Embed Size (px)
Citation preview
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/11648991
Ovarian Non-Hodgkin’s Lymphoma: A Clinicopathologic Study of Eight
Primary Cases
Article in Modern Pathology · December 2001
DOI: 10.1038/modpathol.3880442 · Source: PubMed
CITATIONS
85
READS
66
5 authors, including:
Some of the authors of this publication are also working on these related projects:
Do Skin Tears with Arthroscopic Knot Tying Represent a Contamination Risk? View project
Roger Warnke
Stanford University
309 PUBLICATIONS 34,222 CITATIONS
SEE PROFILE
Michael T Deavers
Houston Methodist Hospital
288 PUBLICATIONS 11,348 CITATIONS
SEE PROFILE
All content following this page was uploaded by Michael T Deavers on 09 February 2015.
The user has requested enhancement of the downloaded file.

Ovarian Non-Hodgkin’s Lymphoma: A ClinicopathologicStudy of Eight Primary CasesRussell Vang, M.D., L. Jeffrey Medeiros, M.D., Roger A. Warnke, M.D., John P. Higgins, M.D.,Michael T. Deavers, M.D.
Stanford University Medical Center (RV, RAW, JPH), Department of Pathology (Laboratory of SurgicalPathology), Stanford, California; and The University of Texas-M.D. Anderson Cancer Center (JM, MTD),Houston, Texas
Primary (localized) non-Hodgkin’s lymphoma(NHL) of the ovary is rare. We studied eight cases ofprimary ovarian NHL to better understand the clin-icopathologic and immunophenotypic features ofthese tumors. The patients ranged in age from 29 to62 years (mean 47 years). Pelvic complaints werethe most common symptoms; however, three ofeight neoplasms were discovered incidentally. Alltumors were unilateral and Ann Arbor stage IE. Thethree incidental NHL were microscopic (largest 1.2cm), whereas the grossly evident lesions rangedfrom 7.5 to 20 cm (mean 13.3). Each tumor wasclassified according to the World Health Organiza-tion Classification as follows: diffuse large B-celllymphoma (three cases), follicular lymphoma (twocases), Burkitt lymphoma (one case), T-cell anaplas-tic large cell lymphoma (one case), and precursorT-lymphoblastic lymphoma (one case). Six tumorswere of B-cell lineage, and two tumors were of T-celllineage. All three diffuse large B-cell lymphomaswere positive for BCL-6, two were positive for CD10,and two were positive for BCL-2. Estrogen and pro-gesterone receptors were negative in all NHLs as-sessed. Patients were treated by various combina-tions of surgery, chemotherapy, and radiotherapy.Clinical follow-up ranged from 1.3 to 11.7 years(mean 5.2) and all patients were alive without dis-ease at last follow-up. We conclude that most pa-tients with primary ovarian NHL present withsymptoms attributable to an ovarian mass, but in asubset of patients ovarian NHL may be detectedincidentally. With appropriate therapy, patients ap-pear to have a favorable prognosis althoughfollow-up is short for some patients in this study.
KEY WORDS: Gynecologic, Immunohistochemistry,Lymphoma, Ovary.
Mod Pathol 2001;14(11):1093–1099
Non-Hodgkin’s lymphoma (NHL) may involve thegynecologic tract, and the ovary is one of the morecommon anatomic sites to be involved. Ovarianinvolvement by NHL is usually secondary, occur-ring as a part of systemic disease. Localized, pre-sumably primary, NHL of the ovary is rare (1).
Previous reports of ovarian NHL have includedboth primary and secondary cases. In these studies,primary NHLs of the ovary represent only a minor-ity of the cases reported, usually less than 10%.Thus, secondary cases have been well characterizedin the literature (2, 3), but information about pri-mary cases is limited.
Furthermore, several reported cases of primaryovarian NHL did not have adequate Ann Arbor stag-ing information, and therefore may not have beentruly localized. For these reasons, we chose to col-lect well-characterized cases of primary ovarianNHL to describe their clinicopathologic and immu-nophenotypic features.
MATERIALS AND METHODS
Cases of primary NHL of the ovary were identi-fied from the surgical pathology files of StanfordUniversity Medical Center and The University ofTexas-M.D. Anderson Cancer Center. These casesincluded both in-house surgical specimens andconsultation cases. We collected low-stage cases,designated as Ann Arbor stage IE after clinicopath-ologic staging, and considered these tumors to beprimary. In contrast, we considered NHL involvingthe ovary as a part of Ann Arbor stage IIIE and IVdisease to probably represent secondary involve-ment and excluded those cases from the study.However, we acknowledge that by using these def-initions, any NHL that arose in the ovary and sub-sequently disseminated would be eliminated from
Copyright © 2001 by The United States and Canadian Academy ofPathology, Inc.VOL. 14, NO. 11, P. 1093, 2001 Printed in the U.S.A.Date of acceptance: July 21, 2001.Address reprint requests to: Michael T. Deavers, M.D., The University ofTexas-M.D. Anderson Cancer Center, Department of Pathology, Box 85,1515 Holcombe Boulevard, Houston, TX 77030-4095; e-mail:[email protected].
1093
our study. We did not encounter any stage IIE cases.Four cases were previously reported in a clinico-pathologic review of NHL involving the gynecologictract (1), and the clinical features of three of thesecases were also reported elsewhere (4).
