Embed Size (px)
Citation preview

Overcoming Presbyopia by Manipulating
the Eyes’ Optics
by
Leonard A. Zheleznyak
Submitted in Partial Fulfillment
of the
Requirements for the Degree
Doctor of Philosophy
Supervised by
Professor Geunyoung Yoon
The Institute of Optics Arts, Sciences and Engineering
Edmund A. Hajim School of Engineering and Applied Sciences
University of Rochester Rochester, NY
2014

ii
To my grandfather, Professor Boris D. Rakover,
whose memory has guided me here.

iii
Biographical Sketch
Leonard Zheleznyak was born in Rochester, NY on November 19, 1983. He
attended the University of Rochester, completing a Bachelor of Science in Optics, with
minors in Mathematics and Russian Language in 2005 and a Master of Science in Optics
in 2006. From 2006 to 2008, he was employed as an optical engineer at Ometric
Corporation in Columbia, South Carolina. He returned to the University of Rochester in
the Fall of 2008 and began doctoral studies in Optics where he pursued research in
physiological optics under the direction of Professor Geunyoung Yoon.
The following publications were a result of work conducted during doctoral study:
Zheleznyak, L., Jung, H., & Yoon, G. (2014). Impact of pupil transmission apodization on presbyopic through-focus visual performance with spherical aberration. Investigative
ophthalmology & visual science, 55(1), 70-77.
Zheleznyak, L., Sabesan, R., Oh, J. S., MacRae, S., & Yoon, G. (2013). Modified monovision with spherical aberration to improve presbyopic through-focus visual performance. Investigative ophthalmology & visual science, 54(5), 3157-3165. Sabesan, R., Zheleznyak, L., & Yoon, G. (2012). Binocular visual performance and summation after correcting higher order aberrations. Biomedical optics express, 3(12), 3176-3189. Zheleznyak, L., Kim, M. J., MacRae, S., & Yoon, G. (2012). Impact of corneal aberrations on through-focus image quality of presbyopia-correcting intraocular lenses using an adaptive optics bench system. Journal of Cataract & Refractive Surgery, 38(10), 1724-1733. Kim, M. J., Zheleznyak, L., MacRae, S., Tchah, H., & Yoon, G. (2011). Objective evaluation of through-focus optical performance of presbyopia-correcting intraocular lenses using an optical bench system. Journal of Cataract & Refractive Surgery, 37(7), 1305-1312.

iv
Acknowledgements
The research presented herein would not have been possible without the support
of many individuals, whom I would like to acknowledge here.
Firstly, I wish to sincerely thank my advisor, Dr. Geunyoung Yoon. His resolute
dedication, encouragement and guidance have been invaluable on this journey. His
enthusiasm for research and determination to see the forest from the trees set a standard
to which I will always aspire. Late night brainstorming sessions at the white-board made
for some of the most creative and fun moments in the lab. It has been a privilege and a
pleasure to be a member of his lab.
I would like to thank Scott MacRae, David Williams, Duje Tadin and Wayne
Knox for being on my thesis committee and for their valuable time and contributions to
this research. I would particularly like to thank Scott for constantly reminding me of the
clinical importance of our work. I would like to thank David Williams for his exemplary
research ethic, insightful observations and for creating a rich environment for science as
the director of the Center for Visual Science. I would like to acknowledge Duje Tadin for
his encouragement, contagious passion and patient explanation of neural processes. I
would also like to thank Wayne Knox for his advice on this research and encouraging me
to pursue a doctorate. Without his support, I would not have made it back to Rochester
for the doctoral program. I would also like to thank my committee chair, Jennifer Hunter,
for contributing her time and efforts.
I am thankful to my research collaborators for their important contributions:
Myoung-Joon Kim, Jens Bühren, Ian Cox, Griff Altmann and Jill Schaefer. To Myoung-
Joon, for his clinical expertise and supplying intraocular lenses for testing. To Jens, for

v
obtaining corneal topography data for pseudophakic patients in Frankfurt. To Ian, for his
scientific insight, thoughtful encouragement in our research, and with whom it was
always a pleasure to work on multiple projects. To Griff, for his support and attention to
detail in our collaboration. To Jill, for screening patients and performing eye exams on
research volunteers.
I am indebted to my lab-mates, past and present, who provided friendship, in and
out of the lab. I would like to thank Ramkumar Sabesan and Rahul Yadav for welcoming
me to the lab and setting an example of passion and dedication to research. Thank you for
reminding me of life outside the lab and becoming true, life-long friends. I would like to
thank Aixa Alarcon, Leslie Richardson and Daniel Pamplin for embracing our
memorable Hafiz poetry breaks. I would also like to thank Ranjini Kottaiyan, Ashutosh
Richhariya, Cynthia Tung, Je-Sun Oh, Shizuka Koh, Lana Nagy, HaeWon Jung, Joung
Yoon Kim, Michael Martino, Mengchen Xu, Amanda Kingston, Ben Fiefke and Brett
Sternfield.
I am sincerely grateful to the brilliant professors of the Institute of Optics: they
planted the seed of curiosity in my early days as an undergraduate. I would especially like
to thank professors James R. Fienup, Jim Zavislan, Andrew Berger, Tom Brown,
Nicholas George, Lukas Novotny and Miguel Alonso for introducing me to the elegance
of optics.
I would like to acknowledge the technical staff at the Center for Visual Science
for their assistance in many areas of my research. A very special thanks are due to
Kamran Ahmad and Keith Parkins, for their great help in developing software
applications for all the optical systems I built: without their help, none of the research

vi
presented here would have been possible. I would also like to thank Martin Gira, Ted
Tweitmeyer and Chris Freemesser for their help and expertise in electronics and IT
related issues.
I would like to thank my optics friends for helping me survive the first year and
defeat the preliminary exam: David Tourjee, Tammy Lee, Manuel Guizar, Yusufu Sulai,
Robin Sharma, Peter McCarthy, Kyle Fuerschbach, Richard Smith, Daniel Sidor. I would
also like to thank my colleagues at the Center for Visual Science for their valuable input:
Ben Masella, Ying Geng, Alfredo Dubra, Kevin Dieter, Davis Glasser, Michael Melnick,
Lu Yin, Jesse Schallek, Ethan Rossi, James Feeks and Andres Guevara.
I am sincerely thankful to the administrative staff of the Flaum Eye Institute,
Center for Visual Science and the Institute of Optics for patiently helping with ordering
items assistance with paperwork and deadlines. This includes Dollie Aiken, Peter
MacDowell, Teresa Williams, Debbie Shannon, Michele Schultz, Sara Peterson, Gayle
Thompson, Lori Russell, Noelene Votens, Gina Kern, Maria Schnitzler and the ever
optimistic Betsy Benedict.
Following my Masters degree, I joined Ometric Corporation in South Carolina,
never expecting to return to academia. This outstanding team of intellectuals created a
thoroughly enjoyable work environment and encouraged me to return to Rochester to
pursue my doctorate. I am grateful for their mentorship and stimulation. I would like to
thank Robert Freese, Walter Alessandrini, Ryan Priore, Bill Soltmann, David Perkins,
Professor Michael Myrick, Terrell Teague, Jason Williamson and John Blackburn.
I owe my sincere thanks to all the research subjects who kindly volunteered their
time to participate in our studies. These generous individuals endured painful eye drops,

vii
dental moulds, hours of tedious psychophysical experiments and incessant requests to
“blink and open wide”.
I would like to thank my parents, Anna and Alexander Zheleznyak, who have
been an endless source of guidance, home-cooked meals and therapeutic trips to the JCC
sauna. I would like to thank my brother, Matthew, for his endless support and keeping my
inner child alive and well. I would like to thank my wife’s parents, Svetlana and Sam
Radunsky, for their support and encouragement. I would also like to thank my brother-in-
law and fellow optics alum, Dr. Aleksandr Radunsky, for being a true friend and
colleague.
Most of all, I would like to thank my wonderful wife, Galina Radunsky, whom I
am truly fortunate to have as my life partner. Thank you for supporting me through the
hard times and turbulence of this adventure. It was a long journey, and it has been a
blessing to have you by my side every step of the way.

viii
Abstract
Presbyopia, the age-related loss of accommodation, is a visual condition affecting
all adults over the age of 45 years. In presbyopia, individuals lose the ability to focus on
nearby objects, due to a lifelong growth and stiffening of the eye’s crystalline lens. This
leads to poor near visual performance and affects patients’ quality of life. The objective
of this thesis is aimed towards the correction of presbyopia and can be divided into four
aims.
First, we examined the characteristics and limitations of currently available
strategies for the correction of presbyopia. A natural-view wavefront sensor was used to
objectively measure the accommodative ability of patients implanted with an
accommodative intraocular lens (IOL). Although these patients had little accommodative
ability based on changes in power, pupil miosis and higher order aberrations led to an
improvement in through-focus retinal image quality in some cases. To quantify the
through-focus retinal image quality of accommodative and multifocal IOLs directly, an
adaptive optics (AO) IOL metrology system was developed. Using this system, the
impact of corneal aberrations in regard to presbyopia-correcting IOLs was assessed,
providing an objective measure of through-focus retinal image quality and practical
guidelines for patient selection.
To improve upon existing multifocal designs, we investigated retinal image
quality metrics for the prediction of through-focus visual performance. The preferred
metric was based on the fidelity of an image convolved with an aberrated point spread
function. Using this metric, we investigated the potential of higher order aberrations and
pupil amplitude apodization to increase the depth of focus of the presbyopic eye.

ix
Thirdly, we investigated modified monovision, a novel binocular approach to
presbyopia correction using a binocular AO vision simulator. In modified monovision,
different magnitudes of defocus and spherical aberration are introduced to each eye,
thereby taking advantage of the binocular visual system. Several experiments using the
binocular AO vision simulator found modified monovision led to significant
improvements in through-focus visual performance, binocular summation and
stereoacuity, as compared to traditional monovision.
Finally, we addressed neural factors, affecting visual performance in modified
monovision, such as ocular dominance and neural plasticity. We found that pairing
modified monovision with a vision training regimen may further improve visual
performance beyond the limits set by optics via neural plasticity. This opens the door to
an exciting new avenue of vision correction to accompany optical interventions.
The research presented in this thesis offers important guidelines for the clinical
and scientific communities. Furthermore, the techniques described herein may be applied
to other fields of ophthalmology, such as childhood myopia progression.

x
Contributors and Funding Sources This work was supervised by a dissertation committee consisting of Professor
Geunyoung Yoon (advisor) from the Department of Ophthalmology, Professor David
Williams from the Institute of Optics, Professor Wayne Knox from the Institute of Optics,
Professor Duje Tadin from the Department of Brain and Cognitive Sciences and
Professor Scott MacRae from the Department of Ophthalmology.
Portions of chapter 3 have been published in – Zheleznyak, L., Kim, M. J.,
MacRae, S., & Yoon, G. (2012). Impact of corneal aberrations on through-focus image
quality of presbyopia-correcting intraocular lenses using an adaptive optics bench
system. Journal of Cataract & Refractive Surgery, 38(10), 1724-1733 and Kim, M. J.,
Zheleznyak, L., MacRae, S., Tchah, H., & Yoon, G. (2011). Objective evaluation of
through-focus optical performance of presbyopia-correcting intraocular lenses using an
optical bench system. Journal of Cataract & Refractive Surgery, 37(7), 1305-1312. The
intraocular lenses were provided by Dr. Scott MacRae and Dr. Myoung-Joon Kim. The
control software for the adaptive optics IOL metrology system was developed by Kamran
Ahmad from the Center for Visual Science, University of Rochester, with the directions
provided by the author.
Portions of chapter 4 have been published in – Zheleznyak, L., Jung, H., & Yoon,
G. (2014). Impact of pupil transmission apodization on presbyopic through-focus visual
performance with spherical aberration. Investigative ophthalmology & visual
science, 55(1), 70-77. The control software for the Badal optometer was developed by
Kamran Ahmad with directions provided by the author. The visual stimulus projectors

xi
were modified for use in the adaptive optics vision simulator by Ted Tweitmeyer from
the Center for Visual Science, University of Rochester.
Portions of chapter 5 have been published in – Zheleznyak, L., Sabesan, R., Oh, J.
S., MacRae, S., & Yoon, G. (2013). Modified monovision with spherical aberration to
improve presbyopic through-focus visual performance. Investigative ophthalmology &
visual science, 54(5), 3157-3165 and Sabesan, R., Zheleznyak, L., & Yoon, G. (2012).
Binocular visual performance and summation after correcting higher order
aberrations. Biomedical optics express, 3(12), 3176-3189. Ramkumar Sabesan and
Geunyoung Yoon built the first generation of the binocular adaptive optics vision
simulator. The control software for the binocular adaptive optics vision simulator was
developed by Kamran Ahmad and Keith Parkins from the Center for Visual Science,
University of Rochester, with inputs from the author. The LED pupil illumination system
was fabricated by Martin Gira from the Center for Visual Science, University of
Rochester.
Unless mentioned above or in the thesis, the research presented here was
performed by the author. The research done for this thesis was supported by a graduate
training fellowship provided by the National Institute of Health (National Eye Institute)
and research grants provided by the National Institute of Health (National Eye Institute),
Research to Prevent Blindness, Center for Emerging and Innovative Sciences and Bausch
& Lomb.

xii
Table of Contents
Title Page ............................................................................................................................. i
Dedication ........................................................................................................................... ii
Biographical Sketch ........................................................................................................... iii
Acknowledgements............................................................................................................ iv
Abstract ............................................................................................................................ viii
Contributors and Funding Sources...................................................................................... x
Table of Contents.............................................................................................................. xii
List of Tables .................................................................................................................... xv
List of Figures .................................................................................................................. xvi
Chapter 1. Introduction ....................................................................................................... 1
1.1 Background and Significance ................................................................................... 1
1.2 Physiology of Accommodation and Presbyopia ....................................................... 5
1.3 Impact of Presbyopia on Retinal Image Quality....................................................... 7
1.4 Presbyopia Correction Strategies ............................................................................ 13
1.4.1 Pseudophakic Accommodation........................................................................ 14
1.4.2 Increasing the Eye’s Depth of Focus ............................................................... 17
1.5 Binocular Vision and Presbyopia............................................................................ 21
1.6 Neural Aspects to Presbyopic Correction ............................................................... 24
1.6.1 Ocular Dominance ........................................................................................... 24
1.6.2 Neural Plasticity............................................................................................... 26
1.7 Thesis Outline ......................................................................................................... 32
Chapter 2. Objective Measurement of Accommodating Intraocular Lens Efficacy......... 35
2.1 Introduction to Accommodating IOLs.................................................................... 35
2.2 Objective Measurement of Accommodation .......................................................... 41
2.3 Accommodative Response with the Crystalens Accommodating IOL................... 45
2.4 Conclusions............................................................................................................. 51
Chapter 3. Impact of Corneal Aberrations on Optical Quality of Presbyopia-Correcting
Intraocular Lenses ............................................................................................................. 52
3.1 Introduction............................................................................................................. 52

xiii
3.2 Corneal Aberrations of Post-Cataract Extraction Patients...................................... 54
3.3 Adaptive-Optics Intraocular Lens Metrology......................................................... 54
3.4 Experimental Protocol ............................................................................................ 57
3.5 Impact of Pupil Size with Aberration-Free Cornea ................................................ 59
3.6 Impact of Corneal Astigmatism.............................................................................. 62
3.7 Impact of Corneal Higher Order Aberrations ......................................................... 65
3.8 Summary................................................................................................................. 67
Chapter 4. Extending The Eye’s Depth of Focus ............................................................. 69
4.1 Introduction............................................................................................................. 69
4.2 Retinal Image Quality Metrics................................................................................ 71
4.2.1 Convolution Based Image Quality Metric ....................................................... 74
4.2.2 Experimental Validation with Adaptive Optics Vision Simulator .................. 78
4.2.3 Prediction of Through-Focus Visual Acuity.................................................... 80
4.3 Optimizing Wavefront Aberrations for Increased Depth of Focus......................... 85
4.3.1 Higher Order Aberrations and Through-Focus Image Quality........................ 86
4.3.2 Through-Focus Visual Performance with Spherical Aberrations.................... 95
4.3.3 Discussion ........................................................................................................ 97
4.4 Interaction of Transmission Apodization and Higher Order Aberrations ............ 101
4.4.1 Introduction.................................................................................................... 101
4.4.2 Through-Focus Image Quality with Combined Apodization and Higher Order
Aberrations.............................................................................................................. 102
4.4.3 Through-Focus Visual Performance with Combined Apodization and Higher
Order Aberrations ................................................................................................... 105
4.4.4 Discussion ...................................................................................................... 110
4.5 Summary............................................................................................................... 113
Chapter 5. Modified Monovision: A Binocular Approach To Presbyopia Correction... 114
5.1 Introduction........................................................................................................... 114
5.2 Modifying Monovision with Monocular Spherical Aberration ............................ 117
5.2.1 Theoretical Modeling of Binocular Through-focus Retinal Image Quality .. 118
5.3 Binocular Through-Focus Visual Performance .................................................... 121
5.3.1 Binocular Adaptive Optics Vision Simulator ................................................ 121

xiv
5.3.2 Experimental Protocol ................................................................................... 131
5.3.3 Through-Focus Contrast Sensitivity and Binocular Summation ................... 132
5.3.4 Through-Focus Visual Acuity........................................................................ 135
5.4 Optimization of Modified Monovision................................................................. 139
5.5 Discussion ............................................................................................................. 146
Chapter 6. Neural Factors Affecting Visual Performance in Modified Monovision...... 149
6.1 Introduction........................................................................................................... 149
6.2 The Role of Ocular Dominance in Binocular Visual Performance ...................... 150
6.2.1 Sighting Versus Sensory Ocular Dominance................................................. 150
6.2.2 Determining the Degree of Ocular Dominance ............................................. 153
6.2.3 Impact on Through-Focus Visual Acuity ...................................................... 156
6.2.4 Impact on Through-Focus Contrast Sensitivity ............................................. 158
6.2.5 Discussion ...................................................................................................... 160
6.2.6 Summary........................................................................................................ 162
6.3 Perceptual Learning in Modified Monovision...................................................... 163
6.3.1. Introduction................................................................................................... 163
6.3.2 Experimental Protocol of Vision Training Regimen ..................................... 165
6.3.3 Vision Training with Modified and Traditional Monovision ........................ 172
6.3.4 Discussion ...................................................................................................... 178
6.4 Conclusions........................................................................................................... 182
Chapter 7. Conclusions ................................................................................................... 184
References....................................................................................................................... 190

xv
List of Tables
Table Title Page
1.1 Methods for correcting presbyopia 14
4.1 Unit conversion of letter sizes 80
5.1 Maximum stroke of ALPAO DM97 deformable mirror per Zernike
mode for a 4.0 mm pupil
127
6.1 Perceptual learning training spatial frequencies 171

xvi
List of Figures
Figure Title Page
1.1 Schematic diagram of the eye. 6
1.2 Subjectively measured amplitude of accommodation (Duane, 1912).
Average and upper and lower limits are indicated by black line and
grey area, respectively.
7
1.3 Schematic of presbyopic (i.e. monofocal) eye with clear (top) and
blurred (bottom) retinal image quality for a distant and near object,
respectively.
8
1.4 Optical transfer function of a 4.0 mm pupil with 0, 0.15, 0.30 and
0.60D of defocus. The Nyquist limit imposed by the retinal
photoreceptor sampling frequency is shown for reference.
9
1.5 (a) Well-focused and (b) defocused image of a spoke pattern. 10
1.6 Definition of depth of focus. 12
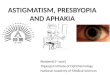
1.7 Curvature-changing accommodating IOL (Source: PowerVision). 15
1.8 (a) Crystalens accommodating IOL. Intended axial movement of the
Crystalens illustrated in (b) and (c) in the eye’s unaccommodated and
accommodated state, respectively.
16
1.9 (a) Schematic eye with ray bundle from a distant object for large and
small pupils. Through-focus blur circles are shown for comparison.
(b) Through-focus point spread functions with 6, 4 and 2mm pupil
diameters. (c) Through-focus normalized retinal image quality in
monochromatic light (550nm) of an aberration-free eye with various
pupil sizes.
18
1.10 Wavefront aberration maps and ray diagrams of (a) monofocal, (b)
refractive bifocal, and (c) spherical aberration wavefronts.
20
1.11 Monocular and binocular contrast sensitivity functions adapted from
Campbell and Green (1965). The upper panel shows the binocular
summation factor of approximately sqrt(2) (defined as the ratio of
22

xvii
binocular to monocular visual performance).
1.12 Example of stereopsis. Cross-fusing the two images leads to a
perception of depth.
23
1.13 Stereoacuity as a function of monocular blur (Lovasik and Szymkiw,
1985).
23
1.14 Illustration of binocular rivalry. Image courtesy of Dieter and Tadin
(2011).
25
1.15 Campbell and Green’s measurement of total and neural contrast
sensitivity functions. The modulation transfer function was computed
by the ratio of neural to total contrast sensitivity.
28
1.16 Improvement in Vernier acuity in adult amblyopia from Levi et al.. 29
1.17 Pre- and post-training contrast sensitivity (y-axis) in the presence of
external noise (x-axis). Image adapted from Dosher and Lu (1999).
30
1.18 Normalized improvement in contrast sensitivity in amblyopic (left
panel) and normal (right panel) subjects from Huang et al.. Vertical
arrows indicate training frequency.
31
2.1 Theoretical approximation of induced accommodation of a single-
optic accommodation IOL.
37
2.2 Accommodative triad: (a) mechanism of ocular power change as
drawn by Helmholtz, (b) pupil constriction data from Alpern et al.
(1961) and (c) convergence to maintain binocular fusion on distal and
proximal objects.
40
2.3 Schematic layout of the natural-view wavefront sensor. 42
2.4 Example images from the Shack-Hartman wavefront sensor and the
pupil cameras for the right and left eyes (OD and OS, respectively).
IPD: interpupillary distance; PD: pupil diameter.
43
2.5 Illustration of through-focus retinal image quality for an eye
accommodating to a visual stimulus at an object distance of 1.5 D.
The amplitude of accommodation was defined as the dioptric location
of peak retinal image quality, or best focus. The accommodative error
was defined as the difference between the object distance and the
44

xviii
dioptric location of best focus.
2.6 (a) Change in convergence angle and (b) absolute pupil size as a
function of target distance.
47
2.7 Accommodative response in young, normal and Crystalens groups. 48
2.8 Through-focus retinal image quality of an Crystalens accommodating
IOL subject with a positive shift in best focus, denoted by the arrows
at the abscissa.
49
2.9 Measure of accommodative amplitude in a Crystalens patient based
on best-focus (blue) and Zernike defocus (red). The gray curve
represents the ideal magnitude of accommodation. Asterisks denote a
statistically significant difference between the two accommodation
measure methods (p<0.05, Student’s t-test, unpaired).
50
3.1 Schematic of adaptive optics IOL metrology optical bench
(CCD=charge-coupled device), from Zheleznyak et al..
55
3.2 Illustration of the correlation-coefficient image quality metric. The
reference column depicts an unaberrated reference image. The
sample column depicts images with ideal, or degraded images of the
model eye.
58
3.3 Through-focus retinal images of the model eye with 4 different IOLs.
Images were collected using a 5.0 mm pupil and an aberration-free
cornea. The letters in the resolution target (from top to bottom rows)
correspond to 20/40, 20/30, 20/25, 20/20 and 20/15 Snellen letters.
60
3.4 Through-focus retinal image quality of presbyopia-correcting IOLs
with an aberration-free cornea. The solid and dotted lines correspond
to 3.0 and 5.0 mm pupils.
61
3.5 Distance image quality with a 3.0mm pupil as a function of corneal
astigmatism.
62
3.6 Through-focus retinal image quality in the presence of corneal
astigmatism for 3.0 and 5.0 mm pupils (left and right panels,
respectively).
64
3.7 Depth of focus in the presence of corneal astigmatism for 3.0 and 5.0 65

xix
mm pupils (left and right panels, respectively).
3.8 Through-focus retinal image quality in the presence of corneal higher
order aberrations for 3.0 and 5.0 mm pupils (left and right panels,
respectively).
66
3.9 Distance image quality (CC) for a 5.0 mm pupil as a function of
corneal higher order RMS.
67
4.1 Illustration of wavefront aberrations and a convolved letter E for
various magnitudes of spherical aberration and defocus. Combining
spherical aberration and defocus yielded the sharpest image, despite
the largest wavefront RMS.
72
4.2 Illustration of the computational steps of the ICM. 76
4.3 (a) Radially averaged power spectra and (b) through-focus image
quality for three distinct reference images: a 20/20 Snellen E (red
line), a letter chart with letters ranging in size from 20/40to 20/15
(blue line) and a natural scene (gray line).
77
4.4 Convolved images of a 20/40 Snellen E with 0, +0.2 and +0.4 µm of
primary spherical aberration from -3 to +3 diopters of defocus for a
4.0 mm pupil.
80
4.5 (a) Through-focus retinal image quality given by the image
convolution metric (ICM) for 0, +0.2 and +0.4 µm of Zernike
primary spherical aberration for a 4.0 mm pupil. (b) Corresponding
average monocular through-focus visual acuity measured in 3
cyclopleged subjects. Error bars represent one standard deviation.
81
4.6 (a) Wavefront RMS, (b) logarithm of VSOTF and (c) ICM plotted as
a function of visual acuity for all subjects and optical conditions.
82
4.7 (a) Snellen letter chart and cameraman images and (b) power spectra
with various slope filters (s). (c) Correlation of visual acuity with
ICM computed with various slope filters.
84
4.8 Illustrative ray diagram of Seidel and Zernike spherical aberrations. 88
4.9 Ray diagram of an aberration-free lens, and a lenses with negative
Zernike primary spherical aberration and negative Zernike secondary
89

xx
spherical aberration.
4.10 Wavefront aberration maps and their cross-sectional profile (black-
lines) for (a) an aberration-free 4.0 mm pupil and pupil with +0.25
µm of (b) Zernike defocus, (c) primary spherical aberration and (d)
secondary spherical aberration.
90
4.11 Through-focus retinal image quality for a 4.0 mm pupil with various
wavefront aberrations.
91
4.12 Through-focus retinal image quality for a 4.0 mm pupil with (a)
primary and (b) secondary spherical aberration. (c) and (d)
correspond to through-focus retinal image quality with primary and
secondary spherical aberrations, respectively, with the peak shifted to
0 diopters.
92
4.13 Two-dimensional distribution of (a) peak retinal image quality and
(b) area-under-through-focus image quality, from 0.0 to 2.5 D, with
primary and secondary spherical aberrations.
94
4.14 (a) Theoretical through-focus retinal image quality and (b) convolved
20/40 Snellen letters for optimal magnitudes and combination of
primary and secondary spherical aberrations.
95
4.15 Through-focus monocular visual acuity measured in 3 cyclopleged
subjects.
96
4.16 (a) Wavefront height and (b) refractive power distribution of the
aberration profiles tested for presbyopic correction.
99
4.17 Intensity transmission profiles with varying degrees of apodization
within a 4.0 mm pupil.
102
4.18 Theoretical retinal image quality at (a) far, (b) intermediate and (c)
near object distances.
103
4.19 Through-focus retinal image quality with (a) 0, (b) +0.2 and (c) -0.2
µm of primary spherical aberration. (d) Through-focus visual benefit
of apodization.
105
4.20 Schematic of vision simulator. 107
4.21 (a) Cross-sectional profile of theoretical and experimental reflectance 108

xxi
profile of spatial light modulator surface. (b) Correlation between
spatial light modulator input and output.
4.22 Average through-focus visual acuity for 3 subjects with (a) 0, (b)
+0.2 and (c) -0.2 µm of primary spherical aberration with (red curve,
α=0.3mm-2) and without (blue curve, α=0.3mm-2) pupil transmission
apodization. Through-focus visual benefit, defined as the difference
in acuity for with and without apodization conditions is shown in (d).
Error bars signify one standard deviation.
109
4.23 Modulation transfer functions of 1.0 D of defocus with (red) and
without (blue) pupil apodization). Arrows indicate the first phase
reversals for apodization conditions.
112
5.1 Monocular through-focus retinal image quality in traditional
monovision.
115
5.2 Binocular contrast summation at 6 cyc/deg as a function of
anisometropia (Pardhan and Gilchrist, 1990).
116
5.3 Theoretical simulation of retinal image quality. (a) and (b) show
monocular through-focus retinal image quality in traditional (TMV)
and modified monovision (MMV) with +0.2 and +0.4 µm of primary
spherical aberration in the non-dominant eye, respectively. (c)
Binocular through-focus retinal image quality. (d) Interocular
difference in through-focus retinal image quality; (c) and (d) share a
common legend.
120
5.4 Binocular adaptive optics vision simulator schematic. LE: left eye;
RE: right eye; TS: translational stage for interpupillary distance;
LED: infrared light emitting diodes for pupil illumination; PC: pupil
camera for subject alignment; PH: 800 µm diameter pinhole; SLD:
super-luminescent diode (λ = 840+20 nm); PHR: phoropter; FL:
fusion lock; DM: deformable mirror; BO: Badal optometer; DF:
dichroic filter; SHWS: custom-made Shack-Hartmann wavefront
sensor; AP: artificial pupil; DLP: digital light processor; L1 and L2:
200 mm focal length achromatic doublet lenses; L3 and L6: 150 mm
123

xxii
focal length achromatic doublet lenses; L4 and L5: 350 mm focal
length achromatic doublet lenses; L7: 180 mm focal length
achromatic doublet lens.
5.5 (a) Left and right eye system wavefront sensors’ measurement of +/-
4 D of defocus induced by the Badal optometers and (b) the residual
error.
125
5.6 Various pupil sizes (colored circles) overlaid with the deformable
mirror’s 97 actuators (grey boxes).
126
5.7 (a) Time-course change in wavefront root mean square (RMS) over a
4.0 mm pupil for both eyes before and after adaptive optics
correction. Wavefront maps for both eyes before and after correction
are shown in (b) and (c), respectively.
128
5.8 Ideal, measured, and wavefront error maps in right and left eyes for
modified monovision over a 4.0 mm pupil.
129
5.9 (a) Through-focus binocular contrast sensitivity for traditional and
modified monovision with +0.2 µm of spherical aberration and (b)
the corresponding through-focus binocular summation factor. (c)
Through-focus binocular MTF at 10 cyc/deg and (d) the
corresponding through-focus binocular summation factor estimated
using the Quadratic summation model (equation 5.1).
133
5.10 Through-focus binocular visual acuity for traditional (TMV) and
modified monovision (MMV) with (a) +0.2 µm and (b) +0.4 µm of
primary spherical aberration induced in the non-dominant eye. The
gray dashed line represents the depth of focus threshold.
135
5.11 (a) Through-focus monocular (DE: dominant eye; NDE: non-
dominant eye) and binocular visual acuity for the modified
monovision conditions with +0.2 µm spherical aberration. (b)
Binocular visual acuity (VA) plotted as a function of monocular
visual acuity of the better eye for each object distance for traditional
and modified monovisions with positive spherical aberration. The
black solid line represents the equal acuity line.
136

xxiii
5.12 Binocular visual acuity versus theoretically calculated binocular
retinal image quality, computed using the image convolution metric.
Black circle: traditional monovision, red square: MMV (SA = +0.2
µm), green square: MMV (SA = -0.2 µm), blue diamond: MMV (SA
= +0.4 µm), orange diamond: MMV (SA = -0.4 µm). The black line
represents the best-fit linear regression.
138
5.13 (a) Overall binocular image quality as a function of overall
interocular difference in image quality for all modified monovision
(MMV) designs (gray diamonds). Traditional monovision (TMV) for
1.5 D anisometropia is represented by the large black diamond. TMV
with remaining anisometropia is represented by the small black
diamonds. Modified monovision designs were grouped by degree of
(b) anisometropia, (c) dominant eye spherical aberration and (d) non-
dominant eye spherical aberration. Error bars represent the standard
deviation within each group of designs. Bold black arrows indicate
the impact of the magnitude of increasing anisometropia or spherical
aberration.
141
5.14 (a) Through-focus retinal image quality and (b) interocular difference
in through-focus retinal image quality. (c) Overall binocular image
quality versus overall interocular difference in image quality.
143
5.15 Through-focus (a) binocular image quality and (b) interocular
difference in image quality for traditional (black) and modified
(green) monovision. (c) Through-visual acuity and (b) stereoacuity.
Asterisks denote a statistically significant difference between
modified and traditional monovision (p<0.05, paired Student’s t-test).
145
6.1 (a) Haploscope schematic diagram. (b) Visual stimulus for left and
right eyes presented by the LCD display.
153
6.2 Portion of time spent viewing right eye stimulus as a function of right
eye contrast for one subject. In this example, this subject had an
ocular dominance score of 0.7 (35% divided by 50% contrast in the
right and left eyes, respectively, for equivalent viewing duration.
154

xxiv
6.3 (a) Histogram and (b) plot of degree of sensory eye dominance in 12
subjects. A degree of dominance value of unity indicates no
dominance. Below and above unity signifies right and left eye
dominance, respectively. The gray band of weak dominance spans
+10% about unity.
155
6.4 Average through-focus visual acuity with (a) modified and (b)
traditional monovision. Blue data corresponds to condition with
dominant eye assigned to distance for 9 subjects. Red data
corresponds to the non-dominant eye assigned to distance. (c)
Average visual acuity difference between eye assignment paradigms
in modified (black empty circles) and traditional (gray filled
diamonds) monovision as a function of subjects’ dominance.
157
6.5 Average through-focus contrast sensitivity with (a) modified and (b)
traditional monovision. Blue data corresponds to condition with
dominant eye assigned to distance for 3 subjects. Red data
corresponds to the non-dominant eye assigned to distance. Asterisks
denote a statistically significant difference (p<0.05, Student’s paired
t-test). (c) Average percent change in contrast sensitivity between eye
assignment paradigms in modified (black empty circles) and
traditional (gray filled diamonds) monovision as a function of
subjects’ dominance.
159
6.6 Through-focus monocular retinal image quality in (a) modified and
(b) traditional monovision. Solid and dashed lines represent dominant
and non-dominant eyes, respectively. (c) Binocular through-focus
retinal image quality. (d) Interocular difference in retinal image
quality. For (c) and (d), solid and dotted lines represent modified and
traditional monovision, respectively.
167
6.7 Pre-training CSFs for all subjects and spatial frequencies at 0.0 (left
column) and 1.5 D (right column). Modified monovision (MMV) is
shown in the two upper rows (a-d) and traditional monovision (TMV)
is shown in the bottom row (e, f).
169

xxv
6.8 Determination of training frequency, indicated by vertical arrow.
Dashed line represents 50% of peak contrast sensitivity. Red arrow
represents training spatial frequency.
170
6.9 Learning curves for modified (a and b) and (c) traditional monovision
subjects. Red and blue data corresponds to learning curves at 0.0 and
1.5 D.
173
6.10 Pre- and post-training CSFs (blue and red, date respectively) for all
subjects and at 0.0 (left column) and 1.5 D (right column). Modified
monovision (MMV) is shown in the two upper rows (a-d) and
traditional monovision (TMV) is shown in the bottom row (e, f).
Training frequencies are indicated with black arrows for each
condition.
175
6.11 Pre- (blue) and post-training (red) through-focus visual acuity in (a,
b) modified and (c) traditional monovision.
177
6.12 Average visual benefit at 0.0 and 1.5 D for modified (red) and
traditional (blue) monovision.
179
6.13 Visual benefit in through-focus visual acuity in modified (red) and
traditional (blue) monovision.
180

1
Chapter 1. Introduction
1.1 Background and Significance
The need to change focus from far to near objects and vice versa in everyday life
is ubiquitous. While crossing the street, a person uses far vision to check for oncoming
traffic and read street signs. Alternatively, reading fine-detail on a road-map or checking
a wrist watch requires near vision. This ability to dynamically change the eyes’ optical
power to bring distant and near objects into focus, a robust facility of the human visual
system, is known as accommodation.
The mechanism of accommodation had puzzled scientists and ophthalmologists
for centuries, until 1801, when Thomas Young reported shape changes of the crystalline
lens due to accommodation1. Thus, the foundation was laid for Hermann Von Helmholtz’
seminal work2 on physiological optics approximately 50 years later. Helmholtz observed
the specular reflections of a candle flame from the optical surfaces of the eye to deduce
that the changes in curvature, thickness and position of the crystalline lens were
responsible for the eye’s ability to change focus.
As the eye ages, the crystalline lens undergoes changes which reduce its ability to
accommodate. From childhood, the crystalline lens gradually increases in size3, 4,
decreases in elasticity5 and becomes opaque6 with the eventual formation of cataract. By
the age of approximately 50 years7, accommodative ability is entirely lost due to lens
growth and stiffening, indicating the onset of presbyopia8.

