constipation Dependent edemaPain Sleep disturbanceFrozen shoulder GERDThick mucous Nasal CongestionPsychological Sexuality
depression, anxiety
Caregiver Burden
Financial Burden
S Kalra, UofA
Management – Overview
Breaking the newsSymptomatic treatment
RehabilitationNutrition management
Respiratory managementAdvanced Directives
Terminal phase and death
S Kalra, UofA
It’s not hopeless
Symptomatic Treatment Disease Modifying Treatment Rehabilitation Education Counseling Research
The Players ClericalResearchPersonnel
Psychologist
PastoralCare
RadOnc
Gastro-enterologist
RTRespirol-
ogist F&SDietician
SWPhysiatry
OT
PT
SpeechLP
Neurologist
Home /Palliative
Care
GPALS
Society
RN /Coordinator
S Kalra, UofA
Symptomatic Treatment: Medical Options
Sialorrhea Anticholinergics: Amitriptyline, glycopyrrolate, transdermal scopolamine, others “thick mucus”: propranolol metoprolol mucomyst guaifenesin manually assisted coughing suction devices parotid irradiation
Spasticity Baclofen Dantrolene Diazepam IT Baclofen Cramps Baclofen Gabapentin Phenytoin Carbamazepine Diazepam Fasciculations Lorazepam Gabapentin Pain Rx spasticity, NSAIDS, gabapentin, TCAs, “stepped-care”
Pseudobulbar symptoms Amitriptyline Fluvoxamine Fear & Anxiety Clonazepam Lorazepam Amitriptyline SSRI Insomnia Amitriptyline Benzodiazepines Depression SSRI TCA
Respiratory NIPPV Morphine Benzodiazepines Nutritional Support PEG

9
S Kalra, UofA
Disease Modifying Treatment
Riluzole• Anti-glutamatergic• Prolongs survival 3-6 months
S Kalra, UofA
Netter
