Embed Size (px)
Citation preview

CASE REPORTJ Neurosurg Spine 28:467–471, 2018
In recent years, cervical disc arthroplasty (CDA) has emerged as a popular alternative to anterior cervical discectomy and fusion (ACDF) for the surgical treat-
ment of cervical degenerative disc disease. The essential advantage of CDA is the potential for reduction of the adjacent-segment degeneration encountered after ACDF.6,9 This reduction in adjacent-segment degeneration is thought to be related to the ability of CDA devices to mimic nor-mal spinal segmental motion, which may reduce the stress transfer to adjacent levels.8,12,14
CDA has been well studied, with efficacy reported to be equivalent to or better than that seen with ACDF, and it is associated with a consistently low incidence of adverse events.7,8,10,13 The development or progression of myelopa-thy after CDA is a particularly rare occurrence, with only a small number of cases described in the literature. Of these described cases, none was reported to be a result of progression of the spondylitic process affecting the central canal and resulting in cord compression. We present, to the best of our knowledge, the first case of progression of spondylosis at the level of a cervical artificial disc result-ing in cord compression and myelopathy.
Case ReportHistory and Presentation
This 55-year-old man with a medical history that in-
cluded prostate cancer, hyperlipidemia, and nephrolithia-sis presented for evaluation of back pain, which had been problematic for 20 years. He denied any neurological dif-ficulties. On examination, strength and sensation were in-tact. Reflexes were 2+ at the left biceps and patella, but 3+ on the right side, with a positive Hoffman’s sign on the right. The patient’s gait was normal. Because of the hyper-reflexia and pathologic reflex, a cervical spine MR image was obtained. At a follow-up visit 3 weeks later, the patient reported numbness and tingling across the fingertips of the second through fifth fingers bilaterally.
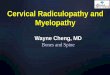
MRI of the cervical spine demonstrated a prominent central disc protrusion with an associated disc/spur com-plex at C5–6, resulting in marked central stenosis and significant bilateral foraminal stenosis (Fig. 1). There was associated increased T2 signal in the right lateral aspect of the spinal cord at this level. There was a slightly less prominent stenosis at C6–7 causing both central and bilat-eral foraminal stenosis.
Initial OperationAnterior cervical discectomies were performed at C5–6
and C6–7. At both levels, significant osteophytes and an overgrown ligament were found. The osteophytes were drilled down, the ligament was removed, and the dura was identified and decompressed at both levels. A C6–7 fusion was done using an interbody device (Medtronic Peek Pre-
ABBREVIATIONS ACDF = anterior cervical discectomy and fusion; AP = anteroposterior; CDA = cervical disc arthroplasty; HO = heterotopic ossification.SUBMITTED November 28, 2016. ACCEPTED August 24, 2017.INCLUDE WHEN CITING Published online February 2, 2018; DOI: 10.3171/2017.8.SPINE161385.
Myelopathy after cervical disc arthroplasty due to progression of spondylosis at the index level: case reportAnita Bhansali, MD,1,2 Michael Musacchio, MD,1,2 and Noam Stadlan, MD1,2
1Department of Neurosurgery, NorthShore University HealthSystem, Evanston; and 2University of Chicago, Pritzker School of Medicine, Chicago, Illinois
Cervical disc arthroplasty (CDA) has emerged as a popular alternative to anterior cervical discectomy and fusion (ACDF) for the surgical treatment of cervical degenerative disc disease. CDA has been well studied, with efficacy reported to be equivalent to or better than that seen with ACDF, and it is associated with a consistently low incidence of adverse events. The development or progression of myelopathy after CDA is a particularly rare occurrence. In this report, the authors describe the first known case of recurrence of myelopathy at the index level of surgery after CDA implantation due the continuation of the spondylitic process after placement of the artificial disc.https://thejns.org/doi/abs/10.3171/2017.8.SPINE161385KEY WORDS cervical disc arthroplasty; anterior cervical discectomy and fusion; cervical artificial disc; myelopathy; spinal cord compression
J Neurosurg Spine Volume 28 • May 2018 467©AANS 2018, except where prohibited by US copyright law
Unauthenticated | Downloaded 08/03/20 08:17 PM UTC

A. Bhansali et al.
J Neurosurg Spine Volume 28 • May 2018468
vail) filled with local bone. No biologics were placed, and bone morphogenetic protein was not used. At C5–6, a disc arthroplasty (Prestige, Medtronic) was performed. The Prestige disc features a semiconstrained design.