2
Presbyopia, the age-related loss of accommodation, is associated with a
significant decrease in the quality of life9. Furthermore, as the population ages,
presbyopia will have an increasing impact, as it affects 100% of the population over the
age of 50 years. The correction of presbyopia entails the restoration of clear near vision.
Currently available options for correcting presbyopia span in complexity from Benjamin
Franklin’s invention of the bifocal spectacles to the sophisticated biomechanical and
optical designs of prosthetic intraocular lenses.
Presbyopia corrections generally fall into one of two categories: pseudophakic-
accommodation and pseudoaccommodation. Pseudophakic-accommodation refers to a
true restoration of the eye’s dynamic accommodative ability. This has been attempted
with various methods, such as replacing the aged, presbyopic crystalline lens with an
elastic polymer gel10, 11 or prosthetic accommodating intraocular lenses designed to
change curvature12, geometry13, 14 or position15, 16 within the eye. Such lenses are
typically implanted at the time of cataract surgery, when the crystalline lens is being
replaced due to opacification. Despite various approaches either currently in use or in
clinical trials, no true restoration of accommodation is currently available.
On the other hand, pseudoaccommodation refers to a static extension of eye’s the
depth of focus. Pseudoaccommodation has been implemented with numerous modalities,
ranging from non-invasive multifocal contact lenses to surgical approaches such as small-
aperture corneal inlays, refractive surgery for the reshaping of the anterior cornea and
multifocal intraocular lenses. While these techniques have been shown to improve
distance-corrected near vision, they also lead to visual side-effects such as reduced

3
contrast, halos and glare. An inherent trade-off to increasing the eye’s depth of focus is a
sacrifice in peak image quality.
Ensuring patient satisfaction with presbyopia-correcting lenses ultimately depends
on the ability to predict visual performance from optical theory. Optical modeling of
retinal image quality has been an active area of research for decades, however, has been
faced with limitations. For example, sharpness and contrast are traits of image quality
which may not be fully represented by a single-value image quality metric. Furthermore,
various visual tasks, such as high-contrast visual acuity or contrast sensitivity may rely on
different aspects of image statistics (e.g. frequency bandwidth and contrast).
Robust retinal image quality metrics allow for accurate prediction of through-
focus optical quality and visual performance. In this thesis, we employ such a metric, and
apply it to the design of presbyopic corrections. Thereby enabling optimization of the
trade-off between peak image quality and depth of focus.
In addition to the optical properties of the eye and the image formed on the retina,
the neural visual system plays a key role in determining visual perception and
performance. For example, the visual system’s ability to combine two monocular
channels into a single binocular perception will be examined in-depth herein as a
potential avenue towards presbyopic correction. In addition, the visual system is capable
of adapting to optical aberrations to reduce side-effects of multifocal lenses17. Moreover,
neural plasticity may be facilitated by perceptual learning (i.e. vision training) to further
improve presbyopic visual performance18.
The first goal of this thesis was to gain an understanding of the limitations of
currently available techniques for correcting presbyopia. Specifically, objective methods

4
were developed to quantify the efficacy of premium presbyopia-correcting intraocular
lens. Both accommodating and extended depth of focus intraocular lenses were evaluated
to determine their ability to produce a change in optical power or improve through-focus
retinal image quality.
The second goal of this thesis was aimed at investigating through-focus visual
performance in the presence of extended depth of focus optical corrections in both
monocular and binocular approaches for correcting presbyopia. The potential of
wavefront interaction was examined for improving through-focus monocular visual
performance with minimal reduction in peak performance. Subsequently, a new binocular
approach is proposed wherein each eye’s refractive state and multifocality was
determined independently so as to capitalize on the dual-channel nature of the binocular
visual system.
The third goal of this thesis was to investigate the potential of improving
through-focus visual performance by combining neural plasticity in the form of
perceptual learning with optimal optical conditions for presbyopic correction. Perceptual
learning refers to a vision training regimen in which patient’s visual performance is
improved by reducing neural noise and increasing neural gain of spatial frequency
channels of the visual pathway19.
The present chapter will review basic concepts to establish a background for the
remainder of this thesis. A broad overview of the mechanism of accommodation and its
age-related decline is described with classical and recent literature. Strategies for
correcting presbyopia will be summarized, in addition to a description of optical factors,
namely diffraction and the wavefront aberrations, which determine through-focus retinal

5
image quality and therefore presbyopic visual performance for various object distances.
Neural factors determining presbyopic visual performance, such as ocular dominance and
neural plasticity will also be reviewed. Finally, we will outline the subsequent chapters of
the thesis.
1.2 Physiology of Accommodation and Presbyopia
The study of the accommodative mechanism has a rich history dating back at least
to the Johannes Kepler’s proposal of axial movement of the crystalline lens20 (schematic
diagram of the eye is shown in Figure 1.1). However, it was Helmholtz in 1855, over 200
years after Kepler’s Dioptrice, who published his famous Treatise on Physiological
Optics2, 21
in which he quantified the eye’s physiological transformations associated with
accommodation.
As described in his treatise, Helmholtz observed the four Purkinje images, or
specular reflections of a candle flame from the corneal and lens anterior and posterior
surfaces of his research subject. As his subject exerted accommodative effort, Helmholtz
witnessed a change in position and size in the reflections corresponding to the crystalline
lens, while the corneal reflections did not change in any way. Helmholtz concluded that
the lens was solely responsible for accommodation, via a mechanism of axial movement
and shape change (thickness and curvature). His theory of accommodation states that
when an eye is focused at a distant object, the ciliary muscles are contracted, flattening
the crystalline lens via zonular fiber tension. As the eye accommodates to a near object,
the ciliary muscles constrict, releasing the tension of the zonular fibers, allowing the
crystalline lens to thicken and its surfaces to increase in curvature. Helmholtz’s model for

6
accommodation has been verified experimentally with high-resolution magnetic
resonance imaging3, Scheimpflug imaging22 and optical coherence tomography23.
Figure 1.1. Schematic diagram of the eye.
As the eye accommodates, pupil size decreases, the two eyes converge to
maintain binocular fusion, and the eyes’ optical power is increased due to the
aforementioned alterations of the crystalline lens. These three processes are commonly
referred to as the accommodative triad, and work together to form a binocularly stable,
clear percept.
The magnitude of accommodation may be defined as the degree of available
dioptric change of the eye’s power24. As shown first by Donders in 1864, and later by
Duane in 19127 (see Figure 1.2 below), the available magnitude of accommodation
gradually decreases, starting at an early age until a plateau is reached at around 50 years.

7
Figure 1.2. Subjectively measured amplitude of accommodation (adapted from Duane, 19127). Average and upper and lower limits are indicated by black line and grey area, respectively.
The age-related loss of accommodation, or presbyopia, is caused by several
biomechanical factors. For example, lifelong crystalline lens growth3, 4 and the loss of
elasticity5 contribute to the onset of presbyopia. Interestingly, the ciliary muscles
maintain functionality in advanced age, despite their inability to conform the crystalline
lens. Ciliary muscle activity in presbyopes has been observed by Strenk et al.25 using
magnetic resonance imaging, confirming the lens’s primary role in presbyopia.
1.3 Impact of Presbyopia on Retinal Image Quality
An emmetropic (i.e. distance-corrected) presbyopic eye that is unable to
accommodate is akin to a monofocal optical system with its object plane at infinity. The

8
top panel of Figure 1.3 illustrates an eye forming a sharp image of a distant object on the
retina. The bottom panel of Figure 1.3 illustrates the problem of the presbyopic eye
unable to refocus a near object resulting in a blur at the retina. Object distance is typically
described in units of diopters (D, inverse meters). Therefore, 0 D refers to an infinitely
distant object and 3 D (or 33.3 cm) to approximately reading distance.
Figure 1.3. Schematic of presbyopic (i.e. monofocal) eye with clear (top) and blurred (bottom) retinal image quality for a distant and near object, respectively.
The impact of defocus on the optical transfer function (OTF) is shown in Figure
1.4. The OTF provides information pertaining to the contrast and spatial phase of spatial
frequencies in an image. In this case, four OTF curves are shown: the black curve
represents the aberration-free case, followed by various magnitudes of defocus (colored
curves). As the magnitude of defocus increases from 0.00 to 0.15 D, the contrast, or

9
modulation, of all spatial frequencies is attenuated. However, as defocus further increases
to 0.30 and 0.60 D, the curves intersect the x-axis, where the negative OTF values
indicate a phase reversal.
Figure 1.4. (a) Optical transfer functions of a 4.0 mm pupil with 0, 0.15, 0.30 and 0.60D of defocus. The Nyquist limit imposed by the retinal photoreceptor sampling frequency is shown for reference.
Figure 1.5 qualitatively illustrates the impact of defocus upon a retinal image of a
spoke pattern. In Figure 1.5a, the spoke pattern is well-focused. However, as shown in
Figure 1.5b, the defocused spoke pattern suffers from low contrast and phase reversals at
higher spatial frequencies (toward the center of the spoke pattern).

10
Figure 1.5. (a) Well-focused and (b) defocused image of a spoke pattern.
Due to the degradation in retinal image quality imposed by optical defocus,
presbyopic visual performance is confined to a narrow range of object distances, limited
by the eye’s depth of focus. The eye’s depth of focus is an extensively studied concept in
vision science with significant clinical implications for presbyopia correction, in addition
to assessing and correcting refractive error. Broadly speaking, the depth of focus is the
dioptric range over which retinal image quality does not deteriorate to an objectionable
degree, i.e. the optical tolerance to blur. This range is influenced by characteristics of the
stimulus (size, spatial frequency content, luminance, and color) and the observer (pupil
size and wavefront aberrations).
Objective measures of depth of focus are intended to avoid subjective perception
of blur. Depth of focus may be objectively determined either computationally, by
calculating an image quality metric for a range of object distances (i.e. through-focus), or
psychophysically by measuring through-focus visual performance. In the field of optical
engineering, depth of focus is typically measured on both sides of best focus, such as the

11
full-width half-maximum of a merit function. However, in the field of visual optics, best
focus is typically optimized for distant objects at 0D. In this case, only positive defocus
values correspond to physical objects, or those with a distance less than infinity. Likewise,
objects with a negative defocus value correspond to imaginary objects which are non-
physical. Therefore, we adopted the convention of depth of focus measured from distance,
0D, to near, positive defocus values, as illustrated in Figure 1.6.
The performance threshold has a significant impact on depth of focus and is not
standardized in visual science. Previous studies examining through-focus retinal image
quality metrics have employed depth of focus thresholds based on the Rayleigh criterion
(80% reduction)26, 50% reduction in image quality27, or absolute metric values28.
Similarly, in visual performance, there is no consensus on the proper task or threshold
with which to quantify the eye’s depth of focus. Some authors have used visual acuity
(e.g. 20/3028 or 20/4029 criterion), whereas other authors used contrast sensitivity (e.g. 80
or 50%30 reduction criterion) to objectively measure depth of focus. Due to the
inconsistency in definition of depth of focus and wide variability in methodologies,
values reported in the literature vary widely (for detailed review, see Wang and
Ciuffedra31).

12
Figure 1.6. Definition of depth of focus.
As described by Atchison et al.32, the focus range for which a target appears clear
is typically much smaller than the focus range over which a target remains legible. Using
a 4mm artificial pupil, Atchison et al.32 measured the depth of focus, for which high and
mid frequency letters (subtending -0.2 and 0.2 log arc minutes, respectively) remained
clear, to be approximately 0.22 and 0.32D, respectively. Alternatively, Tucker and
Charman33 evaluated letter acuity (i.e. legibility or recognition) for a range of vergences
with a 4mm pupil and found a depth of focus of approximately 1.5D using 0.2 log arc
minutes as an acuity threshold (equivalent to 20/30 Snellen acuity). These values are
representative of those found in other published studies31, 34, 35.

13
1.4 Presbyopia Correction Strategies
Evidence of presbyopic correction can be traced to magnifying lenses known as
“reading stones” developed in the 9th century, CE. In 1250, CE, the English friar Roger
Bacon wrote of optical aides to abet his presbyopia:
“It may be observed that old people hold objects that they wish to examine
further from the eye. …If anyone examines letters or other minute objects
through the medium of crystal or glass or other transparent substance, if it
be shaped like the lesser segment of a sphere, with the convex side being
towards the eye, and the eye being in the air, he will see the letters far
better, and they will seem larger to him. …For this reason, such an
instrument is useful to old persons…”36
Aside from magnifying lenses and spectacles, relatively little progress was made for
presbyopic correction until the 18th century with Benjamin Franklin’s invention of the
bifocal spectacles. By using the upper half of his lens for viewing far objects and the
bottom half of his lens for viewing near objects, Benjamin Franklin’s innovation allowed
him to use one set of spectacles for viewing all distances.
In the last few decades, there has been a tremendous increase in research and
development devoted to presbyopic correction. We will give a brief overview of the chief
strategies developed, listed in Table 1.1.

14
Table 1.1. Methods for correcting presbyopia.
1.4.1 Pseudophakic Accommodation
To increase the range of vision beyond the eye’s depth of focus, there has been a
large effort in the past twenty years to restore the eye’s dynamic ability to accommodate37,
38. One such approach is lens capsule refilling, or “phaco-ersatz”, wherein the presbyopic
crystalline lens is removed from the capsular bag and subsequently injected with an
adaptable soft polymer gel10, 11 or a fluid-filled balloon39. The elastic polymer gel in the
capsular bag is intended to enable lens shape changes with accommodative effort of the
ciliary body. However, despite decades of research10, 11, 39, 40, investigators have not
managed to overcome the issues associated with lens refilling. The main limitations of
lens refilling have been leakage of the refilling material from the capsular bag,
opacification of the capsular bag due to proliferation of endothelial cells (also known as

15
secondary cataract), volume control to achieve the target refraction and induction of
aberrations leading to poor optical quality11.
A well-established approach is the use of so-called accommodating IOLs, which
are designed to change surface curvature or axially shift position within the eye with
accommodative effort. A curvature-change design under development is the Powervision
(Belmont, CA) FluidVision IOL, which is comprised of a hollow lens and liquid-filled
reservoir haptics (shown in Figure 1.7). When the eye is in its relaxed state, the liquid
resides within the haptics and the lens rests in a relatively flat shape, defining the
geometry for viewing distant objects. As the eye exerts accommodative effort, the ciliary
muscle contracts, decreasing the equatorial diameter of the capsular bag. This forces the
fluid from the haptic reservoir into the central lens cavity, increasing its curvature and
optical power, thereby providing near vision41.
Figure 1.7. Curvature-changing accommodating IOL (Source: PowerVision).
Accommodative IOL designs based on axial movement are further along in
development and more widespread in clinical use. One such lens is approved for use by

16
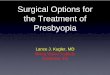
the United States Food and Drug Administration (FDA): the Crystalens accommodating
IOL (Bausch & Lomb, Rochester, NY). The Crystalens is a single-optic IOL mounted on
hinged haptics, as shown in Figure 1.8a. Surgical implantation follows a procedure
similar to conventional IOLs, being placed within the capsular bag. As the ciliary muscle
constricts with accommodative effort, the hinged haptics allow the lens to shift axially
toward the cornea, thereby reducing the anterior chamber depth (illustrated in Figures
1.8b and c).
Figure 1.8. (a) Crystalens accommodating IOL. Intended axial movement of the Crystalens illustrated in (b) and (c) in the eye’s unaccommodated and accommodated state, respectively.
In an theoretical analysis of accommodating IOLs, Hunter et al.42 showed that a
1mm axial shift of a 20D IOL (a common power) induces an optical change of
approximately 1.2D. Therefore, a single-optic accommodating IOL model must travel an
unreasonable distance through the anterior chamber to result in a meaningful amplitude
of accommodation. For example, to accommodate to a near target at reading distance
(3D), a single-optic accommodating IOL would have to travel roughly 3.6mm, traversing
approximately 80% of the anterior chamber.

17
To overcome this limitation, other designs have been proposed. The Synchrony
IOL (Abbott Medical Optics) is an accommodating IOL with two optical elements
connected with a spring mechanism. McLeod et al.13 determined the dual-optic design
results in a 2.2D increase in power with a 1mm axial movement of the anterior lens.
Despite this improvement in movement-to-power-change ratio over the single-optic
accommodation IOL, the dual-optic design has not led to a clinical benefit. In a recent
clinical study comparing two groups of patients with either single- or dual-optic
accommodating lenses, Alio et al.15 found no significant difference in through-focus
visual acuity between the groups. This may be due to a hindrance in IOL movement
caused by the wound healing response of capsular bag fibrosis and stiffening following
IOL implantation43.
1.4.2 Increasing the Eye’s Depth of Focus
Until a true restoration of accommodation is within reach, extending the eye’s
depth of focus has been a common path taken by clinicians to alleviate the symptoms of
presbyopia. The eye’s depth of focus may be increased by reducing the pupil diameter or
by inducing a multifocality to the wavefront aberrations by aspherizing a refractive
surface, using a diffractive optical element, or both.
Reducing the pupil size of the eye is the easiest way to lessen the impact of
presbyopic blur. For example, eyelid squinting is a common means of truncating the
pupil, albeit only vertically, to improve acuity in the presence of refractive error44. Pupil
size also effects aberration-free image quality at 0D of defocus. The cutoff frequency of
the modulation transfer function (MTF) is linearly dependent upon the pupil size.

18
Therefore, as pupil size decreases, so does the cutoff frequency of the MTF and the
spatial bandwidth of the image, thereby degrading distance image quality. Retinal
illuminance also poses a limitation for use of bilateral pinhole apertures for presbyopic
correction.
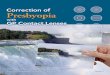
Figure 1.9. (a) Schematic eye with ray bundle from a distant object for large and small pupils. Through-focus blur circles are shown for comparison. (b) Through-focus point

19
spread functions with 6, 4 and 2mm pupil diameters. (c) Through-focus normalized retinal image quality in monochromatic light (550nm) of an aberration-free eye with various pupil sizes.
The small-aperture approach has found some clinical use recently in the form of a
pinhole corneal inlay45, 46 (KAMRA, AcuFocus). The inlay consists of a 10µm thick disk
with an outer diameter of 3.6mm and a central aperture diameter of 1.6mm implanted
within the stroma of the cornea. Despite the improvement in retinal image quality for
near objects, the inlay may only be used unilaterally, due to the reduction in retinal
illuminance of the implanted eye.
The other method for increasing the depth of focus is to manipulate the wavefront
aberrations of the eye. A wavefront is defined as a surface of constant phase, where phase
refers to the electromagnetic field at the pupil plane of the eye. From a ray-optics
perspective, a wavefront may be conceptualized as the surface which is perpendicular to
the rays passing through it. Therefore, a spherical wavefront, illustrated below in Figure
1.10a, produces rays concentric about the center of curvature of the wavefront. The
circular color map represents the wavefront aberration, or departure from a reference
sphere. Ignoring diffraction, a spherical wavefront yields an infinitely small focus spot.
Aspherizing the wavefront by inducing aberrations (i.e. departure from a sphere),
such as discrete zones of refractive power or a continuous profiles such as spherical
aberration (Figures 1.10b and c, respectively), results in portions of the pupil allocated to
imaging a specified object distance on the retina.

20
Figure 1.10. Wavefront aberration maps and ray diagrams of (a) monofocal, (b) refractive bifocal, and (c) spherical aberration wavefronts.
As can be seen from the ray diagrams in Figure 1.10b and c, inducing
multifocality increases the size of the ray bundle at best focus, degrading peak image
quality. The inherent trade-off between depth of focus and peak retinal image quality is
central to the design and optimization of effective presbyopic corrections. Retinal image
quality metrics’ ability to predict visual performance in the presence of large magnitudes
of aberrations will be addressed in detail in this thesis.

21
1.5 Binocular Vision and Presbyopia
When considering retinal image quality in relation to visual performance, it is also
important not to overlook the binocular nature of the visual system. The benefits of
having two eyes are many and diverse. The advantages of binocular vision range from an
increased field of view to enhanced resolution, detection of contrast and depth perception.
An immediate advantage to binocularity is an increase in horizontal field of view. Normal
human monocular field of view is 100 degrees, however binocularly the field of view
increases to 170 degrees47. In the central area of overlap, the eyes’ fused retinal images
are combined in the brain’s neural processing of the lateral geniculate nucleus (LGN) and
visual cortex.
In 1965, Campbell and Green published their seminal work on the binocular
advantage to spatial vision48. They found that binocular contrast sensitivity was on
average a factor of √2 higher than monocular contrast sensitivity (Figure 1.11). In their
experiment, the subjects were exposed to nearly diffraction-limited viewing due to the
use of small (2.8mm) artificial pupils. Campbell and Green explained their results using
signal theory, wherein the signal-to-noise ratio of a system (with detectors with
uncorrelated Poisson noise) is proportional to the square-root of the number of detectors.
More recently, Sabesan, Zheleznyak and Yoon49 found that binocular contrast summation
may exceed the classical value of √2 in the presence of subjects’ native higher order
aberrations. Visual acuity on the other hand, a resolution task, undergoes an
approximately 10% improvement due to binocular summation, as shown by the
horizontal shift in cutoff frequency of the contrast sensitivity function50.

22
Figure 1.11. Monocular and binocular contrast sensitivity functions adapted from Campbell and Green (1965). The upper panel shows the binocular summation factor of approximately sqrt(2) (defined as the ratio of binocular to monocular visual performance).
Depth perception, or stereopsis, is another important function of binocular vision.
Because the two eyes are laterally displaced from one another by the interpupillary
distance (typically between 50 and 80mm51), the two eyes’ retinal images are slightly
different, or “disparate”, due to their shifted perspective. Retinal disparity leads to the
sensation of depth, as outlined by Filippini and Banks52. In their model, the two retinal
images are locally cross-correlated to determine disparity. The magnitude of an object’s
relative disparity between the eyes is then directly related to its position in depth. Figure
1.12 offers a demonstration of stereopsis. By cross-fusing the left and right images in
Figure 1.12, the red cylinder will appear to be in front of the blue cylinder.

23
Figure 1.12. Example of stereopsis. Cross-fusing the two images leads to a perception of depth.
The limit of stereopsis is set by the visual system’s ability to cross-correlate the
left and right eye images. Therefore, any difference in optical quality between the two
eyes introduces uncertainty to correlation, negatively affecting stereopsis. For example,
interocular differences in luminance, pupil size, blur and magnification have all been
shown to limit stereoacuity53-55, as they reduce the similarity between the retinal images.
Figure 1.13 below illustrates the significant degradation in stereoacuity due to monocular
blur published by Lovasik and Szymkiw53.
Figure 1.13. Stereoacuity as a function of monocular blur (Lovasik and Szymkiw, 1985).

24
In the case of presbyopia, inducing a difference in retinal image quality between
the eyes can be advantageous. For example, monovision capitalizes on the binocular
nature of the human visual system by inducing a near-add power, or anisometropia, to the
non-dominant eye. The anisometropia requires binocular suppression56 to disregard the
defocused eye for viewing at a particular distance with the in-focus eye. Therefore, for
distance vision, the dominant eye is used, whereas for near vision, the non-dominant eye
is used. Several studies57-59 have shown that binocular visual acuity (VA) in monovision
is approximately determined by the monocular acuity of eye with superior optical quality.
The difference in refraction between the two eyes is typically in the range of 1-2
D. However, the optimal magnitude of anisometropia may differ by the individual. For
example, a presbyopic patient with relatively small pupils may be able to tolerate a larger
anisometropia (due to extended depth of focus) as compared to a presbyopic patient with
larger pupils. The level of ocular dominance, a neural attribute, has also been shown to
impact the success of monovision in patients60. For these reasons, the optimal degree of
anisometropia remains a debated topic within clinical ophthalmology.
1.6 Neural Aspects to Presbyopic Correction
1.6.1 Ocular Dominance
Ocular dominance, or eye dominance, refers to a predisposition to visual
information from one eye over the other. For example, if the two eyes are presented with
incompatible images, such as orthogonal gratings, observers typically report
spontaneously alternating percepts between the two monocular images, lasting on the

25
order of several seconds61, 62. This condition is known as binocular rivalry, and is
illustrated in Figure 1.14. If one eye is dominant over the fellow eye, its retinal image
will be perceived a larger portion of the time during rivalry, whereas the non-dominant
eye will be suppressed60.
Figure 1.14. Illustration of binocular rivalry. Image courtesy of Dieter and Tadin (2011)62.
Ocular dominance may be classified into two categories: sighting and sensory
dominance. Sighting dominance may be determined by requiring the subject to choose
their dominant eye using a motor task, such as the “hole-in-card” test63. In this test, the
subject gazes at a distant target through a hand-held card with a hole. Despite binocular
viewing, by occluding one eye, the sighting dominant eye is determined as the one
aligned with the target. Methods such as the hold-in-card test are common in clinical
settings due to their simplicity and ease of administration.
By design, such tests are binary, in that their outcome is either left or right eye
dominance. Sensory dominance tests, on the other hand, offer a finer, more robust
measure of ocular dominance and in some cases are able to quantify the degree of
dominance63. Sensory dominance tests measure the balance of sensory input between the

26
eyes using binocular rivalry targets60, 64 or stereo-disparate objects65 to measure the
magnitude of ocular dominance.
Clinically, ocular dominance for eye assignment in monovision is typically
assessed with sighting tests, after which the dominant eye is assigned to distance vision
and the non-dominant eye is assigned to near vision66. This practice is based on the
assumption that patients have a greater need for distance vision as compared to near, and
that suppression is more easily achieved in the non-dominant eye. However, sighting
dominance has been shown to have a poor correlation with patient satisfaction in
monovision63. This may be due to the fact that sighting tasks force subjects to choose one
eye, even in cases of low dominance levels. Therefore, it has been suggested that sensory
dominance tests are more appropriate for differentiating potential from poor monovision
candidates, in addition to eye assignment for distance63. It should be noted as well, that in
the majority of subjects who have a relatively weak degree of dominance, sighting and
sensory dominance are poorly correlated63. Therefore, although sighting tasks offer a
convenient tool in the clinical setting, they may not be appropriate for screening
candidates for monovision treatments.
1.6.2 Neural Plasticity
Spatial vision is limited in performance by neural factors in addition to the optical
quality of the image formed upon the retina. Beyond the discrete sampling of the retinal
image by the photoreceptors (Nyquist sampling limit approximately 60 cyc/deg67, 68), the
nervous system is responsible for the processing which leads to, among others, the
perception of contrast48, 69, orientation70 and color71, 72.

27
Contrast sensitivity, the ability to distinguish small increments in luminance on a
uniform background, is regarded as a fundamental benchmark for spatial vision and a
defining factor for a wide range of visual tasks73. Contrast sensitivity is limited by the
optical transfer function of the eye and the neural contrast sensitivity function of the
nervous system69, 74, 75.
To determine the neural limit of contrast detection, Campbell and Green69, and
later Williams74, employed a method of measuring neural contrast sensitivity while
bypassing the optical transfer function of the eye. This was done by interfering two
coherent laser beams at the retina, producing an interference fringe pattern of variable
spatial frequency and contrast (unattenuated by the eye’s optics). These studies isolated
the nervous system’s role in contrast detection, and quantified the neural transfer function,
as shown in Figure 1.15. One of their main findings was the nervous system’s attenuation
of high spatial frequencies, in a manner similar to the optical transfer function, setting the
ultimate limit for visual performance.

28
Figure 1.15. Campbell and Green’s69 measurement of total and neural contrast sensitivity functions. The modulation transfer function was computed by the ratio of neural to total contrast sensitivity.
Degraded visual performance (e.g. contrast sensitivity) due to optical factors76
such as retinal blur caused by optical aberrations (e.g. presbyopia, ametropia, and higher
order aberrations) are regularly corrected with spectacles, contact lenses, refractive
surgery and intraocular lenses. However, visual deficits due to neural factors, such as
amblyopia77 were long thought to be untreatable in the adult visual system78.
Recent studies have shown evidence of neural plasticity in adults, introducing a
new frontier in vision correction. In 1963, Eleanor Gibson79 defined perceptual learning
as “any relatively permanent and consistent change in the perception of a stimulus array
following practice or experience with this array…”. Perceptual learning is realized via
extensively repetitive practice on a demanding visual task. In the following decades,
perceptual learning has become an active field of vision research with both clinical and

29
scientific implications. A wide variety of visual tasks have been shown to be improved
with perceptual learning, such as Vernier acuity80, 81, contrast sensitivity82, 83, and
stereopsis80, 84 (see Fine and Jacobs85 for review). Researchers have found that repeated
practice at a visual task led to significant improvements in performance in amblyopic
eyes78, 86 however the improvements tended to be task specific85.
In a study by Levi et al.87, amblyopes underwent a perceptual learning regiment of
repeated practice with Vernier acuity (10 sessions, approximately 1,000 trials per session),
as shown in Figure 1.16. Subjects in their study exhibited on average a 50% improvement
in Vernier acuity in their amblyopic eye, with a lesser, but significant, improvement in
the untrained eye as well. The interocular transfer of learning suggests the neural changes
possibly occur in the visual cortex87, where binocular interactions have been previously
reported88.
Figure 1.16. Improvement in Vernier acuity in adult amblyopia from Levi et al.87.

30
Empirical and theoretical models of perceptual learning, though an
oversimplification, have added understanding of the underlying mechanisms behind
perceptual learning19, 83, 89. Dosher and Lu19 followed a systems analysis approach to
differentiate possible mechanisms for perceptual learning. In their perceptual template
model paradigm, contrast sensitivity was measured in the presence of external noise, as
shown in Figure 1.17.
Figure 1.17. Pre- and post-training contrast sensitivity (y-axis) in the presence of external noise (x-axis). Image adapted from Dosher and Lu (1999)19.
The x-axis denotes the magnitude of external noise added to the stimulus, a Gabor
patch at a fixed spatial frequency (2.3 cyc/deg), the y-axis denotes the contrast threshold
(inverse of sensitivity) for detection. Small values of external noise (below approximately

31
8%), did not affect contrast sensitivity, indicating that the internal noise of the neural
system was limiting performance. However, as the external noise surpassed a threshold, it
become the limiting factor in performance, leading to a linear decline in sensitivity. By
comparing the post- and pre-training curves, it is possible to discern possible mechanism
of perceptual learning, namely stimulus enhancement, external noise exclusion, and
internal noise suppression.
Perceptual learning in normal observers has also been found to affect the relative
weighting of individual spatial frequencies channels70, 83. Huang et al.90 studied
perceptual learning at a single spatial frequency in amblyopic and normal subjects. They
found that normal subjects received relatively narrow-band improvement in contrast
sensitivity (approximately one octave about the training frequency), whereas the
amblyopic group improved across approximately 4 octaves, as shown in Figure 1.18.
This finding indicates that learning in abnormal visual systems, such as the amblyopic
eye, generalizes across spatial frequency channels, whereas learning in normal eyes is
channel-specific.
Figure 1.18. Normalized improvement in contrast sensitivity in amblyopic (left panel) and normal (right panel) subjects from Huang et al.90. Vertical arrows indicate training frequency.

32
Perceptual learning has recently been applied to improving presbyopic visual
performance18, 91 for near visual tasks. Optical blur (i.e. defocus), as experienced in
presbyopia, has a larger detrimental impact on the high spatial frequency components of
the retinal image, as compared to low spatial frequencies. It is possible that perceptual
learning not only improves the signal to noise ratio of individual spatial frequency
channels, but also contributes to a re-weighting83 of those channels. Therefore, perceptual
learning may lead to a de-blurring of the retinal image, similar to a deconvolution in
image processing, thereby contributing to an improvement in presbyopic visual
performance.
1.7 Thesis Outline
Presbyopia is a visual impairment which affects everybody over the age of 50
years. Therefore, a great deal of effort has been exerted towards developing methods to
abate presbyopia’s adverse side-effects, namely poor near vision. This chapter has
outlined the physiological mechanisms at work behind accommodation and the
development and consequences of presbyopia. In addition, the optical and neural
implications of presbyopic corrections were reviewed.
The remainder of this thesis focuses on the correction of presbyopia by means of
increasing the eye’s depth of focus, taking advantage of the binocular nature of the visual
system, and exploring neural plasticity as a means for further improving presbyopic
visual performance beyond optical methods. The basic outline for the thesis is as follows.
Chapter 2 explores the mechanism of accommodation in young, healthy eyes and
those implanted with the only FDA approved accommodating IOL. A novel approach for

33
quantifying the magnitude of accommodation under natural, binocular viewing conditions
is proposed, based on simultaneous Shack-Hartmann wavefront sensing while imaging
both pupils, followed by analysis of through-focus retinal image quality. A natural-view
wavefront sensor was developed to enable the simultaneous measurement of wavefront
aberrations, changes in pupil size and pupil convergence during fixation at far and near
objects. With this device, efficacy of accommodating IOLs may be assessed objectively,
providing clinicians and patients with an unbiased expectation for surgical outcomes.
Chapter 3 describes an adaptive-optics bench system developed for the
characterization and metrology of presbyopia-correcting IOLs. Although patients
regularly undergo surgical procedures to replace their natural crystalline lens with a
prosthetic IOL, through-focus image quality of IOLs is poorly understood. The device
presented herein assessed the impact of corneal aberrations, induced with the adaptive-
optics magnetic membrane deformable mirror, on through-focus retinal image quality of
presbyopia-correcting intraocular lenses.
Chapter 4 introduces a robust retinal image quality metric for the prediction of
visual performance in the presence of large magnitudes of optical blur relevant to
presbyopia and multifocal optical designs. The optical design of extended depth of focus
corrections for presbyopia is inherently dependent upon the metric used in the design
process. This metric was subsequently applied to presbyopic corrections intended to
increase the eye’s depth of focus. Several new approaches were investigated, including
induction of higher order wavefront aberrations and pupil apodization. The final optical
designs were evaluated theoretically and psychophysically using a custom-built adaptive-
optics vision simulator.