Clinical information was obtained by review ofthe medical chart and correspondence with the cli-nician. Histologic features were studied using sec-tions routinely stained with hematoxylin-eosin.Each neoplasm was classified according to the re-cently proposed World Health Organization Classi-fication (5).
Immunohistochemical studies were performedusing formalin-fixed, paraffin-embedded tissuesections and a variable panel of antibodies specificfor the following antigens: CD3, CD20, CD21, CD30,CD99, BCL-2, BCL-6, and ALK-1 (DAKO, Carpinte-ria, CA); CD10 (Novocastra, Burlingame, CA); CD43(Becton Dickinson, Franklin Lakes, NJ); estrogenand progesterone receptors (Ventana, Tucson, AZ);and TdT (SuperTechs, Bethesda, MD).
RESULTS
Clinical FeaturesEight cases of localized ovarian NHL, all Ann
Arbor stage IE, were included in this study. Thepatients ranged in age from 29 to 62 years (mean 47years). The most common presenting signs orsymptoms were: pelvic pain (n � 2); pelvic mass (n� 1); and urinary frequency and incontinence (n �1). One patient presented with constitutional symp-toms that were not otherwise specified. Three pa-
tients had neoplasms that were detected as inci-dental findings. Two of these patients underwenttotal abdominal hysterectomy and bilateralsalpingo-oophorectomy for uterine leiomyomas,and one patient had excision of an endometrioticcyst within which NHL was identified in the cystwall. All of the neoplasms were unilateral; sevenwere right-sided and one involved the left ovary.The three incidental tumors were microscopic(�1.2 cm), and no lesion was observed grossly. Fiveneoplasms were grossly identified and ranged insize from 7.5 to 20 cm (mean 13.3).
Treatment consisted of various combinations ofsurgery, chemotherapy, and radiotherapy. Sevenpatients were treated surgically: five underwent to-tal abdominal hysterectomy and bilateral salpingo-oophorectomy, and two underwent bilateralsalpingo-oophorectomy. Seven and two patients,respectively, received chemotherapy and radiother-apy. Clinical follow-up ranged from 1.3 to 11.7 years(mean 5.2 years). All patients were alive, relapse-free, and disease-free at last follow-up.
Histologic and Immunohistochemical Findings(Table 1)
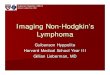
[Table 1] Three tumors (Cases 3, 4, and 7) werediffuse large B-cell lymphoma (DLBCL). Two DL-BCL had entirely diffuse architecture, while approx-imately 25 to 50% of one DLBCL (Case 7) containedfollicular areas. All of the DLBCL consisted of sheetsof large lymphoid cells with a moderate amount ofpale cytoplasm. The nuclei were round or had ir-
TABLE 1. Primary (Stage IE)Non-Hodgkin’s Lymphoma of the Ovary
CaseNo.
Age(y)
Presentation Side Size (cm) DiagnosisImmunophenotype
Therapy Follow-UpLineage CD10 CD99 Bcl-2 Bcl-6
1 29 Pelvic pain R 13 T-LBL T-cell � � ND � TAH-BSO,CT
NED, 5.8 y
2 39 Incidentalfinding
R Microscopic ALCL T-cell ND ND ND ND TAH-BSO NED, 4 y
3 41 Urinaryfrequency,incontinence
L 18 DLBCL B-cell � � � � BSO, CT,RT
NED, 5.5 y
4 43 Pelvic pain R 8 DLBCL B-cell � � � � TAH-BSO,CT
NED, 6 y
5 50 Incidentalfinding
R Microscopic Follicularlymphoma,Grade 2
B-cell � � � � TAH-BSO,CT
NED, 3.5 y
6 51 Incidentalfinding
R Microscopic Follicularlymphoma,Grade 3
B-cell � � � � TAH-BSO,CT
NED, 1.3 y
7 59 Pelvic mass R 7.5 DLBCLwithfollicularareas
B-cell � � � � BSO, CT NED, 3.5 y
8 62 Constitutionalsymptoms,NOS
R 20 BurkittLymphoma
B-cell � � ND � CT, RT NED, 11.7 y
ALCL, anaplastic large cell lymphoma; BSO, bilateral salpingo-oophorectomy; CT, chemotherapy; DLBCL, diffuse large B-cell lymphoma; ER, estrogenreceptor; ND, not done; NED, no evidence of disease; NOS, not otherwise specified (detailed clinical information of presentation not available); PR,progesterone receptor; RT, radiotherapy; TAH, total abdominal hysterectomy; T-LBL, precursor T-lymphoblastic lymphoma; �, positive; �, negative.
1094 Modern Pathology

regular nuclear contours, irregularly distributedchromatin, nucleoli, and many mitoses (Fig. 1). Thefollicular areas in Case 7 were composed of cellssimilar to those seen in the diffuse areas of thetumor. Areas of necrosis and sclerosis were ob-served. All three DLBCL were positive for CD20 andBCL-6, two cases were positive for CD10, and twocases were positive for BCL-2. The DLBCL withfollicular areas was negative for BCL-2.