Postoperative CourseThe surgery was uneventful, and the immediate recov-
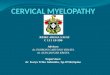
ery was unremarkable. Anteroposterior (AP) and lateral cervical spine radiographs obtained 1 month after sur-
gery demonstrated good placement of the instrumentation (Fig. 2).
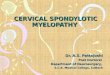
One year after surgery, the patient described some right-hand “soreness” with occasional tingling as well as occasional radiation of this tingling up to the anterior arm to shoulder and associated neck stiffness. Examina-tion findings remained unremarkable. Cervical spine ra-diographs at this time demonstrated bulky anterior osteo-phyte formation at C4–5, which was a significant increase in comparison with previous postoperative images. There was normal motion of the disc with no pathologic sublux-ation on flexion or extension (Fig. 3).
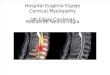
Six months later, the patient reported neck soreness, and right-arm numbness and pain radiating from his shoulder into his hand that had persisted for 2 months. He denied any weakness, gait instability, or bowel/bladder issues. The significant findings on physical examination included hyperreflexia in the upper and lower extremi-ties, more pronounced on the left, and bilateral Hoffman’s signs. Cervical spine radiographs once again showed nor-mal positioning of the hardware. An MR image was non-diagnostic at the level of the disc, and a CT scan did not show obvious stenosis (Fig. 4B).
Approximately 1 year later, after undergoing a total knee replacement, the patient had worsening gait insta-bility. MRI findings of the cervical spine were again un-remarkable but nondiagnostic at the level of the artificial disc due to extensive susceptibility artifact (Fig. 5). There
FIG. 1. Sagittal MR image of the cervical spine, STIR sequence, showing a large superimposed central disc protrusion at C5–6 with an associated disc/spur complex causing marked central stenosis with flattening of the spinal cord and moderate bilateral foraminal stenosis. A C6–7 superim-posed right paramedian protrusion with moderate central stenosis and bilateral foraminal stenosis is seen. There is a small focus of increased T2 signal within the right lateral aspect of the spinal cord at the C5–6 level. FIG. 3. Lateral cervical spine radiograph showing ACDF changes
extending from C-5 through C-7 with interbody spacers at each level. There is a bulky anterior ossified formation at C4–5, which progressed at C-4 when compared with the findings from 4 months earlier.
FIG. 2. Lateral (A) and AP (B) cervical spine radiographs showing placement of an anterior fusion device and disc grafts from the C5–7 levels, which appear satisfactorily aligned.
Unauthenticated | Downloaded 08/03/20 08:17 PM UTC

J Neurosurg Spine Volume 28 • May 2018 469
A. Bhansali et al.
has been recent work to identify MRI sequences that will have less artifact in the presence of metal.4 Because of the increasing concern for myelopathy, CT myelography was performed and revealed severe stenosis at the level of the artificial disc with decreased AP diameter of the spinal cord at C5–6 (Fig. 4A). The hardware remained in a good position, and flexion-extension cervical spine radiographs showed persistent motion of the artificial disc.
Given the progression of myelopathic symptoms and the stenosis, the artificial disc was removed and converted to a fusion. The surgery was uneventful. Surgical findings were consistent with the myelography findings: signifi-cant osteophytes and a hypertrophied ligament with some
scarring of the soft tissue to the dura. Postoperatively, the patient was unchanged neurologically, and radiographs revealed that the hardware was in a satisfactory position (Fig. 6). At follow-up 10 months after the revision surgery, the patient had only minimal improvement, but the grad-ual deterioration that was seen prior to revision surgery was halted.
DiscussionMyelopathy after CDA due to cord compression at
the index level has been described, but rarely. In a case report and literature review of cervical myelopathy after CDA, Chen et al. reported one case of myelopathy due to residual compression and another occurring as a result of the development of postoperative kyphosis.3 Hacker et al. described the development of myelopathy in one patient due to posterior subsidence of the CDA device, and neck pain with radiculopathy in another due to segmental col-lapse and retropulsion of bone.5 In a series of 74 patients undergoing CDA reported by Pickett et al., one patient was reported to have progressive myelopathy postopera-tively, which was attributed to an inadequate posterior osteophyte resection and subsequent development of ky-phosis.11 One case of progressive myelopathy after CDA with absence of radiographic compression was reported in the 2-year Frenchay CDA trial.16 In all of these cases, the myelopathy was caused by inadequate initial surgery, device failure/migration, or alignment changes.