34
Chapter 5 investigates modified monovision, a new binocular approach to
correcting presbyopia. In modified monovision, each eye’s spherical refraction and depth
of focus is varied to optimize binocular through-focus visual performance, minimizing
the trade-off in distance performance and depth perception.. A binocular adaptive-optics
vision simulator was developed to psychophysically test various modified monovision
strategies.
Chapter 6 examines the role of neural factors in determining through-focus
visual performance with modified monovision. The potential of neural plasticity as a
therapy to further improve visual performance, beyond the limits set by optical theory,
was investigated. Another neural factor, ocular dominance, affecting visual performance
with modified monovision was addressed. The potential of using a novel binocular
rivalry technique to determine the degree of ocular dominance was examined as a
screening tool for potential modified monovision candidates.
Chapter 7 summarizes the research presented in this thesis and discusses its
clinical and scientific implications. Future directions for the work presented here are also
discussed.

35
Chapter 2. Objective Measurement of Accommodating
Intraocular Lens Efficacy
2.1 Introduction to Accommodating IOLs
In addition to the loss of accommodation, age causes changes to the transparency
of the crystalline lens. As the eye ages, the lens proteins breakdown, causing the lens to
scatter light and ultimately opacify, causing cataract. In a population study, Klein et al.92
found that approximately 20 and 43% of U.S. residents between the ages of 65-74 and
75-85 years, respectively, develop cataract.
To treat cataract, the scattering crystalline lens is replaced with a transparent
prosthetic lens, known as an intraocular lens (IOL). In cataract surgery, a small incision
(approximately 2mm in length) is made in the periphery of the cornea. Through the
incision, the crystalline lens is ultrasonically emulsified and aspirated from the capsular
bag. The IOL is subsequently implanted within the remaining capsular bag, alleviating
the intraocular scatter caused by the cataractous crystalline lens. Conventionally, IOLs
have had fixed haptics, or side-arms, which served to position the lens within the capsular
bag, along the line of sight, centered within the pupil. Cataract surgery has had excellent
outcomes for providing clear vision, however, the results are limited to one conjugate
distance, typically at 0 D. Thus, pseudophakes, or patients with IOLs, remain presbyopic
due to the static nature of conventional monofocal IOLs. Seeing that cataracts coincide
with presbyopia, IOLs have become a target for restoration of accommodation. Moreover,
IOL intervention is also available for presbyopic patients without cataract formation, in a
procedure known as refractive lens exchange, or clear lens extraction.

36
For the correction of presbyopia, the eyes must regain their dynamic ability to
change optical power. As described in Chapter 1, two key design concepts exist for IOLs
designed to restore accommodation, known in the literature as “accommodating IOLs”.
First, curvature change designs are intended to mimic the behavior of the youthful
crystalline lens by changing their form with accommodative effort. The second design
concept for accommodation IOLs is axial movement of a rigid optic, altering the eye’s
anterior chamber depth.
Clinical studies of accommodating IOL efficacy provide conflicting results93.
Cumming et al.16 found 97% of patients with the Crystalens accommodating IOL to have
a distance-corrected near visual acuity of at least 20/40, whereas Findl et al.94 had only
approximately 25% of patients reach 20/40 distance-corrected near acuity.
Hunter et al.42 theoretically demonstrated that a single-optic accommodating IOL,
such as the Crystalens, obeys the following formula:
( )22corneaeye
n
xΦ−Φ
∆−≅∆Φ (2.1)
where ∆Φ is the induced accommodation, or change in power of the eye (in diopters), ∆x
is the axial shift of the IOL, n is the refractive index of the IOL, Φeye is the power of the
eye refracted at distance and Φcornea is the power of the cornea. Equation 2.1 is expressed
graphically in Figure 2.1, where we take the representative case of n=1.5, Φeye=60 D and
Φcornea=40 D, typical values for the average model eye.

37
Figure 2.1. Theoretical approximation of induced accommodation of a single-optic accommodation IOL.
From Figure 2.1, it can be seen that in an average eye, to accommodate to an
object at reading distance, which is approximately 2.5D (or 40 cm), a single-optic IOL
would need to travel axially over 2mm, traversing approximately 50% of the anterior
chamber. Such a large distance is not reasonable and may lead to further complications,
such as iris bulging and pigment dispersion37, 38. In an ultrasound biomicroscopy study of
the anterior segment during accommodation, Stachs et al.95 found the ciliary processes
shifted anteriorly by approximately 0.15 mm during accommodation to a near target in
the young normal eye. Therefore, single-optic accommodating lenses, such as the
Crystalens, are theoretically not expected to result in substantial magnitudes of
accommodation beyond a fraction of a diopter. Furthermore, confounding factors such as
capsular bag fibrosis37, 38 may further impair IOL mobility.
To assess accommodative IOL movement, several investigators43, 96-98 have
measured the changes in anterior chamber depth resulting from accommodative effort.

38
Koeppl et al.43 used partial coherence tomography to image the anterior chamber depth in
eyes implanted with an accommodating IOL (Crystalens, AT-45). They found that under
pharmacologically induced accommodation, the accommodating IOLs moved posteriorly
(e.i. away from the cornea) by approximately 0.15 mm (p<0.001). In a more recent study,
Marcos et al.96 found similar results under naturally induced accommodation using three-
dimensional optical coherence tomography imaging. Although such imaging studies
reveal the biomechanical changes of the anterior chamber with accommodating IOLs in
vivo, they fail to reveal the perceived retinal image quality of the patient.
During accommodation, several factors other than ocular power change may
conspire to improve near visual performance, thus obscuring the imaging results. For
example, ocular depth of focus may increase under accommodative effort due to pupil
constriction and changes in higher order aberrations. In several patients imaged by
Marcos et al.96, accommodative effort produced a significant tilt in the IOL as opposed to
an axial shift, potentially inducing wavefront aberrations (astigmatism, coma, etc.). In
addition, binocularity has been shown to significantly improve visual performance in the
presence of optical blur99.
To understand the efficacy of accommodating IOLs, it is essential to measure the
amplitude of accommodation objectively, as opposed to using a subjective method such
as blur tolerance. As highlighted by Adrian Glasser100, subjective measures of
accommodation tend to overestimate the amplitude of accommodation due to the eye’s
inherent depth of focus. The most widely clinically used objective technique, dynamic
retinoscopy, is limited in accuracy by examiner-specific results101. Alternatively, Shack-
Hartmann wavefront sensing is ideally suited for objective accommodation studies. From

39
the eye’s wavefront map, image quality metrics can be computed to determine the
optimal defocus for maximizing image quality, thereby objectively determining the eye's
accommodative response102. However, a rigorous investigation of the accommodative
response should not only use an objective measure of the eye’s optical changes, but also
provide the subject with a visual stimulus which represents natural, binocular viewing
conditions.
Previous studies utilizing wavefront sensing to study the accommodative response
used either an instrument which only allowed for monocular viewing of the visual
stimulus, or artificially changed the object distance with a Badal optometer or trial
lenses102, 103. To overcome these limitations, we have developed an instrument to
simultaneously measure all the aspects of the accommodative triad (wavefront, pupil size
and convergence) while presenting the subject with a binocular stimulus at various
distances. The accommodative triad is illustrated in Figure 2.2.

40
Figure 2.2. Accommodative triad: (a) mechanism of ocular power change as drawn by Helmholtz104, (b) pupil constriction data from Alpern et al. (1961) and (c) convergence to maintain binocular fusion on distal and proximal objects.
The purpose of this study was to objectively measure the magnitude of
accommodation in patients implanted with the Crystalens accommodating IOL. We
developed a novel device to simultaneously measure all three aspects of the near triad.

41
Furthermore, we investigated the impact of accommodation on through-focus retinal
image quality.
2.2 Objective Measurement of Accommodation
To objectively assess subjects’ accommodative response, we developed a natural-
view wavefront sensor (shown in Figure 2.3) to monitor wavefront and pupil dynamics
while providing subjects with natural, binocular viewing of a fixation target. The system
consisted of a custom-made Shack-Hartmann wavefront sensor and two pupil cameras
operating simultaneously with a frame rate of 5 Hz. The wavefront sensor used a near-
infrared collimated laser diode (λ=980 nm), well outside of the visible spectrum, to avoid
any visual competition with the fixation stimulus. Due to senile miosis, a relatively high
pupil sampling of the lenslet array (200 µm pitch, 3.4 mm focal length) was used for
adequate sampling of the wavefront within small entrance pupils typically found in the
elderly population. For example, within a 2.0 mm diameter entrance pupil, 80 total
lenslets sample the wavefront, from which the wavefront may be reconstructed using
Zernike coefficients up to 7th radial order with minimal reconstruction error105, 106. The
wavefront sensor was mounted to an XYZ translation and rotational stage to allow
measurement of either eye within the foveal isoplanatic patch107, 108 during changes in
vergence.

42
Figure 2.3. Schematic layout of the natural-view wavefront sensor.

43
The pupils were illuminated with a near-infrared light-emitting diode (λ=880 nm).
Each pupil was imaged with a camera with 10x magnification, resulting in a resolution of
approximately 70 µm at the pupil plane. An example of collected wavefront sensor and
pupil images are shown in Figure 2.4.
Figure 2.4. Example images from the Shack-Hartman wavefront sensor and the pupil cameras for the right and left eyes (OD and OS, respectively). IPD: interpupillary distance; PD: pupil diameter.
For each frame collected from the wavefront sensor, Zernike coefficients were
computed to describe wavefront aberration. Subsequently, the Zernike coefficients were
used to compute a retinal image quality metric based on image convolution109 (described
in detail in chapter 4). To compute this metric, a Matlab program was developed to
calculate the monochromatic incoherent point spread function for each frame’s wavefront
aberration over the natural pupil size. The point spread function was then convolved with
a reference image to produce a simulated retinal image. Finally, the correlation
coefficient between the registered convolved and reference images was obtained as the
final measure of image quality. This process was iteratively repeated with various
amounts of defocus added to the measured wavefront to acquire a “through-focus”
estimate of image quality. This method of determining the amplitude of accommodation

44
from the through-focus retinal image quality curve was adopted due to the well-known
interaction of higher-order aberrations in their impact on best focus110-112.
The amplitude of accommodation was determined by the dioptric location of best
focus, or the peak of the through-focus image quality curve. Accommodative error was
defined as the dioptric difference between the target vergence (location of the visual
stimulus in diopters) and peak image quality (an example is shown in Figure 2.5). Due to
the eye’s longitudinal chromatic aberration between the wavefront sensor (λ=980 nm)
and the center of the visible spectrum (λ=555 nm), the through-focus image quality curve
during far-viewing was shifted to maximize image quality at the object distance of the far
target and served as a reference for measurements with other viewing distances.
Figure 2.5. Illustration of through-focus retinal image quality for an eye accommodating to a visual stimulus at an object distance of 1.5 D. The amplitude of accommodation was

45
defined as the dioptric location of peak retinal image quality, or best focus. The accommodative error was defined as the difference between the object distance and the dioptric location of best focus.
The visual stimulus consisted of a computer-controlled microdisplay presenting a
20/40 letter ‘E’ (subtending 10 minutes of arc) in white light. The microdisplay was
mounted on a sliding rail to allow axial adjustment of object distance from the subject. As
shown in Figure 2.3, the patient’s line of sight and the device were separated by a large
(10 x 13 cm) dichroic filter acting as a beam splitter, transmitting the visible spectrum
(patient’s line of sight) and reflecting the near infrared (device). Therefore, the device
was out of sight, allowing measurement of the accommodative triad unbeknownst to the
subject.
2.3 Accommodative Response with the Crystalens Accommodating IOL
To examine the efficacy of the Crystalens accommodating IOL, the
accommodative response of 14 eyes of 7 patients (66+11 years of age) implanted with the
Crystalens IOL was evaluated with the natural-view wavefront sensor. For comparison, 6
eyes of 4 emmetropic, young (26+5 years) normal subjects were included in this study as
a control. All subjects were refracted with trial lenses to maximize their subjective image
quality at the far target, which they wore throughout the experiment.
Subjects were instructed to fixate at a target at far (0.25 D), intermediate (1.5 D)
and near (2.5 D) object distances during simultaneous recording of their wavefront and
pupil dynamics. At each object distance, during fixation the natural-view wavefront

46
sensor collected 50 frames (over 10 seconds) of wavefront and pupil images for post hoc
analysis.
The magnitude of convergence and pupil miosis with accommodative effort for
the normal and Crystalens group is shown in Figure 2.6. The convergence ratio (change
in convergence per diopter) in the normal and Crystalens groups, respectively, were
1.79+0.26 and 1.88+0.62 degrees/D. These values are consistent with previous reports for
normal (1.96+0.41 degrees/D)113 and pseudophakic patients with the ICU
accommodating IOL (1.33+0.95 degrees/D)114. The theoretically expected convergence
ratio was calculated using equation 2.2, where IPD is interpupillary distance in meters
and TV is target vergence in diopters.
⋅= TVIPD
2
1arctan Ratio eConvergenc (2.2)
The ideal convergence ratio based on a 65 mm interpupillary distance,
representative of population statistics51, is 1.86 degrees/D and is shown in Figure 2.6a for
comparison (gray line). The appropriate convergence ratios observed in our subjects
indicate proper binocular fusion and serves as an objective confirmation of binocular
fixation at all object distances.
The pupil constriction ratio (change in pupil size per diopter) in the normal and
Crystalens group, respectively, were 0.08+0.14 and 0.23+0.37 mm/D. In a study
published by Wolffsohn et al.114, pseudophakic patients with the ICU accommodating
IOL exhibited a pupil constriction ratio of 0.10+0.10 mm/D, within reasonable agreement
with our results. The difference in pupil constriction ratio between the two groups in our
study can be explained by their age difference. Kasthurirangan and Glasser115, 116 found
that the pupil constriction ratio increases with age, confirming our observation. The

47
changes in pupil size signify a true effort in accommodation, as they suggest a
constriction of the ciliary body with accommodative effort.
Figure 2.6. (a) Change in convergence angle and (b) absolute pupil size as a function of target distance.
As shown in Figure 2.6b, despite both normal and Crystalens groups having a
similar trend in pupil constriction, their magnitudes were significantly different. For
example, during far viewing (0.25 D), the average pupil diameters for the normal and
Crystalens groups were 5.94+0.30 and 4.69+0.38 mm, respectively (p<0.002, unpaired
Student’s t-test). This is due to the large age difference between the normal and
pseudophakic groups, as pupil sizes decrease with age117, 118.
The accommodative response of the two groups is shown in Figure 2.7. When
presented with the intermediate and near stimuli (at 1.5 and 2.5 D, respectively), the
average magnitude of accommodation in the young, normal group was 1.17+0.22 and
2.27+0.30 D, respectively. In addition, a decrease in the magnitude of primary spherical

48
aberration (C40) in all subjects accompanied accommodative effort (-0.02+0.02 µm per
diopter, over a 5 mm pupil). Other higher order aberrations did exhibit a systematic
change with accommodation, in agreement with previous studies119, 120. Additionally, the
residual error, or lag, in accommodation and changes in spherical aberration observed
were consistent with previous studies102, 103, 119, 120.
Figure 2.7. Accommodative response in young, normal and Crystalens groups.
Most subjects in the Crystalens group did not exhibit a significant change in their
wavefront aberrations indicating little shift in optical power. Although the intersubject
variability was large, on average, the magnitude of accommodation was of the incorrect,
negative direction, a result consistent with biomechanical imaging studies43, 96 which
observed an increase in anterior chamber depth with accommodative effort. As shown in
Figure 2.7, the Crystalens subjects’ amplitude of accommodation was -0.07+0.39 and -
0.11+0.53 D for the 1.5 and 2.5 D stimuli, respectively, resulting in an average
accommodation amplitude of -0.05+0.23 DW/DT (where DW/DT represents the diopter of
wavefront change per diopter of target vergence).

49
However, individual eyes showed a large amount of variability in the shift of best
focus with accommodative effort. Of the 14 eyes measured, 6 eyes showed a small, albeit
positive shift in accommodation (0.14+0.23 DW/DT), 6 eyes showed a negative shift in
accommodation (-0.26+0.21 DW/DT), and 2 eyes showed no change.
Figure 2.8 shows an example of through-focus image quality from a Crystalens
subject. This example illustrates the importance of understanding through-focus retinal
image quality for assessing presbyopic corrections. The grey, orange and magenta curves
represent the through-focus retinal image quality computed from the wavefront aberration
for the natural pupil size. The arrows at the abscissa denote the location of peak image
quality (0.25, 0.25 and 0.75 D) during fixation at a target at far, intermediate and near
distances. In contrast, if accommodative amplitude been defined using only the lower-
order aberration Zernike defocus (C20) for a fixed pupil size, the magnitude of
accommodation to the intermediate and near target would have been -0.09 and -0.0 7 D,
respectively.
Figure 2.8. Through-focus retinal image quality of an Crystalens accommodating IOL subject with a positive shift in best focus, denoted by the arrows at the abscissa.

50
This subject had a significantly significant difference between estimation of
accommodation amplitude when computed using through-focus retinal image quality
curve (Figure 2.8) as opposed to only considering the Zernike defocus coefficient (C20).
This difference is shown in Figure 2.9.
Figure 2.9. Measure of accommodative amplitude in a Crystalens patient based on best-focus (blue) and Zernike defocus (red). The gray curve represents the ideal magnitude of accommodation. Asterisks denote a statistically significant difference between the two accommodation measure methods (p<0.05, Student’s t-test, unpaired).
As described above, the improvement in near image quality not predicted by
changes in Zernike defocus may arise from changes in higher order aberrations. As this
subject accommodated from far to near, astigmatism increased from 0.60+0.13 to
0.71+0.08 D (p<0.00005, Student’s t-test, unpaired). In addition, Zernike coma also
increased due to accommodation from 0.03+0.02 to 0.05+0.02 µm over a fixed 3.2 mm
pupil (p<0.00005, Student’s t-test, unpaired). Previous studies96, 121, 122 have shown that
IOL tilt causes increase of astigmatism and coma. Although our study did not include
intraocular imaging, lens tilt is a possible cause for the observed wavefront changes.

51
2.4 Conclusions
In conclusion, single-optic accommodating IOL technology, such as the
Crystalens IOL holds promise, however current ability to improve near image quality in
presbyopic patients was lacking. Accommodating IOLs, such as the Crystalens, are
limited by low efficiency of displacement-to-power conversion (approximately 1 mm per
diopter). In addition, we found significant changes in asymmetric aberrations such as
astigmatism and coma, which may be caused by lens tilting in the capsular bag due to
irregular capsular fibrosis96, 121, 122.
We have shown that ocular higher order aberrations have a significant impact on
determining the location of best focus and are critical for accurate representation of
retinal image quality. This is especially important for the objective measurement of
accommodation and understanding of presbyopic visual performance. The methods
proposed and described here can be applied to understanding the mechanism of
accommodation in young, normal subjects, presbyopic subjects with accommodating
IOLs and may be applied to other areas of vision science, such as ocular development,
emmetropization and myopia control.

52
Chapter 3. Impact of Corneal Aberrations on Optical
Quality of Presbyopia-Correcting Intraocular Lenses
3.1 Introduction
As discussed in the previous chapter, IOLs have become ubiquitous for treating
cataracts. Although accommodating IOLs promise a true restoration of dynamic
accommodation, they represent a small portion of presbyopia-correcting IOLs implanted.
Instead, the majority of presbyopia-correcting IOLs aim to increase the eye’s depth of
focus via multifocality, a strategy termed pseudoaccommodation. Specialty IOLs which
aim to extend the eye’s depth of focus are growing in popularity among patients and
surgeons, therefore the understanding of their optical quality is increasingly important.
Many different designs for multifocal IOLs are available to clinicians. The
primary design types fall into two categories, refractive and diffractive, multifocal optical
designs, which split incoming light into 2 or more discrete foci123. Although this
approach can significantly increase the range of useful vision, the negative consequences
of increasing the depth of focus of any optical system are well known.
Typical side-effects of multifocal IOLs include decreased contrast sensitivity124-
126 and photic phenomena such as halos and glare125, 127, 128, which are especially
problematic in low light levels when the pupil is enlarged (e.g. night driving)129.
Although multifocal IOLs reduce dependency on spectacles for presbyopes, some
patients may be dissatisfied due to side-effects to the point of explantation127, 130.
For clinicians to successfully select multifocal IOL candidates and to
subsequently set appropriate expectations for patients, a clear understanding of IOLs’

53
optical characteristics and retinal image quality is critical. Optical bench testing of IOLs7,
9-12 is one such means to uncovering the characteristics and limitations of presbyopia-
correcting IOLs. However, to date, optical bench studies of IOLs have only examined
IOLs in isolation, that is, without consideration for patient-specific optical factors, such
as corneal aberrations and pupil size.
The eye is an optical system with three primary optical components: cornea, iris
and lens. The corneal aberrations interact with those induced by the lens to yield the
complete ocular aberrations, which with the pupil, determine retinal image quality131, 132.
Although positive spherical aberration is the only corneal higher order aberration
consistently found across large populations, individual corneas may have significant
magnitudes of astigmatism and other higher order aberrations133, 134. Furthermore,
cataract implantation is known to induce aberrations in the cornea such as astigmatism,
coma and trefoil134, 135. Although the impact of corneal astigmatism and higher order
aberrations on visual performance has been studied11, 14-16 in normal and pseudophakic
patients, the explicit effect on in-vitro optical quality has not been investigated previously.
As such, objective evaluation of optical quality in optical bench systems has the
advantage of isolating optical factors from the neural visual system.
Investigating the potential impact of these factors on through-focus pseudophakic
retinal image quality is essential for the accurate understanding of visual outcomes and
limitations of extended depth of focus IOLs. The aim of this section was to develop a
new method to determine the influence of corneal aberrations on presbyopia-correcting
IOLs’ through-focus retinal image quality. Therefore, an adaptive optics (AO) system136
was combined with an IOL optical bench system137 to enable optical metrology of a

54
model eye consisting of various IOLs, an artificial pupil, and an artificial cornea with
variable lower and higher order aberrations imparted using a deformable mirror.
3.2 Corneal Aberrations of Post-Cataract Extraction Patients
To correctly model the corneal aberrations of presbyopes following cataract
surgery, a group of normal, asymptomatic post-cataract extraction patients were recruited
for this study. All patients signed an informed consent form prior to participation, and all
procedures were approved by the University of Rochester Research Review Board and
were in accord with the tenets of the Declaration of Helsinki..
Topography of the anterior and posterior corneal surfaces of 21 eyes from 21
patients were measured with an Orbscan corneal topographer (Bausch & Lomb). From
the topographical elevation maps, the corneal aberrations were calculated following a
method established elsewhere138. Over a 5.0 mm pupil, the mean corneal higher order
RMS and Zernike primary spherical aberration (C40), respectively, were 0.29+0.10 and
0.15+0.09 µm. For a 3.0mm pupil, mean corneal higher order RMS and Zernike primary
spherical aberration (C40), respectively, were 0.06+0.02 and 0.02+0.01 µm.
3.3 Adaptive-Optics Intraocular Lens Metrology
The AO-IOL metrology system consisted of three parts: a model eye (artificial
cornea, wet cell, IOL), an imaging arm (to obtain the retinal image of the model eye) and
AO (to induce corneal aberrations). This system was described in detail by Zheleznyak et
al.139 and in part by Kim et al.137. A schematic of the system is shown in Figure 3.1.

55
Figure 3.1. Schematic of adaptive optics IOL metrology optical bench (CCD=charge-coupled device), from Zheleznyak et al.139.
A wet cell and an aspheric, achromatic doublet with a power of 40.0 D comprised
the model eye, as recommended by ISO 11979-2140. The wet cell, within which the IOL
was mounted, consisted of a fluid-filled (balanced salt solution) compartment between
two optically flat windows. The airspace between the wet cell and artificial cornea
ensured the proper pupil magnification ratio in accordance with the Gullstrand model eye.
Entrance pupil size was determined with an artificial pupil conjugate to the model eye’s
pupil plane. An external pupil camera was used to confirm alignment of IOLs placed
within the model eye on an XY translational stage.
A resolution target consisting of a tumbling letter “E” acuity chart with lines
equivalent to 20/40, 20/30/ 20/25, 20/20 and 20/15 letter sizes was displayed in white

56
light by a digital light processor (DLP) projector (PG-M20X, Sharp) at a retinal conjugate.
The model eye’s retinal plane was relayed by a microscope objective onto a 5-megapixel
charge-coupled device to ensure adequate sampling of the retinal image. To adjust the
target vergence at the model eye for through-focus imaging while maintaining constant
magnification, a Badal optometer was implemented in the system.
The pupil plane of the model eye was relayed to a large-stroke deformable mirror
(Mirao 52D, Imagine Eyes) using a pair of achromatic lenses. By changing the surface
profile of the deformable mirror, aberrations are induced to the model eye, allowing for
the simulation of various corneal topographies. A custom-made Shack-Hartmann
wavefront sensor validated the aberration profiles generated by the deformable mirror.
Three presbyopia-correcting IOLs were included in this study: Crystalens HD500
(Bausch & Lomb), ReSTOR +3D SN6AD1 multifocal (Alcon Laboratories, Inc.) and
Tecnis ZM900 multifocal (Abbott Medical Optics, Inc.). Each IOL has a unique design
and approach toward presbyopic correction. The Crystalens HD500 is a single-optic
accommodating IOL. The optical element of this IOL has a bispheric design with positive
power (1.0 D) added to its central 1.5 mm zone, thus falling in the category of a refractive
bifocal (see Figure 1.10b). To isolate the optical performance of the IOL, no axial
movement of the IOL was imposed in the model eye. The ReSTOR +3D SN6AD1 and
Tecnis ZM900 are both diffractive multifocal IOLs based on the Fresnel zone-plate
principal of a kinoform. The ZM900, described as a full-aperture diffractive IOL, equally
distributes light to the zeroth (distance vision) and first (near vision) orders of diffraction
independent of pupil size. Conversely, the ReSTOR 3D SN6AD1 IOL has an apodized
design, in which the diffraction efficiency is pupil-dependent. In this design, distance

57
vision is favored for large pupils123. A detailed description of diffractive multifocal IOL
design is outlined elsewhere141. For comparison, a monofocal IOL (AcrySof SN60AT,
Alcon Laboratories, Inc.) was included in the study. All IOLs in this study had a 20.0 D
base power.
3.4 Experimental Protocol
Through-focus images with the model eye were captured over a dioptric range of
6.00 D, ranging from -1.00 D (object beyond infinity) to +5.00 D (near object) in steps of
0.125 D. At each dioptric step, 3 images were obtained and averaged to reduce the impact
of electronic noise in the imaging device.
To evaluate the impact of corneal astigmatism, the through-focus imaging
sequence was performed in the presence of Zernike horizontal astigmatism (C22) induced
by the deformable mirror (up to 1.00 D in steps of 0.25 D). To assess the effect of corneal
higher order aberrations, a through-focus image sequence was collected for each of the 21
corneal aberration profiles induced by the deformable mirror. As a control condition, a
through-focus image sequence was also obtained with an aberration-free cornea for each
IOL. Each aberration condition was carried out for 3.0 and 5.0 mm pupil diameters.
Several techniques exist for quantifying optical quality of IOLs in an optical
bench. A routine test for measuring the optical quality of IOLs in an optical bench is the
measurement of the modulation transfer function (MTF)129, 142, 143. The MTF represents
an optical system’s contrast attenuation for individual spatial frequencies (i.e. contrast in
the image plane of an object with 100% contrast). The MTF can be calculated by Fourier
transforming the captured image of a point-source or by directly measuring the contrast

58
of gratings from a resolution target, such as the commonly used United States Air Force
resolution target. Image sharpness144 of IOLs has also been quantified from resolution
target imaging.
In the presence of corneal lower and higher order aberrations, the eye’s point
spread function is radially asymmetric and may be highly directional. Therefore,
measuring optical quality in only two meridians (e.g. vertical and horizontal) may not be
representative of overall image quality in all directions. Therefore, we employed a
technique based on the 2-dimensional spectral analysis of the retinal image. The benefit
of this technique is that it quantifies overall image quality regardless of the orientation of
point spread function relative to the resolution target.
Figure 3.2. Illustration of the correlation-coefficient image quality metric. The reference column depicts an unaberrated reference image. The sample column depicts images with ideal, or degraded images of the model eye.
Through-focus image quality was determined using the correlation coefficient
(CC), as demonstrated previously by Zheleznyak et al.139 and Kim et al.137. In this
technique, the CC between the captured images through the model eye and a registered

59
reference image (un-aberrated) quantifies image quality (as illustrated in Figure 3.2). A
CC value of one is indicative of a perfect match between the un-aberrated reference and
captured image and therefore represents ideal image quality. CC values less than one
indicate a degradation in image quality. The captured images of the model eye were
registered prior to CC computation. The CC was calculated using custom-developed
Matlab software. In line with the clinical practice of optimizing distance image quality,
the distance image (0.00 D) was defined as the image with the peak CC value for each
pupil size. Defocus points for the remaining images were shifted accordingly. Depth of
focus was defined as the dioptric range, from distance (0 D) to near, for which the CC
values was above 80% of the peak value of the control IOL (AcrySof monofocal). If the
CC value fluctuated about the depth of focus criterion, the regions for which the CC
value was above the threshold were summed.
3.5 Impact of Pupil Size with Aberration-Free Cornea
Figure 3.3 shows the captured images of the resolution target for all IOLs under
test with an aberration-free cornea and 5.0 mm pupil. The quantification of image quality
using the CC for 3.0 and 5.0 mm pupil sizes are shown in Figure 3.4. The AcrySof
monofocal and HD500 IOLs both exhibited a single through-focus peak in image quality.
At distance (0 D), the monofocal IOL had superior optical quality for both pupil sizes
compared to the presbyopia-correcting IOLs. Since the introduction of diffractive
multifocal IOLs in the 1980’s, reduced image quality at distance and unwanted visual
side-effects have been regularly reported124-126. At intermediate distances (1.5 D), the
HD500 was superior to other IOLs due to its bispheric design.

60

61
Figure 3.3. Through-focus retinal images of the model eye with 4 different IOLs. Images were collected using a 5.0 mm pupil and an aberration-free cornea. The letters in the resolution target (from top to bottom rows) correspond to 20/40, 20/30, 20/25, 20/20 and 20/15 Snellen letters.
The ReSTOR and ZM900 diffractive IOLs (apodized and full-aperture,
respectively) exhibited bimodal through-focus image quality curves, as shown in Figures
3.3 and 3.4. As the pupil size decreased, intermediate image quality improved
significantly for both diffractive multifocals. However, the ReSTOR distance and near
image quality were dependent upon the pupil size due to its phase-apodized design123. In
contrast, pupil size did not have a significant impact on the relative energy distributed to
distance and near foci for the ZM900. The add-power of the ReSTOR and ZM900
multifocals, for a 6.0 mm pupil, was 3.0 and 4.0 D, respectively.
Figure 3.4. Through-focus retinal image quality of presbyopia-correcting IOLs with an aberration-free cornea. The solid and dotted lines correspond to 3.0 and 5.0 mm pupils.

62
3.6 Impact of Corneal Astigmatism
The impact of corneal astigmatism on distance image quality for a 3.0 mm pupil
is shown in Figure 3.5. With the exception of a vertical offset in distance image quality,
all IOLs exhibited similar reduction in distance image quality as a function of corneal
astigmatism. For all IOLs, percent reduction in distance image quality with 0.5 and 1.0 D
corneal astigmatism was 14.3+1.4 and 25.8+3.2 %, respectively. The trend with a 5.0 mm
pupil was similar, but with a larger magnitude (20.2+2.8 and 33.5+3.2 %, respectively).
Figure 3.5. Distance image quality with a 3.0mm pupil as a function of corneal astigmatism.
The impact of corneal astigmatism on through-focus image quality can be seen in
Figure 3.6. For comparison, through-focus retinal image quality with an aberration-free
cornea is shown with black lines. Through-focus image quality with 0.25, 0.50, 0.75, 1.00
D of corneal astigmatism is shown with blue, green, orange and red lines respectively.

63
As corneal astigmatism increased in a monofocal eye, the peak image quality of
vertical edges underwent a hyperopic shift and horizontal edges underwent a myopic shift.
The consequence of distinct meridians shifting in best focus degrades overall image
quality, as shown in Figure 3.5 and 3.6. However, astigmatism’s effect of separating the
best-focus for perpendicular meridians produced an interesting observation in the
multifocal IOLs: an improvement in intermediate image quality. This was likely caused
by the combining of myopically shifted horizontal edges from the distance focus with
hyperopically shifted vertical edges from the near focus of the multifocal IOLs. A similar
observation was made by Hayashi et al.145 in through-focus visual acuity measurements
in patients with the SN6AD1 (ReSTOR) IOL and trial-lens induced astigmatism. Their
study found an improvement in visual acuity at intermediate distances in the presence of
trial-lens induced astigmatism.

64
Figure 3.6. Through-focus retinal image quality in the presence of corneal astigmatism for 3.0 and 5.0 mm pupils (left and right panels, respectively).
In the absence of corneal astigmatism, for a 3.0 mm pupil, the depth of focus was
1.13 D for the monofocal IOL, 1.75 D for the HD500, 2.38 D for the ReSTOR, and 2.38
D for the ZM900. The bispheric design of the HD500 led to a significant improvement in
depth of focus over the monofocal SN60AT only for the smaller pupil size. With a 5.0
mm pupil, the depth of focus was 0.88 D, 1.00 D, 0.75 D, and 1.63 D, respectively.
Figure 3.7 illustrates the change in depth of focus as corneal astigmatism was induced to

65
the model eye. As corneal astigmatism exceeded 0.75 D, the diffractive multifocal IOLs
lost their benefit of extended depth of focus as compared to monofocal and HD500 IOLs.
Figure 3.7. Depth of focus in the presence of corneal astigmatism for 3.0 and 5.0 mm pupils (left and right panels, respectively).
3.7 Impact of Corneal Higher Order Aberrations
Through-focus image quality in the presence of corneal higher order aberrations is
shown in Figure 3.8. Corneal higher order aberrations had a small magnitude over a 3.0
mm pupil (0.06+0.02 µm), and consequently had relatively little impact on image quality.
However, with a 5.0 mm pupil, corneal higher order aberrations had a universal
consequence of diminishing peak image quality and slight improvement in intermediate
image quality, however these effects were much smaller than the astigmatism case.