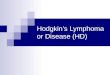
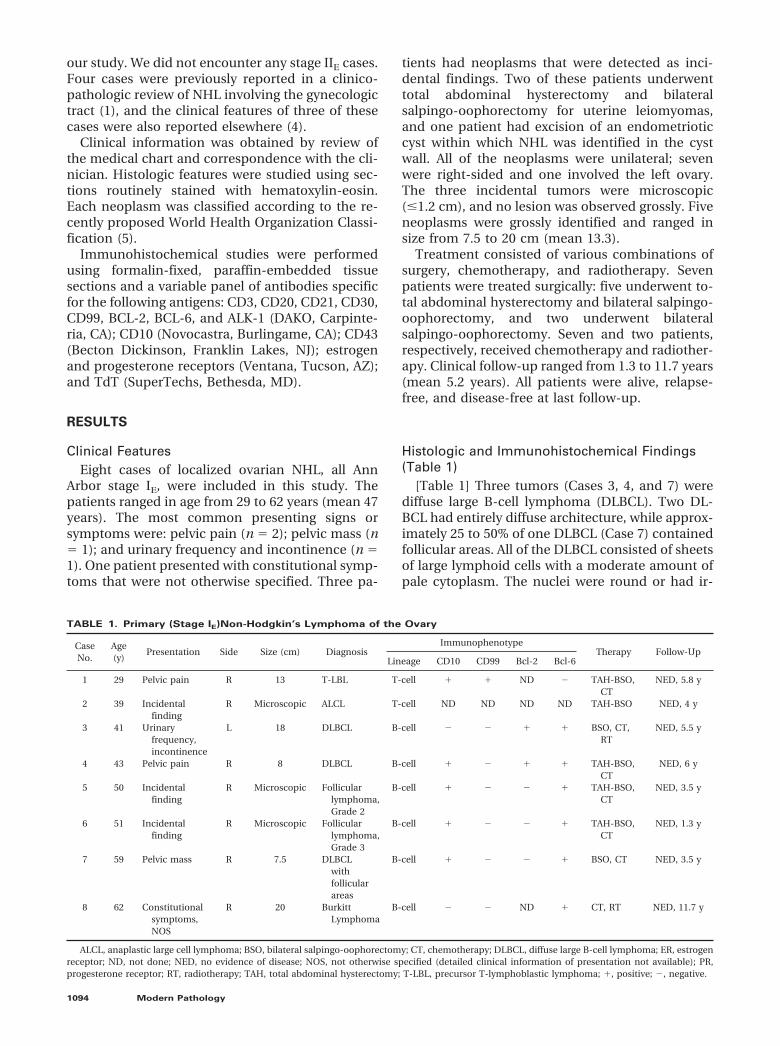
Two cases (Cases 5 and 6) were follicular lympho-mas. Case 5 was Grade 2, with a mixture of smallcleaved and atypical large cells. Case 6 was Grade 3(Fig. 2), with a predominance of large cleaved cells.Both cases were positive for CD10, CD20, andBCL-6 and negative for BCL-2. Staining for CD21 inCase 6 highlighted a network of follicular dendriticcells in follicles; the neoplastic cells were negative.
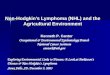
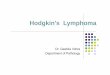
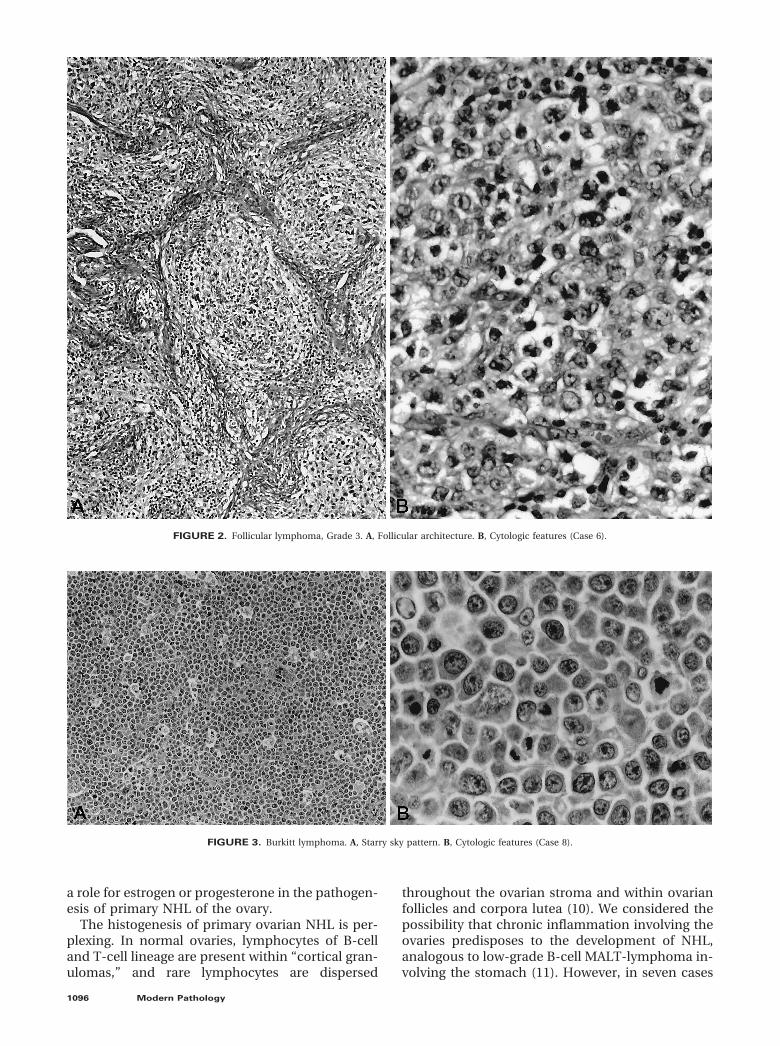
One case each was classified as Burkitt lym-phoma, T-cell anaplastic large cell lymphoma(ALCL), and T-precursor lymphoblastic lymphoma(T-LBL). The Burkitt lymphoma showed a starry-skybackground and was composed of a relatively mo-notonous population of intermediately-sized neo-plastic cells. These cells had round to slightly irreg-ular nuclear contours, an extremely high mitoticrate, and some cells had vesicular chromatin (Fig. 3,A–B). Thus, this tumor fits within the category ofatypical Burkitt lymphoma (previously designatedas Burkitt-like) in the WHO classification (4). Thistumor was positive for CD20 and BCL-6 but failedto stain for CD10. The T-cell ALCL was composed ofsheets of large round cells with a moderate amountof amphophilic cytoplasm. The nuclei were large,ovoid, and vesicular with large nucleoli. This neo-plasm was positive for CD43 and CD30, but wasnegative for ALK-1. The T-LBL was diffuse and com-posed of small cells with minimal cytoplasm thatinfiltrated collagen in a single file (“indian file”)pattern. The nuclei were round and convoluted.
