-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
1/14
Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies The basic functional unit of the
kidney is the nephron, which consists of the
glomerulus and the tubular system. Glomeruli are the basic units
of the
nephrons; there are about 1 million glomeruli in each kidney
(constituting
about 5% of the kidney weight).The glomerulus is a
net of
anastomosis of afferent
capillaries which are held
together by the mesangium
(composed of mesangial
cells and matrix) which
keeps the capillaries patent.
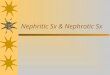
The figure on the right demonstrates the structure
of
the glomerulus; it is
composed of capillaries
lined by endothelial cells.
Podocytes (the epithelial
cells that make up the
visceral layer of Bowman’s
capsule) extend foot
processes that cover the
capillaries.
Fusion of the basement
membranes of the epithelial
cells (podocytes) and endothelial cells make up the glomerular
basement
membrane (GBM), the charge and size dependent filtration barrier
(it
prevents large and negatively charged molecules such as
albumin from being filtrated).
• Important terminology in kidney disease:-
Diffuse: all the glomeruli in the kidney are involved.
- Focal: patchy involvement of glomeruli.
- Global: the whole glomerulus is affected by the
pathologic process.
- Segmental: part of the mesangium is involved in the
pathologic
process.
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
2/14
• Mechanisms of kidney inflammation: there is involvement of
antibodies,
immune complexes and T cells.-
Humoral mediated: through antibodies that bind structures in
the
kidneys (as anti-GBM disease), or antibodies that bind
structures
outside the kidneys, resulting in the formation of immune
complexes
that later deposit in the kidneys (as lupus nephritis
with anti-DNA
antibodies). Normally, when immune complexes form,
the cells ofthe reticuloendothelial system get rid of them and
they are cleared. In
susceptible patients, the immune complexes will not be cleared
and
will accumulate and deposit in the kidneys causing
complement
activation and inflammation.
- Cell mediated: T cell activation and the release of
cytokines and
chemokines results in inflammation (in the kidneys and other
organs
as well).
• Classification of glomerulonephritis (GN):
-
Clinical classification: according to the history and
physical
examination (which are the key to the diagnosis) GNs are
classified into either acute or chronic, primary (starting in
the
kidney) or secondary (kidney involvement is secondary to a
systemic disease as SLE, multiple myeloma or infection),
andnephrotic and/or nephritic.
-
Pathologic classification: according to the histopathology on
kidney
biopsies GNs are classified into proliferative and
non-proliferative.
The clinical picture, diagnosis, treatment and outcome
differ between
them.
o Proliferative: proliferation of mesangial cells, endothelial
cells
or epithelial cells. The proliferation can be global, crescentic
or segmental.
o Non-proliferative such as minimal change nephropathy,
focal
segmental glomerulosclerosis (FSGS) and
membranous glomerulonephritis (MGN).
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
3/14
Nephrotic Syndrome It is a syndrome characterized by the
following features:
- Proteinuria > 3.5 g/day (3+ or 4+); due disturbance
in the GBM.-
Hypoalbuminemia.
- Dyslipidemia; due to the hypoproteinemia and reduction
in oncotic
pressure which stimulate the liver to synthesize LDL and
releasemore cholesterol.
± Edema; especially of the face (puffy face).
• Nephrotic syndrome has important complications; such
as
atheroslcerosis due to the dyslipidemia, and increased risk of
thrombosis
(such as renal vein thrombosis) due to urinary loss of
anti-thrombin III;
the more the proteinuria, the more is the risk of
thrombosis.
Also, patients are at an increased risk of infections
due to urinary loss of
immunoglobulins, apart from the fact that the treatment is that
of immunosuppression.
• Work up in nephrotic syndrome:
-
Urinalysis (dipstick): chemical reaction with the urine; it
gives
information about RBCs, WBCs, sugars, ketones, and proteins. It
is
sensitive to only albumin.
