Embed Size (px)
Citation preview

Global screening and eradication of Helicobacter pylori
Peter MalfertheinerKlinik für Gastroenterologie, Hepatologie und Infektiologie
Otto‐von‐Guericke‐Universität Magdeburg

Points to consider
• Size of the problem• Options for solution• H.pylori screening and eradication

Alcohol
Main effect on the esophagus!
No ? influence on gastric carcinogenesis
Franke DigDis 2005

Global burden of cancer• 7.9 million (= 13% of all deaths) worldwide in 2007• 72% of all cancer deaths in 2007 occurred in low- and middle-income
countries• Gastrointestinal- represent highest contingent
• Gastric cancer „ranks“ sadly second concerning death rate
WHO Fact sheet N° 297, July 2008

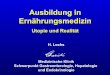
Age-standardized Incidence Rates for Gastric Cancer Data shown per 100,000
Parkin DM et al. Global Cancer Statistics, 2002
• Geographic distribution of gastric shows wide international variations.
• High-risk areas (ASR in men, >20 per 100,000) include East Asia (China, Japan), Eastern Europe, and parts of Central and South America.
• Incidence rates are low (<10 per 100,000 in men) in Southern Asia, North and East Africa, North America, and Australia and New Zealand

40% of patients with no dyspeptic symptoms
• Dyspepsia
• nausea and vomit
• Epigastric pain
• no appetite
• weight loss
GASTRIC CANCERVariable symptoms,usually as red flags in advanced stage

Points to consider
• Size of the problem
•Options for solution other than• H.pylori screening and eradication

Gastric cancer prevention
•Options for solution• Diet change• Stop smoking• chemoprevention

Vegetables / citrus fruits
• Protective effect?– High content of anti-oxidants, Vit A / E / C– Vegetables „possibly“ and fruits „likely“ protective– Garlic: 1 positive meta-analysis, overall: contrary results
Gonzalez Int J Cancer 2006Bae Gastric Cancer 2008
0.72 [0.64 – 0.81]

Salt• Increased risk in case of higher
salt intake (up to 2.5-fold)• Heterogenous results• Influence decreasing in
Western countries (refridgerators, modern means of food conservation)
Interference with the mucosal barrier
Higher occurence of nitroso-compounds
Peleteiro BrJCanc 2011Sjödahl CancEpidBiomPrev 2008Tsugane CancSci 2005Fox&Wang NEJM 2001
! Influence only in case of pre-existing gastric mucosal damage
H. pylori !

Slide withheld at request of author
Online Lecture Library

Slide withheld at request of author
Online Lecture Library

Chemo-Prevention
• Antioxidants (H. pylori lower bio-availability of Vit C)
• COX- inhibitors (ASA, NSAIDs, COX-2-Inhib.)

Points to consider
• Size of the problem• Options for solution• H.pylori screening and eradication

Screen and treat H. pylori in prevention of gastric cancer
RATIONALE behind
H. pylori infection and gastric cancer link ••Epidemiology
•Histological cascade
• Molecular events in gastric carcinogenesis
• Experimental models (cell biology, animal models)

Cases – Controls
n 68 n 360
Exclusion: T4 gastric cancerSerum taken > 90 day following gastrectomyCag A not considered if H. pylori negative
H. pylori + Cag - OR 3,7 18,3
H. pylori + Cag + OR 5,7 28,4
Brenner et al., Am J Epidemiol 2004, 159:252-258
Necessary condition for gastric cancer development

H.pylori and Gastric Cancer
EpidemiologyHow relevant is the location?distal versus proximal
How relevant is the histological type?intestinal versus diffuse

Gastric cancer
Siewert Br J Surg 1998
proximal
distal
AEG: Adenocacrinoma of the oesophagogastric junction
Tumor allocation
AEG IIAEG IIIProx. 1/3 corpus
Dist. 2/3 corpusAntrum
H.pylori infection with similar association in proximal AEG I-II and distal gastric cancerBornschein et al DDW 2009

Gastric cancer
in corpus
intestinal type
Gastric cancersubcardialintestinal type

Screen and treat H. pylori in prevention of gastric cancer
H. pylori infection and gastric cancer link
••Role of host genes
•Bacterial virulence factors
• Ambiental and nutritional factors