66
Figure 3.8. Through-focus retinal image quality in the presence of corneal higher order aberrations for 3.0 and 5.0 mm pupils (left and right panels, respectively).
The impact of corneal higher order aberrations on distance image quality with a
5.0 mm pupil is shown in Figure 3.9. Distance image quality was significantly degraded,
especially for the ReSTOR multifocal IOL. The coefficient of determination (R2-value)
for distance image quality (5.0 mm pupil) with corneal higher order RMS was 0.69, 0.77,
0.82, and 0.54, for the SN60AT, HD500, SN6AD1 and ZM900 IOLs, respectively. Of all
the individual higher order aberrations, distance image quality was most strongly
influenced by corneal spherical aberration (C04) in the monofocal IOL (SN60AT). The

67
R2-value for distance image quality with corneal spherical aberration was 0.58, 0.37, 0.32
and 0.27, respectively.
Figure 3.9. Distance image quality (CC) for a 5.0 mm pupil as a function of corneal higher order RMS.
3.8 Summary
In summary, we found that the optical characteristics of presbyopia-correcting
IOLs could be determined using an adaptive-optics IOL metrology system. By inducing
corneal aberrations in a model eye using adaptive-optics, it is possible to visualize and
assess, both objectively and subjectively, through-focus retinal image quality.
Understanding the characteristics and limitations of presbyopia-correcting IOLs’ through-
focus retinal image quality will allow clinicians to better understand their options and
screen potential candidates for certain lenses. For example, we found that patients with
corneal astigmatism greater than 0.75 D are poor candidates for diffractive multifocal

68
IOLs. These findings will enhance the ability to predict and explain clinical outcomes
after IOL implantation and also allow clinicians to choose the best IOL for individual
patients based on their corneal aberrations and expectations.

69
Chapter 4. Extending The Eye’s Depth of Focus
4.1 Introduction
Increasing the eye’s depth of focus, or pseudoaccommodation, is a means of
lessening the symptoms of presbyopia. Although a true restoration of the eye’s dynamic
ability to change focus is preferable, this alternative is currently out of reach for the
presbyopic population. In the interim, an abundance of depth of focus extending options
are available for presbyopes.
Depth of focus of the normal human eye has been studied extensively throughout
the twentieth century (see Wang and Ciuffreda for review31). Due to its dependence on
pupil size, wavefront aberrations, spatial frequency of visual stimulus, method of
measurement, and retinal eccentricity, reported values in the literature vary widely
between 0.3 – 0.45 D in the fovea 35 to 2.5 – 6.5 D in the periphery146. However, within
the context of presbyopia, the general consensus in the literature is that a typical
presbyopic eye is capable of resolving 20/40 letters with up to approximately 1.5 D of
blur33, 59, 147, 148.
The simplest method to increase the eye’s depth of focus is to reduce the pupil
size33, 34, 149. As mentioned previously, pinhole apertures (1-2 mm in diameter)33, 150
significantly increase the eye’s depth of focus via diffraction. Although this strategy is
straightforward and intuitive, it has practical limitations. For example, due to the
significant reduction in retinal illuminance, it may only be applied monocularly45.
Furthermore, Tabernero and Artal151 have shown with optical modeling that accurate

70
centration of corneal apertures to within several hundred microns in the eye is critical to
minimize monochromatic and transverse chromatic aberrations.
Alternatively, wavefront aberrations offer an avenue to improving near vision.
Nio et al.152 found that the eye’s native higher order aberrations increase depth of focus,
however are also correlated with loss of contrast at high spatial frequencies. A multitude
refractive options that modify the eye’s wavefront aberrations are available to presbyopic
patients. Bifocal contact lenses typically are divided into two or more radial zones of
alternate refractive power153, 154. In so-called center-near contact lenses, the central zone
has additional refractive power for near vision. On the other hand, center-distance designs
allocate the increased power zone to the peripheral zone. Surgical wavefront procedures
include the implantation of a refractive corneal inlay in the corneal stroma to aspherize
the anterior corneal surface155, 156, aspheric ablation profiles in laser refractive surgery157,
158, and multifocal IOLs137, 139. However, the ultimate goal of pseudoaccommodation
strategies is to maintain excellent distance vision while improving vision at intermediate
and near object distances. While the exchange of distance image quality with depth of
focus is inescapable, our goal was to optimize this trade-off.
To accurately model through-focus visual performance with optical theory, a
robust retinal image quality metric is required. Therefore, we begin by introducing a
novel image quality metric to be subsequently used in the optimization of presbyopic
wavefront corrections. In this chapter, we will investigate methods of increasing the eye’s
depth of focus using higher order wavefront aberrations, in particular, primary and
secondary spherical aberrations. Subsequently, we will investigate the interaction of the

71
phase and amplitude function of the eye for presbyopic correction by combing multifocal
wavefronts with pupil transmission apodization.
4.2 Retinal Image Quality Metrics
Single-value image quality metrics computed from the wavefront aberration
provide a means of objectively quantifying the eye’s optical quality. However, of the
myriad of potential metrics, only a handful are well-correlated to visual performance.
Furthermore, as optical quality degrades, predicting visual performance from optical
theory becomes even more challenging159, 160. Several studies111, 112, 161, 162 have examined
the potential of using wavefront derived metrics to predict patients’ manifest refractions
(i.e. spectacles’ prescription). Thibos et al.112 found that certain metrics, but not all, were
capable of accurately predicting subjective refractions to within an 1/8th of a diopter.
Interestingly, these studies111, 112, 161, 162 also found that wavefront RMS, a quantity
commonly used in lens design, is one of the poorer indicators of refraction and visual
performance.
Wavefront RMS, defined as the standard deviation of the wavefront surface
topography, can be calculated as the square root of the sum of squared Zernike
coefficients162:
( )∑=mn
m
nC,
2RMSWavefront (4.1)
Where Cnm is the magnitude coefficient of the Zernike polynomial corresponding to the
mth radial order and nth azimuthal order. The poor correlation between wavefront RMS
and image quality is exemplified in Figure 4.1.

72
Figure 4.1. Illustration of wavefront aberrations and a convolved letter E for various magnitudes of spherical aberration and defocus. Combining spherical aberration and defocus yielded the sharpest image, despite the largest wavefront RMS.
The leftward column shows the wavefront map and simulated retinal image (via
convolution) of an eye with C40 = 0.25 µm of Zernike primary spherical aberration for a
4.0 mm pupil. The central column contains a wavefront map and simulated retinal image
with C20 = 0.52 µm of defocus. Finally, the rightward column exhibits a wavefront map
obtained by summing the previous two, (0.25 and 0.52 µm of spherical aberration and
defocus, respectively) with an RMS of 0.58 µm and the corresponding retinal image.
Despite having the largest RMS, due to wavefront interaction of defocus and spherical
aberration, this condition produces the clearest image.
Therefore, a more robust image quality metric capable of predicting visual
performance in the presence of large aberrations is needed for the design of presbyopic

73
corrections. For depth of focus extending strategies, image quality must be optimized
over a range of defocus from distant objects (i.e. at optical infinity, 0 D) to reading
distance (approximately 33 cm, or 3 D). This range of 3 D represents a substantial
degradation in image quality for a diffraction limited optical system. For example, with
4.0 mm pupil (typical in the presbyopic population117, 118) and at a wavelength in the
center of the visible spectrum at 555 nm, 3 D of defocus blur decreases the Strehl ratio by
4 orders of magnitude, from 1 to 0.0003.
Natural images regularly encountered in daily life are rich in contrast and spatial
frequency163, 164. With the plethora of information available in a natural image, judging
image quality based on one feature is not practical. To wit, the perception of image
quality may be driven by various features of the retinal image, such as edge sharpness,
contrast, spatial phase or local luminance. Depending on the visual task, subjects may
favor one image feature for another. For example, in contrast sensitivity measured with a
Gabor stimulus at one spatial frequency, the relative phase and contrast of other spatial
frequencies is irrelevant165. Alternatively, in an acuity task, where the visual stimulus
incorporates a broad range of spatial frequencies, these factors becoming increasingly
important.
In our study, we chose high-contrast visual acuity to serve as the benchmark for
visual performance due to its wide-spread clinical use and its relevance to real-life tasks,
such as reading. Cheng et al.111 compared 31 image quality metrics’ ability to predict
through-focus acuity (over a range of less than 2 D) in the presence of spherical
aberration (0.09, 0.18 and 0.45 µm for a 5.0 mm pupil). Among the worst predictors of
through-focus visual acuity were wavefront RMS and the half-width at half-maximum of

74
the point-spread function (R2 = 0.24 and 0.13, respectively). The metric with the highest
correlation (R2 = 0.68) with through-focus visual acuity was the visual Strehl ratio
(VSOTF), which is defined as112:
( ) ( ){ }
( ) ( )∫ ∫
∫ ∫∞
∞−
∞
∞−
∞
∞−
∞
∞−
⋅
⋅
=
yxyxDLyxN
yxyxyxN
dfdfffOTFffCSF
dfdfffOTFffCSF
,,
,Re,
VSOTF (4.2)
Where fx and fy correspond to spatial frequency coordinates, CSFN(fx,fy) represents
neural contrast sensitivity69, 74, OTF(fx,fy) and OTFDL(fx,fy) denote the optical transfer
function of the aberrated and diffraction-limited cases, respectively. The VSOTF can be
interpreted as the volume under the optical transfer function weighted by the visual
system’s neural contrast sensitivity function, normalized by the diffraction-limited case.
Although the VSOTF exhibited the highest correlation with visual performance compared
to other metrics, residual inaccuracies of one to two lines of acuity present a limitation for
the optical design of presbyopic-corrections111. Therefore, our goal was to develop a
more accurate image quality metric for predicting through-focus visual performance in
the presence of wavefront aberrations.
4.2.1 Convolution Based Image Quality Metric
We chose to examine a new metric based on the two-dimensional convolution of
a reference image with the ocular intensity point spread function, first investigated by
Watson and Ahumada109. The so-coalled image convolution metric (ICM) is defined as
the correlation coefficient of an un-aberrated reference image, a(x,y), and an aberrated
and co-registered (i.e. convolved) image b(x,y), as shown below:

75
−−= ∫ ∫∞
∞−
∞
∞−
ηξηξ ddyxbyxa ),( ),( maxICM * (4.3)
Where (x,y) and (ξ,η) represent the spatial coordinates of the reference and aberrated
images, respectively. This metric was further extended to yield an estimate of through-
focus retinal image quality by incrementally adding defocus to the convolution point
spread function. The computation of through-focus image quality using ICM is illustrated
in Figure 4.2. The symbol in step 3 represents the convolution and the symbol in
step 5 represents the auto-correlation.
It should be noted that the point spread function used for convolution incorporated
the Stiles-Crawford effect. Based on a population study by Applegate and
Lakshminarayanan166, the average magnitude of the Gaussian amplitude apodization
function of the pupil function is approximately αa = 0.025mm-2, where the pupil function
is defined in equation 4.4 below:
)(2
2
10)(rWi
rerp a λ
πα−= (4.4)
where αa is the amplitude apodization coefficient representing the Stiles-Crawford effect,
r is the pupil radius, λ is the wavelength, and W(r) is the wavefront phase.

76
Figure 4.2 Illustration of the computational steps of the ICM.
In Figure 4.2, the ICM is illustrated using an image of a letter “E”. Because the
ICM is a spectral analysis of the similarity between the convolved and aberration-free
reference image, the spectral composition of the chosen image has an impact on the
ICM’s efficacy. We examined the role of the image power spectrum by computing
through-focus image quality with the ICM using three different images: a 20/20 Snellen
letter E, a letter chart containing letters ranging in size from 20/40 (top line) to 20/15
(bottom line) and a natural image. As shown in Figure 4.3a, these images have
significantly distinct power spectra. Subsequently, their through-focus image quality
predictions are significantly different, as shown in Figure 4.3b. The ICM corresponding

77
to the 20/20 Snellen letter (red curves), which had the most low, mid and high spatial
frequency content, was most severely impacted by defocus. Conversely, the ICM
corresponding to the natural scene (gray curves) with relatively less high spatial
frequency content was less affected by defocus.
Figure 4.3. (a) Radially averaged power spectra and (b) through-focus image quality for three distinct reference images: a 20/20 Snellen E (red line), a letter chart with letters ranging in size from 20/40 to 20/15 (blue line) and a natural scene (gray line).
As shown above, the ICM is highly dependent upon the spectral composition of
the images used in the computation. However, with different images the through-focus
trend is similar, despite the value of the ICM being different. This acts as a obstacle in
comparing studies which use different images in the ICM computation. Therefore, a

78
limitation of this metric is that its values are not universal and comparing results based on
different images is not appropriate.
4.2.2 Experimental Validation with Adaptive Optics Vision Simulator
The performance of the ICM as compared to other retinal image quality metrics
was assessed using an adaptive optics (AO) vision simulator, described in detail
elsewhere136. Briefly, the AO vision simulator measures a subject’s wavefront aberrations
with a Shack-Hartmann wavefront sensor, which provides a closed-loop signal to an AO
wavefront correction device (i.e. a deformable mirror) which is relayed to the subject’s
pupil plane. Thus the subject views a visual stimulus for vision testing while their
aberrations are being manipulated in real-time at a rate of approximately 10 Hz. The AO
vision simulator is capable of correcting and inducing large magnitudes of aberrations
with a residual root mean square error of 0.10+0.02 µm136.
The research presented in this section was approved by University of Rochester
Research Review Board. All subjects signed an informed consent form and underwent a
clinical eye exam prior to participation in this study. All procedures involving human
subjects were in accordance with the tenets of the Declaration of Helsinki.
Three subjects (age: 43+15 years) participated in this study. Cycloplegic eye-
drops (tropicamide, 1%) were used to dilate subjects’ pupils and paralyze
accommodation167. The AO system was used to fully correct subjects’ monochromatic
wavefront aberrations over a 4.0 mm pupil. Through-focus high-contrast visual acuity
was measured under three wavefront aberration conditions for each subject. We chose to
induce Zernike primary spherical aberration (C40 = 0.0, +0.2 and +0.4 µm) due to its

79
inherently multifocal nature as a 4th-order aspheric wavefront168. For each magnitude of
spherical aberration, retinal image quality was subjectively optimized to account for the
interaction of spherical aberration and defocus. The interaction between spherical
aberration and defocus will be discussed in greater detail subsequently.
During aberration manipulation with the AO system, through-focus visual acuity
was measured in 0.5 D increments, from -1.5 to 2.0 D. High-contrast visual acuity
measurement was measured with a single black letter “E” on a white background (retinal
illuminance of 70 cd/m2) and a four-alternate forced-choice paradigm. A psychometric
function based on 30 trials was obtained using the QUEST169 algorithm where acuity was
defined as the letter size for which 62.5% of responses were correct. Three acuity
measurements were averaged for each optical condition and were represented in units of
the logarithm of the minimum angle of refraction (logMAR). 0.1 logMAR units
corresponds to one line of visual acuity on clinically used letter charts. The unit
conversion of letter sizes in Snellen, logMAR, arc minute subtense and fundamental
spatial frequency is shown in Table 4.1.

80
Table 4.1. Unit conversion of letter sizes.
4.2.3 Prediction of Through-Focus Visual Acuity
Through-focus convolved 20/40 letter E’s are shown in Figure 4.4 for
polychromatic light, a 4.0 mm pupil and 0.0, +0.2 and +0.4 µm of primary spherical
aberration. Defocus has been added to the nonzero spherical aberration cases to optimize
image quality at 0 D59, 170.
Figure 4.4. Convolved images of a 20/40 Snellen E with 0, +0.2 and +0.4 µm of primary spherical aberration from -3 to +3 diopters of defocus for a 4.0 mm pupil.

81
Through-focus retinal image quality computed with the ICM and the
corresponding average visual acuity is shown in Figure 4.5. As can be seen in Figure 4.5a,
induction of Zernike primary spherical aberration both increases depth of focus and
degraded peak image quality. The through focus image quality trends in Figure 4.5a are
asymmetric about 0.0 D in the presence of spherical aberration. With spherical aberration,
the letter at -1.0 D is sharper than at +1.0 D, however it also suffers from more haloing.
Alternatively, the letter at -2.0 D is more difficult to resolve than at +2.0 D. Subjectively,
the image quality metric and visual acuity data are representative of the convolved
images shown in Figure 4.4. Firstly, in the absence of spherical aberration, defocus had a
profound negative impact on image quality.
The interaction of defocus with primary spherical aberration in a study by
Ravikumar et al.171. The investigators concluded that the spatial phase transfer function,
to a greater extent than the modulation transfer function, is critical to determining image
quality. Furthermore, when defocus and spherical aberration are of the same sign (e.g.
both positive), the phase-reversed regions of the modulation transfer function have less
relative energy as compared to the opposite sign case.
Figure 4.5. (a) Through-focus retinal image quality given by the image convolution

82
metric (ICM) for 0, +0.2 and +0.4 µm of Zernike primary spherical aberration for a 4.0 mm pupil. (b) Corresponding average monocular through-focus visual acuity measured in 3 cyclopleged subjects. Error bars represent one standard deviation.
Figure 4.6 shows the correlation of the acuity data with three retinal image quality
metrics: wavefront RMS, logarithm of VSOTF, and ICM.
Figure 4.6. (a) Wavefront RMS, (b) logarithm of VSOTF and (c) ICM plotted as a function of visual acuity for all subjects and optical conditions.
The ICM had the highest correlation (R2 = 0.81), whereas the poorest predictor of
visual performance was wavefront RMS (R2 = 0.34). These results are supported by the
finding of Chen et al.161, that retinal image quality metrics derived from the image plane,
such as the Strehl ratio, MTF, VSOTF and ICM are more representative of image quality
than metrics derived from the pupil plane, such as wavefront RMS.
The benefit of using the ICM over other metrics is its more accurate prediction of
visual acuity in the presence lower (defocus) and higher (spherical aberration) order
aberrations, as compared to traditional metrics of optical quality. Several previous
studies18, 20, 21 comparing traditional metrics found the VSOTF and area under the MTF
metrics to be better than other metrics, such as the Strehl ratio. The limitation of VSOTF
and area under MTF is that they fail to consider spatial phase shifts. Both these metrics
integrate the modulation transfer function, which is an all-positive quantity172 (see

83
equation 4.2). In this process, information of which spatial frequencies are phase shifted
is lost, however spatial phase shifts have a significant impact on image quality.
Alternatively, the two-dimensional cross-correlation of a reference and aberrated image
compares the phase in addition to the contrast of spatial frequencies173. This distinction
may contribute to ICMs superior estimation of visual acuity.
The first study, to our knowledge, which used an image convolution technique to
predict visual performance was published by Watson and Ahumada109 in 2008. Their
study used a similar paradigm to that presented above. However, their convolution
process included neural factors such as the neural contrast sensitivity function and neural
noise. The impact of taking the neural contrast sensitivity function (e.g. a low-pass filter
shown in Figure 1.15) and neural noise into account is to modify the spectral composition
of the reference image. Their study found that the image convolution based retinal image
quality metric was superior in predicting through-focus visual acuity to other metrics,
such as the VSOTF, area under the MTF, Strehl ratio, and wavefront RMS. Thus, their
findings were in agreement with ours, however they did not investigate the role of the
image used in the convolution.
To determine the role of the image used in the ICM, we manipulated the power
spectrum of the letter chart image by applying spectral filters. For each image, the
original amplitude spectrum was multiplied by fs, where f is the spatial frequency and s is
the slope factor. The slope factor, s, varied from -1.0 to +1.0 in 0.25 steps. Negative s
values acted as a low-pass filter, blurring the images. Positive s values acted as a high-
pass filter, sharpening the images. Two images were used in the analysis: a Snellen letter
chart and a natural scene of a camera man (Figure 4.7). By comparing the power spectra

84
of the unfiltered letter chart and cameraman images, it is clear the cameraman image has
less high spatial frequency content.
Figure 4.7. (a) Snellen letter chart and cameraman images and (b) power spectra with various slope filters (s). (c) Correlation of visual acuity with ICM computed with various slope filters.
Figure 4.7c shows the coefficient of determination (R2-value) between the visual
acuity data presented in Figure 4.5b and the ICM computed with both letter chart and
cameraman images with various slope filters. With the letter chart, the highest R2 value
(0.81) was found with a filter slope of 0. With the cameraman image, the highest R2 value

85
was found with a filter slope of 0.5. From this analysis, it is clear that images which lack
low spatial frequencies (negative slope filters) result in poor correlation of the ICM with
visual acuity. Conversely, if the slope factor is too high, as in the case of the letter chart
with a slope factor larger than 0, the correlation of ICM and visual acuity is compromised.
Therefore, the image used for ICM computation should be carefully selected, such that it
adequately contains both low and high spatial frequencies.
In conclusion, the ICM was used in subsequent sections of this thesis to as a
theoretical means of predicting visual performance under various optical conditions. This
metric can be used as a powerful tool to predict visual performance in the presence of
large aberrations (e.g. presbyopia, keratoconus, corneal transplant, etc.). This metric can
therefore be used in the design and optimization of optical systems which require an
extended depth of focus, such as, but not limited to, the presbyopic eye.
4.3 Optimizing Wavefront Aberrations for Increased Depth of Focus
The image quality metric presented in the previous section was used to optimize
the wavefront aberrations of the eye to extend the eye’s depth of focus with minimal
sacrifice of distance image quality. Specifically, we investigated the use of Zernike
primary and secondary spherical aberrations to induce a refractive multifocality to the
presbyopic ocular optics. First, a theoretical simulation was performed to assess the
impact of primary and secondary spherical aberration on through-focus image quality.
Subsequently, a monocular AO vision simulator, described section 4.2.2 and elsewhere136,
was used to validate the efficacy of the wavefront designs by measuring through-focus
visual performance in human subjects.

86
4.3.1 Higher Order Aberrations and Through-Focus Image Quality
We chose to use Zernike polynomials, an orthogonal set of mathematical
functions describing the topography of a circular aperture174, for describing the wavefront
aberrations of the eye. Zernike polynomials are typically defined in polar coordinates (ρ,
θ). The normalized radial pupil coordinate, ρ, ranges from 0 to 1 and is defined below,
where r and rmax represent the variable and maximal pupil radius in units of length:
maxr
r=ρ (4.5)
The azimuthal coordinate, θ, ranges from 0 to 2π. Zernike polynomials are defined as the
product of three terms: a normalization term, Nnm, a radial term, Rn
|m|(ρ), and an
azimuthal term A(mθ). The indices n and m refer to the highest order of Rn|m|(ρ) and the
sinusoidal frequency of A(mθ), respectively. The standard forms174 for Zernike
polynomials are defined as:
( )( ) ( )
( ) ( )
<⋅⋅−
≥⋅⋅=
0mfor ; sin
0mfor ; cos,
θρ
θρθρ
mRN
mRNZ
m
n
m
n
m
n
m
nm
n (4.6)
where,
( )
01
12
m
m
n
nN
δ+
+= (4.7)
and
( ) ( ) ( )( )( ) ( )( )∑
−
=
−
−−−+
−−=
2/)(
0
2
! 5.0 ! 5.0 !
! 1mn
s
sn
sm
nsmnsmns
snR ρρ (4.8)

87
In the normalization term, Nnm, δm0 is the Kronecker delta function, where:
≠
==
0m ; 0
0m ; 10mδ (4.9)
Increasing the eye’s depth of focus requires the use of wavefront aberrations with
a multifocal nature. Therefore, the wavefront aberrations of interest in this study were
Zernike defocus, primary spherical aberration and secondary spherical aberration, and are
defined below:
Defocus: [ ]123 202
02 −= ρCZ (4.10)
Primary Spherical Aberration: [ ]1665 2404
04 +−= ρρCZ (4.11)
Secondary Spherical Aberration: [ ]11230207 24606
06 −+−= ρρρCZ (4.12)
where Cnm is the magnitude coefficient of the corresponding polynomial. Zernike primary
spherical aberration is similar to the traditional Seidel definition of spherical aberration,
in that a positive quantity is defined as peripheral rays having a shorter focal length than
paraxial rays175. Conversely, negative spherical aberration (Seidel and Zernike) is defined
as the peripheral rays having a longer focal length than the paraxial rays. The definition
of Seidel spherical aberration is shown in equation 4.13:
( ) 4400ρρ WW = (4.13)
Where W(ρ) is the wavefront aberrations, W400 is the magnitude coefficient of Seidel
spherical aberration and ρ is the normalized pupil radius. Comparing Zernike (eq. 4.11)
and Seidel (eq. 4.13) spherical aberrations, it is clear that Zernike spherical aberration is
identical to the Seidel form, however it includes a negative quadratic defocus term (ρ2)

88
and multiplicative constants. An illustrative ray diagram of Seidel and Zernike spherical
aberrations is shown in Figure 4.8. The impact of the negative ρ2 term of Zernike
spherical aberration (equation 4.11) is visible in Figure 4.8 as a reduction in focusing
power of the lens.
Figure 4.8. Illustrative ray diagram of Seidel and Zernike spherical aberrations.
Figure 4.9 illustrates the ray diagrams of a lens with no aberrations, with positive
Zernike primary spherical aberration and positive Zernike secondary spherical aberration.
As seen in Figure 4.9, both Zernike primary and secondary spherical aberrations exhibit a
multifocal ray diagram, where radial zones of the lens aperture correspond to different
focal lengths. For the remainder of the thesis Zernike spherical aberrations will be used.

89
Figure 4.9. Ray diagram of an aberration-free lens, and a lenses with negative Zernike primary spherical aberration and negative Zernike secondary spherical aberration.
The wavefronts for defocus, primary and secondary spherical aberrations,
represented by equations 4.10 – 4.12 are shown in Figures 4.10 (b-d), respectively. The
wavefront profiles and their cross-sectional profiles (black lines) were computed over a
4.0 mm pupil and with equal magnitude of +0.25 µm.

90
Figure 4.10. Wavefront aberration maps and their cross-sectional profile (black-lines) for (a) an aberration-free 4.0 mm pupil and pupil with +0.25 µm of (b) Zernike defocus, (c) primary spherical aberration and (d) secondary spherical aberration.
The corresponding through-focus retinal image quality curves are shown below in
Figure 4.11. From this Figure, the impact on through-focus retinal image quality of the
aberrations in isolation can be observed. Inducing Zernike defocus produced a shift in
best focus without affecting peak image quality. The shift in best focus can be calculated
based on the following conversion of micrometers to diopters of defocus112:
2max
02 34
Dioptersr
C= (4.14)
where the magnitude of Zernike defocus (C20) is in units of microns and the maximum
pupil radius (rmax)is in units of millimeters. Alternatively, induction of primary and
spherical aberration produced a shift in best-focus, in addition to a decrease in peak
image quality. The broadening of the through-focus retinal image quality curve due to
both spherical aberrations indicates the increase in the depth of focus.

91
Figure 4.11. Through-focus retinal image quality for a 4.0 mm pupil with various wavefront aberrations.
As discussed previously, it is customary in clinical practice to optimize visual
quality for distant objects. Therefore, induction of spherical aberrations would be
accompanied by the appropriate magnitude of defocus to shift the through-focus image
quality curve, thereby maximizing distance image quality. The amount of defocus
required to optimize distance image quality in the presence of spherical aberrations may
be determined computationally7, 37, 38 or psychophysically28, 176. A Matlab program was
used to determine the shift in best-focus caused by induction of primary and secondary
spherical aberration (Figure 4.12).
Through-focus retinal image quality for various magnitudes of primary and
secondary spherical aberration is shown in Figure 4.12. Through-focus retinal image
quality from -6.0 to +6.0 D was computed for an aberration-free model eye with primary
and secondary spherical aberration ranging from -0.4 to +0.4 µm over a 4.0 mm pupil.

92
Figure 4.12. Through-focus retinal image quality for a 4.0 mm pupil with (a) primary and (b) secondary spherical aberration. (c) and (d) correspond to through-focus retinal image quality with primary and secondary spherical aberrations, respectively, with the peak shifted to 0 diopters.
As shown in Figure 4.12, primary spherical aberration causes a larger shift in best
focus as compared to secondary spherical aberration. The magnitude of best-focus shift
was in agreement with previous studies59, 175, 177. If distance image quality is not

93
optimized, negative primary and secondary spherical aberrations lead to better
intermediate and near image quality as compared to positive spherical aberrations.
When peak image quality is shifted to 0.0 D, then positive primary and secondary
spherical aberration yield superior intermediate and near image quality as compared to
the aberration-free case, as shown in Figure 4.12c and d. Secondary spherical aberration
produced a bimodal through-focus retinal image quality pattern with two distinct peaks.
The dioptric separation of the two peaks scaled with magnitude of secondary spherical
aberration.
Figure 4.13a shows the degradation in peak retinal image quality in the presence
of spherical aberrations. To optimize the combination of primary and secondary spherical
aberrations, the through-focus ICM was averaged from 0.0 to 2.5 D to provide a single-
value metric for through-focus retinal image quality. Figure 4.13b shows the single value
metric various combinations of primary and secondary spherical aberrations. In isolation,
+0.28 and 0.20 µm of primary and secondary spherical aberrations, respectively,
maximized through-focus image quality and are represented by the white squares in
Figure 4.13b. However, their combination offers a larger range of potential wavefront
designs for extended depth of focus. The range of optimal combinations of primary and
secondary spherical aberrations is indicated with the dotted white ellipse in Figure 4.13.

94
Figure 4.13. Two-dimensional distribution of (a) peak retinal image quality and (b) area-under-through-focus image quality, from 0.0 to 2.5 D, with primary and secondary spherical aberrations.
In this study, four wavefront inductions were examined psychophysically. The
aberration induction conditions consisted of primary spherical aberration only

95
(C40=0.28µm), secondary spherical aberration only (C6
0=0.20µm), a combination of
primary and secondary spherical aberration (C40=0.10µm and C6
0=0.15µm, represented
by the thick white box in Figure 4.13), and an aberration-free case (C40=C6
0=0µm) for
comparison. Theoretical through-focus image quality for these four conditions and an
example convolved image of a 20/40 letter ‘E’ is shown in Figure 4.14.
Figure 4.14. (a) Theoretical through-focus retinal image quality and (b) convolved 20/40 Snellen letters for optimal magnitudes and combination of primary and secondary spherical aberrations.
4.3.2 Through-Focus Visual Performance with Spherical Aberrations
To validate the theoretical investigation, an adaptive-optics vision simulator was
used to measure monocular high-contrast visual acuity in 3 subjects (average age: 26+3
years). The research presented in this section was approved by University of Rochester
Research Review Board. All subjects signed an informed consent form and underwent a
clinical eye exam prior to participation in this study. All procedures involving human
subjects were in accordance with the tenets of the Declaration of Helsinki.
Subjects were cyclopleged with 1% tropicamide solution to dilate the pupil and
paralyze accommodation167. Visual acuity was measured from distance to near in 0.5 D

96
steps in white light. While the subjects viewed through a 4.0 mm pupil for vision testing,
the AO system corrected subjects’ native lower and higher order aberrations and induced
defocus and spherical aberrations for vision testing. The AO system manipulated
aberrations over a 4.5 mm pupil, whereas subjects viewed the stimulus through a 4.0 mm
artificial pupil. This method was employed to minimize edge effects from the wavefront
correction of the deformable mirror. The same procedure outlined in section 4.2.2 was
used to measure high-contrast visual acuity.
The through-focus visual acuity results are shown below in Figure 4.15. In the
aberration-free case, distance visual acuity was maximized at -0.24+0.10 logMAR.
Visual acuity rapidly declined with defocus, at an approximate rate of 3 lines (0.3
logMAR units) per diopter. Induction of spherical aberrations marginally reduced
distance acuity, however only the secondary spherical aberration condition produced a
statistically significant degradation of 1.4 lines (p=0.03, paired Student’s t-test).
Figure 4.15. Through-focus monocular visual acuity measured in 3 cyclopleged subjects.
As seen in Figure 4.15, induction of primary and secondary spherical aberrations
can significantly improve through-focus visual performance. Primary spherical aberration
improved intermediate acuity (0.5-2.0 D), whereas the secondary spherical aberration

97
condition had a larger improvement of near acuity (1.5-4.5 D). Positive secondary
spherical aberration resulted in a bimodal through-focus visual acuity trend, with a near
peak in acuity at 2.0 D. For distances between 0.0 and 2.0 D, combining primary and
secondary spherical aberration provided an average benefit in acuity of 0.13+0.17
logMAR, as compared to the primary only or secondary only spherical aberration
(0.02+0.08 and 0.05+0.22 logMAR, respectively). Through-focus visual acuity was well-
predicted by the ICM (R2 = 0.80), as can be seen by comparing Figures 4.14 and 4.15.
4.3.3 Discussion
These findings were in agreement with several previous studies38, 39, 41. Benard et
al.176, 178 evaluated subjective depth of focus and found a benefit of primary and
secondary spherical aberrations. Yi et al.28 measured through-focus visual acuity and
concluded that primary and secondary spherical aberrations should be of opposite signs to
have the greatest positive impact on depth of focus. Our study showed the opposite trend,
that when secondary spherical aberration remained positive, the both signs of primary
spherical aberration improved through-focus retinal image quality, as indicated by the
dotted white ellipse in Figure 4.13. This discrepancy is due to Yi et al.’s definition of
depth of focus. In their study, depth of focus was defined as the full dioptric range for
which a retinal image quality metric (the visual Strehl ratio) was above a chosen
threshold. However, this definition is not practical, due to the clinical convention of
optimizing distance image quality. In the realistic case, defocus vergences “beyond
infinity” correspond to imaginary objects (existing in the image space) and are therefore

98
are not utilized. Alternatively, our study only considered object distances from peak
image quality (defined as distance) to near.
Benard et al.176, 178 assessed the subjective depth of focus in the presence of
primary and secondary spherical aberrations. The subjectively determined depth of focus
was based on a judgment of the limit of objectionable blur179. These studies also found
that appropriate combinations of primary and secondary spherical aberrations led to
significant increases in depth of focus, however subjective depth of focus was poorly
predicted by retinal image quality metrics.
To better understand the impact of higher order aberrations on through-focus
image quality, it is helpful to consider the Zernike power polynomial168, 170. The Zernike
power polynomials describe the distribution of refractive power across a wavefront
aberration, as determined by the wavefront’s local curvature. The expression for the
pupil’s power distribution is shown below:
( ) ( )dr
rdW
rr
1=Φ (4.15)
In the case of a wavefront, W(r) with defocus and primary and spherical aberrations, the
power map is expressed as follows:
( )
+
−+
−+=Φ 115
72412
512342
2
2
2
2
062
2
2
042
02
R
r
R
r
RC
R
r
RC
RCr (4.16)
The wavefront height, W(r), and power distribution Ф(r), for the conditions described are
shown below in Figure 4.16.