-
Urine sediment examination under the
microscope (oval fat bodies in nephrotic
syndrome, as seen in the adjacent figure).- Measurement of
urine protein, by 24 hour
urine collection (normally it is
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
4/14
- Serology; according to the clinical picture (we can look
for ANA,
anti-DNA antibodies if lupus is suspected, C3 and C4 levels,
HBV,
HCV, HIV antigens…etc).
- Renal ultrasound: it gives information about the size of
the kidney (if
small; biopsy is contraindicated, the patient may be in end
stage renal
disease (ESRD)).
-
Doppler ultrasound; which can detect renal vein thrombosis
(whichitself can cause proteinuria, hematuria, and acute
kidney injury).
- Renal biopsy for definitive diagnosis; most adult
patients with GN
undergo a renal biopsy.
• Diseases that cause nephrotic syndrome:1.
Minimal change disease (MCD): the most common cause in
children, and is responsible for 5-10% of cases in adults. There
is a
defect in the charge or pore size of the GBM, and there will
be effacement of the foot processes of the podocytes which is
seen on the
electron microscope. This disease is of sudden onset, and
results in fluid and salt retention, edema and weight gain.
Symptoms are related to fluid overload, and 30% develop
hypertension and microscopic hematuria (with no RBC casts, or
dysmorphic RBCs). 20% of adult
patients (> 40 years of age) present with renal
dysfunction due to either
intravascular volume depletion and 3rd spacing of fluid, or
direct protein
toxicity on the tubules (acute tubular necrosis). Patients
with MCD have selective proteinuria (only to albumin), with
normal complement levels and serological tests.
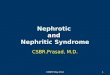
Diagnosis (in adults) is by renal
biopsy; where electron microscopy
shows effacement of the podocyte foot
processes, as seen in the figure on the
right. Light microscopy and
immunofluorscence are normal; hencethe name.
Treatment is with steroids (2mg/kg for 46 weeks, followed by
1mg/kg
for 46 weeks in adults).
Relapses could be infrequent, frequent (2 or more within 6
months), or
steroid dependent (while the patient is on steroids or within 2
weeks of
therapy). After treatment, 30% remit with no relapses, 30% will
have
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
5/14
infrequent relapses (in such patients, the course of steroids
has to be
repeated), and a further 30% will have frequent relapses and
need to be
treated with steroids and second line therapy
(cyclophospohamide,
mycophenolate mofetil (MMF), or calcineurin inhibitor (CNI));
the choice
of a second line drug depends on the patient; for
example,
cyclophosphoamide is not favorable in young female patients due
to side
effects on reproduction. Second line drugs have also to be used
in steroid dependent relapses.
Minimal change disease could also be secondary (not idiopathic);
to
drugs (NSAIDs for example), or to malignancies (as
Hodgkin’s
lymphoma, and leukemias).MCD does not progress to chronic kidney
disease.
2.
Focal segmental glomerulosclerosis (FSGS): this is a
histological
description with involvement of parts of some glomeruli in the
kidneys,
and thus its diagnosis requires a kidney biopsy.
20-25 % of cases are idiopathic (more common in
African Americans).
Other forms are familial (autosomal dominant or recessive);
and these
are usually resistant to treatment.
The cause is believed to be the presence of a permeability
factor in the
serum of patients, which increases the GBM permeability to
protein;
that’s why plasma exchange is a modality of treatment. It is
important to
know if the patient has primary (idiopathic) or secondary
FSGS,
especially if the patient is going to have a renal
transplantation (to know
the recurrence rate of the disease in the transplanted
kidney).
Proteinuria (nonselective) can be asymptomatic or it can reach
the
nephrotic range, with edema and swelling. 30-50% of patients
will have
hypertension, 20-30% will have a reduced glomerular filtration
rate
(GFR) at presentation and 50% will have microscopic
hematuria.
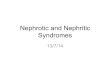
Diagnosis is by kidney biopsy, which
shows sclerosis on light microscopy as seen in the figure
on the right, electron
microscopy shows foot process
effacement as that seen in MCD.