Dysarthria
S Kalra, UofA
Mobility
Clinical Research
S Kalra, UofA
Clinical research – what’s hot
Cognitive impairment
Neuroprotective drugs
Effect of interventions on quality of life• Nutritional, respiratory, assistive devices
Surrogate Markers / Biomarkers
S Kalra, UofA
Candidate drugs under human investigation
CoQ 10
Ceftriaxone, Memantine
Lithium
Combination Therapy• celecoxib / creatine• minocycline / creatine
10
S Kalra, UofA
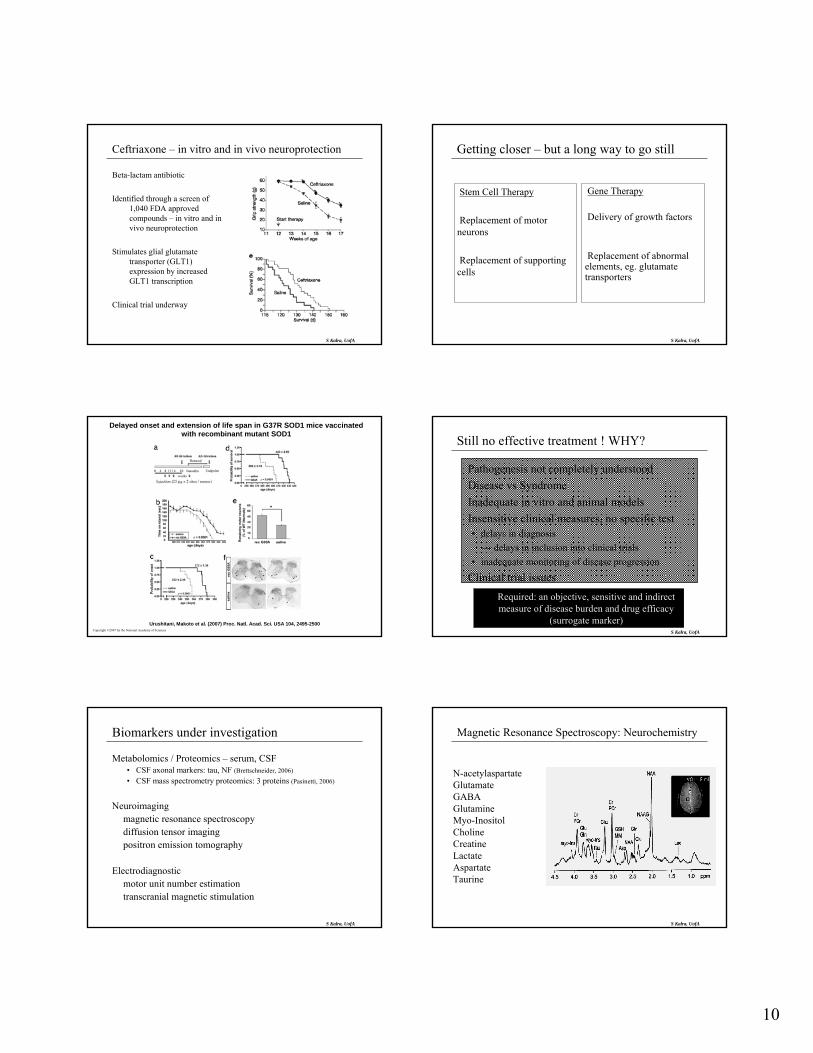
Ceftriaxone – in vitro and in vivo neuroprotection
Beta-lactam antibiotic
Identified through a screen of 1,040 FDA approved compounds – in vitro and in vivo neuroprotection
Stimulates glial glutamate transporter (GLT1) expression by increased GLT1 transcription
Clinical trial underway
S Kalra, UofA
Getting closer – but a long way to go still
Stem Cell Therapy
Replacement of motor neurons
Replacement of supporting cells
Gene Therapy
Delivery of growth factors
Replacement of abnormal elements, eg. glutamate transporters
Copyright ©2007 by the National Academy of Sciences
Urushitani, Makoto et al. (2007) Proc. Natl. Acad. Sci. USA 104, 2495-2500
Delayed onset and extension of life span in G37R SOD1 mice vaccinated with recombinant mutant SOD1
S Kalra, UofA
Still no effective treatment ! WHY?
Pathogenesis not completely understood Disease vs Syndrome Inadequate in vitro and animal models Insensitive clinical measures, no specific test
• delays in diagnosis→ delays in inclusion into clinical trials
• inadequate monitoring of disease progression
