-
7/29/2019 Pulm Edema Nav
1/20
CASE PRESENTATION
35 years old male from CCU
c/c chest pain and SOB for 3 daysClinically having ACS with
anterior
wall MI with CCF
CXR PA view done.
-
7/29/2019 Pulm Edema Nav
2/20
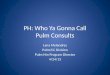
B/L symmetrical alveolar opacities present in perihilar
region
giving bat wing appearance with sparing of periphery.
-
7/29/2019 Pulm Edema Nav
3/20
IMPRESSION
ACS with anterior wall MI with CCF(clinically)
with pulmonary edema(on CXR).
-
7/29/2019 Pulm Edema Nav
4/20
Pulmonary oedema
Pulmonary oedema is a broad descriptive
term and is usually defined as an abnormal
accumulation of fluid in the extra-vascular
compartments of the lung.
-
7/29/2019 Pulm Edema Nav
5/20
Pathophysiology One method of classifying pulmonary oedema is as
four
main categories on the basis of pathophysiology which
include increased hydrostatic pressure oedema
two pathophysiological and radiological phases are recognizedin
the development of pressure oedema
interstitial oedema
alveolar flooding or oedema these phases are virtually identical
for left-sided heart
failure and fluid overload
permeability oedema with diffuse alveolar damage (DAD)
permeability oedema without diffuse alveolar damage
mixed edema due to simultaneous increased hydrostaticpressure
and permeability changes
http://radiopaedia.org/articles/missing?article[title]=left-sided+heart+failurehttp://radiopaedia.org/articles/missing?article[title]=fluid+overloadhttp://radiopaedia.org/articles/missing?article[title]=left-sided+heart+failurehttp://radiopaedia.org/articles/missing?article[title]=left-sided+heart+failurehttp://radiopaedia.org/articles/missing?article[title]=fluid+overloadhttp://radiopaedia.org/articles/missing?article[title]=fluid+overloadhttp://radiopaedia.org/articles/missing?article[title]=left-sided+heart+failurehttp://radiopaedia.org/articles/missing?article[title]=left-sided+heart+failurehttp://radiopaedia.org/articles/missing?article[title]=left-sided+heart+failurehttp://radiopaedia.org/articles/missing?article[title]=left-sided+heart+failure
-
7/29/2019 Pulm Edema Nav
6/20
CausesCardiogenic pulmonary edema.
Heart failure
Coronary artery disease with left ventricular failure.
Cardiac arrhythmias Fluid overload -- for example, kidney
failure.
Cardiomyopathy
Obstructing valvular lesions -- for example, mitral stenosis
Myocarditis and infectious endocarditis
Non-cardiogenic pulmonary edema -- due to changes in capillary
permeability
Smoke inhalation.
Head trauma
Overwhelming sepsis.
Hypovolemia shock
Re-expansion
By drainage of a large pleural effusion with thoracentesis Of
the lung collapsed by a large pneumothorax
High altitude pulmonary edema
Disseminated intravascular coagulopathy (DIC)
Near-drowning
Overwhelming aspiration
Adult (acute) respiratory distress (deficiency) syndrome
(ARDS)
http://www.learningradiology.com/archives03/COW%20072-Mitral%20stenosis/mscorrect.htmhttp://www.learningradiology.com/archives/COW%20019-Re-expansion%20pulm%20edema/reexpulmedemacorrect.htmhttp://www.learningradiology.com/archives06/COW%20211-Aspiration%20pneumonia/aspirationcorrect.htmhttp://www.learningradiology.com/lectures/chestlectures/ardrsppt_files/frame.htmhttp://www.learningradiology.com/lectures/chestlectures/ardrsppt_files/frame.htmhttp://www.learningradiology.com/archives06/COW%20211-Aspiration%20pneumonia/aspirationcorrect.htmhttp://www.learningradiology.com/archives/COW%20019-Re-expansion%20pulm%20edema/reexpulmedemacorrect.htmhttp://www.learningradiology.com/archives/COW%20019-Re-expansion%20pulm%20edema/reexpulmedemacorrect.htmhttp://www.learningradiology.com/archives/COW%20019-Re-expansion%20pulm%20edema/reexpulmedemacorrect.htmhttp://www.learningradiology.com/archives03/COW%20072-Mitral%20stenosis/mscorrect.htmhttp://www.learningradiology.com/archives03/COW%20072-Mitral%20stenosis/mscorrect.htm
-
7/29/2019 Pulm Edema Nav
7/20
Pulmonary oedema grading One grading system ofpulmonary oedema
based
on chest radiograph appearances and pulmonarycapillary wedge
pressure (PCWP) is as.
grade 0 : normal chest radiograph - PCWP 8 -12mmHg
grade 1: shows evidence of upper lobe diversionon a chest
radiograph - PCWP 13- 18 mmHg
grade 2 : shows interstitial oedema on a chest
radiograph : PCWP 19 - 25 mmHg grade 3 : shows alveolar oedema
on a chest
radiograph : PCWP > 25 mmHg
http://radiopaedia.org/articles/pulmonary-oedemahttp://radiopaedia.org/articles/pulmonary-oedemahttp://radiopaedia.org/articles/pulmonary-oedema
-
7/29/2019 Pulm Edema Nav
8/20
Imaging Findings
The key findings ofpulmonary interstitial edema: Kerley B lines
(septal lines) Seen at the lung bases, usually no more than 1 mm
thick and 1 cm
long, perpendicular to the pleural surface.
Pleural effusions Usually bilateral, frequently the right side
being larger than the left
If unilateral, more often on the right.