Treatment is with steroids for at least 6
months, and if patients don’t respond
well, second line drugs can be used such
as ciclosporin and CNI. Left untreated, patients with FSGS will
progress
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
6/14
to ESRD in about 5-20 years (the range depends on the type of
FSGS,
and other therapies such as ACE inhibitors).
Secondary causes of FSGS could be:
a.
Viral infections such as HIV (especially in African
Americans),
Hepatitis B virus and Parvovirus B19.
b.
Drugs such as INF-α, lithium and bisphosphonates
(pamidronate).
c.
Hypertensive nephropathy.d.
Reduced renal mass and hyperfiltration (as in patients with
a
single kidney).
e.
Reflux nephropathy.
f.
Obesity.
g. Sick cell disease.
3. Membranous glomerulonephritis (MGN): it is the
commonest
cause of nephrotic syndrome in white people. Most cases in the
west are
idiopathic, whereas in our part of the world, they are mostly
secondary.
Manifestations are those of the nephrotic syndrome; patients can
also
have hypertension and microscopic hematuria. Renal function is
normal
at the time of diagnosis (normal GFR).
MGN is the worst disease, among the causes of nephrotic
syndrome, in
terms of thrombosis, and the risk is increased if serum albumin
is
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
7/14
screening should be done, since malignancy is one secondary
cause of
MGN.
Treatment depends on the level of proteinuria:
-
If mild (
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
8/14
Nephritic Syndrome It is a syndrome characterized by the
following features:
- Hematuira (with RBC casts or dysmorphic
RBCs).-
Hypertension.
- Edema.
-
Mild to moderate proteinuria (< 3g/day; not in the nephrotic
range).- Increased serum creatinine.
± Oliguria (often)
There might also be generalized nonspecific symptoms such
headache and
fatigue.
The mechanism is inflammation of the glomeruli, which causes
hematuria,
reduction in the GFR, oliguria, as well as salt and water
retention which
causes hypertension and edema (as opposed to nephrotic syndrome
where
they are caused by hypoalbuminemia).Most of the diseases that
cause nephritic syndrome are proliferative,
whether they are primary or secondary.
• Diseases that cause nephritic syndrome:1. Post-infectious
glomerulonephritis: this is due to formation
ofimmune complexes that deposit in the kidneys, and activate
thecomplement system resulting in proliferation and
inflammation. Most of
the cases are due to Group A β hemolytic streptococci
strains 12 and 49.With strain 12, the GN occurs 1-3 weeks after the
pharyngitis, while withstrain 49, the GN occurs 2-6 weeks after the
impetigo. It is very important to know the time frame between
the initial infection and the onset of the nephritic syndrome
to differentiate it from IgA nephropathy in which
the nephropathy occurs concurrently with, or immediately after
the infection. Other microorganisms can cause post-infectious
glomerulonephritis, including other bacteria, viruses and
fungi.
The classic presentation is an acute nephritic picture with
hematuria, pyuria, RBC casts, edema, hypertension, and
oliguric renal failure, which
may be severe enough to appear as rapidly progressive
glomerulonephritis
(RPGN).
Diagnosis:
-
History: infection in the recent previous months (pharyngitis
or
impetigo).
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
9/14
- Blood tests: the titer of Anti-
Streptolysin O (ASO) antibodies, which
are usually raised. Its absence however
doesn’t exclude the disease, but its
presence strongly suggests it. It may
remain positive in the serum for several
months.- Urinalysis; which shows protein.
Microscopic examination of the urine
may show dysmorphic RBCs, RBC
casts (as shown on the right), or WBC
casts (active urine sediment).
- High serum creatinine.
- Hypocomplementemia (returning to the
normal values within 6 to 8 weeks).
-
Renal biopsy confirms the diagnosis;
but it is invasive and not done to all
patients (especially if the other methods
are suggestive); biopsy shows mesangial
hypercellularity,
endocapillary hypercellularity and leukocytes.
Treatment is nonspecific and supportive. More than 90% of
patients fully
recover (especially children), hematuria might be prolonged (for
1 to 2months) but renal failure is rare.
2.