El Omar et al Gastroenterology 2000
0
5
10
15
20
25
30
35
Hypochlorhydria Atrophy
27%
34%
relatives of gastric cancer patients (n100), H. pylori prevalence 63%
3% 5%
control subjects (n 100) ), H. pylori prevalence 64%%
of s
ubje
cts
H.pylori plusgeneticpre-
disposition..IL 1 –beta polymorphisms
H. pylori and gastric cancer

Increased polymorphisms of pro-inflammatory genes and risk of non-cardia gastric cancer
Polymorphisms of IL-1β(o), IL-1 receptor antagonist, TNFα, and IL-10 conferred a greater risk for gastric cancer
ORs (95% CI) •Single gene 2.8 (1.6-5.1) •Two genes 5.4 (2.7-10.6)•Three or four genes 27.3 (7.4-99.8)
El-Omar EM, et al. Gastroenterology,2003;124:1193-201

H. pylori virulence factors
increase the risk of gastric cancer
Cag A, Vac A and others
cause stronger inflammatory reaction-preneoplastic conditions

Pro-inflammatory cytokine gene polymorphismsIL-1B-511*TIL-1RN*2*2IL-10 ATA haplotypeTNF-A-308*A
Innate immune response gene polymorphismsTLR4+896*G
Bacterial factorsCag AVac A s1/i1/m1
Environmental factorssmokingdiet
Bacterial-Host- Environmental factors
in H. pylori-related gastric cancer
Gastric cancer
SUMMARY

H. pylori infection and gastric cancer: A prospective endoscopy study
• 1526 patients with NUD, DU, GU or gastrichyperplasia (GH)
• Endoscopy: enrollment and every 1-3
years Uemura et al, N Engl J Med 2001; 345:784
Hp- Hp+ NUD GU GH DU
0
2,9
4,7
3,4
2,2
00
1
2
3
4
5Incidence of gastric cancer (%)

• Metaanalysis 6 studies >6000 patients
Fuccio et al Ann Int Med 2009
H.pylori eradication and gastric cancer prevention
Number needed to treat 227!

7
11
0
10
20%
OAM Placebo
OAM Placebo
P=0.95
0
5
0
10
20%
OAM Placebo
OAM Placebo
6
Gastric cancerGastric cancer in subjects with no preneoplastic changes on entry
Eradication H. pylori infection In a general population prevents gastric cancer:
A 7-year prospective randomized placebo-controlled study
Wong et al. JAMA2004
p=0.025

Where is the point of no return?

Probability of regression of the pre-neoplastic lesions
Gastric cancer
Prob
abili
ty o
f reg
ress
ion
Infection with H.pylori
Atrophic gastritisIntestinal
metaplasia
Dysplasia
months years decades
Chronic active gastritis
H. pylori and gastric cancer

Fukase et al Lancet 2008
H.pylori eradication after EMR of early gastric cancer=never to late!!!!!!
• 3 year follow up:
• gastric cancer relapse– controls: 24– After eradication: 9
•OR for metachronous NPL0.353 (95% CI 0.161-0.775)
•HR (intent. to treat)0.339 (95% CI 0.157-0.729)

Does H. pylori eradication therapy for PUD prevent gastric cancer ?
Mabe et al. World J Gastroenterol 2009;15(34):4290-97
„Yamagata Prefecture, Japan“Study 2000-2007, follow up 5,6 years
4133 patients with PUD
Gastric cancer
0,21 %/year
Gastric cancer
0,50 %/year
Eradication therapy no Eradication therapy

Mabe et al. World J Gastroenterol 2009;15(34):4290-97
Proportion free of gastric cancer in the eradication group was compared according to results of eradication therapy, using Kaplan-Meier analysis.

H. pylori eradication in the prevention of gastric cancer
ERADICATIONNNT 227
But consider additional benefits:Ulcer prevention,cure of dyspepsia,extragastric disease

Global screening andH.pylori eradication?
NoBut……

Surveillance for gastric cancer –DECISION MODEL
Yearly endoscopy for 10 years after newly detected gastric IM in 10.000 Americans
- estimated gastric cancer incidence 1,8%/year
- 556 (3738) endoscopies for detection of 1 gastric cancer
- US $ 72.519 per life year gained
Hassan et al Helicobacter 2010; 15:221