Clinical trial issuesRequired: an objective, sensitive and indirect measure of disease burden and drug efficacy
(surrogate marker)
S Kalra, UofA
Biomarkers under investigation
Metabolomics / Proteomics – serum, CSF• CSF axonal markers: tau, NF (Brettschneider, 2006)
• CSF mass spectrometry proteomics: 3 proteins (Pasinetti, 2006)
Neuroimagingmagnetic resonance spectroscopydiffusion tensor imagingpositron emission tomography
Electrodiagnosticmotor unit number estimationtranscranial magnetic stimulation
S Kalra, UofA
Magnetic Resonance Spectroscopy: Neurochemistry
N-acetylaspartate Glutamate GABA Glutamine Myo-Inositol Choline Creatine Lactate Aspartate Taurine
11
S Kalra, UofA
Magnetic Resonance Spectroscopy: Motor and extramotor involvement
Primary motor ↓↓↓Parietal / Occipital ↔Frontal ↓ or ↔Cingulate ↓Brainstem ↓
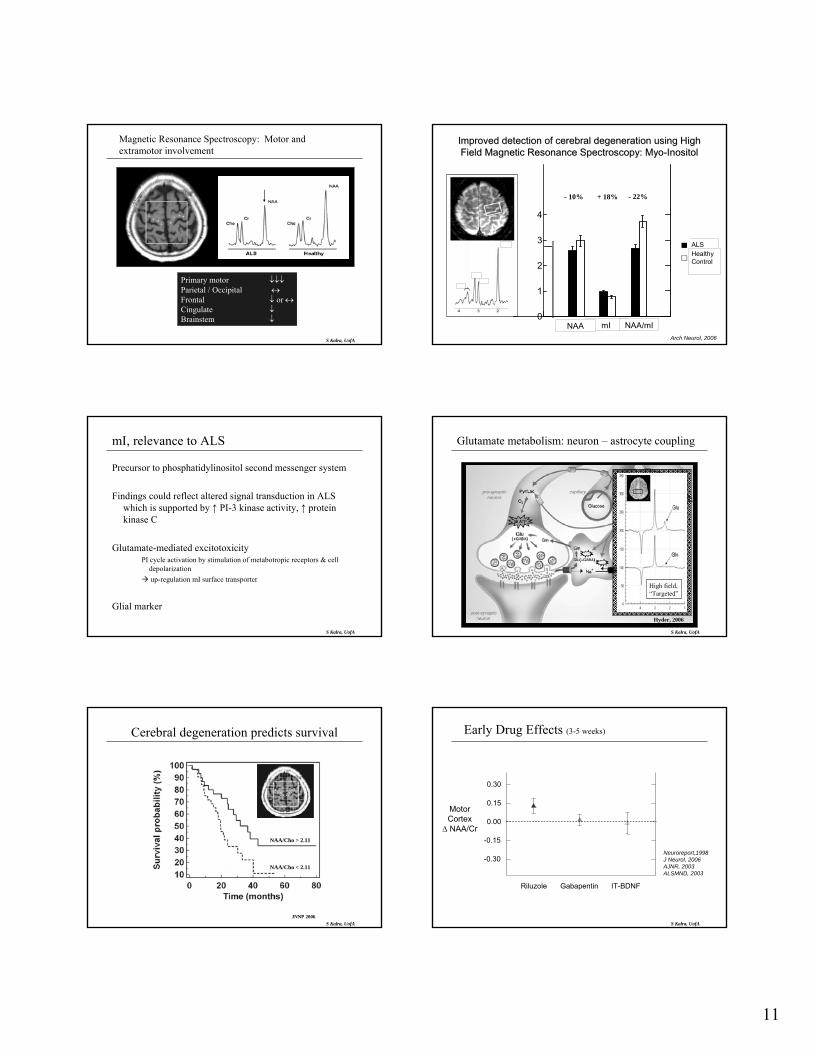
Improved detection of cerebral degeneration using High Improved detection of cerebral degeneration using High Field Magnetic Resonance Spectroscopy: Field Magnetic Resonance Spectroscopy: MyoMyo--InositolInositol
Arch Neurol, 2006
ALSHealthy Control
1 1 1mI NAA/mINAA0
1
2
3
4
- 22%+ 18%- 10%
S Kalra, UofA
mI, relevance to ALS
Precursor to phosphatidylinositol second messenger system
Findings could reflect altered signal transduction in ALS which is supported by ↑ PI-3 kinase activity, ↑ protein kinase C
Glutamate-mediated excitotoxicityPI cycle activation by stimulation of metabotropic receptors & cell
depolarizationup-regulation mI surface transporter