Rapidly progressive glomerulonephritis (RPGN): it is a syndrome,
not
a single disease characterized by a rapid increase in serum
creatinine and
deterioration of kidney function. It is uncommon, and comprises
10-15% of
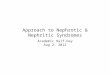
all the glomerulonephritidies. It is due to damage of the
glomeruli and the
formation of crescents; which
occur due to triggering of the
proliferation of the podocytes that form layers of
cells in Bowman’s
capsule, along with macrophages
and monocytes. This can affect
some or all of the glomeruli. The
figure on the right shows two
cresentic glomeruli.
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
10/14
RPGN is classified according to immunological findings in the
kidneys
into:
1.
Anti-GBM disease (5–6 mg/dL, if oliguria
is present, or if there is a need for acute dialysis.
In Goodpasture’s syndrome,
the lung hemorrhage should also be treated. Patients are
treated with high
dose steroids, cyclophosphoamide and plasma exchange.
Isolated renal
involvement needs less aggressive treatment.• ANCA small vessel
vasculitidies:
1.
Granulomatosis with polyangiitis (GPA): formerly known as
Wegener’s granulomatosis. Patients present with respiratory
(usually upper, but also
lower) and renal symptoms. Usually in the 5th and 6th decades.
Patients classically present with fever, purulent rhinorrhea,
nasal ulcers, sinus pain, polyarthralgias or arthritis,
cough, hemoptysis, shortness of breath, microscopic hematuria,
and non-nephrotic range proteinuria; occasionally
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
11/14
there may be cutaneous purpura and
mononeuritis multiplex. Proptosis may occur
due to retro-orbital inflammation as seen in the
figure on the right, leading to diplopia. Chest x-
ray often reveals nodules and persistent
infiltrates, sometimes with cavities, as seen in
the figure. This disease can spare the kidneys; where it is
called limited GPA. When there is
renal involvement, the prognosis is bad, with
80% progression to GN. This disease is PR3-
ANCA (formerly known as c-ANCA) positive.
Treatment is by steroids and
immunosuppresion.
2.
Microscopic polyangiitis: clinically, these
patients look somewhat similar to those with
GPA, except they rarely have significant lung
disease or destructive sinusitis. The distinction is made on
biopsy, where
the vasculitis in microscopic polyangiitis is without
granulomas. Patients
are usually MPO-ANCA (formerly known as p-ANCA) positive.
3.
Eosinophilic granulomatosis with polyangiitis (EGPA): formerly
known
as Churg-Strauss syndrome. Patients usually have peripheral
eosinophilia,
cutaneous purpura, asymmetrical mononeuritis, asthma, and
allergic rhinitis. Lung inflammation, including fleeting cough
and pulmonary
infiltrates, often precedes the systemic manifestations of
disease by years.
The lung is rarely spared in this disease.
• Immune complex disease:
1. IgA nephropathy: it is an immune complex disease, in
which IgA
antibodies deposit in the mesangium of glomeruli. It is the most
common
cause of GN; especially in Asia. It is usually diagnosed
incidentally,
because it causes microscopic hematuria. It is slightly
commoner in malesand has a peak incidence in the second and third
decades of life, and rare
familial clustering. IgA deposition in the mesangium is either
idiopathic, or
associated with other diseases including chronic liver disease,
Crohn's
disease, gastrointestinal adenocarcinoma, celiac disease,
dermatitis
herpetiformis, chronic bronchiectasis, idiopathic interstitial
pneumonia,
mycosis fungoides, ankylosing spondylitis, and Sjögren's
syndrome.
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
12/14
It is usually asymptomatic, but there are episodic attacks of
macroscopic
hematuria during or immediately after an upper respiratory tract
infection,
often accompanied by proteinuria or persistent asymptomatic
microscopic
hematuria. Acute renal failure and a rapidly progressive
clinical picture is
rare. Prognosis for the kidneys is good, unless there is renal
impairment at
presentation, hypertension, or proteinuria > 1g/day.