The chromatin was fine with inconspicuous nucle-oli and mitoses were numerous (Fig. 4). The neo-plastic cells were positive for CD3, CD10, CD99, andTdT and were negative for BCL-6.
CD99 was assessed in seven tumors, one T-LBL(discussed above) and six B-cell NHL tumors: threeDLBCL, two follicular lymphomas, and one Burkittlymphoma (Cases 3 to 8). All six B-cell neoplasmswere negative for CD99. Residual ovarian stroma inthe hilum and reactive small lymphocytes withinthe lymphomatous infiltrate, were CD99-positive.Stains for estrogen (eight cases tested) and proges-terone (seven cases tested) receptors were negativein all cases assessed.
DISCUSSION
NHL uncommonly involves the gynecologic tract.However, when involved by NHL, the ovary is oneof the more common anatomic sites. Previous stud-ies of NHL involving gynecologic sites (1–3) haveshown that most NHL involving the ovary are sys-temic tumors, of which ovarian involvement is onlyone aspect. Less than 10% of all ovarian NHLs re-ported have been localized, presumably arising inthe ovary.
In the current study, we collected eight localized(Ann Arbor stage IE) ovarian NHL, which appear tohave arisen in the ovary, to further understand theirclinicopathologic and immunophenotypic features.The mean age of the patients was 47 years. Patientsusually sought medical attention for pelvic com-plaints, but in three patients the NHL was discov-ered as an incidental finding during the work-up ofother gynecologic diseases. The incidental neo-plasms were microscopic, whereas the grossly iden-tified lesions were large, up to 20 cm. The mostcommon types were DLBCL (three cases) and fol-licular lymphoma (two cases), and six of eight NHLwere of B-cell lineage. The patients were treated invarious fashions and all were disease free with amean follow-up of 5.2 years.
There is a suggestion in the literature that hor-mone receptors may be expressed by some hema-topoietic neoplasms. Although two primary ovarianNHL studied by Monterroso et al. (2) failed to ex-press estrogen receptors, others have shown estro-gen and progesterone receptor expression in pa-tient samples and cell lines of plasma cell myeloma,T-cell leukemia/lymphoma, acute myeloid leuke-mia, and B-cell chronic lymphocytic leukemia, asdetermined by immunocytochemical and bio-chemical assays (6 –9). Because the NHL in ourseries presumably arose within the gynecologictract, we assessed for the presence of estrogen andprogesterone receptors. All cases were negative.Thus, there is no immunohistochemical support ofFIGURE 1. Diffuse large B-cell lymphoma (Case 4).
Primary Ovarian Lymphoma (R. Vang et al.) 1095
a role for estrogen or progesterone in the pathogen-esis of primary NHL of the ovary.
The histogenesis of primary ovarian NHL is per-plexing. In normal ovaries, lymphocytes of B-celland T-cell lineage are present within “cortical gran-ulomas,” and rare lymphocytes are dispersed
throughout the ovarian stroma and within ovarianfollicles and corpora lutea (10). We considered thepossibility that chronic inflammation involving theovaries predisposes to the development of NHL,analogous to low-grade B-cell MALT-lymphoma in-volving the stomach (11). However, in seven cases
FIGURE 2. Follicular lymphoma, Grade 3. A, Follicular architecture. B, Cytologic features (Case 6).
FIGURE 3. Burkitt lymphoma. A, Starry sky pattern. B, Cytologic features (Case 8).
1096 Modern Pathology
there was no clinical or histologic evidence of in-flammation. In the ALCL, a background of dis-persed plasma cells and eosinophils of mild densitywas present within the wall of the endometrioticcyst. Thus, there is no obvious role for chronicinflammation in the pathogenesis of these tumors.
One of the findings in this series is that manycases of localized ovarian NHL are of follicle centerorigin. Three of eight (38%) NHLs in this study hadobvious follicular differentiation: two cases of fol-licular lymphoma (Cases 5 and 6) and one DLBCLwith follicular areas (Case 7). Also, the results of thestaining for CD10 and BCL-6 in our series maysuggest follicle center derivation for primary ovar-ian DLBCL. All three tumors expressed CD10and/or BCL-6. CD10 expression in non-neoplasticlymph nodes is confined predominantly to germi-nal centers and CD10 is also commonly expressedin follicular lymphomas (12, 13). Likewise, expres-sion of BCL-6, positive in all three DLBCL in thisstudy, is restricted to centroblasts and centrocytesof germinal centers (14), and is commonly ex-pressed by follicular lymphomas and DLBCL of fol-licle center origin (14, 15). Thus, the presence ofCD10 and/or BCL-6 expression in the DLBCL of thisstudy supports follicle center origin, as suggestedby others (12–15). The relatively high frequency ofovarian NHL of possible follicle center origin foundin this study has not been previously noted in theliterature (Table 2). The explanation for this is un-certain, but in most prior studies antibodies spe-cific for CD10 and BCL-6 that could be applied tofixed, paraffin-embedded tissue sections were notavailable.