Fluid in the fissures Thickening of the major or minor
fissure.
Peribronchial cuffing
Visualization of small doughnut-shaped rings representing fluid
inthickened bronchial walls.
Collectively, the above four findings
comprisepulmonaryinterstitial edema.
-
7/29/2019 Pulm Edema Nav
9/20
Increased hydrostatic pressure edema in a 33-year-old man with
acute
myelocytic leukemia who was admitted for fluid overload with
renal and
cardiac failure.chest radiograph demonstrate progressive lobar
vessel
enlargement, peribronchial cuffing (arrows).
-
7/29/2019 Pulm Edema Nav
10/20
Fluid in the major or minor fissure(shown here) produces
thickening of thefissure beyond the pencil-point
thickness it can normally attain.
Cephalization meanspulmonary venoushypertension,
-
7/29/2019 Pulm Edema Nav
11/20
Kerley B Lines are short, white linesperpendicular to the
pleural surfaceat the lung base.
Peribronchial cuffing results whenfluid-thickened bronchial
wallsbecome visible producing doughnut-like densities in the lung
parenchyma
-
7/29/2019 Pulm Edema Nav
12/20
Pulmonary alveolar edema(Bat Wing
Edema) refers to a central, nongravitational distribution
of alveolar edema.
It is seen in less than 10% of cases of pulmonary
edema and generally occurs with rapidlydeveloping severe cardiac
failure as seen in acutemitral insufficiency (associated with
papillarymuscle rupture, massive myocardial infarct, and
valve leaflet destruction due to septicendocarditis) or renal
failure. In bat wing edema,the lung cortex is free of alveolar or
interstitialfluid.
-
7/29/2019 Pulm Edema Nav
13/20
Bat wing edema in a 71-year-old woman with fluid overload
and
cardiac failure. Chest radiograph (a) and high-resolution CT
scan(b) demonstrate bat wing alveolar edema with a central
distribution and sparing of the lung cortex.
-
7/29/2019 Pulm Edema Nav
14/20
Differential diagnosis
General imaging differential considerationsinclude
diffuse pulmonary haemorrhage : has no
dependent gradient and usually no pleural
effusion.
diffuse pulmonary infection : usually there is
no dependent gradient.can involve any part of
lung.
http://radiopaedia.org/articles/diffuse-pulmonary-haemorrhagehttp://radiopaedia.org/articles/missing?article[title]=diffuse+pulmonary+infectionhttp://radiopaedia.org/articles/missing?article[title]=diffuse+pulmonary+infectionhttp://radiopaedia.org/articles/missing?article[title]=diffuse+pulmonary+infectionhttp://radiopaedia.org/articles/diffuse-pulmonary-haemorrhage
-
7/29/2019 Pulm Edema Nav
15/20
SPOTTER
-
7/29/2019 Pulm Edema Nav
16/20
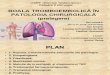
Intraosseous lipomaseen in fouth decade
a clump of dystrophic calcification may be seen within the
osteolytic lesion
on plain radiographs and CT scans target or doughnut shaped
sequestrum.
The calcification represents infarcted fat.
D/D on X RAY: Simple bone cyst :3-14 years of age
Chondroblastoma
well marginated, round to oval,osteolytic lesion.The tumor
matrix often containscalcification, which is better appreciated on
CT scans.Occasionally, the tumor may have
multiloculatedappearance.
Enchondroma.- children and young adults. one orseveral, round or
oval areas of decreased radiopacityare seen in the calcaneum. The
lesions have well-defined margins. The tumor matrix is often
calcified.
-
7/29/2019 Pulm Edema Nav
17/20
THANK YOU
REFERENCES:
http://radiographics.rsna.org/content/19/6/1
507.full.
http://www.learningradiology.com/
http://radiographics.rsna.org/content/19/6/1507.fullhttp://radiographics.rsna.org/content/19/6/1507.fullhttp://radiographics.rsna.org/content/19/6/1507.fullhttp://radiographics.rsna.org/content/19/6/1507.fullhttp://radiographics.rsna.org/content/19/6/1507.fullhttp://radiographics.rsna.org/content/19/6/1507.fullhttp://radiographics.rsna.org/content/19/6/1507.full
-
7/29/2019 Pulm Edema Nav
18/20
-
7/29/2019 Pulm Edema Nav
19/20
Cardiogenic and non cardiogenic
pumonary edema In NCPE, the initial site of fluid accumulation
is the pulmonary
interstitium including peribronchial cuffs and septal lines.
This typeof edema appears predominantly as alveolar filling, since
thealtered (disrupted) alveolar-capillary membrane allows for
thedirect accumulation in the air spaces of fluid that is
tooproteinaceous to be cleared via the interstitium. In contrast,
incardiogenic pulmonary edema filling of air spaces
(alveolarflooding) occurs when the interstitial space is finally
overwhelmed.
2. Kerley lines are never seen in increased permeability
edemawhereas they are a common finding in cardiogenic. The
appearanceof Kerley lines in NCPE, indicates the coexistence of
cardiogenic
pulmonary edema. 3. Patchy or peripheral pattern of edema is
relatively specific for
NCPE. Air bronchograms are frequently seen in patients with
NCPE.
-
7/29/2019 Pulm Edema Nav
20/20
In cardiogenic pulmonary edema thedistribution of edema is
central and pleuraleffusion usually coexists.
5. In NCPE, cardiac size, vascular pedicle widthand pulmonary
blood volume are usuallynormal. On the contrary, in
cardiogenicpulmonary edema cardiac size is increased,vascular
pedicle width is enlarged and there isinverted distribution of
blood flow.