99
Figure 4.16. (a) Wavefront height and (b) refractive power distribution of the aberration profiles tested for presbyopic correction.
The value of the power profile is to visualize the distribution of refractive power
across the pupil in the presence of spherical aberrations. This is especially beneficial
when considering changes in pupil size during accommodative effort. The power
distribution has also been previously shown to be useful for determining the objective
refraction (i.e. best sphere and cylinder correction) from a wavefront profile168.
From the power profiles shown in Figure 4.16b, it can be seen that primary
spherical aberration has a 2nd order power distribution, with the central zone allocated for
distance vision and the periphery for near vision. Alternatively, secondary spherical
aberration has a 4th order power distribution, with the near zone of the pupil distributed at
the center and the margin of the pupil, with a peak add-power of 3.8 D. The combination
of primary and secondary spherical aberration had a central zone for intermediate vision
(2.1 D) with the pupil margin containing the near add-power (3.5 D).
An advantage of combining primary and secondary spherical aberrations is their
distribution of near add-powers both at the center and margin of the pupil. As discussed

100
in chapter 2, the pupil constricts during accommodative effort. Therefore, positive
primary spherical aberration designs may not be optimal for a subject whose pupil has
significant magnitude of miosis. In this case, during near viewing, the pupil would
constrict, thereby obstructing the pupillary region with near-add power168. Conversely,
this same subject’s near image quality would improve during pupillary miosis in the case
of secondary and combination of primary and secondary spherical aberrations due to the
central near-add zone of the pupil.
The wavefront approach to correcting presbyopia has its own set of limitations.
The foremost limitation, as discussed above, is the trade-off in peak image quality in the
presence of spherical aberrations10, 39, 43, 44. A practical challenge is the centration of
wavefront profiles, whether they are implemented with contact lenses, refractive surgery,
corneal inlays or IOLs. Previous studies55-57 have shown that decentration of spherical
aberrations induces rotationally asymmetric aberrations such as astigmatism, coma and
trefoil, which degrade retinal image quality.
In conclusion, we have shown that the ICM is the optimal tool for understanding
the interaction and consequences of primary and spherical aberrations upon through-
focus retinal image quality. Furthermore, using an adaptive optics vision simulator, we
have shown that the wavefront approach to presbyopic correction is promising in
significantly increasing the eye’s depth of focus, albeit at the expense of a reduction in
peak image quality. Finally, appropriate combinations of primary and secondary spherical
aberrations are more effective at increasing depth of focus than primary or secondary
spherical aberrations alone.

101
4.4 Interaction of Transmission Apodization and Higher Order
Aberrations
4.4.1 Introduction
Induction of higher order aberrations can significantly increase depth of focus,
relieving presbyopes’ spectacle dependence for far and near vision. However, as shown
in Figure 4.13a, this effect is accompanied by a reduction in peak image quality. Previous
investigations have shown that eyes with multifocal corrections experience reduction in
contrast sensitivity180, 181 and photic phenomena, such as halos and glare129, 182. These
side-effects are further exacerbated in low light conditions, such as night driving, when
the pupil enlarges to collect more light.
In the previous section, we showed how the imaginary component of the eye’s
pupil function, wavefront phase, can be manipulated to achieve multifocality. However,
altering the real component, the transmission function, offers an additional degree of
freedom for optimizing through-focus optical quality. In this section, we investigate the
combination of wavefront multifocality with pupil transmission apodization.
Figure 4.17 illustrates the transmission function, T(r), of the pupil with various
magnitudes of apodization as defined by equation 4.16, where r is the pupil radius and α
is the apodization coefficient.
2
10)( rrT α−= (4.16)

102
Figure 4.17. Intensity transmission profiles with varying degrees of apodization within a 4.0 mm pupil.
4.4.2 Through-Focus Image Quality with Combined Apodization and Higher
Order Aberrations
To assess the interaction of transmission and phase manipulation of the eye’s
pupil function on through-focus retinal image quality, theoretical and psychophysical
studies were performed. For the theoretical portion, the ICM was used to compute
through-focus retinal image quality for various combinations of pupil apodization and
multifocal wavefront aberrations (primary spherical aberration). Subsequently, a vision
simulator equipped with a spatial light modulator was used to measure through-focus
visual acuity to validate the theoretical results.
Through-focus retinal image quality was evaluated from 0.0 to 3.0 D with the
ICM in monochromatic light (555 nm) for a 4.0 mm pupil diameter. The apodization
coefficient was varied from 0.0 to 0.5 mm-2 and Zernike primary spherical aberration was
varied from -0.5 to 0.5 µm for each magnitude of apodization. The results of the
theoretical simulation are shown at 0.0, 1.5 and 3.0 D object distances in Figure 4.18.

103
Figure 4.18. Theoretical retinal image quality at (a) far, (b) intermediate and (c) near object distances.

104
In a diffraction-limited optical system, pupil apodization reduces image quality
due to an attenuation of high spatial frequencies in the modulation transfer function183. As
seen in Figure 4.18, in the presence of positive and negative spherical aberration, pupil
apodization has a significant impact on retinal image quality. At distance (Figure 4.18a),
image quality in the presence of spherical aberration improved as the apodization
coefficient increased. This trend was the same for both positive and negative spherical
aberration. However, for intermediate and near distances, the sign of spherical aberration
did affect pupil apodization’s impact on image quality. For example, intermediate and
near image quality both improve in the presence of negative spherical aberration as
apodization increased. Conversely, apodization reduced intermediate and near image
quality in the presence of positive spherical aberration. This is further illustrated in
Figures 4.19 (a-c), where through-focus retinal image quality is plotted for 0, +0.2 and -
0.2 µm of primary spherical aberration. No apodization is shown in blue curves
(α=0.0mm-2) and the case with apodization (α=0.3mm-2). For comparison, apodization
corresponding to the Stiles-Crawford effect (α=0.05mm-2) is represented by the thin
black line. Figure 4.19d shows the through-focus visual benefit of apodization, defined as
the percent change in retinal image quality due to apodization at each level of defocus.

105
Figure 4.19. Through-focus retinal image quality with (a) 0, (b) +0.2 and (c) -0.2 µm of primary spherical aberration. (d) Through-focus visual benefit of apodization.
This observation can be understood by considering the parabolic power
distribution of the pupil in the presence of primary spherical aberration (Figure 4.16b).
Positive and negative spherical aberrations differ in that the central pupillary region is
either allocated to distance or near focal lengths, respectively. Therefore, the sign of
spherical aberration plays an important role on the effect of apodization, wherein the
transmission of the pupil’s periphery is penalized.
4.4.3 Through-Focus Visual Performance with Combined Apodization and
Higher Order Aberrations
The research presented in this section was approved by University of Rochester
Research Review Board. All subjects signed an informed consent form and underwent a

106
clinical eye exam prior to participation in this study. All procedures involving human
subjects were in accordance with the tenets of the Declaration of Helsinki.
A vision simulator (Figure 4.20), described in detail elsewhere170, was used to test
through-focus monocular visual performance in 3 subjects (average age: 28+1 years) in
the dominant eye. Cyclopentolate hydrochloride (1%) was used to dilate the pupil and
paralyze accommodation167. Subjects’ native aberrations were within the normal age-
matched range184: higher order root-mean-square of 0.09+0.02 µm and 0.03+0.02 µm of
primary spherical aberration for a 4.0 mm pupil.
Subjects’ alignment was maintained with a 3-axis translational stage mounted
dental impression bit-bar and a camera focused on the eye’s pupil plane. A Badal
optometer was used to adjust the target vergence for through-focus vision testing. A
liquid-crystal-on-silicon (X10468, Hamamatsu Photonics, Hamamatsu City, Japan)
spatial light modulator conjugate to the pupil plane and situated between two crossed
linear polarizers manipulated the eye’s transmission profile and induce the apodization
profiles. The spatial light modulator alters a beam’s intensity profile by locally rotating
the plane of polarization before the beam is directed to a linear polarizer. The
transmission through the linear analyzer is determined by the relative orientation of its
transmission axis with the polarization of the incident beam.
An artificial pupil with a 4.0 mm diameter was used for all optical conditions.
Spherical aberration was induced via phase plates located in a plane conjugate to the
pupil. The visual stimulus was presented with a digital light processor (LightCommander,
Texas Instruments, Dallas, Texas) and rendered monochromatic (λ = 550+5 nm) with an
interference filter.

107
High-contrast visual acuity was measured following a procedure similar to that
described in section 4.2.2. Visual acuity measured in the presence and absence of
apodization (α = 0.3 and 0.0 mm-2) for spherical aberration magnitudes of 0.0, +0.2 and -
0.2 µm.
Figure 4.20. Schematic of vision simulator.
Theoretical and measured cross-section of the reflectance profile of the spatial
light modulator surface with an apodization profile is shown in Figure 4.21a. Figure
4.21b shows a high correlation (R2=0.991) between input signal and measured reflectance
profile of spatial light modulator surface.

108
Figure 4.21. (a) Cross-sectional profile of theoretical and experimental reflectance profile of spatial light modulator surface. (b) Correlation between spatial light modulator input and output.
Average through-focus visual acuity is shown below in Figure 4.22. Asterisks
denote a statistically significant difference (p<0.05) between acuities with and without
apodization at a given level of spherical aberration and target vergence. Through-focus
visual benefit, defined as the difference in acuities with and without apodization
summarizes this result, and is shown in Figure 4.22d. Positive values refer to an
improvement in VA due to apodization, whereas negative values refer to a degradation.

109
Figure 4.22. Average through-focus visual acuity for 3 subjects with (a) 0, (b) +0.2 and (c) -0.2 µm of primary spherical aberration with (red curve, α=0.3mm-2) and without (blue curve, α=0.3mm-2) pupil transmission apodization. Through-focus visual benefit, defined as the difference in acuity for with and without apodization conditions is shown in (d). Error bars signify one standard deviation.
Visual performance testing confirmed the theoretical results and was well-
predicted by the image convolution metric (R2 = 0.85). Apodization improved through-
focus acuity in the presence of zero and negative spherical aberration induction, however
acuity worsened with apodization in the presence of positive spherical aberration.
For all spherical aberration conditions, distance acuity was -0.2 logMAR and was
not significantly impacted by apodization. In the zero spherical aberration condition
(Figure 4.22a), apodization resulted in a significant visual benefit of approximately 1.5
lines of acuity at intermediate and near vergences. A similar benefit of apodization was
observed in the negative spherical aberration condition (Figure 4.22c). However, with

110
positive spherical aberration (Figure 4.22b), apodization degraded acuity by
approximately one line at 1 and 2 D of target vergence.
4.4.4 Discussion
It is well-known that the eye has an intrinsic apodization function. This arises
from the waveguiding nature of the retinal photoreceptors, and is known as the Stiles-
Crawford effect185. Applegate and Lakshminarayanan166 found an average factor of
α=0.05mm-2 in a large population of healthy eyes. This leads to a reduction in
transmittance at the edge of 4, 6 and 8 mm pupils of 37%, 65% and 84%, respectively.
Previous studies186, 187 found positive visual impact of the Stiles-Crawford effect to be
limited to relatively large pupils.
Our study found that pupil transmission apodization led to a significant impact on
through-focus retinal image quality and visual acuity for a pupil size relevant to the
presbyopic population. Due to senile miosis, under normal photopic conditions, the
typical pupil sizes117, 118 found in presbyopes (3.0-5.0 mm) is too small for the Stiles-
Crawford effect to have a significant impact on vision. Our study shows that presbyopes
with extended depth of focus optical corrections stand to gain from an artificial pupil
apodization. Pupil apodization techniques would be best applied to contact or intraocular
lenses, as the gaze-dependency of spectacles poses a significant limitation. Decentration
of the pupil from the center of the apodization profile causes vignetting and loss of visual
field.
Our findings are in agreement with previous studies63-66. Zhang et al.186, Mino and
Okano188, and Atchison et al.189 found that pupil apodization improved through-focus

111
retinal image quality in monofocal optical systems. Visual tasks such as acuity or viewing
natural scenes rely on a broad bandwidth of spatial frequency and are particularly
sensitive to spatial phase shifts190.
Previous studies have also shown that correcting the phase effects caused by
optical blur (i.e. phase-rectification) significantly improves visual acuity171, 191. Although
apodization does not phase-rectify the retinal image, it does improve through-focus
retinal image quality by increasing contrast and shifting the first phase reversal of the
optical transfer function to higher spatial frequencies. For example, 1.0 D of defocus in
an otherwise diffraction-limited system with a 4.0 mm pupil results in the first phase
reversal of the optical transfer function occurs at approximately 5.6 cyc/deg. However, in
the presence of pupil apodization (α=0.3 mm-2), the first phase reversal occurs at
approximately 9.1 cyc/deg, a factor of 1.63 increase in spatial frequency. The
corresponding modulation transfer functions are plotted in Figure 4.23. The red and blue
arrows indicate the first phase reversals for the with and without apodization conditions,
respectively.

112
Figure 4.23. Modulation transfer functions of 1.0 D of defocus with (red) and without (blue) pupil apodization). Arrows indicate the first phase reversals for apodization conditions.
A limitation of this study was that all vision testing conditions was performed at
luminance matched conditions. However, the chosen magnitude of pupil apodization
(α=0.3 mm-2) reduces retinal illuminance for a 4.0 mm pupil by approximately 60%.
Despite retinal cone photoreceptors’ more than four orders of magnitude of gain control
for photopic vision192, reduction in retinal illuminance is well known to degrade spatial
vision193, 194. Future work is needed to determine the safety of pupil apodization,
particularly in low light levels.

113
4.5 Summary
In conclusion, we have shown that the eye’s depth of focus may be significantly
increased by manipulating the wavefront aberration with higher order aberrations and
pupil apodization. However, despite the recovery of through-focus acuity, the
pseudoaccommodation approach of increasing depth of focus is not a replacement for
true restoration of dynamic accommodation. Increasing the eye’s depth of focus causes a
decrease in peak image quality and contrast, as shown in Figure 4.13a.
Despite the well-known drawbacks of the multifocal approach to presbyopic
correction, it is possible to minimize the side-effects via optimization of appropriate
variables, such as spherical aberrations and pupil amplitude apodization. This research
proposes the use of a robust image quality metric, the image convolution metric, as a tool
for accurately predicting through-focus visual performance in the presence of multifocal
corrections. In addition, we have shown that the magnitudes of higher order aberrations
and pupil apodization interact to significantly impact visual performance and need to be
selected carefully.

114
Chapter 5. Modified Monovision: A Binocular
Approach To Presbyopia Correction
5.1 Introduction
We have shown that through-focus visual performance in presbyopia can be
significantly improved by manipulating wavefront multifocality and pupil apodization.
As discussed previously, extension of the depth of focus also results in a trade-off in
distance image quality. Furthermore, the majority of previous investigations of
presbyopia correction have focused on monocular optical designs, failing to incorporate
the binocularity of the visual system. In this chapter, a binocular approach towards
presbyopia correction is investigated. By leveraging the dual channel nature of the
binocular visual system, a new range of possibilities for presbyopic correction becomes
available.
A familiar presbyopic correction which makes use of the binocular visual system
is monovision. In traditional monovision, the dominant eye is assigned to distance vision,
and the fellow, non-dominant, eye is assigned to near vision via a monocular induction of
optical power (i.e. anisometropia)54, 66, 195. The degree of anisometropia varies clinically,
typically ranging from 1-2 D55, 66. It has been shown that anisometropia greater than 1
diopter is effective for improving distance-corrected near visual acuity, however, with
anisometropia greater than 2 D, intermediate visual performance and binocular visual
function is significantly degraded30, 55.
Success rates with traditional monovision in contact-lens wearers is
approximately 80%, after excluding contact lens related failures195. Review of the

115
literature54, 66, 195 indicates primary limitations of traditional monovision are reduction in
binocular visual functions, such as binocular contrast summation and stereopsis.
Additionally, poor intermediate image quality and interocular suppression of blur pose
challenges to the monovision patient.
Figure 5.1 shows through-focus retinal image quality for both eyes in traditional
monovision with an anisometropia of 1.5 D. As can be seen from this figure, the
dominant and non-dominant eyes have peaks in retinal image which occur at distinct
object distances.
Figure 5.1. Monocular through-focus retinal image quality in traditional monovision.
Visual functions which rely on the binocular input include binocular summation
and stereopsis. As discussed previously, binocular contrast summation of approximately
42% is observed when the eyes have equal and optimal optical quality48, 49. This result
has been expanded with the quadratic summation model, proposed by Gordon Legge196,
shown below.
( ) ( )22
RLB CCC += (5.1)

116
Where CB, CL and CR are the contrast thresholds for viewing binocularly, with the left eye
and with right eye, respectively. This model predicts the summation factor found by
Campbell and Green48 and the loss in binocular contrast summation as the optical quality
between the two eyes differs9-12. This was shown experimentally by Pardhan and
Gilchrist, who measured contrast sensitivity at 6 cyc/deg as a function of induced
anisometropia. Their results, shown in Figure 5.2, reveal the steady loss of summation
with anisometropia, leading to inhibition.
Figure 5.2. Binocular contrast summation at 6 cyc/deg as a function of anisometropia (Pardhan and Gilchrist, 1990)197.
In addition to the loss of binocular contrast summation, anisometropia also
debilitates stereopsis. Due to the interpupillary distance, the two eyes have distinct
vantage points, leading to perspective-dependent differences in the retinal images, giving
rise to the sensation of depth. Filippini and Banks52 proposed a model which describes
stereopsis as a local cross-correlation of retinal images to determine stereopsis. It follows
that as optical quality is degraded in one or both retinal images, the local cross-
correlation becomes less reliable, impairing depth perception in traditional monovision52-

117
55, 66, 195, 198. The impact of monocular defocus on stereoacuity is shown previously in
Figure 1.853.
Therefore, traditional monovision compromises binocular visual function (e.g.
binocular summation and depth perception) due to the large difference in interocular
retinal image quality, caused by anisometropia and short monocular depth of focus.
5.2 Modifying Monovision with Monocular Spherical Aberration
To overcome the limitations of traditional monovision, we propose a new
approach, modified monovision, in which spherical aberration is used to extend the depth
of focus of each eye. By increasing monocular depth of focus, binocular retinal image
quality is improved in addition to reducing the difference in interocular retinal image
quality at each object distance.
Modified monovision may be achieved with a variety of modalities for spherical
aberration induction in one or both eyes. For example, Reinstein et al.199-201 have
proposed the use of nonlinear aspheric corneal ablation in refractive surgery with the
intent of inducing spherical aberration and anisometropia for a modified monovision
outcome. Due to the nature of LASIK, this surgical technique leaves patients going into
the surgery who were previously hyperopic with residual negative spherical aberration,
and myopic patients with residual positive spherical aberration202.
With the development of presbyopic corrections, such as contact lenses, corneal
inlays, corneal refractive surgery, and IOLs, it is increasingly important to understand the
mechanism of binocular vision with such tools. It was the goal of this study to investigate
the impact of modified monovision on through-focus visual performance.

118
Additionally, we examined the optimization of modified monovision variables
using the ICM to improve through-focus visual performance. Compared to other
pseudoaccommodation strategies, modified monovision offers the opportunity to take
advantage of the binocular visual system by treating each eye as an independent design
parameter.
5.2.1 Theoretical Modeling of Binocular Through-focus Retinal Image
Quality
To investigate the impact on through-focus visual performance of modified
monovision, we performed a theoretical and psychophysical analysis of various
magnitudes of positive and negative primary spherical aberration (+0.2 and +0.4 µm over
a 4.0 mm pupil) in the non-dominant eye while the dominant eye was fully corrected for
distance. Anisometropia of 1.5 D was constant for all modified monovision conditions.
Traditional monovision (i.e. no spherical aberration) was included for comparison as a
control.
Monocular through-focus retinal image quality for each eye was computed
independently using the image convolution based retinal image quality metric (ICM)
described in chapter 4. In this investigation, we used the polychromatic adaptation of the
metric19, 20. This was accomplished by convolving the reference image with a
polychromatic point spread function, which consisted of the sum of monochromatic point
spread functions from 405 to 695 nm wavelength, weighted by the photopic spectral
sensitivity function, Vλ. The expression for the polychromatic point spread function is
shown in equation 5.2.

119
( )( ) ( )
( )λ
λλ
λλ
λλ
∑
∑
=
==nm
nm
mono
nm
nmpoly
V
yxPSFV
yxPSF695
405
695
405
,,
, (5.2)
Monocular through-focus retinal image quality for the modified monovision
conditions is shown in Figure 5.3. Both Figures 5.3a and 5.3b have aberration-free curves
depicting the dominant (DE, black solid line) and non-dominant (NDE, solid line) in
traditional monovision. Figure 5.3a also shows the monocular through-focus retinal
image quality trends for modified monovision with positive and negative 0.2 µm of
primary spherical aberration (dotted and dashed red lines, respectively) in the non-
dominant eye. Similarly, Figure 5.3b shows monocular through-focus retinal image
quality for modified monovision with positive and negative 0.4 µm of primary spherical
aberration (dotted and dashed blue lines, respectively) in the non-dominant eye.
To obtain a single-value retinal image quality metric to characterize binocular
visual performance at each object distance, interocular blur suppression was incorporated
into the model. Binocular summation was not incorporated into the binocular ICM
because the purpose of the ICM metric was to predict high-contrast visual performance,
which is subject to minimal binocular summation. Visual acuity is approximately equal to
the cutoff frequency of the contrast sensitivity function. Although contrast sensitivity
improves by 42% due to summation, this results in a shift in cutoff frequency of
approximately 10%, as shown by Cagenello et al.50. Furthermore, as the eyes’ retinal
image quality begins to differ, the acuity summation factor is expressed to further
decrease.

120
Therefore, at each through-focus position, the superior of the two eye’s image
quality metric value was taken to represent a single binocular metric value. Through-
focus binocular retinal image quality is shown in Figure 5.3c. In addition, the interocular
difference in image quality between the dominant and non-dominant eyes was computed
at each level of defocus for a given monovision condition and is shown in Figure 5.3d. A
zero value indicates the two eyes have identical image quality.
Figure 5.3. Theoretical simulation of retinal image quality. (a) and (b) show monocular through-focus retinal image quality in traditional (TMV) and modified monovision (MMV) with +0.2 and +0.4 µm of primary spherical aberration in the non-dominant eye, respectively. (c) Binocular through-focus retinal image quality. (d) Interocular difference in through-focus retinal image quality; (c) and (d) share a common legend

121
As shown in Figure 5.3, induction of spherical aberration in the non-dominant eye
increases binocular depth of focus and reduces the difference in interocular image quality
at distance and intermediate object distances. However, the sign of the non-dominant eye
spherical aberration determines the trade-off between binocular depth of focus (supports
near acuity) and interocular difference in retinal image quality (supports binocular
summation and stereopsis). This trade-off arises from the asymmetric nature of through-
focus image quality in the non-dominant eye in the presence of spherical aberration175.
Negative spherical aberration induction decreased the difference in interocular
retinal image quality, particularly at distance, as shown in Figure 5.3d. It also led to a
slight improvement in near retinal image quality. On the other hand, positive spherical
aberration significantly improved near retinal image quality at the expense of lesser
benefit in interocular image quality difference at distance.
5.3 Binocular Through-Focus Visual Performance
To investigate binocular visual performance under various modified monovision
conditions, it is critical to simultaneously control and manipulate both eyes’ wavefront
aberrations. To achieve this, a binocular adaptive optics vision simulator was developed.
5.3.1 Binocular Adaptive Optics Vision Simulator
A system schematic is shown in Figure 5.4. The binocular adaptive optics vision
simulator consists of two monocular systems operating simultaneously, and is described
in detail elsewhere59. Each monocular adaptive optics vision simulator is comprised of

122
several key components: the wavefront correction/induction device, wavefront
measurement device and the visual stimulus.

123
Figure 5.4. Binocular adaptive optics vision simulator schematic. LE: left eye; RE: right eye; TS: translational stage for interpupillary distance; LED: infrared light emitting

124
diodes for pupil illumination; PC: pupil camera for subject alignment; PH: 800 µm diameter pinhole; SLD: super-luminescent diode (λ = 840+20 nm); PHR: phoropter; FL: fusion lock; DM: deformable mirror; BO: Badal optometer; DF: dichroic filter; SHWS: custom-made Shack-Hartmann wavefront sensor; AP: artificial pupil; DLP: digital light processor; L1 and L2: 200 mm focal length achromatic doublet lenses; L3 and L6: 150 mm focal length achromatic doublet lenses; L4 and L5: 350 mm focal length achromatic doublet lenses; L7: 180 mm focal length achromatic doublet lens.
Pupil cameras (PC) were used to align subjects’ left and right eyes in the vision
simulator. A dental-impression bite bar mount mounted to a translational stage was used
to stabilize head movements. Translational stages (TS) were used to account for
intersubject variation of interpupillary distance, typically ranging from 50 to 80 mm in
the normal population51. To aid in maintaining fusion, artificial apertures subtending 4
degrees conjugate to the subjects’ retinal planes were used as peripheral fusion locks (FL).
To accurately measure and manipulate the wavefront aberrations of the eye’s exit
pupil, the Shack-Hartmann wavefront sensor and deformable mirror were made conjugate
to the eye’s pupil, similar to the monocular adaptive-optics vision simulator described in
the previous chapter. As illustrated in Figure 5.4, this is accomplished by optical relays of
the pupil plane using achromatic doublet lenses in a “4-f” configuration.
Each custom-made Shack-Hartmann wavefront sensor consisted of a lenslet array
(Adaptive Optics Associates; Cambridge, Massachusetts) located at a plane conjugate to
the eye’s exit pupil with unitary magnification. The lenslet array consisted of 5.4 mm
focal length lenslets with 203 µm spacing. A charge-coupled device (CohuHD, Poway,
California) with 7.4 µm pixel size imaged the spot array pattern produced by the lenslet
array. The displacement of each lenslet spot corresponds to the local wavefront slope203
across the surface of the lenslet. The wavefront aberrations were computed from the local
slopes and expressed in terms of Zernike coefficients up to the 10th order according to

125
ANSI Z80.28-2004 standard174. The light source for wavefront sensing was a super-
luminescent diode (SLD) with central wavelength of 840 nm and a full-width half-
maximum of 40 nm operating at approximately 15 µW of incident power at the pupil,
well below the maximum permissible exposure (ANSI Z136.1-2007).
Figure 5.5a shows a verification of the Shack-Hartmann wavefront sensor
measurement of defocus induced by the Badal optometer. The Badal optometers induced
-4.0 to +4.0 D of defocus in 0.5 diopter increments by adjusting the separation between
L5 and L6 by axially translating the prism shown in Figure 5.4. The prism was mounted
on a computer-controlled motorized translation stage (Velmex Inc., Bloomfield, New
York). The Badal optometer’s telecentricity is critical for through-focus vision testing, as
the magnification of the visual stimulus remains constant. Figure 5.5b shows the residual
error, defined as the difference between induced and measured defocus for both
wavefront sensors.
Figure 5.5 (a) Left and right eye system wavefront sensors’ measurement of +/- 4 D of defocus induced by the Badal optometers and (b) the residual error.
The custom-built Shack-Hartmann wavefront sensors were designed for optimal
performance for pairing with the deformable mirror of the adaptive optics system204, 205.

126
The lenslet array of the wavefront sensor was chosen such that the lenslet to deformable
mirror actuator ratio was 3.1. This ensured a stable adaptive optics correction by
minimizing the condition number of the adaptive optics response matrix206. Previous
work by Alf Dubra205 has shown that the number of wavefront sensor lenslets assigned to
each actuator has a significant impact on adaptive optics correction performance, with a
minimum lenslet to actuator ratio of approximately 2.
Each monocular system was equipped with a continuous-sheet, 97-actuator
magnetic membrane deformable mirror (DM97, ALPAO; Montbonnot, France) to serve
as the wavefront control device. The deformable mirror had a clear aperture of 16.5 mm,
corresponding to a de-magnified 7.0 mm ocular pupil. Figure 5.6 illustrates the layout of
deformable mirror actuators corresponding to various eye’s pupil sizes.
Figure 5.6. Various pupil sizes (colored circles) overlaid with the deformable mirror’s 97 actuators (grey boxes).
As shown in Figure 5.6, approximately 6 actuators run along the diameter of a 4.0
mm pupil. To induce a wavefront aberration with a deformable mirror, at least 2n+1
actuators are required to induce an aberration of nth radial order. For example three

127
actuators are required to induce defocus, a 2nd order polynomial, and 5 actuators are
required to induce primary spherical aberration, a 4th order polynomial. Table 5.1 lists the
maximum deformable mirror stroke available per Zernike aberration.

128
Table 5.1. Maximum stroke of ALPAO DM97 deformable mirror per Zernike mode for a 4.0 mm pupil.
Figure 5.7a shows an example of the performance of the AO system for correcting
a subject’s native aberrations. This subject’s native wavefront RMS error was 0.70+0.01
and 0.61+0.01 µm, in the left and right eye, respectively, over a 4.0 mm pupil. After AO
correction was initiated, the wavefront RMS error quickly decreased to 0.03+0.01 and
0.05+0.01 µm, in the left and right eye, respectively. The spikes in the time-course data
correspond to blinks. The wavefront maps corresponding to before and after AO
correction are shown in Figures 5.7b and c, respectively.
Figure 5.7. (a) Time-course change in wavefront root mean square (RMS) over a 4.0 mm pupil for both eyes before and after adaptive optics correction. Wavefront maps for both eyes before and after correction are shown in (b) and (c), respectively.
In addition to correcting the eye’s wavefront aberrations, the adaptive optics
system was used to induce defocus and spherical aberrations to create various modified
monovision conditions. Figure 5.8 shows the wavefront maps for the right and left eyes in
modified monovision at distance (0.0 D) with 4.0 mm pupils. In this case, the right eye is

129
the dominant eye, refracted for distance with +0.2 µm of primary spherical aberrations.
The left eye has -0.2 µm primary spherical aberration and is corrected for 1.5 D. The
leftmost column shows the ideal wavefront for the right and left eyes at 0.0 D. The
central column shows the measured wavefront with the AO correction and aberration
induction. The rightmost column shows the wavefront error map, defined as the
difference between the ideal and measured wavefronts. Colorbars correspond to right and
left eye rows.
Figure 5.8. Ideal, measured, and wavefront error maps in right and left eyes for modified monovision over a 4.0 mm pupil.
As discussed previously117, 118, pupil size decreases with age, and the presbyopic
population has a typical pupil size between 3 and 5 mm in diameter. Therefore, the 52-
actuator Mirao deformable mirror was upgraded to the 97-actuator ALPAO deformable

130
mirror to allow for higher-order aberration correction and induction within relatively
smaller pupil sizes.
The visual stimulus was displayed by a digital light processor of a computer
projector (XR-10X, Sharp) equipped with a 0.6” digital light processor (DLP) XGA
(1024x768 pixels) resolution. The focal length of lens L7 was chosen such that the DLP
support adequate resolution. The entire DLP active area subtended 3.9x2.9 degrees. As
such, each pixel (11.9 µm spacing) subtended 0.227 minutes of arc, approximately half of
the foveal cone photoreceptors (0.5 minutes of arc)207, allowing the generation of visual
stimuli below the retina’s Nyquist sampling frequency of 60 cyc/deg68. It follows that the
smallest Snellen letter capable of being presented by the DLP was 20/4.5.
The projection lens was removed and the DLP was operated in white light with a
60 Hz refresh rate. The DLP luminance was approximately 10 cd/m2 for vision testing in
the photopic regime. The projector’s luminance response was linearized (gamma-
corrected) and bit-depth was expanded from 256 gray-levels (8-bit) to 1786 gray-levels
(10.8-bit) using the bit-stealing, or pseudo-gray technique208. Two identical apertures
were placed in the retinal plane (FL, Figure 5.4) of each monocular system to minimize
fixation disparity by acting as a fusion lock and to limit the angular subtense of the DLP
to a 2 degree diameter, within the eye’s isoplanatic patch107, 108. The isoplanatic patch is
defined as the angular field of view over which the wavefront aberrations are constant.
Therefore, although the adaptive optics system corrects and induces aberrations on-axis,
the performance was still maintained across the visual stimulus.

131
5.3.2 Experimental Protocol
Visual performance was assessed in three normal emmetropic subjects (age: 34 +
11 years). All subjects’ pupil were dilated and accommodation was paralyzed with
cyclopentolate hydrochloride (1%)167. Therefore, cycloplegia impaired the
accommodative ability of the subjects, despite their age being younger than the typical
presbyope. The University of Rochester Research Review Board approved this research
and informed consent was obtained from all subjects prior to their participation in the
study. All procedures involving human subjects were in accordance with the Declaration
of Helsinki.
Visual performance was assessed both binocularly and monocularly with high-
contrast visual acuity and contrast sensitivity for target vergences ranging from distance
to near. During monocular measurements, the non-test eye was occluded with an eye
patch. During vision testing, the binocular adaptive optics vision simulator corrected all
subjects’ native lower and higher order aberrations in closed-loop, in addition to
aberration induction. All aberration conditions and vision testing described in this study
pertain to a 4.0 mm pupil diameter.
High-contrast visual acuity was measured according to the method described in
the previous chapter. Binocular through-focus acuity was measured for modified and
traditional monovision conditions described above. Monocular through-focus acuity was
measured with three magnitudes of primary spherical aberration: 0.0, +0.2 and +0.4 µm.
Depth of focus was defined as the defocus range in diopters from distance (0.0 D) to near
(positive D) for which acuity surpassed 0.18 logMAR (20/30 Snellen acuity).

132
Contrast sensitivity at 10 cyc/deg was measured using a Gabor stimulus and a
two-alternate forced choice method. The stimulus was presented with retinal illuminance
of 5.0 cd/m2. A psychometric function based on 40 trials was obtained using the
QUEST169 algorithm. The stimuli were displayed on a 14-bit analog cathode ray tube
(CRT) display (NEC Multisync fp950). Contrast threshold (sensitivity-1) was defined as
the contrast for which 75% of responses were correct. Three threshold measurements
were averaged for each optical condition.
Through-focus contrast sensitivity at 10 cyc/deg was measured in modified
monovision with +0.2 µm primary spherical aberration induced in the non-dominant eye
and traditional monovision (1.5 D anisometropia) both binocularly and monocularly to
assess binocular contrast summation. The binocular contrast summation factor was
defined as the ratio of the binocular contrast sensitivity to the superior monocular contrast
sensitivity at each target vergence.
5.3.3 Through-Focus Contrast Sensitivity and Binocular Summation
Average binocular contrast sensitivity and binocular summation factor at 10
cyc/deg for the three subjects tested is plotted as a function of defocus in Figures 5.9a and
b, respectively. The error bars represent one standard deviation of three subjects.