Although 85% of nodal follicular lymphomasoverexpress BCL-2 (16) as a result of t(14;18), follic-ular lymphomas arising in extranodal sites are lessoften BCL-2-positive. Thus absence of BCL-2 ex-pression, as in the follicular areas of Cases 5 to 7 in
this study, may be a feature of primary follicularlymphoma of the ovary, analogous to follicular lym-phomas arising in other extranodal sites (17). How-ever, the follicular areas in our cases containedincreased numbers of large cells, and it is knownthat BCL-2 is expressed less often in Grade 3 follic-ular lymphoma (16, 17). Alternatively, our findingscould suggest that the bcl-2 gene does not play arole in the pathogenesis of primary ovarian follicu-lar lymphoma. Further molecular investigation toaddress this possibility has not been done.
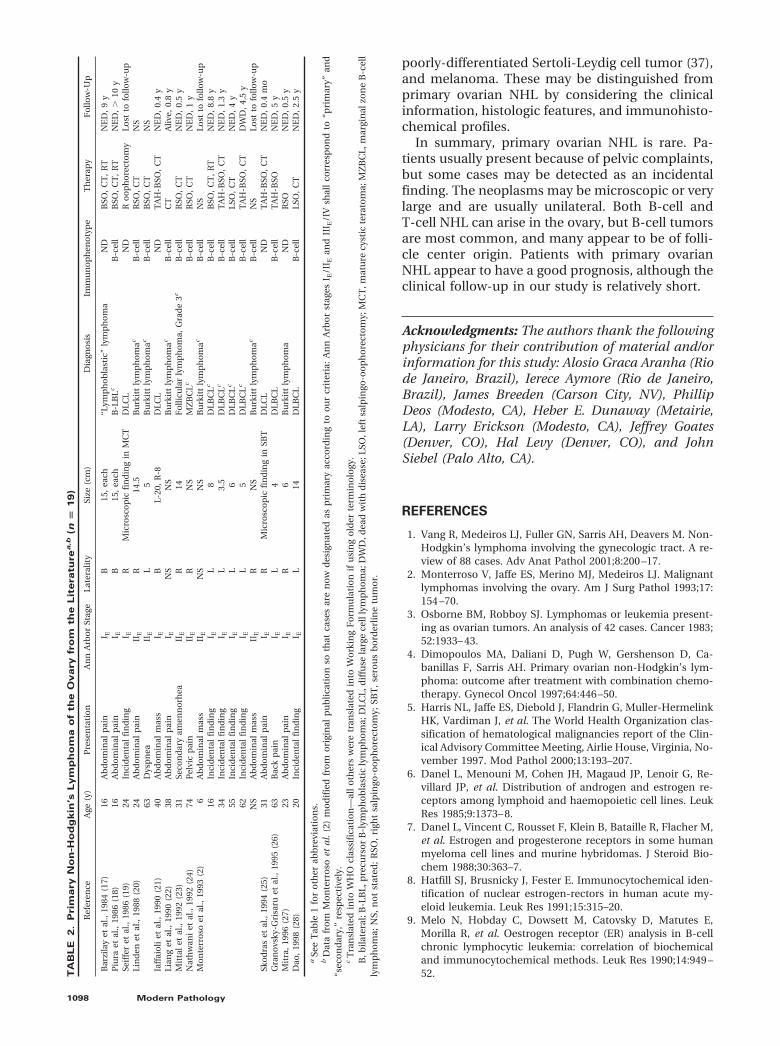
A summary of 19 cases of primary ovarian NHL(Ann Arbor stages IE or IIE) NHL (2, 18 –29) from theliterature is listed in Table 2. Some cases originallypublished using FIGO staging, but for which there isinsufficient information to translate into the AnnArbor system have not been included (3). The find-ings in our study are somewhat comparable. Thepatients have a wide age range, and most patientspresent with pelvic or abdominal complaints. How-ever, it is noteworthy that almost one third of casesare detected as incidental findings. The incidentalneoplasms may arise in unusual settings, such aswithin the wall of an ovarian endometriotic cyst(Case 2 of this study), or associated with a maturecystic teratoma (20) or serous borderline tumor(26). Bilaterality is infrequent, and neoplasms maybe microscopic or extremely large. DLBCL appearsto be the most common type of primary ovarianNHL. This is also true for other primary NHL arisingin other sites within the female genital tract (30 –32). Slight differences between the survival of pa-tients in our series, 100% at 5 years, and that ofpatients reported in the literature, 80% at 5 years,may be due to a paucity of cases with follow-uplonger than 5 years. Only one patient with primaryovarian NHL has died. However, the follow-up isrelatively short for several cases in our series, aswell as for those from the literature. Longerfollow-up is needed to more reliably determine thelong-term behavior of these lesions.