There is limited discussion in the literature regarding CDA in the setting of central stenosis and/or cord signal. In a recent article, Chang et al. demonstrated that CDA was safe and effective in cases of T2-weighted cord chang-es.1 Another group demonstrated that multilevel CDA was safe and effective in cases of stenosis due to a congeni-tally small canal, at least over the short term. However, the long-term outcomes and results needed to be monitored.2
There have also been reports on progression of facet disease at the level where the disc has been replaced. Wenger and Markwalder reported on 3 patients who de-
FIG. 5. MR image of the cervical spine showing extensive susceptibility artifact at the level of the artificial disc.
FIG. 4. A: CT myelogram of the cervical spine obtained 3 years after surgery, showing adequate hardware placement. A broad-based disc osteophyte complex is seen at C5–6 (left), and subtle ventral soft tissue possibly represents disc protrusion with a considerable decreased AP diameter of the thecal sac (right). Myelographic views also show decreased concentration of contrast material in the thecal sac at C5–6. B: CT scan of the cervical spine obtained 1.5 years after surgery, illustrating the growth of the endplate osteophytes resulting in worsening canal narrowing and cord compression. The effect of the ligament cannot be seen on the plain CT scan, but can be seen by the indentation into the CSF space on the myelogram (panel A, left). The C4–5 anterior osteophytes are seen on both CT scans.
Unauthenticated | Downloaded 08/03/20 08:17 PM UTC

A. Bhansali et al.
J Neurosurg Spine Volume 28 • May 2018470
veloped radiculopathy more than a year after CDA with the Bryan disc.15 Myelography/CT was performed in all cases to confirm the recurrent root compression. In the case described here, the cord compression was the result of progression of the spondylotic process in the disc at the level of the CDA itself. It is not clear what factors contrib-uted to this occurrence, whether individual, technical, or device related. The initial compression was due to spondy-losis and not a gross herniated disc, but CDA devices are indicated and frequently placed in cases of compression from spondylitic changes. As can be seen on the CT scan, our patient developed a large anterior osteophyte at the level above the CDA, perhaps indicating a predilection for excessive bone growth. He also required lumbar fusion for spondylolisthesis 1 year after his initial surgery. Perhaps a significant contribution was the patient’s spondylitic in-clination.
The device was positioned well and remained mobile. Although difficult to assess due to the artifact, there does not appear to be a significant amount of heterotopic os-sification (HO). Perhaps more HO in this case would have been beneficial in limiting the amount of movement, re-sulting in a diminution of the spondylitic process. The de-vice also covers an adequate amount of the disc endplate. Inadequate coverage has been cited as a possible contrib-uting factor to HO.
There does not appear to have been a device failure, and as noted it continued to function well as a motion
preservation device. We have not been able to identify any characteristics of this particular disc that would have con-tributed to the outcome.
The incidence of adverse events after CDA has been reported to be universally low, and the development of new myelopathic symptoms after CDA is very rare in the literature. We describe here the first reported case of new-onset myelopathy at the index level of surgery after CDA device implantation due to the development of posterior osteophytes. The importance of this report is not just the documentation of a potential late outcome to be tracked. The usual diagnostic test for patients with myelopathy is MRI. However, current CDA devices produce significant artifact, making the MR images nondiagnostic at the level of the CDA. It might be a common assumption that steno-sis does not recur at the CDA level. With that assumption, an MR image showing no stenosis at the other levels of the cervical spine but inadequately visualizing the index level might be assumed to be adequate to rule out a compres-sive myelopathy. This could result in a failure to diagnose a compressive myelopathy or a delay in diagnosis, possibly resulting in preventable neurological deterioration. Recur-rent cord compression due to progression of spondylosis should be kept in mind as a possible etiology of recurrent myelopathy in patients with a CDA device.
AcknowledgmentsWe thank Vimal Patel, PhD, Medical and Scientific Writer at
NorthShore Neurological Institute, for copyediting this manuscript for submission.