133
Figure 5.9. (a) Through-focus binocular contrast sensitivity for traditional and modified monovision with +0.2 µm of spherical aberration and (b) the corresponding through-focus binocular summation factor. (c) Through-focus binocular MTF at 10 cyc/deg and (d) the corresponding through-focus binocular summation factor estimated using the Quadratic summation model (equation 5.1).
Contrast sensitivity at distance and intermediate (0.0 to 1.0 D) was not
significantly affected in modified monovision. However, at 1.5 D, contrast sensitivity in
modified monovision was significantly lower than traditional monovision due to the
induction of spherical aberration, as predicted by the MTF in Figure 5.9c. The induction
of -0.2 and +0.2 µm of spherical aberration in modified monovision degraded contrast
sensitivity at 1.5 D by a factor of 2.1 and 2.5, respectively, compared to traditional
monovision.

134
At distance and beyond 1.0 D, binocular summation was close to unity for all
monovision conditions. However, at 0.5 D, modified monovision with -0.2 and +0.2 µm
of spherical aberration exhibited binocular summation factors of 1.47+0.49 and
1.58+0.38, respectively. By comparison, traditional monovision also showed increased
levels of summation (1.28+0.25). The theoretical prediction based on the MTF and the
quadratic summation model also predicts summation at 0.5 D, however the magnitude is
less than that observed experimentally.
As shown in Figure 5.3d, the interocular difference in through-focus retinal image
quality reached a minimum in the neighborhood of 0.5 D. Therefore, it was not surprising
to observe a peak in binocular summation in all monovision conditions. At 0.5 D,
modified monovision led to binocular summation improvement by 19+6% compared to
traditional monovision, however this improvement was not statistically significant. It
should also be noted that binocular summation factor in modified and traditional
monovision may vary at additional spatial frequencies.
The interocular difference in retinal image quality is known to adversely affect
summation5, 8, 10, 11, 38. Similar to the result of Pardhan and Gilchrist197 (shown in Figure
5.2), Loshin et al.209 found summation to be absent in subjects with 1.5 D of
anisometropia for mid to high spatial frequencies. This study confirmed these results for
distance vision, however found that as the monocular retinal image quality converges on
a single value at the object distances midway between the two eyes’ best focus,
summation increases.

135
5.3.4 Through-Focus Visual Acuity
Average high-contrast visual acuity for the three subjects tested is plotted in units
of logMAR as a function of defocus in Figure 5.10. The error bars represent one standard
deviation of three subjects.
Figure 5.10. Through-focus binocular visual acuity for traditional (TMV) and modified monovision (MMV) with (a) +0.2 µm and (b) +0.4 µm of primary spherical aberration induced in the non-dominant eye. The gray dashed line represents the depth of focus threshold.
Distance visual acuity at 0.0 and 0.5 D in traditional monovision was -0.29+0.06
and -0.12+0.04 logMAR, respectively, and was not significantly affected by in modified
monovision. However, at the intermediate distance of 1.0 D, modified monovision with
positive significantly improved acuity by approximately 0.18+0.06 and 0.12+0.04
logMAR (+0.2 and +0.4 µm primary spherical aberration respectively). Negative
spherical aberration also improved acuity at 1.0 D compared with traditional monovision,
however, this improvement was not statistically significant. Modified monovision with
negative spherical aberration led to a larger improvement at 2.0 D than positive spherical
aberration, as compared with traditional monovision.

136
Visual acuity at near object distances beyond 2.0 D was improved in all modified
monovision conditions as compared to traditional monovision. Modified monovisions
with -0.2 and +0.4 µm spherical aberration had the largest benefit with respect to
traditional monovision from 2.0-3.5 and beyond 3.5 D, respectively. Binocular depth of
focus in modified monovision was 3.2+0.3, 3.5+0.0, 3.2+0.8, and 4.2+0.3 D for spherical
aberration values of -0.4, -0.2, +0.2 and +0.4 µm in the non-dominant eye, respectively.
By comparison, binocular depth of focus in traditional monovision was 2.7+0.3 D.
In an investigation of the effect of anisometropia on distance acuity, Collins et
al.210 found binocular acuity to be approximately equal to the monocular acuity of
distance-corrected eye. This can be attributed to what Schor et al.56 described as
interocular suppression of anisometropic blur.
The current study extended this finding from performance at distance to include
intermediate and near object positions. Figure 5.11a illustrates average monocular
through-focus visual acuity measured in both eyes and binocular visual acuity for the
corresponding modified monovision condition (+0.2 µm spherical aberration). Figure
5.11b shows the strong correlation (r = 0.97) between binocular and superior monocular
visual acuity in modified and traditional monovisions for all tested object distances. As
described above, binocular suppression was incorporated to the theoretical model to
predict binocular retinal image quality.

137
Figure 5.11. (a) Through-focus monocular (DE: dominant eye; NDE: non-dominant eye) and binocular visual acuity for the modified monovision conditions with +0.2 µm spherical aberration. (b) Binocular visual acuity (VA) plotted as a function of monocular visual acuity of the better eye for each object distance for traditional and modified monovisions with positive spherical aberration. The black solid line represents the equal acuity line.
A high correlation (R2 = 0.84) was found between theoretically computed
binocular retinal image quality using the ICM and measured binocular visual acuity for
all monovision conditions, as shown in Figure 5.12. The same dataset was applied to
other retinal image quality metrics, such as the logarithm of the visual Strehl ratio
(VSOTF), the logarithm of the area under the modulation transfer function (aMTF) and
the logarithm of the Strehl ratio. The correlations of binocular through-focus visual acuity
in all modified and traditional monovision conditions with the log(VSOTF), log(aMTF)
and log(Strehl) were R2 = 0.75, 0.73 and 0.62, respectively.

138
Figure 5.12. Binocular visual acuity versus theoretically calculated binocular retinal image quality, computed using the image convolution metric. Black circle: traditional monovision, red square: MMV (SA = +0.2 µm), green square: MMV (SA = -0.2 µm), blue diamond: MMV (SA = +0.4 µm), orange diamond: MMV (SA = -0.4 µm). The black line represents the best-fit linear regression.
The ICM provided a robust estimate of binocular visual acuity in the presence of
large magnitudes of presbyopic blur. The situation was further complicated by significant
differences in interocular retinal image quality due to anisometropia and spherical
aberration of modified and traditional monovision corrections. The image quality metric
was shown to be reliable and enables the optimization of modified monovision variables
for the design of binocular presbyopic correction strategies.

139
5.4 Optimization of Modified Monovision
The ICM was used to investigate the impact of varying the fundamental variables
associated modified monovision: anisometropia and sign and magnitude of spherical
aberration in both eyes. By gaining an understanding of the interaction of these variables
upon binocular through-focus visual performance, it is possible to design optimal
modified monovision strategies to maximize through-focus visual performance, while
minimizing the sacrifice in binocular visual function, such as binocular summation and
stereopsis.
To evaluate the performance of a modified monovision design, we chose two
outcome measures: overall binocular image quality and overall interocular difference in
image quality. The calculation of overall binocular image quality comprised of 3 steps.
First, two monocular through-focus retinal image quality curves were computed using the
image convolution metric. Next, binocular through-focus retinal image quality was
obtained by selecting the better of the two monocular values at each defocus value to
account for binocular suppression, as described previously59. Finally, average through-
focus binocular retinal image quality between 0.0 and 2.5 D was computed to represent
the overall binocular image quality with a scalar value. The overall interocular difference
in image quality was quantified similarly, by taking the absolute magnitude of the
difference of the two eyes’ retinal image quality at each through-focus position, and
averaging from 0 to 2.5 D. The outcome measures are described algebraically below in
equations 5.3 and 5.4.

140
{ }∑=
−=
2
1
, max Quality ImageBinocular Overall 12d
dnnrightnleft RIQRIQ
n
dd (5.3)
[ ]∑=
−−
=2
1
Quality Imagein Differencer Interocula Overall 12d
dnnrightnleft RIQRIQ
n
dd (5.4)
The optimization variables included anisometropia (0.0 to 2.0 D, with 0.5 diopter
increments) and primary spherical aberration in both eyes (-0.4 to +0.4 µm, with 0.1 µm
increments). Both eye’s pupils were constrained to 4.0 mm diameter. This procedure
resulted in a total of 405 potential modified monovision designs. However, only modified
monovision designs which had peak image quality at distance were included for final
analysis, leaving 240 designs. The remaining modified monovision designs are
summarized in Figure 5.13a, where each design’s overall binocular image quality is
plotted against its overall interocular difference in image quality (gray diamonds).
Traditional monovision with 1.5 D of anisometropia is represented by the large black
diamond. The small black diamonds correspond to traditional monovision with 0.0, 0.5,
1.0 and 2.0 D of anisometropia.

141
Figure 5.13. (a) Overall binocular image quality as a function of overall interocular difference in image quality for all modified monovision (MMV) designs (gray diamonds). Traditional monovision (TMV) for 1.5 D anisometropia is represented by the large black diamond. TMV with remaining anisometropia is represented by the small black diamonds. Modified monovision designs were grouped by degree of (b) anisometropia, (c) dominant eye spherical aberration and (d) non-dominant eye spherical aberration. Error bars represent the standard deviation within each group of designs. Bold black arrows indicate the impact of the magnitude of increasing anisometropia or spherical aberration.
The modified monovision designs cover a large gamut of overall binocular image
quality and overall interocular difference, indicating the importance of optimization. An
ideal design would have high overall binocular image quality and low overall interocular
difference in image quality, putting the ideal location in the upper left-hand corner of the
figure. As shown by the traditional monovision data points (black diamonds) in Figure
5.13a, as the anisometropia increases, both the overall binocular image quality and

142
overall interocular difference increase. This trend embodies the trade-off inherent to
traditional monovision.
To generalize the results from the simulations, Figures 5.13(b-d) group the
modified monovision designs into categories based on (b) anisometropia, (c) dominant
eye spherical aberration and (d) non-dominant eye spherical aberration. When grouped by
degree of anisometropia (Figure 5.13b), the modified monovision designs have both
higher overall interocular image quality and lower overall interocular difference, as
compared to their corresponding traditional monovision designs.
The impact of spherical aberration was shown to have a significantly larger effect
on interocular difference as compared to binocular image quality, as shown in Figure
5.13c. This can be appreciated by the disproportionate distribution of modified
monovision designs (colored circles, Figure 5.13c) along the x-direction (interocular
difference) as compared with the y-direction (binocular image quality). Alternatively,
non-dominant eye spherical aberration had an influence on both binocular image quality
and interocular difference, as shown in Figure 5.13d.
The sign of spherical aberration in each eye has a significant impact on through-
focus image quality and interocular difference in image quality. In Figure 5.14, four
modified monovision conditions with common 1.5 D of anisometropia are compared. The
dominant and non-dominant eyes have +0.2 µm of spherical aberration in all possible
combinations: positive in both eyes (red, MMV (+ +)), negative in both eyes (purple,
MMV (- -)), positive/negative in dominant/non-dominant eyes (green, MMV (+ -)) and
negative/positive in dominant/non-dominant eyes (blue, MMV (- +)). In addition,
traditional monovision with 1.5 D was included for comparison (black).

143
Figure 5.14. (a) Through-focus retinal image quality and (b) interocular difference in through-focus retinal image quality. (c) Overall binocular image quality versus overall interocular difference in image quality.
As shown in Figure 5.14a, sign of spherical aberration in the dominant eye does
not have a significant impact on binocular image quality. However, positive spherical
aberration in the non-dominant eye significantly improved near image quality. In addition,
interocular difference in image quality was smallest when positive and negative spherical
aberration was in the dominant and non-dominant eyes, respectively. However,
regardless of the combination of signs, modified monovision was superior to traditional
monovision (Figure 5.14c).

144
The modified monovision design with the maximum overall binocular image
quality included 1.5 D anisometropia and spherical aberration of +0.1 and -0.4 µm in the
dominant and non-dominant eyes, respectively. This design has an overall binocular
image quality value of 0.84 and an overall interocular difference value of 0.24. Through-
focus binocular image quality and interocular difference in image quality are shown in
Figure 5.15a and b, respectively. While this design maximized overall image quality,
further study is needed to clarify the ambiguity between similar modified monovision
designs. This design was also chosen for its relatively small induction of spherical
aberration in the dominant eye and therefore maintaining near optimal distance image
quality. We evaluated the performance of this design by measuring through-focus visual
acuity. Figure 5.15c shows through-focus visual acuity in three cyclopleged subjects,
measured following the procedure described above using the binocular adaptive optics
vision simulator. Two-line stereoacuity was also measured using the binocular adaptive-
optics vision simulator and is shown in Figure 5.15d. Method of constant stimuli was
used to determine stereoacuity for 15 presentations at various disparity levels.

145
Figure 5.15. Through-focus (a) binocular image quality and (b) interocular difference in image quality for traditional (black) and modified (green) monovision. (c) Through-visual acuity and (b) stereoacuity. Asterisks denote a statistically significant difference between modified and traditional monovision (p<0.05, paired Student’s t-test).
The image-quality-optimized modified monovision design significantly improved
visual acuity at 0.5, 2.5, 3.0 and 3.5 D by an average of 0.14+0.05 logMAR as compared
to traditional monovision. However, at 1.5 D, modified monovision led to a significant
degradation in acuity to -0.31+0.11 logMAR from -0.19+0.06 logMAR with traditional
monovision.
As predicted by the increase in interocular image quality in modified monovision,
stereoacuity at distance was significantly improved as compared to traditional
monovision. Alternatively, at 1.0 D, both modified and traditional have relatively similar
interocular image quality and therefore were observed to a yield similar stereoacuity.

146
Using the clinically common Titmus stereo test, Lovasik and Szymkiw53 measured an
average stereoacuity of approximately 150 arcseconds in the presence of 1.5 D of
anisometropia. By comparison, in the absence of anisometropia, stereoacuity was
approximately 45 arcseconds. Although modified monovision did not restore stereoacuity
to normal values, it did offer a significant improvement over traditional monovision.
5.5 Discussion
This chapter represents a major step forward in the correction of presbyopia by
shifting from monocular designs to those that take advantage of the binocular visual
system. By optimally using both eyes, it is possible to achieve results unattainable with
strategies based on monocular retinal image quality. In this chapter we have shown that
increasing monocular depth of focus in modified monovision leads to improved through-
focus visual acuity as compared to traditional monovision. In addition, binocular
summation and stereoacuity are improved compared to traditional monovision due to the
reduction in the interocular difference in retinal image quality.
Our findings were supported by those of previous studies. In a study by Fisher211,
modified monovision was implemented with multifocal soft contact lenses. His study
found that stereoacuity was not significantly degraded modified monovision as compared
to spectacle wear. In another soft contact lens study, Richdale et al.212 also found a
superiority in stereoacuity with modified monovision as compared to traditional
monovision.
In addition to wavefront multifocality, other methods of implementing modified
monovision have been investigated. Several studies43-46 investigated a variation on

147
modified monovision using the pinhole effect to extend the depth of focus of the non-
dominant eye. These studies showed a significant improvement in near acuity46, 213 and
stereoacuity214, 215 when a pinhole aperture was positioned in the non-dominant eye with a
contact lens215, surgical corneal inlay46 or a binocular adaptive optics vision simulator213,
214. However, side-effects of the monocular pinhole aperture approach include significant
reduction in retinal illuminance, peripheral visual field loss, and distortions in spatial
perception due to Pulfrich effect216.
A limitation of our psychophysical analysis was the use of a fixed artificial pupil
size during through-focus vision testing. Under natural conditions, as the presbyope
fixates on near stimuli, the pupil size decreases. In the case of modified monovision,
pupil miosis will reduce the magnitude of spherical aberration and can lead to changes in
retinal image quality.
Furthermore, this study did not take into account subjects’ native higher order
aberrations, in order to isolate the optical contribution of modified monovision. For future
study, it will be important to assess visual performance in a more practical situation, that
is, under natural viewing conditions with the native higher order aberrations present.
In conclusion, we have found that the binocular approach of traditional
monovision suffers from a trade-off in through-focus visual performance and binocular
visual function. A binocular adaptive optics vision simulator was developed for the
psychophysical investigation of binocular presbyopic correction strategies.
Increasing monocular depth of focus in combination with anisometropia, as in
modified monovision, was a successful strategy for partially regaining lost binocular

148
functions such as stereoacuity and binocular summation. Modified monovision also
increased the binocular depth of focus, thereby improving through-focus visual acuity.
This study also found that the dominant and non-dominant eyes play different
roles in through-focus visual performance. For instance, increasing the dominant eye’s
depth of focus is useful for reducing the interocular difference in image quality. The non-
dominant eye’s depth of focus was found to be a more useful design parameter for
optimizing near acuity.
We have shown modified monovision to be a promising strategy for the
correction of presbyopia. By implementing the appropriate degree of anisometropia and
spherical aberration to the binocular visual system, we demonstrated a marked
improvement in through-focus visual acuity, binocular summation and stereoacuity.
Despite these benefits however, the degradation in contrast due to spherical aberration
did reduce performance at the anisometropic point, as compared to traditional
monovision.
While optical investigations such as this are important for understanding the
interaction between binocular retinal image quality and visual performance, it is
important to not disregard the role of the neural visual system. In the following section,
we address neural factors’ influence on binocular visual performance in modified and
traditional monovision.

149
Chapter 6. Neural Factors Affecting Visual
Performance in Modified Monovision
6.1 Introduction
In the previous chapter, we investigated the efficacy of modified monovision
using optical theory and binocular visual performance, but there is one important aspect
that is missed, that is, the role of the neural visual system. Presbyopic correction
strategies such as modified monovision rely upon the neural system to combine the two
monocular inputs into a single binocular perception. Thus, the goal of this chapter was to
address neural factors which may affect the monocular-to-binocular combination and
binocular through-focus visual performance.
Specifically, we addressed the role of ocular dominance and its effect on modified
and traditional monovision. Ocular dominance is important in monovision corrections, as
it may determine a patient’s ability to accept a monovision treatment and determine the
final outcome. As an increasing portion of presbyopia correction strategies become
surgical procedures which may not be easily reversible (e.g. refractive surgery,
implantation of prosthetic corneal inlays or IOLs), accurate assessment of eye dominance
prior to intervention becomes critical.
While ocular dominance offers a means of classifying potential candidates based
on their pre-surgery condition, neural plasticity allows for the alteration of the neural
system after an optical correction has been applied. Therefore, we subsequently
investigated the potential of neural plasticity to aid in neural adaptation to binocular

150
presbyopic corrections. In this final section, we used a perceptual learning vision training
regimen to improve visual performance beyond the limits set by the eyes’ optical quality.
6.2 The Role of Ocular Dominance in Binocular Visual Performance
The human body is symmetrically organized about the central vertical axis,
however, most individuals find an imbalance in proficiency with one side of their body
over the other. For example, writing is carried out with a preferred hand, or kicking a ball
with a preferred foot due to a laterality, or dominance. Similarly, under certain visual
conditions, one eye may be preferred over the other. In the current section, we investigate
the consequences of this phenomenon, termed “ocular dominance”, on binocular visual
performance in modified and traditional monovision.
As mentioned above, ocular dominance is important to the clinical community for
correctly selecting potential patients for surgical employments of monovision-type
presbyopia corrections. However, from a scientific perspective, the understanding of the
binocular merger of two monocular channels into one perception, particularly in the case
of imbalanced optical quality, is not well-understood. Therefore, modified monovision
provides an ideal platform in which to investigate the impact of ocular dominance on
visual performance.
6.2.1 Sighting Versus Sensory Ocular Dominance
In 1903, Rosenbach discovered this phenomenon using a simple sighting task. He
asked subjects to point to a distant target with a finger while both eyes were held open.

151
Eye dominance was then determined by alternate occlusion: the dominant eye was
aligned both to the finger and target, whereas the non-dominant eye was misaligned with
the finger217. As a side-note, handedness and ocular dominance are not correlated218, 219.
Ocular dominance may play a critical role in the overall success of monovision,
therefore, its assessment is becoming increasingly important in the clinical setting195.
With the ongoing advances of refractive surgery and IOL design, monovision strategies
applied in the operating room are becoming more common. However, surgical
implementations of monovision are not easily reversible and therefore require reliable
assessment of eye dominance prior to surgery.
Tests for ocular dominance fall into one of two categories: sighting and sensory
dominance. Motor tasks such as that used by Rosenbach, or binocularly aligning a hole in
a card with a far target fall into the class of sighting dominance tests. The myriad of
sighting dominance tests220 are generally straightforward, convenient and are widespread
in clinical settings63.
Despite the simplicity and clinical ubiquity of sighting tasks for the assessment of
eye dominance, their accuracy is questionable. In a comparison of sighting tasks, Rice et
al.219 found a high test-retest reliability for each sighting test, however, only moderate
agreement was found between different sighting dominance tests, as confirmed by several
other studies220, 223. Conversely, others221, 222 have found high correlations among sighting
tests. Furthermore, sighting tests are dependent upon factors such as the hand used in the
test223, gaze angle224, 225 and the patient’s knowledge of the task226. What is clear,
however, is that sighting tasks only offer a binary outcome: either right or left eye is

152
dominant. Thus, such tests are not capable of differentiating the degree of dominance in a
subject.
Alternatively, sensory dominance tests offer a finer, more robust measure of
ocular dominance, and in some cases offer a quantification of the degree of dominance63,
227. Such tests measure the imbalance of sensory input to the two eyes, making use of
binocular rivalry60, 64 or stereo-disparate objects65 to measure the magnitude of
dominance. Handa et al.60 have suggested a rivalry sensory dominance test to screen
potential candidates for surgically implemented monovision with IOLs during cataract
surgery using a subjective questionnaire. They found that pseudophakic monovision
patients with strong degree of sensory dominance tended to be unsatisfied, due to
difficulty in suppressing the dominant eye.
The goal of this investigation was to determine the role of the degree of sensory
dominance in relation to through-focus visual performance in modified and traditional
monovision. The binocular suppression required to cope with large difference in retinal
image quality, as found in traditional monovision, may be inhibited by large degrees of
dominance56. Therefore, a modified monovision correction which aims to reduce the
difference in interocular image quality (i.e. the need for suppression) is expected to be
less affected by the degree of dominance.
To address the role of eye dominance, subjects’ degree of sensory dominance was
quantified using a binocular rivalry method. Subsequently, through-focus visual
performance was measured with both modified and traditional monovision under two
conditions: dominant eye assignment to distance, and non-dominant eye assignment to
distance.

153
6.2.2 Determining the Degree of Ocular Dominance
A binocular rivalry technique for quantifying the degree of sensory ocular
dominance was used, similar to that described by Handa et al.60, 227. As shown in Figure
6.1a, subjects viewed an liquid crystal display computer monitor (VH242H, Asus, Taipei,
Taiwan) through a haploscope, in which rivalrous images were shown to each eye. The
LCD display was placed at 1 meter distance from the subject and had an illuminance of
25 cd/m2. The setup included mirrors for each eye with tip/tilt adjustment to assist in
binocular fusion. Subjects wore trial frame spherical/cylindrical lenses to correct any
ametropia and enable clear visibility of 20/20 Snellen letters at distance.
Figure 6.1. (a) Haploscope schematic diagram. (b) Visual stimulus for left and right eyes presented by the LCD display.
The visual stimulus, shown in Figure 6.1b, consisted of two perpendicular
sinusoidal gratings (4 cyc/deg), one allocated to each eye. Each grating subtended 1
degree of visual field to minimize a patchwork of the rivalrous images. The gratings were
surrounded by a 2x2 degree dashed square as a fusion lock on a gray background.
Binocular viewing of the stimulus invoked binocular rivalry, in which the
perception was of an alternating view of orthogonally oriented gratings. During a 60

154
second period, subjects were asked to press the left or right arrow keys for the duration of
clear visibility of the leftward (+45 degrees) or rightward (-45 degrees) oriented grating,
respectively. If a patchwork of the two gratings was perceived, subjects were instructed
to not press any key. The total time spent with clear visibility with each eye for the 60
second period was recorded. All 60 second periods had fixed 50% contrast of the left eye
grating, whereas the right eye contrast was held fixed at a value between 10 and 95%.
Thus each 60 second period gave a measure of the amount of time spent viewing with
each eye. The percentage of time over a 60 second period spent viewing with the right
eye as a function of right eye contrast was plotted and fitted with a sigmoid function.
Finally, the degree of dominance was defined as the interocular contrast ratio (right eye
contrast divided by left eye contrast) resulting in equal viewing time. An illustrative
example of one subject’s data is shown in Figure 6.2.
Figure 6.2. Portion of time spent viewing right eye stimulus as a function of right eye contrast for one subject. In this example, this subject had an ocular dominance score of

155
0.7 (35% divided by 50% contrast in the right and left eyes, respectively, for equivalent viewing duration).
As illustrated in Figure 6.2, when the right eye contrast is high, the majority of the
60 second period is spent viewing with the right eye. Conversely, when right eye contrast
was low, only a small portion of the time was spent viewing with the right eye. In this
case, for the subject to view with the two eyes an equal portion of time, the right eye
contrast was 35%. Recall, left eye contrast is held fixed at 50%, therefore, values below
unity indicate right eye dominance and values above unity indicate left eye dominance. In
the example of Figure 6.2, this subject was right eye dominant, with a dominance value
of 0.7.
The degree of dominance was measured in 13 subjects (average age: 29+7 years).
One subject was excluded due to amblyopia; this subject never reached equal interocular
viewing ratio, even with 100% contrast in the right eye. The degree of dominance in the
remaining 12 subjects is shown in Figure 6.3a and b. Weak ocular dominance was
defined as a dominance value within +10% of unity (between 0.9 and 1.1) and 3 (25%)
subjects fell into this range. Eleven (92%) subjects were right eye dominant.

156
Figure 6.3. (a) Histogram and (b) plot of degree of sensory eye dominance in 12 subjects. A degree of dominance value of unity indicates no dominance. Below and above unity signifies right and left eye dominance, respectively. The gray band of weak dominance spans +10% about unity.
For comparison, sighting eye dominance was measured using the hole-in-card
test63, in which subjects view a far target through a 1 cm diameter hole in a card.
Alternate occlusion revealed the dominant as the eye viewing the target. The sighting test
was in agreement with the sensory dominance test in 10 (83%) subjects. The 2 subjects
with conflicting dominance results were weak dominant subjects. By comparison,
Pointer228 found 71% of normal, healthy subjects were right eye dominant using the hole-
in-card sighting task and 54% were right eye dominant using a sensory task based on
subject discomfort with a 1.5 D fogging lens.
6.2.3 Impact on Through-Focus Visual Acuity
The research presented in this section was approved by University of Rochester
Research Review Board. All subjects signed an informed consent form and underwent a
clinical eye exam prior to participation in this study. All procedures involving human
subjects were in accordance with the tenets of the Declaration of Helsinki.
Through-focus visual performance was assessed with high-contrast visual acuity
and contrast sensitivity at 10 cyc/deg from distance to near (0.0-3.0 D) in 0.5 D
increments. Subjects were cyclopleged and were tested both in modified and traditional
monovision using the binocular adaptive optics vision simulator. The binocular adaptive
optics vision simulator corrected subjects’ native lower and higher order aberrations. The
modified monovision design consisted of 1.5 D anisometropia and +0.1 and -0.4 µm

157
primary spherical aberration in the distance and near eyes, respectively. This modified
monovision design was chosen due to its high overall retinal image quality as found in
the previous chapter. Traditional monovision consisted of 1.5 D anisometropia. A 4.0 mm
artificial pupil diameter was used for all conditions.
As stated previously, to determine the impact of dominance, visual performance
was measured under two circumstances by (a) assigning the dominant and non-dominant
eyes to distance and near, respectively, and (b) vice versa.
Figures 6.4a and b show through-focus visual acuity measured in 9 subjects in a
manner similar to that described in the previous chapter. The mean degree of dominance
in the subjects was 0.85+0.14 with a range of 0.67 to 1.11.

158
Figure 6.4. Average through-focus visual acuity with (a) modified and (b) traditional monovision. Blue data corresponds to condition with dominant eye assigned to distance for 9 subjects. Red data corresponds to the non-dominant eye assigned to distance. (c) Average visual acuity difference between eye assignment paradigms in modified (black empty circles) and traditional (gray filled diamonds) monovision as a function of subjects’ dominance.
As found previously, modified monovision led to an improvement in near acuity
with respect to traditional monovision. As shown in Figures 6.4a, visual acuity was
slightly degraded at 0.5, 1.0 and 3.0 D when the non-dominant eye was assigned to
distance, however this observation was not statistically significant. In traditional
monovision (Figure 6.4b), eye assignment did not have an impact on visual acuity at any
object distance.
The acuity difference plotted in Figure 6.4c was defined as the average difference
in through-focus visual acuity between the two eye assignment paradigms for each
subject. There was no systematic dependence upon, or significant correlation between,
the degree of ocular dominance and visual acuity for modified or traditional monovision
(R2 = 0.18 and 0.06, respectively).
6.2.4 Impact on Through-Focus Contrast Sensitivity
Figures 6.5a and b show through-focus contrast sensitivity at 10 cyc/deg
measured in 3 subjects in a manner similar to that described in the previous chapter. The
subjects’ degree of dominance was 0.74, 0.86 and 0.89 (mean: 0.83+0.08). The percent
change in contrast sensitivity due to changing eye assignment shown in Figure 6.5c was
defined as the difference in contrast sensitivity between two eye assignment paradigms
divided by the conventional paradigm of dominant eye at distance. A positive value

159
indicates an improvement, whereas a negative value indicates a reduction in contrast
sensitivity at a given object distance. Asterisks denote a statistically significant difference
between eye assignment paradigms (p<0.05, paired Student’s t-test).
Figure 6.5. Average through-focus contrast sensitivity with (a) modified and (b) traditional monovision. Blue data corresponds to condition with dominant eye assigned to distance for 3 subjects. Red data corresponds to the non-dominant eye assigned to distance. Asterisks denote a statistically significant difference (p<0.05, Student’s paired t-test). (c) Average percent change in contrast sensitivity between eye assignment paradigms in modified (black empty circles) and traditional (gray filled diamonds) monovision as a function of subjects’ dominance.
Comparing modified to traditional monovision, it is clear that the induction of
-0.4 µm of primary spherical aberration in the anisometropic eye led to a significant
degradation in contrast sensitivity at 1.5 D as compared to traditional monovision,
regardless of eye assignment paradigm.

160
Contrast sensitivity was significantly impacted by ocular dominance in both
modified and traditional monovision. As shown in Figure 6.5c, at 0 D, there is a benefit
in using the conventional paradigm of assigning the dominant eye to distance vision.
However, this same paradigm led to a significant degradation in contrast sensitivity at
intermediate and near object distances. Alternatively, assigning the non-dominant eye to
distance revealed a reduction in distance contrast sensitivity at 0.0 and 0.5 D, and an
improvement from 1.0 to 3.0 D. Therefore, contrast sensitivity was greatest at each
defocus level when the dominant eye coincided with better retinal image quality.
6.2.5 Discussion
In this section, we introduced a new method of quantifying the degree of ocular
dominance based on a binocular rivalry technique. Furthermore, we found that subjects’
ocular dominance did have an impact on through-focus contrast sensitivity, however not
on high-contrast visual acuity. We have shown in Chapter 5 that binocular summation is
increased in modified monovision due to the reduction in interocular difference in retinal
image quality59. In this study, we found that binocular contrast sensitivity in modified
monovision was more strongly affected by ocular dominance than traditional monovision.
The neurological disorder amblyopia can be considered a special case of a severe
degree of ocular dominance. For example, with a two-fold contrast imbalance between
the dominant and non-dominant eyes (50 and 100%, respectively), our amblyopic subject
perceived clear visibility with the amblyopic eye only approximately 25% of the time.
Amblyopic patients have a large imbalance in monocular visual performance due
to strabismus, anisometropia or untreated cataract during the critical period of

161
development229. Many studies have shown that binocular contrast summation is impaired
in amblyopia22-26. Furthermore, Lema and Blake230 suggested that a shared neural
mechanism mediates binocular summation and stereopsis, two binocular functions which
are optimized in the absence of interocular imbalance in retinal image equality. Based on
these studies, we can expect subjects with exceedingly strong degrees of ocular
dominance to have minimal binocular summation in modified monovision.
Although binocular summation was not quantified in this study by measuring
monocular contrast sensitivity, we can speculate that ocular dominance interacted with
binocular summation. We know from previous literature, that this is the case. Handa et
al.231 found that the degree of ocular dominance determined whether monovision subjects
exhibited any binocular summation. In strongly dominant subjects, binocular summation
was absent, as opposed to the weakly dominant subjects who did exhibit binocular
summation.
A limitation of this study was that the degree of ocular dominance was only
measured at a single spatial frequency (4 cyc/deg). Binocular rivalry is known to be
insensitive to changes in spatial frequency232. However, Handa et al.231 found that ocular
dominance did not affect binocular rivalry for low spatial frequency stimuli (1 and 2
cyc/deg). Future research is needed to determine the spatial frequency dependence of
ocular dominance and its relation to the binocular contrast summation function. It should
be noted that regardless of degree of dominance, binocular suppression of high-contrast
visual acuity letters was present for all acuity levels across a broad range of spatial
frequencies59.

162
6.2.6 Summary
This study found several key findings of clinical and scientific importance. We
have shown that binocular rivalry is a novel and effective technique for quantifying
subject’s degree of ocular dominance, providing a finer measure of dominance than
conventional sighting tasks. In the clinical setting, sensory dominance tests, such as the
one proposed in this chapter, would be valuable in screening potential candidates for
surgical presbyopia treatment. In addition, sensory dominance could be used in pediatric
care to assess the progression of amblyopia in children. This technique could set a
benchmark objective tool to evaluate the efficacy of amblyopia-reversing treatments,
such as dominant eye occlusion with eye-patch.
Furthermore, we have shown that ocular dominance of weak and moderate
magnitudes did not have a significant impact on through-focus binocular visual acuity in
modified and traditional monovision. However, convention tells us to prescribe distance
vision to the dominant eye. We found through-focus binocular contrast sensitivity to be
susceptible to eye assignment. Therefore, although undetectable in visual acuity tasks,
distance contrast sensitivity is truly optimized when the dominant eye is assigned to
distance in both modified and traditional monovision. Alternatively, to optimize
intermediate and near vision, the non-dominant eye should be assigned to distance in
monovision corrections. This finding indicates distinct mechanisms for visual tasks at
threshold and superthreshold contrast levels.