Histologically similar neoplasms that should bedifferentiated from NHL involving the ovary in-clude adult granulosa cell tumor, dysgerminoma,small cell carcinoma of hypercalcemic type (33),and granulocytic sarcoma. Depending on the indi-vidual case, other less histologically problematiclesions that may be included in the differential di-agnosis are poorly differentiated surface-epithelialor metastatic carcinomas, undifferentiated carci-noma (34), small cell carcinoma of pulmonary type(35), inflammatory pseudotumor, primitive neuro-ectodermal tumor (PNET), other non-PNET neuro-ectodermal tumors (36), variants of malignant me-sodermal mixed tumor with scarce epithelialelements and numerous round cells, endometrioidstromal sarcoma, rhabdomyosarcoma, intra-abdominal desmoplastic small round cell tumor,
FIGURE 4. Precursor T-lymphoblastic lymphoma (Case 1).
Primary Ovarian Lymphoma (R. Vang et al.) 1097
poorly-differentiated Sertoli-Leydig cell tumor (37),and melanoma. These may be distinguished fromprimary ovarian NHL by considering the clinicalinformation, histologic features, and immunohisto-chemical profiles.
In summary, primary ovarian NHL is rare. Pa-tients usually present because of pelvic complaints,but some cases may be detected as an incidentalfinding. The neoplasms may be microscopic or verylarge and are usually unilateral. Both B-cell andT-cell NHL can arise in the ovary, but B-cell tumorsare most common, and many appear to be of folli-cle center origin. Patients with primary ovarianNHL appear to have a good prognosis, although theclinical follow-up in our study is relatively short.
Acknowledgments: The authors thank the followingphysicians for their contribution of material and/orinformation for this study: Alosio Graca Aranha (Riode Janeiro, Brazil), Ierece Aymore (Rio de Janeiro,Brazil), James Breeden (Carson City, NV), PhillipDeos (Modesto, CA), Heber E. Dunaway (Metairie,LA), Larry Erickson (Modesto, CA), Jeffrey Goates(Denver, CO), Hal Levy (Denver, CO), and JohnSiebel (Palo Alto, CA).
REFERENCES
1. Vang R, Medeiros LJ, Fuller GN, Sarris AH, Deavers M. Non-Hodgkin’s lymphoma involving the gynecologic tract. A re-view of 88 cases. Adv Anat Pathol 2001;8:200 –17.
2. Monterroso V, Jaffe ES, Merino MJ, Medeiros LJ. Malignantlymphomas involving the ovary. Am J Surg Pathol 1993;17:154 –70.
3. Osborne BM, Robboy SJ. Lymphomas or leukemia present-ing as ovarian tumors. An analysis of 42 cases. Cancer 1983;52:1933– 43.
4. Dimopoulos MA, Daliani D, Pugh W, Gershenson D, Ca-banillas F, Sarris AH. Primary ovarian non-Hodgkin’s lym-phoma: outcome after treatment with combination chemo-therapy. Gynecol Oncol 1997;64:446 –50.
5. Harris NL, Jaffe ES, Diebold J, Flandrin G, Muller-HermelinkHK, Vardiman J, et al. The World Health Organization clas-sification of hematological malignancies report of the Clin-ical Advisory Committee Meeting, Airlie House, Virginia, No-vember 1997. Mod Pathol 2000;13:193–207.
6. Danel L, Menouni M, Cohen JH, Magaud JP, Lenoir G, Re-villard JP, et al. Distribution of androgen and estrogen re-ceptors among lymphoid and haemopoietic cell lines. LeukRes 1985;9:1373– 8.
7. Danel L, Vincent C, Rousset F, Klein B, Bataille R, Flacher M,et al. Estrogen and progesterone receptors in some humanmyeloma cell lines and murine hybridomas. J Steroid Bio-chem 1988;30:363–7.
8. Hatfill SJ, Brusnicky J, Fester E. Immunocytochemical iden-tification of nuclear estrogen-rectors in human acute my-eloid leukemia. Leuk Res 1991;15:315–20.
9. Melo N, Hobday C, Dowsett M, Catovsky D, Matutes E,Morilla R, et al. Oestrogen receptor (ER) analysis in B-cellchronic lymphocytic leukemia: correlation of biochemicaland immunocytochemical methods. Leuk Res 1990;14:949 –52.T
AB
LE
2.
Prim
ary
No
n-H
od
gkin
’sLym
ph
om
ao
fth
eO
va
ry
fro
mth
eL
ite
ra
tu
re
a,b
(n�
19
)
Ref
eren
ceA
ge(y
)P
rese
nta
tio
nA
nn
Arb
or
Stag
eLa
tera
lity
Size
(cm
)D
iagn
osi
sIm
mu
no
ph
eno
typ
eT
her
apy
Fo
llow
-Up
Bar
zila
yet
al.,
1984
(17)
16A
bd
om
inal
pai
nI E
B15
,ea
ch“L
ymp
ho
bla
stic
”ly
mp
ho
ma
ND
BSO
,C
T,
RT
NE
D,
9y
Piu
raet
al.,
1986
(18)
16A
bd
om
inal
pai
nI E
B15
,ea
chB
-LB
LcB
-cel
lB
SO,
CT
,R
TN
ED
,�
10y
Seif
fer
etal
.,19
86(1
9)24
Inci
den
tal
fin
din
gI E
RM
icro
sco
pic
fin
din
gin
MC
TD
LCL
ND
Ro
op
ho
rect
om
yLo
stto
follo
w-u
pLi
nd
enet
al.,
1988
(20)
24A
bd
om
inal
pai
nII
ER
14.5
Bu
rkit
tly
mp
ho
mac
B-c
ell
RSO
,C
TN
S63
Dys
pn
eaII
EL
5B
urk
itt
lym
ph
om
acB
-cel
lB
SO,
CT
NS
Iaff
aio
liet
al.,
1990
(21)
40A
bd
om
inal
mas
sI E
BL-
20,
R-8
DLC
LN
DT
AH
-BSO
,C
TN
ED
,0.