Glial marker
S Kalra, UofA
Glutamate metabolism: neuron – astrocyte coupling
Hyder, 2006
High field,“Targeted”
S Kalra, UofA
Cerebral degeneration predicts survival
JNNP 2006
NAA/Cho < 2.11
NAA/Cho > 2.11
S Kalra, UofA
-0.30
-0.15
0.00
0.15
0.30
MotorCortex
∆ NAA/Cr
Riluzole Gabapentin IT-BDNF
Early Drug Effects (3-5 weeks)
Neuroreport,1998J Neurol, 2006AJNR, 2003ALSMND, 2003
12
S Kalra, UofA
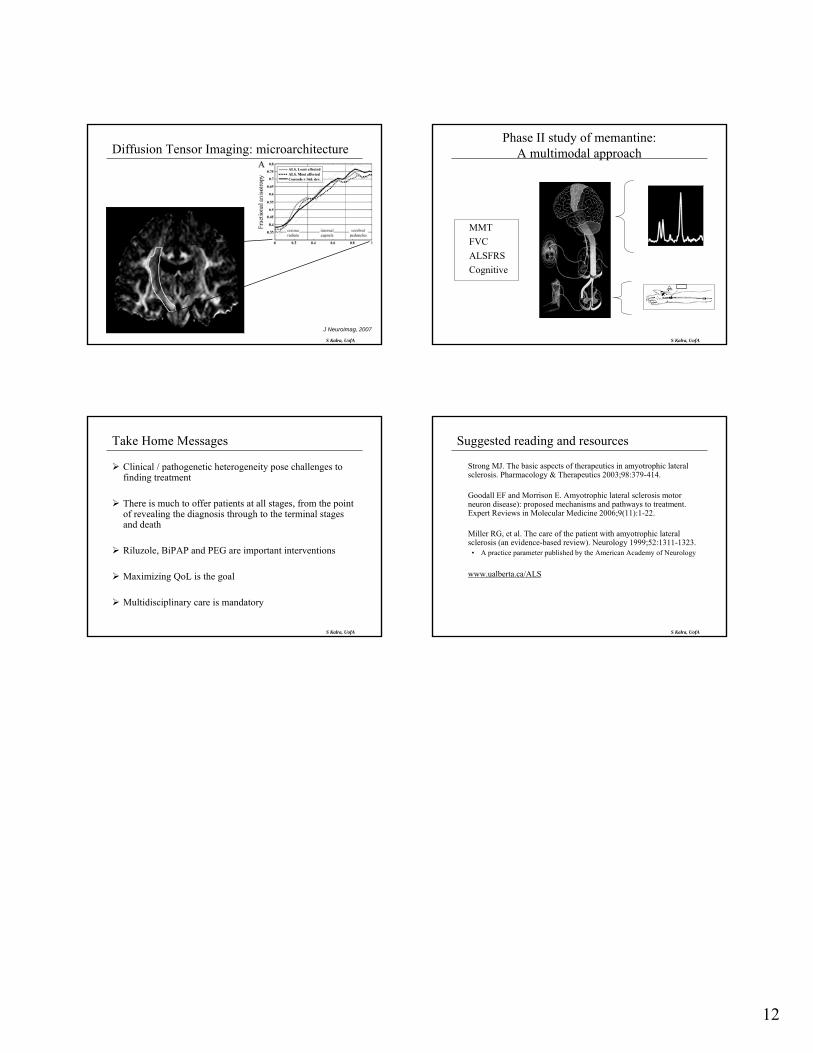
Diffusion Tensor Imaging: microarchitecture
J Neuroimag, 2007
S Kalra, UofA
Phase II study of memantine: A multimodal approach
MMT FVC ALSFRS Cognitive
S Kalra, UofA
Take Home Messages
Clinical / pathogenetic heterogeneity pose challenges to finding treatment
There is much to offer patients at all stages, from the point of revealing the diagnosis through to the terminal stages and death
Riluzole, BiPAP and PEG are important interventions
Maximizing QoL is the goal
Multidisciplinary care is mandatory
S Kalra, UofA
Suggested reading and resources
Strong MJ. The basic aspects of therapeutics in amyotrophic lateral sclerosis. Pharmacology & Therapeutics 2003;98:379-414.
Goodall EF and Morrison E. Amyotrophic lateral sclerosis motor neuron disease): proposed mechanisms and pathways to treatment. Expert Reviews in Molecular Medicine 2006;9(11):1-22.
Miller RG, et al. The care of the patient with amyotrophic lateral sclerosis (an evidence-based review). Neurology 1999;52:1311-1323.
• A practice parameter published by the American Academy of Neurology
www.ualberta.ca/ALS