163
6.3 Perceptual Learning in Modified Monovision
6.3.1. Introduction
We found that minimizing the difference in interocular image quality improves
binocular visual function, such as binocular summation and stereoacuity. The limits of
spatial vision have been investigated from the point of view of both optical25-27 and
neural69, 74 factors. Beyond optical factors such as wavefront aberrations, diffraction and
scatter, the neural contrast sensitivity function defines the limit of spatial vision based on
the sensitivity of individual spatial frequency channels70. Furthermore, the neural visual
system has been found to maintain plasticity into adulthood78 and is capable of
refinement via perceptual learning86, 89.
The underlying mechanisms of perceptual learning have been previously studied
and several models have been proposed28, 39-41. As described in Chapter 1, Dosher and
Lu’s paradigm of the perceptual template model19 is based on noise structures of the
nervous system. Both their theoretical model and experimental data support the claim of
perceptual learning leading to an improvement in the signal to noise ratio of individual
spatial frequency channels, in addition to a re-weighting of those channels19, 83. In other
words, the changes in visual performance due to perceptual learning may be due to
modifications in the neural contrast sensitivity function.
Recently, the field of perceptual learning has been extended to improve
performance in normally developed neural visual systems suffering from imperfect
optical conditions. For example, Zhou et al.91 investigated the importance of ocular
higher order aberration correction in perceptual learning. Their study found that

164
perceptual learning was more efficacious in subjects who underwent training with full
aberration correction using an adaptive optics vision simulator. Alternatively, subjects
who trained with their wavefront aberrations uncorrected, received a smaller visual
benefit due to perceptual learning.
It is well known that the visual system is capable of adapting to short-term233, 234
and long-term235-238 exposure of optical blur. Sabesan et al. found that keratoconic
patients with abnormally large magnitudes of higher order aberrations become adapted to
their wavefront aberrations. Keratoconics have normally developed neural visual systems,
as the optical disability tends to arise in adolescence, after the developmental period.
Following wavefront correction with customized soft contact239 lenses or prosthetic
scleral lenses240, keratoconic subjects did receive an immediate visual benefit, however
the benefit increased with time, suggesting a period of neural adaptation241. Perceptual
learning has been proposed as a vehicle to accelerate the adaptation period of this
population242.
Similarly, perceptual learning has been proposed as a treatment for presbyopia49-51.
Polat et al.18 applied a perceptual learning contrast sensitivity paradigm to 30 presbyopes
to improve their uncorrected near vision. Their goal was to boost the neural signals from
the blurred retinal image to be used more efficiently by the brain. Their study showed that
following perceptual learning with both eyes open, uncorrected near visual performance
in contrast sensitivity, visual acuity and reading speed was significantly improved.
Several studies31, 38, 55 have shown interocular transfer of perceptual learning, that
is, monocular training led to improvement in the untrained eye. This suggests that the site
of plasticity in the nervous system occurs beyond neural combination of the input from

165
the two eyes243. To date, the neural contrast sensitivity function has only been directly
measured monocularly69, 74. Therefore it is unclear whether both eyes share a common
neural limit, or if each eye has a unique neural contrast sensitivity function.
Additionally, all previous studies18, 244, 245 concerning perceptual learning in
presbyopia limited visual training to a single object distance. However, all object
distances, far and near, are relevant to the presbyopic population. Therefore, it may be
beneficial to employ perceptual learning at multiple object distances.
We hypothesize the efficacy of perceptual learning in modified monovision to be
greater than that of traditional monovision. This is due to the improvement in through-
focus retinal image quality which Zhou et al.91 showed to be beneficial for perceptual
learning. In addition, based on previous findings regarding interocular transfer following
monocular training, the reduction of the interocular difference in image quality may also
facilitate perceptual learning by targeting binocular vision.
The goal of this section was to test our hypothesis. Thus, we designed a
perceptual learning paradigm to compare the potential visual benefit of vision training at
multiple object distances in modified and traditional monovision. Perceptual learning is
an exciting new avenue towards non-invasive presbyopic correction. If paired with
optimized optical strategies, presbyopic visual performance can be significantly improved
over a broad range of object distances.
6.3.2 Experimental Protocol of Vision Training Regimen
The research presented in this section was approved by University of Rochester
Research Review Board. All subjects signed an informed consent form and underwent a

166
clinical eye exam prior to participation in this study. All procedures involving human
subjects were in accordance with the tenets of the Declaration of Helsinki.
Three healthy presbyopic subjects were recruited for this study. The subjects had
no history of ocular pathology, were phakic, had normal binocular function and were not
users of anti-anxiety or anti-depressant medication. Previous studies246, 247 have shown
that anti-anxiety and anti-depressant drugs may disrupt the sleep cycle which is important
for consolidation of learning. Topical cyclopleging eye drops (tropicamide, 1%) were
used in both eyes to dilate the pupil and arrest any residual accommodation.
Two subjects (48 and 61 years of age) were assigned to the modified monovision
group and one subject (50 years of age) served as a traditional monovision control. All
vision testing was performed binocularly with the binocular adaptive optics vision
simulator using 4.0 mm artificial pupils. The modified monovision design consisted of
1.5 D of anisometropia, and primary spherical aberration of +0.2 and -0.2 µm in the
dominant and non-dominant eyes, respectively. This modified monovision design was
chosen for its superiority to traditional monovision in both overall binocular retinal image
quality and interocular similarity in image quality, as shown in Figure 5.15 of the
previous chapter.
Monocular through-focus retinal image quality computed with the image
convolution metric for modified and traditional monovision conditions is shown in
Figures 6.6a and b, respectively. Binocular retinal image quality and intraocular
difference, as defined in chapter 5, are shown in Figures 6.6c and d, respectively.

167
Figure 6.6. Through-focus monocular retinal image quality in (a) modified and (b) traditional monovision. Solid and dashed lines represent dominant and non-dominant eyes, respectively. (c) Binocular through-focus retinal image quality. (d) Interocular difference in retinal image quality. For (c) and (d), solid and dotted lines represent modified and traditional monovision, respectively.
Subjects were determined to have normal binocular vision in the clinical eye
exam, and eye dominance was assessed using the “hole-in-card” sighting task; all
subjects reported right-eye dominance. Traditional monovision consisted of 1.5 D
anisometropia. All subjects’ native lower and higher order aberrations were corrected
using adaptive optics.
Pre-training through-focus visual acuity (0.0 to 3.0 D in 0.75 D increments) was
assessed using the method described previously in section 5.3.2. Each eye’s stimulus was
displayed with a digital light projector (XR10-X, Sharp Corporation, Osaka, Japan)
conjugate to the retinal plane for each eye with a retinal illuminance of 70 cd/m2.

168
Subjects practiced with the visual acuity task prior to measurement to ensure task
familiarity.
Pre-training contrast sensitivity was measured with Gabor stimuli at 2, 4, 8 and 16
cyc/deg using a two-alternate forced-choice method described previously in section 5.3.2.
The stimuli were displayed using a bit-stealing method208 implemented in Matlab’s
psychophysics toolbox to increase the bit depth from 256 (8-bit) to 1786 (10.8-bit) gray
levels. The pre-training contrast sensitivity functions (CSFs) were measured at 0.0 and
1.5 D object distances. To ensure subjects were accustomed to the task prior to training,
the pre-training CSFs at 0.0 and 1.5 D were measured on three separate visits prior to
beginning the perceptual learning regimen, shown in Figure 6.7. The pre-training CSFs
confirm that subjects were well-acquainted with the contrast sensitivity task, indicating
that subsequent learning was not familiarization with the task.

169
Figure 6.7. Pre-training CSFs for all subjects and spatial frequencies at 0.0 (left column) and 1.5 D (right column). Modified monovision (MMV) is shown in the two upper rows (a-d) and traditional monovision (TMV) is shown in the bottom row (e, f).
The training spatial frequencies were determined from the pre-training CSF. A
threshold was defined as 50% of the peak of the pre-training CSF. The intersection of this

170
threshold with a linear spline fit of the pre-training CSF determined the training
frequency, as illustrated in Figure 6.8 with the vertical red arrow. The example in Figure
6.8 represents the pre-training CSF at 0.0 D for the traditional monovision subject. The
training frequencies for all subjects are listed in Table 6.1. In both modified and
traditional monovision, the optical quality at 0.0 and 1.5 D was equal, therefore the
training frequencies at the two object distances were expected to be equal. The
discrepancies in training frequencies at 0.0 and 1.5 D for each subject were deemed due
to the inherent variability of the contrast sensitivity measurement.
Figure 6.8. Determination of training frequency, indicated by vertical arrow. Dashed line represents 50% of peak contrast sensitivity. Red arrow represents training spatial frequency.

171
Table 6.1. Perceptual learning training spatial frequencies.
Each training session consisted of 10 measurements of contrast sensitivity, split
equally among 0.0 and 1.5 D distances and training frequencies. The order of
measurements at 0.0 and 1.5 D was randomized within each training session. Each
measurement consisted of 100 trials, for a total of 1000 trials per training session (500 at
0.0 D and 500 at 1.5 D). Consistent with other studies90, 91, each subject completed 10
training sessions, for a total of 10,000 trials, over a period of 2 months. The training
sessions were completed over approximately 2 months. In a 100 trial measurement,
approximately 80% of the trials were near the contrast threshold. Each training session
lasted approximately 1.5 hours.
Post-training visual performance testing was akin to the pre-training assessment.
Through-focus visual acuity was measured and contrast sensitivity at 0.0 and 1.5 D for 2,
4, 8, and 16 cyc/deg, in addition to the training spatial frequencies. Post-training contrast
sensitivity was measured twice on two separate visits and averaged.

172
6.3.3 Vision Training with Modified and Traditional Monovision
The results from the perceptual learning regimen as a function of training session
are shown in Figure 6.9. Blue and red data correspond to learning curves at 0.0 and 1.5 D,
respectively. Modified monovision subject 1 exhibited learning curves with positive and
negative slopes at 0.0 and 1.5 D, respectively. Modified monovision subject 2 exhibited
learning curves with positive slopes both at 0.0 and 1.5 D. The traditional monovision
subject learning curves at both distances were near zero.

173
Figure 6.9. Learning curves for modified (a and b) and (c) traditional monovision subjects. Red and blue data corresponds to learning curves at 0.0 and 1.5 D.

174
Pre- and post-training contrast sensitivity at 0.0 and 1.5 D is shown for the three
subjects in Figure 6.10. Pre-training CSF, shown in blue, is the average of the three pre-
training CSF measurements. Post-training CSF, shown in red, is the average of two post-
training CSF measurements. Asterisks denote a statistically significant difference
between pre- and post-training CSFs for a particular spatial frequency (p<0.05, Student’s
t-test, unpaired). Black arrows indicate the spatial frequency for vision training in each
condition (listed in Table 6.1).

175

176
Figure 6.10. Pre- and post-training CSFs (blue and red, date respectively) for all subjects and at 0.0 (left column) and 1.5 D (right column). Modified monovision (MMV) is shown in the two upper rows (a-d) and traditional monovision (TMV) is shown in the bottom row (e, f). Training frequencies are indicated with black arrows for each condition.
The perceptual learning regimen resulted in significant improvement in CSF at
several spatial frequencies. At 0.0 D, only the modified monovision subjects had a
statistically significant improvement in contrast sensitivity at the training frequency. At
1.5 D, only modified monovision subject 2 showed an improvement at the training
frequency. Both modified monovision subjects showed an improvement transfer to other
spatial frequencies. In contrast, the traditional monovision subject did not show an
significant improvement in CSF at 0.0 or 1.5 D, with the exception of 8 cyc/deg at 1.5 D.
Another important finding was the transfer of visual benefit to a visual acuity. In
accordance with previous studies18, 244, perceptual learning with contrast detection tasks
has been shown to transfer to high-contrast visual acuity
Pre- and post-training through-focus visual acuity for the three subjects is shown
in Figure 6.11. Asterisks denote a statistically significant difference between pre- and
post-training acuity particular spatial value of defocus (p<0.05, Student’s t-test, unpaired).

177
Figure 6.11. Pre- (blue) and post-training (red) through-focus visual acuity in (a, b) modified and (c) traditional monovision.
In modified monovision, perceptual learning led to a significant improvement of
0.08+0.01 logMAR at 0.75 D in both subjects 1 and 2 (p<0.05). As shown in Figure 6.6,
the theoretical monocular through-focus retinal image quality curves intersect at 0.75 D.
Therefore, the interocular difference is zero at this location and both eyes have equal
image quality, potentially enabling binocular summation. Perceptual learning also led to
an improvement at 0.0 and 1.5 D, however this improvement was not statistically
significant. However, based on the improvement in CSF at 0.0 and 1.5 D, we would
expect an improvement in visual acuity at these object distances. In addition, the post-

178
training acuity at near object distances (2.25 and 3.0 D) declined with respect to pre-
training performance.
In traditional monovision, the training regimen led to an improvement in acuity at
0.0, 2.25 and 3.0 D and a degradation at 0.75 and 1.5 D. However, this change in visual
acuity was only statistically significant at 2.25 and 3.0 D.
6.3.4 Discussion
Perceptual learning has been shown to be an effective method for improving
visual performance at first limited by habitual higher order aberrations91, 242, presbyopic
blur18, 244, and amblyopia25, 31, 35. In this study, we employed simultaneous perceptual
learning at multiple object distances presbyopia correction strategies capitalizing on the
binocular visual system. Presbyopia corrections which aim to decrease the difference in
interocular retinal image quality, such as modified monovision, led to significantly larger
improvement in contrast sensitivity than traditional monovision.
In Polat et al.’s18 seminal study of perceptual learning in presbyopia, 30
presbyopic subjects underwent an average of 37+11 vision training sessions over the span
of 3 months using Gabor stimuli at multiple spatial frequencies. In their study, subjects
trained with both eyes open without any induced multifocality or anisometropia. Their
study found an improvement of 25+8% in contrast sensitivity at 2, 4 and 6 cyc/deg. In
our study, contrast sensitivity at 2, 4 and 8 cyc/deg improved by 22+6% and 11+18% in
modified and traditional monovision, respectively. The visual benefit of perceptual
learning, defined as the ratio of post- to pre-training CSF is shown in Figure 6.12.
Furthermore, in the modified monovision group, the visual benefit increased dramatically

179
at spatial frequencies above 8 cyc/deg, however the same trend was not observed in the
traditional monovision subject.
Figure 6.12. Average visual benefit at 0.0 and 1.5 D for modified (red) and traditional (blue) monovision.
The visual benefit of perceptual learning in visual acuity was defined as the
difference between post- and pre-training performance, and is summarized in Figure 6.13.
A positive visual benefit value signifies an improvement, whereas a negative value
signifies a decline.

180
Figure 6.13. Visual benefit in through-focus visual acuity in modified (red) and traditional (blue) monovision.
As shown in Figure 6.13, vision training in modified monovision improved
through-focus visual performance from 0.0 – 1.5 D, effectively the range of vision with
relatively low interocular difference in retinal image quality and high retinal image
quality. At 2.25 and 3.0 D, the degradation in visual acuity may have been due to the
relatively large degradation in image quality degraded and increase in interocular
difference in image quality at these object distances.
As shown in Figure 6.12, spatial frequencies above approximately 8 cyc/deg
received a larger benefit due to training than lower spatial frequencies. Albeit the low
spatial frequencies did not exhibit degradation. Furthermore, the spatial frequencies
corresponding the visual acuity obtained at 2.25 and 3.0 D (>0.0 logMAR and >15
cyc/deg) were showed an improvement in contrast sensitivity. These findings suggest an
inhibitory mechanism in training-induced changes in visual acuity.

181
A significant limitation of this study was the limited number of subjects. Further
investigation with a larger sample size is needed to verify these preliminary results.
Despite the small sample size, this study has shown promise for perceptual learning as a
tool to improve presbyopic visual performance. In addition, the role of the similarity in
retinal image quality between the eyes is also a determining factor of efficacy of the
regimen.
Another limitation of this study was the subjects’ temporary experience with the
monovision conditions in the binocular adaptive optics vision simulator. Previous studies
have shown that habitual, daily experience has a significant impact on the perceptual of
blur48, 49, 63. It is important for future studies to consider the passive adaptation due to
daily, prolonged exposure to modified monovision.
Collins et al.58 found that during the first 8 weeks of traditional monovision
contact lens wear, patients subjectively observed improvement in hand-eye coordination
and walking confidence, however this was not supported by objective visual performance
(visual acuity, stereoacuity and blur suppression). Sheedy et al.248 also failed to find an
improvement in visual acuity and stereoacuity over 8 weeks of traditional monovision
contact lens wear. Future studies of neural adaptation to modified monovision may be
practically implemented by measuring the time-course change in visual performance in
monovision LASIK199, 200 patients or by dispensing soft multifocal contact lenses with an
induced anisometropia. Adaptive-optics vision simulators are a valuable tool for such
studies, as they enable accurate control of wavefront aberrations during vision testing.
As the goal of perceptual learning regimens is to improve the quality of life, it is
important to assess the transfer of visual benefit across tasks. In addition, the effects of

182
training should be long-lasting. Future studies should assess transfer to tasks common to
daily life, such as reading accuracy and speed. It will also be important to follow-up with
subjects after vision training to determine the permanence of learning.
In conclusion, we have shown, for the first time, the impact of perceptual learning
on through-focus visual performance in modified and traditional monovision. Although
the conclusions are limited due to the small sample size, we observed a significant
improvement in contrast sensitivity and visual acuity due to training. As predicted by our
hypothesis, modified monovision received a larger benefit due to training than traditional
monovision. This was likely due to the relative benefit in through-focus retinal image
quality and similarity in interocular retinal image quality in modified monovision,
however, further study is required to confirm this hypothesis.
Perceptual learning in conjunction with presbyopic corrections is an exciting and
new field. We have demonstrated the potential of perceptual learning with modified
monovision. In the future, vision training techniques based on more user-friendly
platforms, such as video games249, may be paired with optical corrections to maximize
positive patient outcomes.
6.4 Conclusions
In this chapter, we have addressed several neural factors which may affect visual
performance in modified monovision. We found that binocular rivalry is useful paradigm
for quantifying the degree of ocular dominance in subjects, and may be a useful tool for
screening patients. Furthermore, we found that the clinical convention of assigning

183
dominant eye to distance in monovision corrections has an impact on contrast threshold
tasks, as opposed to super-threshold tasks, such as visual acuity.
Finally, we investigated the potential of neural plasticity as a strategy for
improving binocular visual performance beyond the limits set by the eyes’ optical quality.
In particular, perceptual learning may be a powerful tool to accelerate neural adaptation
to an optical correction. It will be interesting for future studies to apply perceptual
learning to clinical populations of patients after undergoing surgical procedures for
modified or traditional monovision.

184
Chapter 7. Conclusions
Presbyopia, the age-related loss of accommodation, affects each person over the
age of 50 years. Although many correction strategies for presbyopia have been proposed
and are clinically available, none truly restore dynamic accommodation. Because
presbyopia affects large and growing portion of population, the demand for finding a
solution for presbyopia is increasingly more important. However, to avoid previous
strategies’ shortcomings, it is critical to have a solid understanding of their mechanism
and characteristics. Therefore, the research described in this thesis has accomplished four
main goals.
Firstly, this thesis investigated the attributes and limitations of existing
intraocular lenses designed to alleviate the symptoms of presbyopia. These findings
have important implications for ophthalmologists making use of such techniques and the
scientific community devoted to developing new strategies. We have shown that alleged
“accommodating intraocular lenses” approved by the United States Food and Drug
Administration do not operate as intended. A custom-built natural-view Shack-Hartmann
wavefront sensor enabled the quantification of the dynamic changes in through-focus
retinal image quality in patients implanted with accommodating IOLs while
simultaneously monitoring pupil miosis and binocular fusion. This device provided
subjects with unobstructed, binocular and natural viewing conditions. This is a key
requirement to facilitate binocular fusion, one of three hallmarks of the accommodative
triad. We found that despite accurate fusion on far and near targets, and significant
pupillary miosis, indicating a true accommodative effort, the accommodating IOLs

185
produced minimal amounts of accommodation. More importantly, we found that
wavefront defocus changes, or the absence thereof, does not give a complete picture of
the patient’s experience of retinal image quality. Instead, using a retinal image quality
metric which incorporated the natural pupil size and higher order aberrations, we can
learn about changes in through-focus retinal image quality, giving new insight into these
patients’ vision. To quantify the optical quality of existing presbyopia-correcting IOLs,
an adaptive optics IOL bench testing system was developed to determine consequence of
corneal aberrations on through-focus retinal image quality in pseudophakic eyes. This
study found that if patients with corneal astigmatism larger than 0.75 D are implanted
with diffractive multifocal IOLs, they receive not benefit in depth of focus.
Understanding the characteristics and limitations of presbyopia-correcting IOLs’ through-
focus retinal image quality will allow clinicians to have a clearer understanding of their
options and to properly screen potential candidates for extended depth of focus surgical
procedures.
Secondly, this thesis investigated retinal image quality metrics, a critical
requirement for the design of efficacious extended depth of focus optical designs. We
found the metric based on image convolution to be a significantly better predictor of
through-focus visual acuity than more traditional optical metrics, such as the Strehl ratio
or modulation transfer function. Using this metric, higher order aberrations may be
optimized to provide both monocular and binocular approaches for presbyopic correction.
In addition, this metric may be applied to both optical bench and computational studies,
allowing clinicians to predict the outcome of implanting a different premium IOL in each
eye. Patients’ satisfaction and visual performance with extended depth of focus

186
corrections ultimately determines the clinical success of an optical procedure. Therefore,
a theoretical model capable of accurately predicting visual performance is critical for the
design of ophthalmic corrections for presbyopia. As opposed to tradition, single-vision
ophthalmic corrections, which seek to maximize retinal image quality at one object
distance, presbyopia corrections require optimization over a wide range of object
distances. This complicates the design process and introduces a trade-off between peak
image quality and depth of focus.
Higher order wavefront aberrations were an effective means of increasing the
eye’s depth of focus. Although this thesis primarily used spherical aberrations, these are
just one possible tool. We found that combining primary and secondary spherical
aberrations, a larger visual benefit for through-focus retinal image quality was achieved
than using primary or secondary spherical aberration in isolation. In addition, the
interaction of pupil transmission apodization with wavefront aberration strategies was
investigated. Pupil transmission apodization in the presence of wavefront aberrations had
a significant impact on through-focus visual performance by diminishing the contribution
of peripheral wavefront aberration to the retinal image. The design principles found from
computational studies were subsequently verified psychophysically using adaptive optics
vision simulators.
Thirdly, modified monovision, a binocular approach to presbyopia
correction was proposed. By independently controlling the through-focus optical
quality of each eye, the combined binocular visual performance may be optimized
beyond the capabilities of monocular pseudoaccommodation strategies. The clinically
well-established approach of traditional monovision, in which one eye is assigned to

187
distant vision and the other eye to near vision, has significant limitations. The large
interocular difference in image quality caused by traditional monovision’s anisometropia
significantly reduces stereoacuity and binocular summation. Furthermore, in traditional
monovision, each eye remains monofocal and has a narrow depth of focus. Therefore,
binocular through-focus image quality is lacking at object distances midway between the
two eyes’ best focus and at near distances.
Alternatively, in modified monovision, spherical aberration is used to increase the
depth of focus of one or both eyes. Two major benefits of this strategy are (a) an
improvement in binocular depth of focus and (b) a reduction of the interocular difference
in image quality. To verify this approach, a binocular adaptive optics vision simulator
was developed to test binocular visual performance while simultaneously manipulating
the wavefront aberrations of both eyes. Using this powerful and unique instrument, we
found that modified monovision led to a significant improvement in through-focus visual
acuity, stereoacuity and binocular summation, as compared to traditional monovision.
Thus far, we have used advanced optical techniques to investigate presbyopic
corrections based on optimizing the retinal image quality of both eyes. However, also
wished to investigate neural factors’ impact on binocular visual performance. Therefore,
our fourth goal was to study the consequences of ocular dominance and the
potential for neural plasticity in regard to visual performance in modified
monovision.
In monovision corrections, the clinical convention is to assign the dominant eye to
distance vision and the non-dominant eye to near vision. However, ocular dominance is
typically assessed with sighting tasks which overlook the degree of eye dominance63.

188
Therefore, to measure the degree of ocular dominance, a binocular rivalry technique was
employed. The role of dominant eye assignment in modified and traditional monovision
was examined using the binocular adaptive optics vision simulator. High-contrast visual
acuity was not affected by subject’s degree of ocular dominance. However, we found that
the clinical convention of assigning the dominant eye to distance did improve contrast
sensitivity. Assessing patient’s ocular dominance is especially important maximizing
patient satisfaction in surgical monovision procedures which are not easily reversible.
Perceptual learning is an exciting new approach of improving visual performance
by way of neural plasticity. The plasticity of the adult visual system has been shown to
allow for perceptual learning to provide long-lasting improvements to vision in a wide
variety of patient populations, from optical maladies such as presbyopia18 and
keratoconus242, to neurological disorders such as amblyopia78 and stroke250. We therefore
applied perceptual learning to investigate its impact on visual performance in modified
monovision. Previous work91 has shown that perceptual learning is more effective when
retinal image quality is improved. Therefore, due to the optical benefits of modified
monovision, it was hypothesized to yield a greater visual benefit from vision training than
traditional monovision. The results presented in this thesis support the hypothesis. Indeed,
visual performance did improve more in the modified monovision group as compared to
traditional monovision after vision training. While these results are promising, they raise
several key questions. We performed vision training using single spatial frequency Gabor
stimuli. How does training transfer to other visual tasks, such as stereoacuity? What is the
optimal set of object distances for training? For how long do the effects of perceptual
learning last? Answering these questions will be important for future work. This study

189
opens the door to a host of possibilities for vision therapies aimed at improving visual
function beyond the limits imposed by optical quality. Theoretical models19, 83 of
perceptual learning suggest its mechanism lies in the reweighting of individual spatial
frequency channels in the neural system, suggesting adjustment of the neural contrast
sensitivity function. To elucidate the mechanism of perceptual learning in regard to
monocular versus binocular vision, it will be important to determine the neural contrast
sensitivity function of each eye independently in addition to binocularly. Thus the
anatomical region susceptible to perceptual learning, whether before or after convergence
of the monocular inputs to a single binocular channel, will be clarified. The binocular
adaptive optics vision simulator is an ideal tool for studying binocular visual function, in
addition to non-invasively assessing the performance of various ophthalmic surgical
procedures.
In addition to presbyopia correction, this thesis offers valuable insight and
methods for the area of childhood myopia progression. Around the world, the occurrence
of myopia progression is rapidly increasing, decreasing patients’ quality of life251 and
putting them at increased risk for potentially blinding conditions, such as glaucoma252
and retinal detachment253. Multifocal contact lenses have been proposed as an
intervention to slow the progression of myopia. However, the optical designs of such
myopia treatments are still in early phases and at risk for interfering with central vision.
Therefore, the approach embodied in this thesis is of direct consequence and value to the
field of myopia research.

190
References 1. Young T. The Bakerian Lecture: on the mechanism of the eye. Philosophical
Transactions of the Royal Society of London 1801;91:23-88. 2. Helmholtz H. Ueber die accommodation des auges. Graefe's Archive for Clinical
and Experimental Ophthalmology 1855;1:1-74. 3. Strenk SA, Strenk LM, Semmlow JL, DeMarco JK. Magnetic resonance imaging study of the effects of age and accommodation on the human lens cross-sectional area. Investigative ophthalmology & visual science 2004;45:539-545. 4. Strenk SA, Semmlow JL, Strenk LM, Munoz P, Gronlund-Jacob J, DeMarco JK. Age-related changes in human ciliary muscle and lens: a magnetic resonance imaging study. Investigative Ophthalmology & Visual Science 1999;40:1162-1169. 5. Glasser A, Campbell M. Biometric, optical and physical changes in the isolated human crystalline lens with age in relation to presbyopia. Vision Research 1999;39:1991-2015. 6. Pokorny J, Smith VC, Lutze M. Aging of the human lens. Applied Optics 1987;26:1437-1440. 7. Duane A. Normal values of the accommodation at all ages. Journal of the
American Medical Association 1912;59:1010-1013. 8. Glasser A, Campbell MC. Presbyopia and the optical changes in the human crystalline lens with age. Vision Research 1998;38:209-229. 9. Luo BP, Brown GC, Luo SC, Brown MM. The quality of life associated with presbyopia. American Journal of Ophthalmology 2008;145:618-622. 10. Parel J-M, Gelender H, Trefers W, Norton E. Phaco-Ersatz: cataract surgery designed to preserve accommodation. Graefe's Archive for Clinical and Experimental
Ophthalmology 1986;224:165-173. 11. Nishi Y, Mireskandari K, Khaw P, Findl O. Lens refilling to restore accommodation. Journal of Cataract & Refractive Surgery 2009;35:374-382. 12. Pepose J. Design strategies for new accommodating IOLs. Cataract & Refractive
Surgery Today 2009;9:39-45. 13. McLeod SD, Vargas LG, Portney V, Ting A. Synchrony dual-optic accommodating intraocular lens: Part 1: Optical and biomechanical principles and design considerations. Journal of Cataract & Refractive Surgery 2007;33:37-46. 14. Simonov AN, Vdovin G, Rombach MC. Cubic optical elements for an accommodative intraocular lens. Optics Express 2006;14:7757-7775. 15. Alió JL, Plaza-Puche AB, Montalban R, Ortega P. Near visual outcomes with single-optic and dual-optic accommodating intraocular lenses. Journal of Cataract &
Refractive Surgery 2012;38:1568-1575. 16. Cumming JS, Slade SG, Chayet A. Clinical evaluation of the model AT-45 silicone accommodating intraocular lens* 1:: Results of feasibility and the initial phase of a food and drug administration clinical trial. Ophthalmology 2001;108:2005-2009. 17. Pepose J. Maximizing satisfaction with presbyopia-correcting intraocular lenses: the missing links. American Journal of Ophthalmology 2008;146:641-648. 18. Polat U, Schor C, Tong J-L, et al. Training the brain to overcome the effect of aging on the human eye. Scientific Reports 2012;2.

191
19. Dosher BA, Lu Z-L. Mechanisms of perceptual learning. Vision Research 1999;39:3197-3221. 20. Wade NJ, Finger S. The eye as an optical instrument: from camera obscura to Helmholtz's perspective. Perception 2001;30:1157-1178. 21. von Helmholtz H, Southall JP. Helmholtz's treatise on physiological optics, Vol 1 (Trans. 1924. 22. Koretz JF, Strenk SA, Strenk LM, Semmlow JL. Scheimpflug and high-resolution magnetic resonance imaging of the anterior segment: a comparative study. JOSA A 2004;21:346-354. 23. Baikoff G, Lutun E, Ferraz C, Wei J. Static and dynamic analysis of the anterior segment with optical coherence tomography. Journal of Cataract & Refractive Surgery 2004;30:1843-1850. 24. Keeney AH, Hagman RE, Fratello CJ. Dictionary of ophthalmic optics: Butterworth-Heinemann; 1995. 25. Strenk SA, Strenk LM, Guo S. Magnetic resonance imaging of aging, accommodating, phakic, and pseudophakic ciliary muscle diameters. Journal of Cataract
& Refractive Surgery 2006;32:1792-1798. 26. Marcos S, Moreno E, Navarro R. The depth-of-field of the human eye from objective and subjective measurements. Vision Research 1999;39:2039-2049. 27. Bakaraju RC, Ehrmann K, Papas EB, Ho A. Depth-of-focus and its association with the spherical aberration sign. A ray-tracing analysis. Journal of Optometry 2010;3:51-59. 28. Yi F, Robert Iskander D, Collins M. Depth of focus and visual acuity with primary and secondary spherical aberration. Vision Research 2011;51:1648-1658. 29. Plakitsi A, Charman WN. Comparison of the depths of focus with the naked eye and with three types of presbyopic contact lens correction. Journal of The British Contact
Lens Association 1995;18:119-125. 30. Legras R, Hornain V, Monot A, Chateau N. Effect of induced anisometropia on binocular through-focus contrast sensitivity. Optometry & Vision Science 2001;78:503-509. 31. Wang B, Ciuffreda KJ. Depth-of-focus of the human eye: theory and clinical implications. Survey of Ophthalmology 2006;51:75-85. 32. Atchison DA, Charman WN, Woods RL. Subjective depth-of-focus of the eye. Optometry & Vision Science 1997;74:511-520. 33. Tucker J, Charman W. The depth-of-focus of the human eye for Snellen letters. American Journal of Optometry and Physiological Optics 1975;52:3-21. 34. Campbell FW. The depth of field of the human eye. Journal of Modern Optics 1957;4:157-164. 35. Ogle KN, Schwartz JT. Depth of focus of the human eye. Journal of the Optical
Society of America A 1959;49:273-279. 36. James R. The father of British optics: Roger Bacon, c. 1214-1294. The British
Journal of Ophthalmology 1928;12:1-14. 37. Menapace R, Findl O, Kriechbaum K, Leydolt-Koeppl C. Accommodating intraocular lenses: a critical review of present and future concepts. Graefe's Archive for
Clinical and Experimental Ophthalmology 2007;245:473-489.

192
38. Dick HB. Accommodative intraocular lenses: current status. Current Opinion in
Ophthalmology 2005;16:8-26. 39. Nishi O, Nakai Y, Yamada Y, Mizumoto Y. Amplitudes of accommodation of primate lenses refilled with two types of inflatable endocapsular balloons. Archives of
Ophthalmology 1993;111:1677-1684. 40. Gindi J, Wan WL, Schanzlin D. Endocapsular cataract surgery, I. Surgical
technique Cataract 1985;2:6-10. 41. Sheppard AL, Bashir A, Wolffsohn JS, Davies LN. Accommodating intraocular lenses: a review of design concepts, usage and assessment methods. Clinical and
Experimental Optometry 2010;93:441-452. 42. Hunter JJ, Campbell MCW, Geraghty E. Optical analysis of an accommodating intraocular lens. Journal of Cataract & Refractive Surgery 2006;32:269-278. 43. Koeppl C, Findl O, Menapace R, et al. Pilocarpine-induced shift of an accommodating intraocular lens: AT-45 Crystalens. Journal of Cataract & Refractive
Surgery 2005;31:1290-1297. 44. Sheedy JE, Truong SD, HAYES JR. What are the visual benefits of eyelid squinting? Optometry & Vision Science 2003;80:740-744. 45. Yilmaz ÖF, Bayraktar S, Agca A, Yilmaz B, McDonald MB, van de Pol C. Intracorneal inlay for the surgical correction of presbyopia. Journal of Cataract &
Refractive Surgery 2008;34:1921-1927. 46. Seyeddain O, Riha W, Hohensinn M, Nix G, Dexl AK, Grabner G. Refractive surgical correction of presbyopia with the AcuFocus small aperture corneal inlay: Two-year follow-up. Journal of Refractive Surgery 2010;26:707-715. 47. Steinman SB, Steinman BA, Garzia RP. Foundations of binocular vision: a
clinical perspective: McGraw-Hill New York; 2000. 48. Campbell FW, Green DG. Monocular versus binocular visual acuity. Nature 1965;208:191-192. 49. Sabesan R, Zheleznyak L, Yoon G. Binocular visual performance and summation after correcting higher order aberrations. Biomedical Optics Express 2012;3:3176-3189. 50. Cagenello R, Arditi A, Halpern DL. Binocular enhancement of visual acuity. Journal of the Optical Society of America A 1993;10:1841-1848. 51. Dodgson NA. Variation and extrema of human interpupillary distance. Electronic
Imaging 2004: International Society for Optics and Photonics; 2004:36-46. 52. Filippini HR, Banks MS. Limits of stereopsis explained by local cross-correlation. Journal of Vision 2009;9:1-18. 53. Lovasik JV, Szymkiw M. Effects of aniseikonia, anisometropia, accommodation, retinal illuminance, and pupil size on stereopsis. Investigative ophthalmology & visual
science 1985;26:741. 54. Johannsdottir KR, Stelmach LB. Monovision: a review of the scientific literature. Optometry & Vision Science 2001;78:646. 55. Hayashi K, Yoshida M, Manabe SI, Hayashi H. Optimal Amount of Anisometropia for Pseudophakic Monovision. Journal of refractive surgery (Thorofare,
NJ: 1995) 2010;1. 56. Schor C, Landsman L, Erickson P. Ocular dominance and the interocular suppression of blur in monovision. American journal of Optometry and Physiological
Optics 1987;64:723.