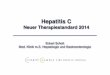
Geographic differences in gastric cancer incidence explained by differences between H. pylori strains
Yamaoka Y. et al. Internal Medicine. 2008; 47(12):1077-83
Present distribution of six main H. pylori genotypes
The circles coincide with countries in which the H. pylori genotypes have been
examined

Gastric cancer
Actions to take
Screening for early gastric cancer
Screening & treating H.pylori
Surveillance of chronic gastritis and IM

Gastric cancer screening and subsequent risk of gastric cancer
Population 42.150 36 % screened by photofluorography
2 fold decrease in gastric cancer mortality in screened vs non screened
13 years follow up
Lee KJ et al, Int. J. Cancer 2006;118,9
Gastric cancer screening associated with reduced risk of mortality
RR 0.54CI 0.36-0.74
179 cancer deaths
636incident cancer

Gastric cancer
studies from Japan show a twofold risk reduction for gastric cancer mortality
Lee at al. Int J Cancer 2006
Significant higher number of early gastric cancer with screening endoscopy
Hosokawa et al. Scand J Gastroenterol 2008
Nam et al. Europ J Gastroenterol Hepatol 2009
•Population based screening

How to select subjects at risk
for gastric cancer development?
At presentNo role for determinationof cytokine related gene polymorphisms
No role for determination of bacterial virulence
What about histology???

Risk gastritisWell established

Multifocal atrophyaccompaniedby intest. metaplasia
Auto immune Corpus-predominant with antrum normal
Initial infection
Antrum predominant,Minimal corpus Involvement
gastriccancerGastric Cancer
Chronic gastritis phenotypein gastric cancer
Host susceptibilty. Bacterial strain virulenceenvironment

Chronic atrophic gastritis

Atropphy and Intestinal Metaplasia
Narrow band imaging

Atrophic gastritis

Atrophic border

Atrophie
mit intestinaler Metaplasie
Atrophic gastritis an IM

HistologyAbnormalities atBase Line
All HP+Patients(n=1246)
HP+ Patientswith Gastric Ca
(n=36)
Relative Risk(95% CI)*
Grade of atrophyNone or mild 381 3 (0.8) 1.0Moderate 657 18 (2.7) 1.7 (0.8–3.7)
Severe 208 15 (7.2) 4.9 (2.8–19.2)
Distribution of gastritisAntrum predominant 699 2 (0.3) 1.0Pangastritis 337 14 (4.2) 15.6 (6.5–36.8)
Corpus predominant 210 20 (9.5) 34.5 (7.1–166.7)
N Uemura. N Engl J Med 2001; 345:794-9Follow up period 7-8 yrs

H. pylori infection – Surveillance Risk assessment of gastritis progression to gastric cancer
1
2
Operative link for gastritis assessment (OLGA)
Rugge et al. APT 2010;31:1104
OLGIM for surveillancede Vries et al. Helicobacter2010;15:259

Adapted from Vauhkonen et al. Best Pract. and Res. Clin. Gastroenterol. 20,4,2006
diffuse gastric cancer intestinal gastric cancer
adenomadysplasia
atrophic gastritisintestinal metaplasia
Chronicactive gastritisH. pylori
normal
„genetic disposition“transmitted CHD1-mutation
Methylation: CDH1, DAP-K,HRASLS, LOX, MGMT,p14, RAR-ßAmplification: C-MET, K-SAMMutation: CHD1, TP53Expression: hTERT
CIMP/Microsatellite-InstabilityMethylation: p16, COX-2, GSTP1, hMLH1, MGMT, RASSF1A, RUNX3, TFF1Amplification: ERBB2Mutation: K-RAS, TP53LOH: APC, MCC, TP53
Expression: CDX1/2, COX-2, hTERT
Mutation: APC, TP53Methylation: APC, CDH1, DAP-K, hMLH1, p14, THBS1, TIMP-3Expression: EGFR, TGF-
adenoma

Endoscopic surveillance of gastric premalignant lesions improves cancer survival
Whiting et al. Gut 2002; 50: 278-81

Surveillance practice of pre-malignant gastric lesions- a long term nationwide study in the Netherlands
Cohort study 1991-2004
90,316 patients
-24% atrophic gastrits-67% intest. Metaplasia-9% dysplasia
Follow up 2005
25,793 patients1.7 % gastric cancer
-3.4% initial atrophic gastritis-7% initial intest. Metaplasia-17% initial mild/moder. dysplasia-68% initial severe dysplasia
Surveillance!!de Vries et al. Gastroenterology 2008