Treatment is
supportive and nonspecific, ACE inhibitors or ARBs can be used
when there is proteinuria. Fish oil might help as well. When
presenting as
RPGN, patients typically receive steroids, and cytotoxic agents
(but not
plasmapheresis). Henoch-Schönlein purpura is a similar
disease with
systemic features; it is associated with purpra over the
buttocks and lower
legs, abdominal pain or bleeding, and arthritis; usually
following an upper
respiratory tract infection. Weeks later, it can be followed by
nephritis.
Tissue biopsy shows IgA deposition in blood vessels.
2.
Lupus nephritis: lupus nephritis is a common and serious
complication ofsystemic lupus erythematosus (SLE) and most severe
in African-American
female adolescents. 60% of patients with SLE will have lupus
nephritis.
Patients might present with lupus nephritis alone, or with other
manifestations
of SLE. The most common clinical sign of renal disease is
proteinuria, but
hematuria, hypertension, varying degrees of renal failure, and
active urine
sediment with RBC casts can all be present. Proteinuria can be
in the
nephrotic or non-nephrotic range. SLE can also have
non-glomerular renal
manifestations such as tubulointerstitial nephritis and
vasculitis.
Lupus nephritis has 6 classes; they differ in their
presentation, treatment
and prognosis. Patients can have more than one class (for
example; class
III and V, together). Most of the classes present as nephritic
syndrome.
Class V can present as nephrotic syndrome. Class V usually
occurs with
another class. Treatment depends on the class; but is usually
with
steroids, cytotoxic drugs (MMF or cyclophosphoamide), and
rituximab.
3. Membranoproliferative glomerulonephritis (MPGN): this
disease
usually presents in young age. It has two types; 1 and 2.
- Type 1: patients have a history of recent upper
respiratory tract
infection. It usually manifests as nephrotic syndrome.
- Type 2 (dense deposit disease): less common. It usually
presents as
nephritic syndrome. It is associated with
hypocomplementemia,
and it is C3 (nephritic factor) positive. Treatment is by
cortisone,
and antiplatelet drugs such as aspirin. 50% will have ESRD
in 10
years.
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
13/14
Other diseases that can cause GN: 1. Hereditary
nephritis: Alport syndrome (nephritis, with deafness, and
eye
disorders).2.
Subacute bacterial endocarditis: patients present
with gross or
microscopic hematuria, pyuria, and mild proteinuria or, less
commonly,
RPGN with rapid loss of renal function.
3.
Cryoglobulonemic vasculitis: cryglobulins are antibodies which
from
against immunoglobulins forming immune complexes that deposit in
the
cold. They are classified into 3 types according to the
immunoglobulin
involved. Type III is associated with polyclonal antibodies
directed at IgG,
and it is the one that is usually associated with GN. It is
caused by HBV,
HCV, or rheumatoid arthritis (RA). In type III cryglobulonemia,
there will
be necrotizing skin lesions, arthralgia, fever, and
hepatosplenomegaly. The
GN can lead to RPGN.
4.
HIV nephropathy: it usually occurs in young black men,
especially IV
drugs abusers. It usually presents as nephrotic syndrome with
normal
complement levels.
5. Hepatitis C virus infection: this can cause either
nephritic or nephrotic
syndrome. It can cause three patterns of GN: MPGN (type I), MGN,
or
cryoglobulonemia associated GN. Treatment is with
INF-α.
6.
Amyloidosis: renal amyloidosis is of two types: primary (AL)
which is
idiopathic, or associated with multiple myeloma, and secondary
(AA)which is associated with RA, inflammatory bowel disease (IBD),
familial
mediterranean fever (FMF) and tuberculosis. Treatment includes
alkylating
agents, melphalan, and corticosteroids. Renal transplantation
could be
indicated in secondary amyloidosis.
This table lists the causes of GN that cause
hypocomplementemia:
-
8/18/2019 Nephrotic and Nephritic Syndromes and the
Glomerulonephritidies
14/14
This table summarizes the important GNs:
Done by: Mohammed Bashabsheh & Osama Thiabat