References 1. Chang HK, Huang WC, Wu JC, Chang PY, Tu TH, Fay LY,
et al: Should cervical disc arthroplasty be done on patients with increased intramedullary signal intensity on magnetic resonance imaging? World Neurosurg 89:489–496, 2016
2. Chang PY, Chang HK, Wu JC, Huang WC, Fay LY, Tu TH, et al: Is cervical disc arthroplasty good for congenital cervical stenosis? J Neurosurg Spine 26:577–585, 2017
3. Chen J, Wang X, Yuan W, Tang Y, Zhang Y, Wan M: Cervi-cal myelopathy after cervical total disc arthroplasty: case re-port and literature review. Spine (Phila Pa 1976) 37:E624–E628, 2012
4. Elliott CA, Fox R, Ashforth R, Gourishankar S, Nataraj A: Magnetic resonance imaging artifact following anterior cer-vical discectomy and fusion with a trabecular metal cage. J Neurosurg Spine 24:496–501, 2016
5. Hacker FM, Babcock RM, Hacker RJ: Very late complica-tions of cervical arthroplasty: results of 2 controlled random-ized prospective studies from a single investigator site. Spine (Phila Pa 1976) 38:2223–2226, 2013
6. Hilibrand AS, Robbins M: Adjacent segment degeneration and adjacent segment disease: the consequences of spinal fusion? Spine J 4 (6 Suppl):190S–194S, 2004
7. Hisey MS, Zigler JE, Jackson R, Nunley PD, Bae HW, Kim KD, et al: Prospective, randomized comparison of one-level Mobi-C cervical total disc replacement vs. anterior cervi-cal discectomy and fusion: results at 5-year follow-up. Int J Spine Surg 10:10, 2016
8. Janssen ME, Zigler JE, Spivak JM, Delamarter RB, Darden BV II, Kopjar B: ProDisc-C total disc replacement versus anterior cervical discectomy and fusion for single-level symptomatic cervical disc disease: seven-year follow-up of the prospective randomized U.S. Food and Drug Administra-
FIG. 6. Cervical spine radiograph showing stable and unremarkable results with unchanged vertebral contours after placement of anterior fixation hardware spanning C5-C6-C7.
Unauthenticated | Downloaded 08/03/20 08:17 PM UTC

J Neurosurg Spine Volume 28 • May 2018 471
A. Bhansali et al.
tion investigational device exemption study. J Bone Joint Surg Am 97:1738–1747, 2015
9. Lawrence BD, Hilibrand AS, Brodt ED, Dettori JR, Brodke DS: Predicting the risk of adjacent segment pathology in the cervical spine: a systematic review. Spine (Phila Pa 1976) 37 (22 Suppl):S52–S64, 2012
10. Mummaneni PV, Burkus JK, Haid RW, Traynelis VC, Zde-blick TA: Clinical and radiographic analysis of cervical disc arthroplasty compared with allograft fusion: a randomized controlled clinical trial. J Neurosurg Spine 6:198–209, 2007
11. Pickett GE, Sekhon LH, Sears WR, Duggal N: Complica-tions with cervical arthroplasty. J Neurosurg Spine 4:98–105, 2006
12. Puttlitz CM, Rousseau MA, Xu Z, Hu S, Tay BK, Lotz JC: Intervertebral disc replacement maintains cervical spine ki-netics. Spine (Phila Pa 1976) 29:2809–2814, 2004
13. Sasso RC, Smucker JD, Hacker RJ, Heller JG: Artificial disc versus fusion: a prospective, randomized study with 2-year follow-up on 99 patients. Spine (Phila Pa 1976) 32:2933–2942, 2007
14. Vital JM, Boissière L: Total disc replacement. Orthop Trau-matol Surg Res 100 (1 Suppl):S1–S14, 2014
15. Wenger M, Markwalder TM: Posterior decompression sal-vages Bryan total disc arthroplasty in post-operatively recur-
rent uncoforaminal stenosis. J Clin Neurosci 21:741–744, 2014
16. Wigfield CC, Gill SS, Nelson RJ, Metcalf NH, Robertson JT: The new Frenchay artificial cervical joint: results from a two-year pilot study. Spine (Phila Pa 1976) 27:2446–2452, 2002
DisclosuresDr. Musacchio: consultant for Paradigm Spine and Medtronic.
Author ContributionsConception and design: Stadlan. Acquisition of data: Stadlan, Bhansali. Analysis and interpretation of data: all authors. Draft-ing the article: all authors. Critically revising the article: Stadlan. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Stad-lan. Study supervision: Stadlan.
CorrespondenceNoam Stadlan: NorthShore University HealthSystem, Evanston, IL. [email protected].
Unauthenticated | Downloaded 08/03/20 08:17 PM UTC