4y
Lian
get
al.,
1990
(22)
38A
bd
om
inal
pai
nI E
NS
NS
Bu
rkit
tly
mp
ho
mac
B-c
ell
CT
Aliv
e,0.
8y
Mit
tal
etal
.,19
92(2
3)31
Seco
nd
ary
amen
no
rhea
IIE
R14
Fo
llicu
lar
lym
ph
om
a,G
rad
e3c
B-c
ell
RSO
,C
TN
ED
,0.
5y
Nat
hw
ani
etal
.,19
92(2
4)74
Pel
vic
pai
nII
ER
NS
MZ
BC
LcB
-cel
lR
SO,
CT
NE
D,
1y
Mo
nte
rro
soet
al.,
1993
(2)
6A
bd
om
inal
mas
sII
EN
SN
SB
urk
itt
lym
ph
om
acB
-cel
lN
SLo
stto
follo
w-u
p16
Inci
den
tal
fin
din
gI E
L8
DLB
CLc
B-c
ell
BSO
,C
T,
RT
NE
D,
8.8
y34
Inci
den
tal
fin
din
gI E
L3.
5D
LBC
LcB
-cel
lT
AH
-BSO
,C
TN
ED
,1.
3y
55In
cid
enta
lfi
nd
ing
I EL
6D
LBC
LcB
-cel
lLS
O,
CT
NE
D,
4y
62In
cid
enta
lfi
nd
ing
I EL
5D
LBC
LcB
-cel
lT
AH
-BSO
,C
TD
WD
,4.
5y
NS
Ab
do
min
alm
ass
IIE
RN
SB
urk
itt
lym
ph
om
acB
-cel
lN
SLo
stto
follo
w-u
pSk
od
ras
etal
.,19
94(2
5)31
Ab
do
min
alp
ain
I ER
Mic
rosc
op
icfi
nd
ing
inSB
TD
LCL
ND
TA
H-B
SO,
CT
NE
D,
0.4
mo
Gra
no
vsky
-Gri
saru
etal
.,19
95(2
6)63
Bac
kp
ain
I EL
4D
LBC
LB
-cel
lT
AH
-BSO
NE
D,
5y
Mit
ra,
1996
(27)
23A
bd
om
inal
pai
nI E
R6
Bu
rkit
tly
mp
ho
ma
ND
RSO
NE
D,
0.5
yD
ao,
1998
(28)
20In
cid
enta
lfi
nd
ing
I EL
14D
LBC
LB
-cel
lLS
O,
CT
NE
D,
2.5
y
aSe
eT
able
1fo
ro
ther
abb
revi
atio
ns.
bD
ata
fro
mM
on
terr
oso
etal
.(2
)m
od
ifie
dfr
om
ori
gin
alp
ub
licat
ion
soth
atca
ses
are
no
wd
esig
nat
edas
pri
mar
yac
cord
ing
too
ur
crit
eria
:A
nn
Arb
or
stag
esI E
/II E
and
III E
/IV
shal
lco
rres
po
nd
to“p
rim
ary”
and
“sec
on
dar
y,”
resp
ecti
vely
.c
Tra
nsl
ated
into
WH
Ocl
assi
fica
tio
n—
all
oth
ers
wer
etr
ansl
ated
into
Wo
rkin
gF
orm
ula
tio
nif
usi
ng
old
erte
rmin
olo
gy.
B,b
ilate
ral;
B-L
BL,
pre
curs
or
B-l
ymp
ho
bla
stic
lym
ph
om
a;D
LCL,
dif
fuse
larg
ece
llly
mp
ho
ma;
DW
D,d
ead
wit
hd
isea
se;L
SO,l
eft
salp
ingo
-oo
ph
ore
cto
my;
MC
T,m
atu
recy
stic
tera
tom
a;M
ZB
CL,
mar
gin
alzo
ne
B-c
ell
lym
ph
om
a;N
S,n
ot
stat
ed;
RSO
,ri
ght
salp
ingo
-oo
ph
ore
cto
my;
SBT
,se
rou
sb
ord
erlin
etu
mo
r.
1098 Modern Pathology
10. Suzuki T, Sasano H, Takaya R, Fukaya T, Yajima A, Date F, etal. Leukocytes in normal-cycling human ovaries: immuno-histochemical distribution and characterization. Hum Re-prod 1998;13:2186 –91.
11. Hussell T, Isaacson PG, Crabtree JE, Spencer J. The responseof cells from low-grade B-cell gastric lymphomas of mucosa-associated lymphoid tissue to Helicobacter pylori. Lancet1993;4:571– 4.
12. Dogan A, Bagdi E, Munson P, Isaacson PG. CD10 and BCL-6expression in paraffin sections of normal lymphoid tissueand B-cell lymphomas. Am J Surg Pathol 2000;24:846 –52.