193
57. Collins M, Goode A, Brown B. Distance visual acuity and monovision. Optometry and vision science: official publication of the American Academy of
Optometry 1993;70:723. 58. Collins M, Bruce A, Thompson B. Adaptation to monovision. International
Contact Lens Clinic 1994;21:218-224. 59. Zheleznyak L, Sabesan R, Oh J-S, MacRae S, Yoon G. Modified monovision with spherical aberration to improve presbyopic through-focus visual performance. Investigative Ophthalmology & Visual Science 2013;54:3157-3165. 60. Handa T, Mukuno K, Uozato H, et al. Ocular dominance and patient satisfaction after monovision induced by intraocular lens implantation. Journal of Cataract &
Refractive Surgery 2004;30:769-774. 61. Blake R. A neural theory of binocular rivalry. Psychological Review 1989;96:145-167. 62. Dieter KC, Tadin D. Understanding attentional modulation of binocular rivalry: a framework based on biased competition. Front Hum Neurosci 2011;5:1-12. 63. Seijas O, Gómez de Liaño P, Gómez de Liaño R, Roberts CJ, Piedrahita E, Diaz E. Ocular dominance diagnosis and its influence in monovision. American Journal of
Ophthalmology 2007;144:209-216. 64. Handa T, Uozato H, Higa R, et al. Quantitative measurement of ocular dominance using binocular rivalry induced by retinometers. Journal of Cataract & Refractive
Surgery 2006;32:831-836. 65. Heinrich SP, Kromeier M, Bach M, Kommerell G. Vernier acuity for stereodisparate objects and ocular prevalence. Vision Research 2005;45:1321-1328. 66. Evans BJW. Monovision: a review. Ophthalmic and Physiological Optics 2007;27:417-439. 67. Hirsch J, Curcio CA. The spatial resolution capacity of human foveal retina. Vision Research 1989;29:1095-1102. 68. Williams DR. Aliasing in human foveal vision. Vision Research 1985;25:195-205. 69. Campbell FW, Green DG. Optical and retinal factors affecting visual resolution. Journal of Physiology (London) 1965;181:576-593. 70. Blakemore C, Campbell FW. On the existence of neurones in the human visual system selectively sensitive to the orientation and size of retinal images. Journal of
Physiology (London) 1969;203:237-260. 71. Maloney LT, Wandell BA. Color constancy: a method for recovering surface spectral reflectances. Journal of the Optical Society of America A 1986;3:29-33. 72. Neitz J, Carroll J, Yamauchi Y, Neitz M, Williams DR. Color perception is mediated by a plastic neural mechanism that is adjustable in adults. Neuron 2002;35:783-792. 73. Campbell F. Why do we measure contrast sensitivity? Behavioural Brain
Research 1983;10:87-97. 74. Williams DR. Visibility of interference fringes near the resolution limit. Journal
of the Optical Society of America A 1985;2:1087-1093. 75. Michael R, Guevara O, de la Paz M, Alvarez de Toledo J, Barraquer RI. Neural contrast sensitivity calculated from measured total contrast sensitivity and modulation transfer function. Acta Ophthalmologica 2011;89:278-283.

194
76. Yoon GY, Williams DR. Visual performance after correcting the monochromatic and chromatic aberrations of the eye. Journal of the Optical Society of America a-Optics
Image Science and Vision 2002;19:266-275. 77. Bradley A, Freeman R. Contrast sensitivity in anisometropic amblyopia. Investigative Ophthalmology & Visual Science 1981;21:467-476. 78. Levi DM. Perceptual learning in adults with amblyopia: A reevaluation of critical periods in human vision. Developmental Psychobiology 2005;46:222-232. 79. Gibson EJ. Perceptual learning. Annual review of psychology 1963;14:29-56. 80. Fahle M, Edelman S, Poggio T. Fast perceptual learning in hyperacuity. Vision
Research 1995;35:3003-3013. 81. Saarinen J, Levi DM. Perceptual learning in vernier acuity: what is learned? Vision Research 1995;35:519-527. 82. Zhou Y, Huang C, Xu P, et al. Perceptual learning improves contrast sensitivity and visual acuity in adults with anisometropic amblyopia. Vision Research 2006;46:739-750. 83. Dosher BA, Lu Z-L. Perceptual learning reflects external noise filtering and internal noise reduction through channel reweighting. Proceedings of the National
Academy of Sciences 1998;95:13988-13993. 84. Gantz L, Patel SS, Chung ST, Harwerth RS. Mechanisms of perceptual learning of depth discrimination in random dot stereograms. Vision Research 2007;47:2170-2178. 85. Fine I, Jacobs RA. Comparing perceptual learning across tasks: A review. Journal
of Vision 2002;2:190-203. 86. Sagi D, Tanne D. Perceptual learning: learning to see. Current Opinion in
Neurobiology 1994;4:195-199. 87. Levi DM, Polat U, Hu Y-S. Improvement in Vernier acuity in adults with amblyopia. Practice makes better. Investigative Ophthalmology & Visual Science 1997;38:1493-1510. 88. Hubel DH, Wiesel TN. Receptive fields and functional architecture of monkey striate cortex. The Journal of Physiology 1968;195:215-243. 89. Gold J, Bennett P, Sekuler A. Signal but not noise changes with perceptual learning. Nature 1999;402:176-178. 90. Huang C-B, Zhou Y, Lu Z-L. Broad bandwidth of perceptual learning in the visual system of adults with anisometropic amblyopia. Proceedings of the National
Academy of Sciences 2008;105:4068-4073. 91. Zhou J, Zhang Y, Dai Y, et al. The eye limits the brain's learning potential. Scientific Reports 2012;2:1-6. 92. Klein B, Klein R, Linton K. Prevalence of age-related lens opacities in a population. The Beaver Dam Eye Study. Ophthalmology 1992;99:546-552. 93. Findl O, Leydolt C. Meta-analysis of accommodating intraocular lenses. Journal
of Cataract & Refractive Surgery 2007;33:522-527. 94. Findl O, Kriechbaum K, Menapace R, et al. Laserinterferometric assessment of pilocarpine-induced movement of an accommodating intraocular lens: a randomized trial. Ophthalmology 2004;111:1515-1521. 95. Stachs O, Martin H, Kirchhoff A, Stave J, Terwee T, Guthoff R. Monitoring accommodative ciliary muscle function using three-dimensional ultrasound. Graefe's
Archive for Clinical and Experimental Ophthalmology 2002;240:906-912.

195
96. Marcos S, Ortiz S, Pérez-Merino P, Birkenfeld J, Durán S, Jiménez-Alfaro I. Three-Dimensional Evaluation of Accommodating Intraocular Lens Shift and Alignment In Vivo. Ophthalmology 2014;121:45-55. 97. Langenbucher A, Seitz B, Huber S, Nguyen NX, Kuchle M. Theoretical and measured pseudophakic accommodation after implantation of a new accommodative posterior chamber intraocular lens. Archives of Ophthalmology 2003;121:1722. 98. Marchini G, Mora P, Pedrotti E, Manzotti F, Aldigeri R, Gandolfi SA. Functional assessment of two different accommodative intraocular lenses compared with a monofocal intraocular lens. Ophthalmology 2007;114:2038-2043. 99. Plainis S, Petratou D, Giannakopoulou T, Atchison DA, Tsilimbaris MK. Binocular summation improves performance to defocus-induced blur. Investigative
Ophthalmology & Visual Science 2011;52:2784-2789. 100. Glasser A. Accommodation: mechanism and measurement. Ophthalmol Clin
North Am 2006;19:1-12. 101. Aldaba M, Vilaseca M, Díaz-Doutón F, Arjona M, Pujol J. Measuring the accommodative response with a double-pass system: Comparison with the Hartmann-Shack technique. Vision Research 2012;62:26-34. 102. Plainis S, Ginis HS, Pallikaris A. The effect of ocular aberrations on steady-state errors of accommodative response. Journal of Vision 2005;5. 103. Buehren TF, Collins MJ. Accommodation stimulus-response function and retinal image quality. Vision Research 2006;46:1633-1645. 104. Helmholtz Hv. Treatise on Physiological Optics. 2nd ed. New York: Dover; 1866. 105. Yoon G, Pantanelli S, MacRae S. Comparison of Zernike and Fourier wavefront reconstruction algorithms in representing corneal aberration of normal and abnormal eyes. Journal of Refractive Surgery 2008;24:582-590. 106. Prieto PM, Vargas-Martin F, Goelz S, Artal P. Analysis of the performance of the Hartmann–Shack sensor in the human eye. JOSA A 2000;17:1388-1398. 107. Atchison DA, Lucas SD, Ashman R, Huynh MA, SCHILT DW, Ngo PQ. Refraction and Aberration Across the Horizontal Central 10 [degrees] of the Visual Field. Optometry & Vision Science 2006;83:213-221. 108. Bedggood P, Daaboul M, Ashman R, Smith G, Metha A. Characteristics of the human isoplanatic patch and implications for adaptive optics retinal imaging. Journal of
Biomedical Optics 2008;13:024008-024008-024007. 109. Watson AB, Ahumada Jr AJ. Predicting visual acuity from wavefront aberrations. Journal of Vision 2008;8:1-19. 110. Applegate RA, Marsack JD, Ramos R, Sarver EJ. Interaction between aberrations to improve or reduce visual performance. Journal of Cataract and Refractive Surgery 2003;29:1487-1495. 111. Cheng X, Bradley A, Thibos LN. Predicting subjective judgment of best focus with objective image quality metrics. Journal of Vision 2004;4. 112. Thibos LN, Hong X, Bradley A, Applegate RA. Accuracy and precision of objective refraction from wavefront aberrations. Journal of Vision 2004;4:329-351. 113. Ripps H, Chin NB, SIEGEL IM, Breinin GM. The effect of pupil size on accommodation, convergence, and the AC/A ratio. Investigative ophthalmology & visual
science 1962;1:127-135.

196
114. Wolffsohn JS, Hunt OA, Naroo S, et al. Objective accommodative amplitude and dynamics with the 1CU accommodative intraocular lens. Investigative ophthalmology &
visual science 2006;47:1230-1235. 115. Kasthurirangan S, Glasser A. Age related changes in accommodative dynamics in humans. Vision Research 2006;46:1507-1519. 116. Kasthurirangan S, Glasser A. Age related changes in the characteristics of the near pupil response. Vision Research 2006;46:1393-1403. 117. Winn B, Whitaker D, Elliott D, Phillips NJ. Factors affecting light-adapted pupil size in normal human subjects. Investigative Ophthalmology & Visual Science 1994;35:1132-1137. 118. Watson AB, Yellott JI. A unified formula for light-adapted pupil size. Journal of
Vision 2012;12:1-16. 119. Cheng H, Barnett JK, Vilupuru AS, et al. A population study on changes in wave aberrations with accomodation. Journal of Vision 2004;4:272-280. 120. He JC, Burns SA, Marcos S. Monochromatic aberrations in the accommodated human eye. Vision Research 2000;40:41-48. 121. Cazal J, Lavin-Dapena C, Marín J, Vergés C. Accommodative intraocular lens tilting. American journal of ophthalmology 2005;140:341-344. 122. Jardim D, Soloway B, Starr C. Asymmetric vault of an accommodating intraocular lens. Journal of Cataract & Refractive Surgery 2006;32:347-350. 123. Davison JA, Simpson MJ. History and development of the apodized diffractive intraocular lens. Journal of Cataract & Refractive Surgery 2006;32:849-858. 124. Montés-Micó R, España E, Bueno I, Charman WN, Menezo JL. Visual performance with multifocal intraocular lenses: mesopic contrast sensitivity under distance and near conditions. Ophthalmology 2004;111:85-96. 125. Pieh S, Weghaupt H, Skorpik C. Contrast sensitivity and glare disability with diffractive and refractive multifocal intraocular lenses. Journal of Cataract & Refractive
Surgery 1998;24:659-662. 126. Zhao G, Zhang J, Zhou Y, Hu L, Che C, Jiang N. Visual function after monocular implantation of apodized diffractive multifocal or single-piece monofocal intraocular lens: Randomized prospective comparison. Journal of Cataract & Refractive Surgery 2010;36:282-285. 127. Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. Journal of Cataract & Refractive Surgery 2009;35:992-997. 128. Pieh S, Lackner B, Hanselmayer G, et al. Halo size under distance and near conditions in refractive multifocal intraocular lenses. British journal of ophthalmology 2001;85:816-821. 129. Choi J, Schwiegerling J. Optical performance measurement and night driving simulation of ReSTOR, ReZoom, and Tecnis multifocal intraocular lenses in a model eye. Journal of Refractive Surgery 2008;24:218-222. 130. de Vries NE, Webers CA, Touwslager WR, et al. Dissatisfaction after implantation of multifocal intraocular lenses. Journal of Cataract & Refractive Surgery 2011;37:859-865. 131. Artal P, Guirao A, Berrio E, Williams D. Compensation of corneal aberrations by the internal optics in the human eye. Journal of Vision 2001;1:1-8.

197
132. Artal P, Benito A, Tabernero J. The human eye is an example of robust optical design. Journal of Vision 2006;6. 133. Guirao A, Redondo M, Artal P. Optical aberrations of the human cornea as a function of age. Journal of the Optical Society of America A 2000;17:1697-1702. 134. Guirao A, Tejedor J, Artal P. Corneal aberrations before and after small-incision cataract surgery. Investigative Ophthalmology & Visual Science 2004;45:4312-4319. 135. Guirao A, Redondo M, Geraghty E, Piers P, Norrby S, Artal P. Corneal optical aberrations and retinal image quality in patients in whom monofocal intraocular lenses were implanted. Archives of Ophthalmology 2002;120:1143-1151. 136. Sabesan R, Ahmad K, Yoon G. Correcting highly aberrated eyes using large-stroke adaptive optics. Journal of Refractive Surgery 2007;23:947-952. 137. Kim MJ, Zheleznyak L, MacRae S, Tchah H, Yoon G. Objective evaluation of through-focus optical performance of presbyopia-correcting intraocular lenses using an optical bench system. Journal of Cataract & Refractive Surgery 2011;37:1305-1312. 138. Chen M, Yoon G. Posterior corneal aberrations and their compensation effects on anterior corneal aberrations in keratoconic eyes. Investigative Ophthalmology & Visual
Science 2008;49:5645-5652. 139. Zheleznyak L, Kim MJ, MacRae S, Yoon G. Impact of corneal aberrations on through-focus image quality of presbyopia-correcting intraocular lenses using an adaptive optics bench system. Journal of Cataract & Refractive Surgery 2012;38:1724-1733. 140. International Organization for Standardization. Ophthalmic Implants - Intraocular Lenses - Part 2: Optical Properties and Test Methods. ISO 11979-2. 1999. 141. Portney V. Light distribution in diffractive multifocal optics and its optimization. Journal of Cataract & Refractive Surgery 2011;37:2053-2059. 142. Maxwell W, Lane S, Zhou F. Performance of presbyopia-correcting intraocular lenses in distance optical bench tests. Journal of Cataract & Refractive Surgery 2009;35:166-171. 143. Terwee T, Weeber H, van der Mooren M, Piers P. Visualization of the retinal image in an eye model with spherical and aspheric, diffractive, and refractive multifocal intraocular lenses. Journal of Refractive Surgery 2008;24:223-232. 144. Pepose JS, Wang D, Altmann GE. Comparison of through-focus image sharpness across five presbyopia-correcting intraocular lenses. American Journal of Ophthalmology 2012;154:20-28. 145. Hayashi K, Manabe S, Yoshida M, Hayashi H. Effect of astigmatism on visual acuity in eyes with a diffractive multifocal intraocular lens. Journal of Cataract &
Refractive Surgery 2010;36:1323-1329. 146. Ronchi L, Molesini G. Depth of focus in peripheral vision. Ophthalmic Research 1975;7:152-157. 147. Legras R, Benard Y, Rouger H. Through-focus visual performance measurements and predictions with multifocal contact lenses. Vision Research 2010;50:1185-1193. 148. Guo H, Atchison DA, Birt BJ. Changes in through-focus spatial visual performance with adaptive optics correction of monochromatic aberrations. Vision
Research 2008;48:1804-1811. 149. Legge GE, Mullen KT, Woo GC, Campbell F. Tolerance to visual defocus. Journal of the Optical Society of America A 1987;4:851-863.

198
150. Hickenbotham A, Tiruveedhula P, Roorda A. Comparison of spherical aberration and small-pupil profiles in improving depth of focus for presbyopic corrections. Journal
of Cataract & Refractive Surgery 2012;38:2071-2079. 151. Tabernero J, Artal P. Optical modeling of a corneal inlay in real eyes to increase depth of focus: optimum centration and residual defocus. Journal of Cataract &
Refractive Surgery 2012;38:270-277. 152. Nio Y, Jansonius N, Fidler V, Geraghty E, Norrby S, Kooijman A. Spherical and irregular aberrations are important for the optimal performance of the human eye. Ophthalmic and Physiological Optics 2002;22:103-112. 153. Martin JA, Roorda A. Predicting and assessing visual performance with multizone bifocal contact lenses. Optometry & Vision Science 2003;80:812-819. 154. Bradley A, Rahman HA, Soni PS, Zhang X. Effects of target distance and pupil size on letter contrast sensitivity with simultaneous vision bifocal contact lenses. Optometry & Vision Science 1993;70:476-481. 155. Keates RH, Martines E, Tennen DG, Reich C. Small-diameter corneal inlay in presbyopic or pseudophakic patients. Journal of Cataract & Refractive Surgery 1995;21:519-521. 156. Limnopoulou AN, Bouzoukis DI, Kymionis GD, et al. Visual outcomes and safety of a refractive corneal inlay for presbyopia using femtosecond laser. J Refract Surg 2013;29:12-18. 157. Alió JL, Chaubard JJ, Caliz A, Sala E, Patel S. Correction of presbyopia by technovision central multifocal LASIK (presbyLASIK). Journal of Refractive Surgery 2006;22:453-460. 158. Epstein RL, Gurgos MA. Presbyopia treatment by monocular peripheral presbyLASIK. J Refract Surg 2009;25:516-523. 159. Sabesan R, Yoon G. Visual performance after correcting higher order aberrations in keratoconic eyes. Journal of Vision 2009;9:6. 160. Schoneveld P, Pesudovs K, Coster DJ. Predicting visual performance from optical quality metrics in keratoconus. Clinical and Experimental Optometry 2009;92:289-296. 161. Chen L, Singer B, Guirao A, Porter J, Williams DR. Image metrics for predicting subjective image quality. Optometry & Vision Science 2005;82:358-369. 162. Marsack JD, Thibos LN, Applegate RA. Metrics of optical quality derived from wave aberrations predict visual performance. Journal of Vision 2004;4. 163. Tolhurst D, Tadmor Y, Chao T. Amplitude spectra of natural images. Ophthalmic
and Physiological Optics 1992;12:229-232. 164. Bex PJ, Makous W. Spatial frequency, phase, and the contrast of natural images. JOSA A 2002;19:1096-1106. 165. Watson AB, Barlow HB, Robson JG. What does the eye see best? Nature 1983;302:419-422. 166. Applegate RA, Lakshminarayanan V. Parametric representation of Stiles-Crawford functions: normal variation of peak location and directionality. Journal of the
Optical Society of America A 1993;10:1611-1623. 167. Mutti D, Zadnik K, Egashira S, Kish L, Twelker J, Adams A. The effect of cycloplegia on measurement of the ocular components. Investigative Ophthalmology &
Visual Science 1994;35:515-527.

199
168. Iskander RD, Davis BA, Collins MJ, Franklin R. Objective refraction from monochromatic wavefront aberrations via Zernike power polynomials. Ophthalmic and
Physiological Optics 2007;27:245-255. 169. Watson AB, Pelli DG. QUEST: A Bayesian adaptive psychometric method. Attention, Perception, & Psychophysics 1983;33:113-120. 170. Zheleznyak L, Jung H, Yoon G. Impact of pupil transmission apodization on presbyopic through-focus visual performance with spherical aberration. Investigative
Ophthalmology & Visual Science 2014;55:70-77. 171. Ravikumar S, Bradley A, Thibos L. Phase changes induced by optical aberrations degrade letter and face acuity. Journal of Vision 2010;10:1-12. 172. Iskander DR. Computational aspects of the visual Strehl ratio. Optometry &
Vision Science 2006;83:57-59. 173. Gonzalez RC, Woods RE, Eddins SL. Digital image processing using MATLAB: Pearson Education India; 2004. 174. Thibos LN, Applegate RA, Schwiegerling JT, Webb R. Standards for reporting the optical aberrations of eyes. Journal of Refractive Surgery 2002;18:S652-S660. 175. Cheng X, Bradley A, Ravikumar S, Thibos LN. The visual impact of Zernike and Seidel forms of monochromatic aberrations. Optometry and Vision Science 2010;87:300-312. 176. Benard Y, Lopez-Gil N, Legras R. Subjective depth of field in presence of 4th-order and 6th-order Zernike spherical aberration using adaptive optics technology. Journal of Cataract & Refractive Surgery 2010;36:2129-2138. 177. Xu R, Bradley A, Thibos LN. Impact of primary spherical aberration, spatial frequency and Stiles Crawford apodization on wavefront determined refractive error: a computational study. Ophthalmic and Physiological Optics 2013;33:444-455. 178. Benard Y, Lopez-Gil N, Legras R. Optimizing the subjective depth-of-focus with combinations of fourth-and sixth-order spherical aberration. Vision Research 2011. 179. Atchison DA, Fisher SW, Pedersen CA, Ridall PG. Noticeable, troublesome and objectionable limits of blur. Vision Research 2005;45:1967-1974. 180. Leyland M, Zinicola E. Multifocal versus monofocal intraocular lenses in cataract surgery: a systematic review. Ophthalmology 2003;110:1789-1798. 181. Montés-Micó R, Alió J. Distance and near contrast sensitivity function after multifocal intraocular lens implantation. Journal of Cataract & Refractive Surgery 2003;29:703-711. 182. Dick HB, Krummenauer F, Schwenn O, Krist R, Pfeiffer N. Objective and subjective evaluation of photic phenomena after monofocal and multifocal intraocular lens implantation. Ophthalmology 1999;106:1878-1886. 183. Goodman JW. Introduction to Fourier Optics. 3rd ed. Englewood, CO: Roberts and Company Publishers; 2005. 184. McLellan J, Marcos S, Burns S. Age-related changes in monochromatic wave aberrations of the human eye. Investigative ophthalmology & visual science 2001;42:1390. 185. Stiles W, Crawford B. The luminous efficiency of rays entering the eye pupil at different points. Proceedings of the Royal Society of London Series B 1933;112:428-450.

200
186. Zhang X, Ye M, Bradley A, Thibos L. Apodization by the Stiles-Crawford effect moderates the visual impact of retinal image defocus. Journal of the Optical Society of
America A 1999;16:812-820. 187. Atchison DA, Scott DH, Strang NC, Artal P. Influence of Stiles–Crawford apodization on visual acuity. Journal of the Optical Society of America A 2002;19:1073-1083. 188. Mino M, Okano Y. Improvement in the OTF of a defocused optical system through the use of shaded apertures. Applied Optics 1971;10:2219-2225. 189. Atchison DA, Joblin A, Smith G. Influence of Stiles–Crawford effect apodization on spatial visual performance. Journal of the Optical Society of America A 1998;15:2545-2551. 190. Thorn F, Schwartz F. Effects of dioptric blur on Snellen and grating acuity. Optometry & Vision Science 1990;67:3-7. 191. Akutsu H, Bedell HE, Patel SS. Recognition thresholds for letters with simulated dioptric blur. Optometry & Vision Science 2000;77:524-530. 192. Oyster CW. The Human Eye: Structure and Function. Sunderland, MA: Sinauer Associates, Inc.; 1999. 193. De Valois RL, Morgan H, Snodderly DM. Psychophysical studies of monkey vision-III. Spatial luminance contrast sensitivity tests of macaque and human observers. Vision Research 1974;14:75-81. 194. Banks MS, Geisler WS, Bennett PJ. The physical limits of grating visibility. Vision Research 1987;27:l915-1924. 195. Jain S, Arora I, Azar DT. Success of monovision in presbyopes: Review of the literature and potential applications to refractive surgery*. Survey of Ophthalmology 1996;40:491-499. 196. Legge GE. Binocular contrast summation - II. Quadratic summation. Vision
Research 1984;24:385-394. 197. Pardhan S, Gilchrist J. The effect of monocular defocus on binocular contrast sensitivity. Ophthalmic and Physiological Optics 1990;10:33-36. 198. Westheimer G, McKee SP. Stereoscopic acuity with defocused and spatially filtered retinal images. Journal of the Optical Society of America A 1980;70:772-778. 199. Reinstein DZ, Couch DG, Archer TJ. LASIK for hyperopic astigmatism and presbyopia using micro-monovision with the Carl Zeiss Meditec MEL80 platform. Journal of Refractive Surgery 2009;25:37. 200. Reinstein DZ, Archer TJ, Gobbe M. LASIK for Myopic Astigmatism and Presbyopia Using Non-Linear Aspheric Micro-Monovision with the Carl Zeiss Meditec MEL 80 Platform. Journal of Refractive Surgery 2011;27:23. 201. Reinstein DZ. Aspheric ablation profile for presbyopic corneal treatment using the MEL80 and CRS Master Laser Blended Vision module. Journal of Emmetropia 2011;161-175. 202. Yoon G, MacRae S, Williams DR, Cox IG. Causes of spherical aberration induced by laser refractive surgery. Journal of Cataract & Refractive Surgery 2005;31:127-135. 203. Liang J, Grimm B, Goelz S, Bille J. Objective measurement of the wave aberrations of the human eye using a Hartmann-Shack wavefront sensor. Journal of the
Optical Society of America A 1994;11:1949-1957.

201
204. Yoon G, Pantanelli, S., MacRae, S. Optimizing the Shack-Hartmann Wavefront
Sensor. Thorofare, NJ: SLACK Inc.; 2004:131-136. 205. Dubra A. Wavefront sensor and wavefront corrector matching in adaptive optics. Optics Express 2007;15:2762-2769. 206. Porter J, Queener H, Lin J, Thorn K, Awwal AA. Adaptive optics for vision
science: Principles, practices, design and applications: John Wiley & Sons; 2006. 207. Hirsch J, Curcio CA. The spatial resolution capacity of human foveal retina. Vision Research 1989;29:1095-1101. 208. Tyler CW, Chan H, Liu L, McBride B, Kontsevich LL. Bit stealing: how to get 1786 or more gray levels from an 8-bit color monitor. SPIE/IS&T 1992 Symposium on
Electronic Imaging: Science and Technology: International Society for Optics and Photonics; 1992:351-364. 209. Loshin D, Loshin M, Comer G. Binocular summations with monovision contact lens correction for presbyopic patients. Int Contact Lens Clin 1982;9:161-165. 210. Collins M, Goode A, Brown B. Distance visual acuity and monovision. Optometry and Vision Science 1993;70:723. 211. Fisher K. Presbyopic visual performance with modified monovision using multifocal soft contact lenses. International Contact Lens Clinic 1997;24:91-100. 212. Richdale K, Mitchell GL, Zadnik K. Comparison of multifocal and monovision soft contact lens corrections in patients with low-astigmatic presbyopia. Optometry &
Vision Science 2006;83:266-273. 213. Tabernero J, Schwarz C, Fernández EJ, Artal P. Binocular visual simulation of a corneal inlay to increase depth of focus. Investigative ophthalmology & visual science 2011;52:5273-5277. 214. Fernández EJ, Schwarz C, Prieto PM, Manzanera S, Artal P. Impact on stereo-acuity of two presbyopia correction approaches: monovision and small aperture inlay. Biomedical Optics Express 2013;4:822-830. 215. García-Lázaro S, Ferrer-Blasco T, Radhakrishnan H, Cerviño A, Charman WN, Montés-Micó R. Visual function through 4 contact lens–based pinhole systems for presbyopia. Journal of Cataract & Refractive Surgery 2012;38:858-865. 216. Plainis S, Petratou D, Giannakopoulou T, Radhakrishnan H, Pallikaris IG, Charman WN. Reduced-aperture monovision for presbyopia and the Pulfrich effect. Journal of Optometry 2012;5:156-163. 217. Kommerell G, Schmitt C, Kromeier M, Bach M. Ocular prevalence versus ocular dominance. Vision Research 2003;43:1397-1403. 218. Miles WR. Ocular dominance in human adults. The journal of general psychology 1930;3:412-430. 219. Rice ML, Leske DA, Smestad CE, Holmes JM. Results of ocular dominance testing depend on assessment method. Journal of American Association for Pediatric
Ophthalmology and Strabismus 2008;12:365-369. 220. Walls GL. A theory of ocular dominance. Archives of Ophthalmology 1951;45:387. 221. Gronwall DM, Sampson H. Ocular dominance: a test of two hypotheses. British
Journal of Psychology 1971;62:175-185. 222. Coren S, Kaplan C. Patterns of ocular dominance. American journal of optometry
and archives of American Academy of Optometry 1973;50:283.

202
223. Carey DP. Vision research: Losing sight of eye dominance. Current Biology 2001;11:R828-R830. 224. Khan AZ, Crawford JD. Ocular dominance reverses as a function of horizontal gaze angle. Vision Research 2001;41:1743-1748. 225. Banks MS, Ghose T, Hillis JM. Relative image size, not eye position, determines eye dominance switches. Vision Research 2004;44:229-234. 226. Miles WR. Ocular dominance demonstrated by unconscious sighting. Journal of
Experimental Psychology 1929;12:113. 227. Handa T, Mukuno K, Uozato H, Niida T, Shoji N, Shimizu K. Effects of dominant and nondominant eyes in binocular rivalry. Optometry & Vision Science 2004;81:377-383. 228. Pointer JS. Sighting versus sensory ocular dominance. Journal of Optometry 2012;5:52-55. 229. Daw NW. Critical periods and amblyopia. Archives of Ophthalmology 1998;116:502-505. 230. Lema SA, Blake R. Binocular summation in normal and stereoblind humans. Vision Research 1977;17:691-695. 231. Handa T, Shimizu K, Mukuno K, Kawamorita T, Uozato H. Effects of ocular dominance on binocular summation after monocular reading adds. Journal of Cataract &
Refractive Surgery 2005;31:1588-1592. 232. Blake R, Fox R. Binocular rivalry suppression: Insensitive to spatial frequency and orientation change. Vision Research 1974;14:687-692. 233. Mon-Williams M, Tresilian J, Strang N, Kochhar P, Wann J. Improving vision: neural compensation for optical defocus. Proceedings: Biological Sciences 1998;265:71-77. 234. Webster M, Georgeson M, Webster S. Neural adjustments to image blur. Nature
Neuroscience 2002;5:839-840. 235. Sabesan R, Yoon G. Neural compensation for long-term asymmetric optical blur to improve visual performance in keratoconic eyes. Investigative ophthalmology & visual
science 2010;51:3835-3839. 236. Artal P, Chen L, Fernández E, Singer B, Manzanera S, Williams D. Neural compensation for the eye s optical aberrations. Journal of Vision 2004;4:281-287. 237. Sawides L, de Gracia P, Dorronsoro C, Webster MA, Marcos S. Vision is adapted to the natural level of blur present in the retinal image. PLoS One 2011;6:e27031. 238. Georgeson MA, Sullivan GD. Contrast constancy: Deblurring in human vision by spatial frequency channels. Journal of Physiology (London) 1975;253:627-656. 239. Sabesan R, Jeong T, Carvalho L, Cox I, Williams D, Yoon G. Vision improvement by correcting higher-order aberrations with customized soft contact lenses in keratoconic eyes. Optics Letters 2007;32:1000-1002. 240. Sabesan R, Johns L, Tomashevskaya O, Jacobs DS, Rosenthal P, Yoon G. Wavefront-guided scleral lens prosthetic device for keratoconus. Optometry & Vision
Science 2013;90:314-323. 241. Sabesan R. Interaction Between Optical and Neural Factors Affecting Visual Performance. University of Rochester; 2011. 242. Sabesan R, Yoon G. Neural plasticity stimulated by perceptual learning with adaptive optics. Journal of Vision 2012;12:49-49.

203
243. Schoups AA, Orban GA. Interocular transfer in perceptual learning of a pop-out discrimination task. Proceedings of the National Academy of Sciences 1996;93:7358-7362. 244. Polat U. Making perceptual learning practical to improve visual functions. Vision
Research 2009;49:2566-2573. 245. Durrie D, McMinn PS. Computer-based primary visual cortex training for treatment of low myopia and early presbyopia. Transactions of the American
Ophthalmological Society 2007;105:132. 246. Dang-Vu TT, Desseilles M, Peigneux P, Maquet P. A role for sleep in brain plasticity. Developmental Neurorehabilitation 2006;9:98-118. 247. Duncan Jr WC, Zarate Jr CA. Ketamine, Sleep, and Depression: Current Status and New Questions. Current psychiatry reports 2013;15:1-7. 248. Sheedy JE, Harris MG, Gan CM. Does the presbyopic visual system adapt to contact lenses? Optometry & Vision Science 1993;70:482-486. 249. Li R, Polat U, Makous W, Bavelier D. Enhancing the contrast sensitivity function through action video game training. Nature Neuroscience 2009;12:549-551. 250. Das A, Huxlin KR. New approaches to visual rehabilitation for cortical blindness: Outcomes and putative mechanisms. The Neuroscientist 2010;16:374-387. 251. Rose K, Harper R, Tromans C, et al. Quality of life in myopia. British journal of
ophthalmology 2000;84:1031-1034. 252. Mitchell P, Hourihan F, Sandbach J, Jin Wang J. The relationship between glaucoma and myopia: the Blue Mountains Eye Study. Ophthalmology 1999;106:2010-2015. 253. Pierro L, Camesasca F, Mischi M, Brancato R. Peripheral retinal changes and axial myopia. Retina 1992;12:12-17.