Surveillance for gastric cancer
Cost effectivness for endoscopy based surveillancerequires malignancy to occur
at a prevalence of > 6%
Yeh et al. Gastrointest Endosc. 2010 Jul;72(1):33-43

•Single life time screening at age 20,30,40
• single life time screening and rescreening of individuals with negative results
• universal treatment for H. pylori infection at age 20,30,40
Yeh et al. Int J Cancer 2009
H. pylori infection & prevention of gastric cancer
Three models tested in China
GC risk reduction by 15 %
‐ 1500 US$/live year saved
GC risk reduction by 17 %
‐ 2500 US$/live year saved

Screening/Surveillance for gastric cancer
correlation of low pepsinogen I
with corpus prevalent atrophic gastritis
94%
PEPSINOGEN combined with H. pylori antibodies best option
Lombardo et al. Clin Chem Lab Med. 2010 Sep;48(9):1327-32

Serological markers
• Screening for preneoplastic conditions
Gastrin 17
Pepsinogen I + IIPI/II-Ratio
H.pylori-Antibodies+
„Gastropanel“

Watabe et al. Gut 2005; 54: 764-8
The annual incidence of gastric cancer in a Japanese cohort in relation to H. pylori and pepsinogens at baseline
0,4 0,6
3,5
6
0
1
2
3
4
5
6
7
Hp-neg Hp-pos Hp-pos Hp-neg
Normal pepsinogens Low pepsinogens
0/00N=9293

Rationale ofScreening Methods
Endoscopy
Best detection rate (up to 87%)
Most expensive
Most invasive
Gastro-Panel
Less invasive
Relatively cheap
Alone not sufficient(preselects for endoscopy)
13C-UBT
Cheap
Non invasive
„Only“ H.pylori detected, not mucosal lesions

PGI PGII PGI/II G17B G17S HpAB
Atrophic gastritis in corpus low low highAtrophic gastritis in antrum low low highAtrophic gastritis in both a / c low low low low
Non-atrophic gastritis high
Non-atrophic gastritis, H.pylori high high
(GERD) (Low
http://www.gastropanel.net/ Condition of gastric mucosa - atrophic gastritis especially of
corpus and antrum (normal, gastritis / atrophic gastritis) & H. pylori infection
PG I, PG II and gastrin-17 levels describe structure & function More severe atrophic gastritis in corpus, the lower the
pepsinogen I and ratio of pepsinogen I / II More severe atrophic gastritis of antrum, the lower is gastrin-17
GastroPanel®: Diagnosis by an antibody test

Atrophy and Intestinal Metaplasia
Pepsinogen lowGastrin highH.Pylori serology negativeCag A positive

H. pylori and Gastric Cancer
How to proceed in practice?
• Family history• Gastropanel
•Endoscopy plus histology
• Bacterial virulence factors
• Inflammatory Gen- Polymorphisms
• nutrition habits
• smoking
Risk gastritis
Follow up

H.pylori-Eradication and GC-Prevention Hazards
Lee and Moss, Expert Opin Ther Targets 2007; Malfertheiner et al, AJG 2005; Meyer et al, Ann Intern Med 2002
Limitations of Eradication Therapy for GC-Prevention
Complex therapy (multi-agent) Compliance?
Availability(Developing countries) strict indication
Increasing resistance(Clarithromycin/Metronidazole)
Critical point of timefor eradication

Maastricht 3
Statement: H. pylori infection is the most common proven
risk factor for human non-cardia gastric cancer.
Level of Evidence: n.a. Grade of Recommendation: A
97,7
2,30
25
50
75
100
I agree I don't agree
97,7
2,30
25
50
75
100
I agree I don't agreeValues in percentage
Gut 2007

Maastricht 3
Statement: H. pylori eradication has the potential to prevent gastric
cancer gastric cancer.
Level of Evidence: n.a. Grade of Recommendation: A
97,7
2,30
25
50
75
100
I agree I don't agree
97,7
2,30
25
50
75
100
I agree I don't agreeValues in percentage
Malfertheiner et al Gut 2007

Malfertheiner et al J. Dig. Dis. 2010

The incidence of gastric cancer in the community to be targeted
Screening reserved for risk groups and risk populations
Identifying high risk groups
Concluding considerations

„ it is not enough to know,it must also be put into practice“