13. Fang JM, Finn WG, Hussong JW, Goolsby CL, Cubbon AR,Variakojis D. CD10 antigen expression correlates with thet(14;18)(q32;q21) major breakpoint region in diffuse largeB-cell lymphoma. Mod Pathol 1999;12:295–300.
14. Flenghi L, Ye BH, Fizzotti M, Bigerna B, Cattoretti G, VenturiS, et al. A specific monoclonal antibody (PG-B6) detectsexpression of the BCL-6 protein in germinal center B cells.Am J Pathol 1995;147:405–11.
15. Raible MD, His ED, Alkan S. Bcl-6 protein expression byfollicle center lymphomas. A marker for differentiating folli-cle center lymphomas from other low-grade lymphoprolif-erative disorders. Am J Clin Pathol 1999;112:101–7.
16. Gaulard P, d’Agay MF, Peuchmaur M, Brousse N, Gisselbre-cht C, Solal-Celigny P, et al. Expression of the bcl-2 geneproduct in follicular lymphoma. Am J Pathol 1992;140:1089 –95.
17. Cerroni L, Arzberger E, Putz B, Hofler G, Metze D, Sander CA,et al. Primary cutaneous follicle center cell lymphoma withfollicular growth pattern. Blood 2000;95:3922– 8.
18. Barzilay J, Rakowsky E, Rahima M, Yanai-Inbar I. Malignantlymphoma of the ovary: report of a case and review of theliterature. Obstet Gynecol 1984;64:93S.
19. Piura B, Bar-David J, Glezerman M, Zirkin HJ. Bilateral ovar-ian involvement as the only manifestation of malignant lym-phoma. J Surg Oncol 1986;33:126 – 8.
20. Seifer DB, Weiss LM, Kempson RL. Malignant lymphomaarising within thyroid tissue in a mature cystic teratoma.Cancer 1986;58:2459 – 61.
21. Linden MD, Tubbs RR, Fishleder AJ, Hart WR. Immunotypicand genotypic characterization of non-Hodgkin’s lympho-mas of the ovary. Am J Clin Pathol 1988;89:156 – 62.
22. Iaffaioli RV, Frasci G, Di Tuoro AS, Facchini G, Pacelli R,Scala S, et al. Malignant lymphoma of the ovary: report ontwo cases and review of the literature. Eur J Gynaecol Oncol1990;11:205– 8.
23. Liang R, Chiu E, Loke SL. Non-Hodgkin’s lymphomas involv-ing the female genital tract. Hematol Oncol 1990;8:295–9.
24. Mittal KR, Blechman A, Greco MA, Alfonso F, Demopoulos R.Lymphoma of ovary with stromal luteinization, presentingas secondary amenorrhea. Gynecol Oncol 1992;45:69 –75.
25. Nathwani BN, Mohrmann RL, Brynes RK, Taylor CR, Hans-mann ML, Sheibani K. Monocytoid B-cell lymphomas: anassessment of diagnostic criteria and a perspective on his-togenesis. Hum Pathol 1992;23:1061–71.
26. Skodras G, Fields V, Kragel PJ. Ovarian lymphoma and se-rous carcinoma of low malignant potential arising in thesame ovary. A case report with literature review of 14 pri-mary ovarian lymphomas. Arch Pathol Lab Med 1994;118:647–50.
27. Granovsky-Grisaru S, Beller U, Gal M, Diamant YZ, Rosen-mann E. Primary lymphoma of the ovary. A case report andcritical review of the literature. Eur J Gynaecol Oncol 1995;16:392–5.
28. Mitra K. Primary lymphoma of ovary. J Ind Med Assoc 1996;94:161.
29. Dao AH. Malignant lymphoma of the ovary: report of a casesuccessfully managed with surgery and chemotherapy. Gy-necol Oncol 1998;70:137– 40.
30. Vang R, Medeiros LJ, Ha CS, Deavers M. Non-Hodgkin’slymphomas involving the uterus: a clinicopathologic analy-sis of 26 cases. Mod Pathol 2000;13:19 –28.
31. Vang R, Medeiros LJ, Malpica A, Levenback C, Deavers M.Non-Hodgkin’s lymphoma involving the vulva. Int J GynecolPathol 2000;19:236 – 42.
32. Vang R, Medeiros LJ, Silva EG, Gershenson DM, Deavers M.Non-Hodgkin’s lymphoma involving the vagina: a clinico-pathologic analysis of 14 patients. Am J Surg Pathol 2000;24:719 –25.
33. Young RH, Oliva E, Scully RE. Small cell carcinoma of theovary, hypercalcemic type. A clinicopathological analysis of150 cases. Am J Surg Pathol 1994;18:1102–16.
34. Silva EG, Tornos C, Bailey MA, Morris M. Undifferentiatedcarcinoma of the ovary. Arch Pathol Lab Med 1991;115:377–81.
35. Eichhorn JH, Young RH, Scully RE. Primary ovarian smallcell carcinoma of pulmonary type. A clinicopathologic, im-munohistologic, and flow cytometric analysis of 11 cases.Am J Surg Pathol 1992;16:926 –38.
36. Kleinman GM, Young RH, Scully RE. Primary neuroectoder-mal tumors of the ovary. A report of 25 cases. Am J SurgPathol 1993;17:764 –78.
37. Young RH, Scully RE. Ovarian Sertoli-Leydig cell tumors. Aclinicopathological analysis of 207 cases. Am J Surg Pathol1985;9:543– 69.
Primary Ovarian Lymphoma (R. Vang et al.) 1099
View publication statsView publication stats